
Abstract
Objectives
There have been few studies that have fully elucidated the relationship between genomic mutations in pulmonary adenocarcinomas and occult lymph node (LN) metastases (pN1-2) despite a preoperative clinical N0 stage (cN0). It is well known that anaplastic lymphoma kinase (ALK) rearrangements are more likely to occur in younger patients with high grade tumors. The aim of this study was to investigate the genomic status, examine the clinicopathologic features, and evaluate whether ALK mutations are associated with occult LN metastases.
Materials and methods
We retrospectively evaluated 459 Japanese patients who underwent pulmonary resection of cN0 adenocarcinomas between January 2012 and December 2015. The clinicopathologic characteristics, including age, sex, smoking index, tumor maximum diameter and consolidation/tumor ratio on computed tomography (CT), maximum standardized uptake value on positron emission tomography (PET) and gene mutations (epidermal growth factor receptor [EGFR], ALK, and kirsten ras genes (KRAS), were evaluated.
Results
ALK and EGFR and KRAS mutations were all mutually exclusive. Among 324 patients found to have mutations, ALK was involved in 19 (5.9%), EGFR in 266 (82.1%), and KRAS in 39 (12.0%). The incidence of occult LN metastases did not differ significantly between those with or without mutations (p=0.27). On univariate and multivariate analyses, tumors with ALK were more likely to have occult LN metastases (p=0.03). In cN0 tumors with ALK, pN1 was diagnosed in 26.3% and pN2 in 10.5%, whereas pN1 or pN2 stage was found in <10.0% in those with EGFR or KRAS mutations or with no mutations at all. No significant difference was found in the 2-year disease-free survival among those with gene mutations (p=0.08).
Conclusion
This study highlights the frequency of PET- and CT-negative occult LN metastases in resected adenocarcinomas with ALK rearrangement. Our multivariate analysis showed that ALK rearrangements were associated with a significantly higher incidence of occult LN metastasis compared with ALK-negative adenocarcinomas.
Introduction
Lobectomy with systemic lymph node (LN) dissection is a standard procedure for non-small-cell lung cancer (NSCLC). Preoperative diagnosis of patients with LN-negative (cN0) disease poses a clinical dilemma, as approximately 10% of patients with cN0 cancer in our institution are found to have hilar or mediastinal LN involvement on the pathology of the resected specimens. There is evidence that patients with advanced NSCLC benefit from adjuvant chemotherapy after complete pulmonary resection.Citation1–Citation3 Although the value of radical LN dissection remains undetermined, precise LN staging is a clinical essential, as the actual stage can affect the long-term outcome. Computed tomography (CT) is routinely accepted as the standard method for preoperative LN staging. Although the commonly used criterion for a clinical diagnosis of LN metastasis on CT is a short-axis diameter >10 mm, several authors have reported its low sensitivity and specificity.Citation4–Citation6 Currently, positron emission tomography (PET) with 18F-fluorodeoxyglucose is considered clinically superior to CT for LN staging, but even this method carries a false-negative rate for the identification of LN metastasis.Citation7
Genomic mutations as well as histologic features are recognized as critically important predictors of the biological behavior of lung adenocarcinomas. Anaplastic lymphoma kinase (ALK) gene rearrangements are found in approximately 2%–7% of NSCLCs.Citation8 It is well known that ALK rearrangement is more likely to be found in NSCLC with adenocarcinoma histology, younger age, light or never smoking history, and advanced stage.Citation9,Citation10 Choi et alCitation11 reported that adenocarcinoma with ALK rearrangements appeared as solid masses with lobulated margins on CT and were more likely to be associated with lymphangitic metastasis, advanced LN metastasis, and pleural or pericardial metastasis than were tumors with epidermal growth factor receptor (EGFR) mutations. Most of these clinical discoveries highlight the importance of genetic evaluation of tumors that might enable the targeted treatment. However, the frequency of such changes, especially ALK rearrangements, is comparatively low.
Few reports have focused on LN metastases associated with ALK rearrangements, especially in early-stage NSCLC. To the best of our knowledge, there have been few studies of adenocarcinomas with occult LN metastases (pN1–2) despite preoperative cN0 staging. Therefore, the aim of this current study was to investigate the relationship between genomic status, clinicopathology, and pN1–2 adenocarcinoma.
Materials and methods
Patients and clinical evaluation
Between January 2012 and December 2015, 459 Japanese patients who underwent surgical resection for a preoperative diagnosis of cN0 lung adenocarcinoma at the Aichi Cancer Center Hospital were selected for this retrospective study. Patients were included who had had surgery alone as first treatment without neoadjuvant chemotherapy or radiotherapy and no other malignant tumors in the 5 years prior to lung resection. All patients had undergone pulmonary segmentectomy or more with conventional LN dissection. All clinical data were anonymized before analyses of this study. This study was approved by the institutional review board (2017-1-297) at Aichi Cancer Center Hospital. The board waived the need for informed consent because of the retrospective nature of this study.
Clinical staging was based on CT scans of the chest and abdomen, magnetic resonance imaging of the head, abdominal ultrasound, bone scintigraphy, and/or PET. Tumors were staged according to the TNM classification system (seventh edition).Citation12 The pathology diagnosis was classified according to the International Association for the Study of Lung Cancer/American Thoracic Society/European Respiratory Society International Multidisciplinary Classification of Lung Adenocarcinoma.Citation13
On preoperative on thin sliced CT (1–2 mm), we evaluated the tumor maximum diameter (TMD) and the consolidation diameter on the lung window setting (level = −550 HU; width =1,500 HU) and hilar and mediastinal LNs on the mediastinal window setting (level =40 HU; width =360 HU).Citation14,Citation15 The C/T ratio was calculated by dividing the consolidation diameter by the TMD. A C/T ratio of >0.5 has previously been reported to suggest a high frequency of LN metastases in NSCLC.Citation14–Citation16 LN metastasis was diagnosed on imaging when the short axis of a node was at least 10 mm in diameter or if there was evident accumulation of 18F-fluorodeoxyglucose on PET.
The following data were extracted from patient records: age, sex, smoking index, TMD and C/T ratio on CT, maximum standardized uptake value (SUV max) on PET, and gene mutations (EGFR, ALK, and kirsten ras genes (KRAS).
Pathology diagnosis and genetic analysis
Mutation analyzes were carried out for EGFR, KRAS, and ALK as previously reported.Citation17,Citation18 Reverse transcriptase-polymerase chain reaction direct sequencing of EGFR, KRAS, and ALK was used to assess the mutational status. In addition, tissue was screened for immunohistochemistry if the ALK RNA could be assessed or with break-apart fluorescence in situ hybridization for confirmation.
Statistical analysis
We analyzed the relationships between each gene mutation and clinicopathologic factors using JMP software version 10.0 (SAS Institute, Inc., Cary, NC, USA). Significant risk factors for LN metastasis determined by univariate analysis were used for multivariate analysis. Continuous variables were expressed using the median (interquartile range). Categorical variables, given as percentages, were compared using Fischer’s exact test. Comparison among more than 3 groups was calculated by the Kruskal–Wallis test. Multivariate logistic regression analysis was used to calculate odds ratios with 95% confidence intervals and estimated probabilities for pathologic LN metastasis. A p<0.05 was considered significant.
Results
Patient characteristics and gene mutations
The clinicopathologic characteristics are summarized in . Of the 459 patients with adenocarcinomas, 135 (29.4%) were triple negative for the genes evaluated and 324 had a mutation. Significantly lower male-to-female ratio, smoking index, and serum carcinoembryonic antigen (CEA) levels were found in those with genomic mutations than in those with triple-negative NSCLC. The pathological LN metastasis status did not differ significantly between those with and without mutations (p=0.27).
Table 1 Characteristics of patients with cN0 pulmonary adenocarcinoma
Genomic mutations and clinicopathologic findings
ALK rearrangement and EGFR and KRAS mutations were all mutually exclusive. Of the 324 cases of genomic abnormalities, mutations of ALK were present in 19 (5.9%), EGFR in 266 (82.1%), and KRAS in 39 (12.0%) There were significant differences among the three groups in age, smoking index, TMD, C/T ratio, maximum tumor size on pathology, and pathological LN metastases ().
Table 2 Characteristics of patients with cN0 pulmonary adenocarcinoma who had gene mutations
The final LN status is summarized in , with patients with ALK rearrangement being much more likely to have pathologically positive LNs (pN1 26.3% and pN2 10.5%) compared with those with EGFR or KRAS mutations or those who were triple negative on gene testing (pathologically positive LNs found in <10.0% in each group) (p=0.02, ).
Figure 1 The proportion of patients with cN0 pulmonary adenocarcinoma found to have LN metastases on pathology (pN1, gray; pN2, black; node negative patients [cN0 → pN0], white) in each mutational classification.
Notes: Patients with ALK rearrangement tended to have a higher incidence of occult hilar or mediastinal LN metastases. Triple negative indicates patients with no mutation in ALK, EGFR, or KRAS.
Abbreviations: ALK, anaplastic lymphoma kinase; EGFR, epidermal growth factor receptor; KRAS, kirsten ras genes; LN, lymph node.
![Figure 1 The proportion of patients with cN0 pulmonary adenocarcinoma found to have LN metastases on pathology (pN1, gray; pN2, black; node negative patients [cN0 → pN0], white) in each mutational classification.Notes: Patients with ALK rearrangement tended to have a higher incidence of occult hilar or mediastinal LN metastases. Triple negative indicates patients with no mutation in ALK, EGFR, or KRAS.Abbreviations: ALK, anaplastic lymphoma kinase; EGFR, epidermal growth factor receptor; KRAS, kirsten ras genes; LN, lymph node.](/cms/asset/67ea8157-ba22-44ce-8702-97c1accbb6fa/dcmr_a_12185321_f0001_b.jpg)
The relationship between clinicopathologic findings and pathological LN metastases
We further investigated the relationship between selected clinicopathologic findings and the risk of having occult LN metastases. When we enforced multivariate analysis using the factors in verification of the significant difference by univariate analysis, we found that patients with CEA levels >5 ng/mL, TMD >30 mm, C/T ratio >0.5, representative preoperative findings likely to be lymph node metastases, and ALK rearrangement, were more likely to harbor LN metastases ().
Table 3 Univariate and multivariate analyses of clinicopathological variables associated with occult LN metastases in pulmonary adenocarcinoma
Postoperative prognosis
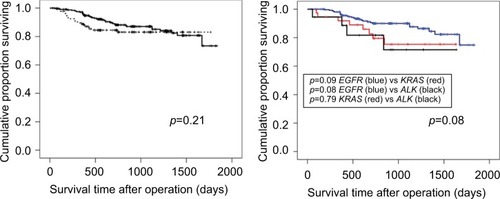
As shown in , the 2-year disease-free survival rates were 88.1% for triple negative and 84.4% for any mutation status, but no significant difference was obtained (p=0.21) (). The 2-year disease-free survival in patients with KRAS (81.7%) and ALK mutations (79.5%) showed a tendency to poorer prognosis as compared to those with EGFR mutations (89.9%), although a significant difference was not obtained (p=0.08) ().
Figure 2 Kaplan-Meier curves for the disease-free survival: (A) comparison of triple negative (dotted line) versus any mutation status (solid line); and (B) comparison of each of the mutations: EGFR, KRAS, and ALK.
Abbreviations: ALK, anaplastic lymphoma kinase; EGFR, epidermal growth factor receptor; KRAS, kirsten ras genes.
Discussion
In this study of patients with cN0 adenocarcinoma, the incidence of pN2 was 7.2% and that of pN1 or 2 was 15.5%, compatible with data reported for previous studies.Citation19 We found that the incidence of occult LN metastases did not differ significantly between tumors with one of the three gene mutations (ALK, EGFR, and KRAS) and those which were triple negative for the mutations. However, we found that tumors with ALK rearrangement were significantly more likely to have occult LN metastases than those with the other two mutations (p=0.03). Finally, on multivariate analysis, ALK rearrangement was associated with a significantly higher risk of occult LN metastases. A few investigators have performed detailed evaluations of the occult LN metastases in cN0 lung adenocarcinomas with ALK rearrangement.
We evaluated preoperative LN status using CT and PET for all patients. Patients with ALK rearrangement were more likely to have occult LN metastases on multivariate analysis. Park et al. reported that SUV max and volume-based parameters are significant risk factors for occult LN metastasis in patients with small peripheral NSCLCs (<3 cm in diameter) who underwent surgical resection with mediastinal LN dissection based on PET findings.Citation20 This observation was consistent with another study.Citation21 On the contrary, no significant difference for SUV or volume was observed on univariate analysis in our study (). The subtle differences between facilities in how PET is performed may be one reason for the discrepancy. They demonstrated that the SUV max was higher, but not significantly so, in patients with pN1–2 (6.95±3.91) compared to those with pN0 (4.12±3.85). In our study, however, the SUV max was significantly higher in patients with pN1–2 (6.99±7.41) than in those with pN0 (3.09±4.61), (p<0.01). Park et alCitation20 noted that accurate markers other than SUV max and solid tumor size are needed because of the results of the area under the curve for SUV max on receiver operating characteristic curve analysis in previous studies.
We previously reported on 27 surgically resected lung adenocarcinomas, analyzing the radiologic patterns. Compared with patients who were negative for ALK rearrangement, those who were ALK positive had significantly smaller tumors and had a lower tumor disappearance rate on CT, and spiculation was more frequent in small lesions.Citation17,Citation22 Recently, Choi et alCitation11 demonstrated that adenocarcinomas with ALK rearrangement appeared as a solid mass with lobulated margins on CT and were more likely to be associated with lymphangitic metastasis, advanced LN metastasis, and pleural or pericardial metastasis than tumors with EGFR mutations. The numbers in most studies are <100, because the frequency of fusion genes is comparatively low. Among clinicopathologic factors in our study aside from ALK rearrangement, CEA levels >5ng/mL, TMD >30 mm, and C/T ratio >0.5 were more likely to be associated with LN metastases on multivariate analysis. These associations may not necessarily correspond with the radiologic features found in those with ALK rearrangement. Clinically, the prediction of LN metastasis on preoperative CT and PET is more difficult in patients with ALK rearrangement than in those with other mutations (EGFR and KRAS) or who are triple negative, although further studies with accumulation of more data may improve our understanding.
In this study, patients with cN0 adenocarcinoma with ALK rearrangement were significantly more likely to have hilar or mediastinal LN metastases than those with KRAS or EGFR mutations. A few studies have performed detailed evaluations of lung adenocarcinomas with ALK rearrangement, noting a tendency for a higher rate of LN metastases.Citation23 Interestingly, Xu et alCitation24 noted that ALK-positive adenocarcinomas might metastasize to LNs early, despite the small size of the primary tumor. Several authors reported a lack of association between ALK rearrangement and prognosis, which was compatible with our current report. Therefore, accurate staging by radical mediastinal LN dissection may be associated with the long-term outcomes for tumors with ALK rearrangements.Citation10,Citation25 It is well known that ALK rearrangement in lung adenocarcinoma has a strong association with younger age, nonsmoking status, and clinically advanced stage.Citation26 However, it is not clear whether preoperative radiologic findings enable definitive prediction of prognosis, LN metastasis, or invasiveness for patients with clinically early-stage ALK-positive adenocarcinomas. Therefore, if ALK positivity is suspected based on clinical features, radical mediastinal LN dissection should be performed.
This current study had several limitations. First, the definition of LN metastasis by imaging is equivocal. A short axis of >10 mm is widely used for enlarged mediastinal and hilar LNs on CT.Citation4,Citation5 However, size criteria provide poor specificity for LN metastases. Although the diagnostic ability of PET-CT is superior to that of CT, diagnostic criteria for LN metastasis on PET-CT are still controversial. Second, the outcome of the patients, such as disease-free survival or overall survival, is not clear in this study because of a relatively short follow-up period.Citation27–Citation29 Third, this was a retrospective, single-institutional study with a small sample size. To provide meaningful data on prognostic differences and to avoid the increasing the error of this study, a prospective, multicenter study is required, which is in the planning phase. Fourth, patient bias existed regarding the procedure selection. We considered that lobectomy is higher in diagnosis precision than segmentectomy about hilum LN dissection. Therefore, we limited the indication of segmentectomy according to the CT mediastinal diameter from the previous studies because segmentectomy is not the standard therapy for invasive lung cancers.Citation14,Citation16 Fifth, it was impossible to argue about the curative effect of adjuvant chemotherapy, because small numbers of patients with mutations in ALK (4/19, 21.1%) underwent adjuvant chemotherapy.
In conclusion, this study highlights the frequency of PET- and CT-negative occult LN metastases in resected adenocarcinomas with ALK rearrangement. Our multivariate analysis showed that ALK rearrangement in cN0 NSCLC is significantly associated with a higher risk of occult LN metastasis compared to tumors without ALK mutations.
Acknowledgments
The authors thank Professor Kenichi Okubo, MD, PhD (Department of Thoracic Surgery, Tokyo Medical and Dental University, Medical Hospital) and Doctor Yusuke Sugita for their support with the supervision of the revised manuscript and the additional data collection.
Disclosure
The authors report no conflicts of interest in this work.
References
- ArriagadaRBergmanBDunantALe ChevalierTPignonJPVansteenkisteJCisplatin-based adjuvant chemotherapy in patients with completely resected non-small-cell lung cancerN Engl J Med200435035136014736927
- PistersKMEvansWKAzzoliCGCancer care Ontario and American society of clinical oncology adjuvant chemotherapy and adjuvant radiation therapy for stages I-IIIA resectable non small-cell lung cancer guidelineJ Clin Oncol2007255506551817954710
- KatoHIchinoseYOhtaMA randomized trial of adjuvant chemotherapy with uracil – tegafur for adenocarcinoma of the lungN Engl J Med20043501713172115102997
- GlazerGMGrossBHQuintLEFrancisIRBooksteinFLOrringerMBNormal mediastinal lymph nodes: number and size according to American Thoracic Society mappingAJR Am J Roentgenol19851442612653871268
- KiyonoKSoneSSakaiFThe number and size of normal mediastinal lymph nodes: a postmortem studyAJR Am J Roentgenol19881507717763258087
- BeadsmooreCJScreatonNJClassification, staging and prognosis of lung cancerEur J Radiol200345181712499060
- LeeAYChoiSJJungKPParkJSLeeSMBaeSKCharacteristics of metastatic mediastinal lymph nodes of non-small cell lung cancer on preoperative F-18 FDG PET/CTNucl Med Mol Imaging2014481414624900137
- SodaMChoiYLEnomotoMIdentification of the transforming EML-4-ALK fusion gene in non-small-cell lung cancerNature200744856156617625570
- SasakiTRodigSJChirieacLRThe biology and treatment of EML4-ALK non-small cell lung cancerEur J Cancer2010461773178020418096
- PaikJHChoiCMKimHClinicopathologic implication of ALK rearrangement in surgically resected lung cancer: a proposal of diagnostic algorithm for ALK-rearranged adenocarcinomaLung Cancer201276340340922129856
- ChoiCMKimMYHwangHJLeeJBKimWSAdvanced adenocarcinoma of the lung: comparison of CT characteristics of patients with anaplastic lymphoma kinase gene rearrangement and those with epidermal growth factor receptor mutationRadiology2015275127227925575117
- GoldstrawPCrowleyJChanskyKInternational Association for the Study of Lung Cancer International Staging Committee; Participating Institutions. The IASLC Lung Cancer Staging Project: proposals for the revision of the TNM stage groupings in the forthcoming (seventh) edition of the TNM Classification of malignant tumoursJ Thorac Oncol2007270671417762336
- TravisWDBrambillaENoguchiMInternational Association for the Study of Lung Cancer/American Thoracic Society/European Respiratory Society International Multidisciplinary Classification of Lung AdenocarcinomaJ Thorac Oncol2011624428521252716
- SakakuraNInabaYYatabeYEstimation of the pathological invasive size of pulmonary adenocarcinoma using high-resolution computed tomography of the chest: a consideration based on lung and mediastinal window settingsLung Cancer201695515627040852
- AokageKYoshidaJIshiiGIdentification of early t1b lung adenocarcinoma based on thin-section computed tomography findingsJ Thorac Oncol201381289129424457240
- SakaoYKurodaHMunMPrognostic significance of tumor size of small lung adenocarcinomas evaluated with mediastinal window settings on computed tomographyPLoS One20149e11030525365326
- FukuiTYatabeYKobayashiYClinicoradiologic characteristics of patients with lung adenocarcinoma harboring EML4-ALK fusion oncogeneLung Cancer20127731932522483782
- KobayashiYMitsudomiTSakaoYGenetic features of pulmonary adenocarcinoma presenting with ground-glass nodules: the differences between nodules with and without growthAnn Oncol20152615616125361983
- DarlingGEAllenMSDeckerPARandomized trial of mediastinal lymph node sampling versus complete lymphadenectomy during pulmonary resection in the patient with N0 or N1 (less than hilar) non-small cell carcinoma: results of the American College of Surgery Oncology Group Z0030 TrialJ Thorac Cardiovasc Surg2011141366267021335122
- ParkSYYoonJKParkKJLeeSJPrediction of occult lymph node metastasis using volume-based PET parameters in small-sized peripheral non-small cell lung cancerCancer Imaging2015152126694918
- TsutaniYMiyataYNakayamaHPrediction of pathologic node-negative clinical stage IA lung adenocarcinoma for optimal candidates undergoing sublobar resectionJ Thorac Cardiovasc Surg201214461365137122883546
- NakadaTOkumuraSKurodaHImaging characteristics in ALK fusion-positive lung adenocarcinomas by using HRCTAnn Thorac Cardiovasc Surg201521210210824899136
- HalpennyDFRielyGJHayesSAre there imaging characteristics associated with lung adenocarcinomas harboring ALK rearrangements?Lung Cancer201486219019425312988
- XuLLeiJWangQZLiJWuLClinical characteristics of patients with non-small cell lung cancers harboring anaplastic lymphoma kinase rearrangements and primary lung adenocarcinoma harboring epidermal growth factor receptor mutationsGenet Mol Res20152114 (4):12973–12983.
- ShawATYeapBYMino-KenudsonMClinical features and outcome of patients with non-small-cell lung cancer who harbor EML4-ALKJ Clin Oncol20091027264247425319667264
- MarchettiAArdizzoniAPapottiMRecommendations for the analysis of ALK gene rearrangements in non-small-cell lung cancer: a consensus of the Italian Association of Medical Oncology and the Italian Society of Pathology and CytopathologyJ Thorac Oncol20138335235823407559
- SilvestriGAGouldMKMargolisMLAmerican College of Chest PhysiciansNoninvasive staging of non-small cell lung cancer: ACCP evidenced-based clinical practice guidelines (2nd edition)Chest2007132178S201S17873168
- GouldMKKuschnerWGRydzakCETest performance of positron emission tomography and computed tomography for mediastinal staging in patients with non-small-cell lung cancer: a meta-analysisAnn Intern Med200313987989214644890
- PaulNSLeySMetserUOptimal imaging protocols for lung cancer staging: CT, PET, MR imaging, and the role of imagingRadiol Clin North Am20125093594922974779