
Abstract
Background
Enhanced recovery after surgery (ERAS) program is an effective evidence-based multidisciplinary protocol of perioperative care, but its roles in thoracic surgery remain unclear. This systematic review of randomized controlled trials (RCTs) aims to investigate the efficacy and safety of the ERAS programs for lung cancer surgery.
Materials and methods
We searched the PubMed and EMBASE databases to identify the RCTs that implemented an ERAS program encompassing more than four care elements within at least two phases of perioperative care in lung cancer surgery. The heterogeneity levels between studies were estimated by the Cochrane Collaborations. A qualitative review was performed if considerable heterogeneity was revealed. Relative risk (RR) and weighted mean difference served as the summarized statistics for the meta-analyses. Additional analyses were also performed to perceive potential bias risks.
Results
A total of seven RCTs enrolling 486 patients were included. The meta-analysis indicated that the ERAS group patients had significantly lower morbidity rates (RR=0.64; p<0.001), especially the rates of pulmonary (RR=0.43; p<0.001) and surgical complications (RR=0.46; p=0.010), than those of control group patients. No significant reduction was found in the in-hospital mortality (RR=0.70; p=0.58) or cardiovascular complications (RR=1.46; p=0.25). In the qualitative review, most of the evidence reported significantly shortened length of hospital and intensive care unit stay and decreased hospitalization costs in the ERAS-treated patients. No significant publication bias was detected in the meta-analyses.
Conclusion
Our review demonstrates that the implementation of an ERAS program for lung cancer surgery can effectively accelerate postoperative recovery and save hospitalization costs without compromising patients’ safety. A worldwide consensus guideline is urgently required to standardize the ERAS protocols for elective lung resections in the future.
Introduction
Rationale
Lung cancer is the leading cause of malignancy-related deaths worldwide and remains the most prevalent cancer in both developed and developing countries.Citation1,Citation2 Nowadays, surgical treatment is regarded not only as the optimal therapeutic measure for early-stage non-small-cell lung cancer (NSCLC), but also as a key component of multidisciplinary treatment for advanced-stage NSCLC.Citation3,Citation4 Advances in the radiographic techniques and the prevalent practice of cancer screening have substantially increased the opportunity for early detection, helping to offer more effective therapeutic options to lung cancer patients. However, despite advances in surgical techniques and perioperative care, the morbidity rate still remains at 20.8%–34.1% in patients undergoing lung cancer surgery, as reported in recent literature.Citation5,Citation6
Postoperative complications are commonly considered as the major cause of delayed recovery after surgery, resulting in the prolonged length of stay (LOS), increased hospitalization cost and poor life quality.Citation7 Thoracic surgeons usually focus on the efficacy of specific interventions during the in-hospital period, although these individual interventions seem not to further improve the postoperative outcomes.Citation8 Therefore, it is necessary to optimize the utilization of a variety of health care resources and implement a multidisciplinary care plan in the perioperative management of operable lung cancer.
Enhanced Recovery after Surgery (ERAS), an evidence-based multimodal protocol of perioperative care, was firstly introduced by Kehlet and MogensenCitation9 in colorectal surgery in the late 1990s, in order to minimize the perioperative stress responses, catabolism and morbidity rates, shorten the LOS, and fasten postoperative recovery to achieve an early return to normal life. Since then, the ERAS strategies have dramatically developed and encompassed an increasing number of elements within all phases of perioperative care. These care elements are believed to have synergistic effects on the attenuation of operative stress responses and the protection of baseline function status, leading to an accelerated recovery postoperatively.Citation10,Citation11
A recent systematic review with meta-analysis based on 38 randomized controlled trials (RCTs) has demonstrated the great efficacy of ERAS programs in terms of reducing the morbidity rate and shortening the LOS across surgical specialties.Citation12 However, these findings could be hardly generalized to lung resections because of the limited supporting data for quantitative synthesis.Citation12 A later evidence-based review reported by Fiore et alCitation7 attempted to evaluate the clinical roles of ERAS programs in elective lung resections, but finally failed to draw a convincing conclusion. Only six comparative analyses were included in that review, while five of them were nonrandomized studies, resulting in high bias risks favoring the intervention. Given such concerns, the authors have appealed for more well-designed RCTs to investigate the effects of ERAS programs on pulmonary resections.Citation7
Objectives
The primary purpose of our evidence-based literature review was to integrate the clinical data from RCTs and lung cancer cases to summarize the clinical significance of ERAS programs on a range of postoperative outcomes (in-hospital morbidity, in-hospital mortality, LOS and hospitalization cost) in patients undergoing lung cancer surgery.
Materials and methods
Protocol
This evidence-based review of published RCTs was conducted in compliance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement.Citation13 Additional PRISMA checklist is shown in the Supplementary materials.
Search strategy
Complete procedures for a comprehensive literature retrieval ranged from July 25 to August 2, 2017. No publication date restriction was imposed during the retrieval.
Three researchers were assigned to search two universal electronic databases, the PubMed and EMBASE (via the Ovid interface), to recognize the eligible articles updated to July 25, 2017. We used the following 9 key words (5 “ERAS” terms and 4 “lung cancer” terms) and two Boolean Operators (“AND” and “OR”) to formulate four search strings in each selected database:
ERAS terms: “fast-track”, “enhanced recovery”, “intensive rehabilitation”, “accelerated rehabilitation” and “ERAS”
Lung cancer terms: “lung cancer”, “lung carcinoma”, “lung neoplasm” and “lung malignancy”
The search details are shown in the Supplementary materials. Moreover, we also manually searched the reference lists of retried publications to identify any possible study with no duplication.
Eligibility criteria
The following eligibility criteria were established to determine the appropriateness of studies for our review.
Study designs
Only RCTs were considered eligible. The sample size was not limited. The following studies were immediately excluded because of their irrelevant styles: cohort studies, case series, reviews, animal experiments and conference abstracts.
Participants
The target diseases were operable lung cancers, including both primary and secondary lesions. A small cohort of mixed malignancies was also included. No limitation was imposed for any basic characteristic of the patients.
Interventions
Elective pulmonary resections operated by traditional thoracotomy and video-assisted thoracoscopic surgery (VATS) approaches were considered eligible.
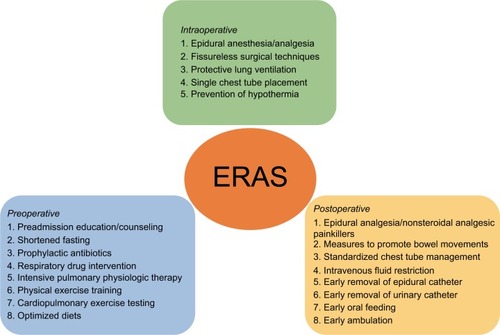
We recognized a total of 21 ERAS elements encompassing all phases of perioperative care (preoperative/intraoperative/postoperative) in the literature,Citation7,Citation10–Citation12 as shown in . An ERAS program involving more than four of these elements and encompassing at least two phases of perioperative care was considered eligible.
Figure 1 Care elements implemented in the ERAS protocols for lung cancer surgery.
Endpoints and outcome measures
The primary outcomes of interest were overall morbidity and in-hospital mortality. Overall morbidity was defined by the presence of any individual complication within 30 days after surgery or later during the same hospitalization. In-hospital mortality was defined as death within 30 days after surgery or later during the same hospitalization.
The secondary outcomes of interest included the LOS, length of intensive care unit (ICU) stay and total hospitalization cost. LOS was calculated from the admission day to the discharge day. Length of ICU stay referred to the duration of time spent in ICU after surgery.
Studies reporting any one of the above outcomes were included in this review. Sufficient demographics or statistics should be available for the estimation of relative risks (RRs) or weighted mean differences (WMDs).
Publications
In addition, only the most recent study was included if a series of studies was performed on overlapping patients. Only full-text papers published in peer-reviewed journals were included. No language restriction was imposed.
Data collection
Process
We designed a Microsoft Office Excel spreadsheet to extract relevant information from each included RCT. This process was performed by two researchers and cross-checked by another reviewer.
Data items
The following details were collected from each study:
“publication data” including authors, years, nations and languages;
“experimental data” including the RCT design (single center/multicenter), study period, surgical procedures, operative approaches (thoracotomy/VATS), ERAS elements and follow-ups;
“demographic data” including the total sample size, the number of patients enrolled in the ERAS group and the control group, gender, age, body mass index, forced expiratory volume in 1 second, American Society of Anesthesiologists scores, histologic subtypes and clinical stages; and
“outcome data” including the dichotomous statistics or demographics about the morbidity and mortality, and continuous data for the LOS, length of ICU stay and hospitalization cost.
Quality assessment
We computed the Jadad score of each included study according to the Jadad scale, as a valid and reliable three-question measure tool for assessing the methodological quality of RCTs.Citation14 A scoring system with up to 5 points was utilized in the Jadad scale. It conferred up to 2 points to the randomization, 2 points to the blinding of studies and 1 point to the reasons of withdrawals. Finally, a Jadad score ≥3 points indicated a high-quality RCT.
Statistical analysis
All of the following statistical analyses were accomplished by STATA 12.0.
Summary measures
For primary outcomes, we calculated the RR with 95% CI to summarize the effects of ERAS programs on postoperative morbidity and mortality. With regard to secondary outcomes, the WMD with 95% CI served as the appropriate statistic to summarize the mean values with SDs for the LOS, length of ICU stay and hospitalization cost.
If the SD was not available for continuous data, we did not incorporate it in the quantitative synthesis because the extrapolation of SD was only applicable for studies with a large sample size and normal distribution of outcomes according to the guidelines of Cochrane Collaborations.Citation15
Synthesis of results
Cochrane Q test and I2 statistic were used to quantify the heterogeneity level. A rough guide to the threshold for interpreting the I2 statistic was given by the Cochrane Collaborations, and I2 of 40%, 60% and 75% represented low, moderate and considerable variance, respectively.Citation15
In our study, fine heterogeneity was defined by I2<40% and p>0.1, and a standard fixed-effect model test (Mantel–Haenszel method) was utilized for quantitative synthesis. Otherwise, a random-effect model test (DerSimonian–Laird method) was adopted when moderate-to-considerable heterogeneity was revealed by 40%≤I2<75% and p≤0.1.
However, if there was considerable heterogeneity between studies (I2≥75% and p≤0.1), a meta-analysis was canceled because it might be misleading to quote an average value for the intervention effects. Instead, a qualitative summary of evidence was performed.Citation15
Additional analyses
We conducted a sensitivity analysis, in which the impact of each study on the overall estimates could be detected by omitting the individual study sequentially, to further examine the stability of pooled estimates. The strong robustness of our meta-analysis was confirmed if there was no substantial variation between the adjusted results and the primary results.Citation15
To evaluate the efficacy of ERAS programs on postoperative morbidity in detail, we classified all enrolled patients into three subgroups according to their pulmonary, surgical and cardiovascular complications. A meta-analysis was then performed on each of these subgroups. Pulmonary, surgical and cardiovascular complications were judged according to the criteria used in recent large-registry trials based on the French Society of Thoracic and Cardiovascular Surgery database.Citation5,Citation16
Publication bias
Both Begg’s test and Egger’s test were used to detect any potential publication bias within the meta-analyses. The presence of bias was suggested by visual symmetry of Begg’s funnel plot, in which log (RRs) or log (WMDs) were plotted against their corresponding standard errors.Citation17 In addition, its significance was also revealed if Egger’s p value was <0.05.
Results
Study selection
Our literature retrieval is presented as a PRISMA diagram ().
Figure 2 PRISMA flow diagram of literature retrieval.
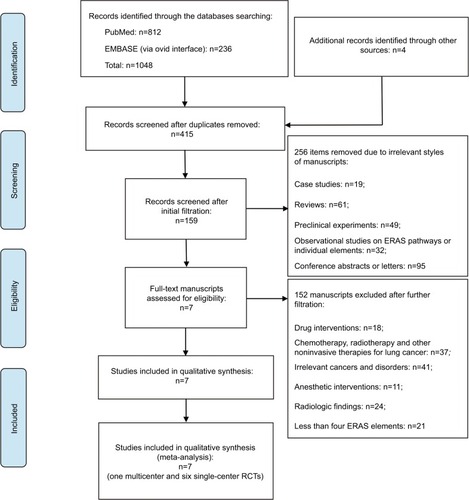
A total of 1048 publication items were primarily identified, including 812 PubMed citations and 236 EMBASE citations. In addition, a manual search of the reference lists also yielded four relevant studies. After excluding the duplicates, 415 items entered the initial filtration by screening on their titles and abstracts. Then, 256 of them were directly excluded from further filtration because of their irrelevant literature styles. By reading through 159 retrieved articles, we further excluded 152 articles addressing irrelevant topics and considered the remaining 7 studies for possible eligibility. Finally, these seven studies were judged to meet all the eligibility criteria and were included in our review.Citation18–Citation24
Study characteristics
Baseline characteristics and major perioperative outcomes in each RCT are summarized in and , respectively.
Table 1 Baseline characteristics
Table 2 Postoperative outcomes
Study designs
The seven included RCTs were published between 2008 and 2017. Six of them were single-center RCTsCitation18–Citation20,Citation22–Citation24 and only one study was a multicenter RCT.Citation21 There were five papers written in English languageCitation18,Citation19,Citation21–Citation23 and two papers written in Chinese language.Citation20,Citation24 Their sample size ranged from 35 to 151.
Participants
This review comprised a total of 486 surgical patients who were consecutively enrolled from 2007 to 2016. Approximately half of these patients were from China (n=217; ratio=44.7%),Citation18–Citation20,Citation24 followed by 209 patients from Europe (ratio=43.0%)Citation21,Citation22 and 60 patients from the Middle East (ratio=12.3%).Citation23 Half of these patients were randomized to the ERAS group (n=243) and the other half to the control group (n=243).
Majority of the patients were diagnosed with primary NSCLCs (n=472; ratio=97.1%). With respect to operative modes, there were 326 patients who underwent lobectomy (ratio=67.1%), while pneumonectomy was performed on 78 patients (ratio=16.0%) and sublobar resections on 82 patients (ratio=16.9%). Most of the patients were operated by standard posterolateral thoracotomy (n=392; ratio=80.7%), and only 94 patients were operated by VATS procedures (ratio=19.3%). The comparisons of the above perioperative parameters and other available patient characteristics between the ERAS group and the control group are shown in .
Interventions
Complete details of ERAS interventions estimated in each RCT are summarized in . The number of ERAS elements utilized in all seven RCTs ranged from 5 to 11.Citation18–Citation24 They varied across these seven RCTs, but overlapped for some common components, as shown in .
Table 3 ERAS protocols implemented in eligible RCTs
Outcome measures
The outcome data reported in each RCT are outlined in .
For the primary outcomes of interest, all seven RCTs compared the morbidity rates between the ERAS group and the control group.Citation18–Citation24 Effective in-hospital mortality rates were available in four included RCTs.Citation19,Citation21–Citation23
For the secondary outcomes of interest, all seven RCTs focused on the LOS, while five of them reported the continuous data that could be incorporated in the quantitative synthesis.Citation18–Citation20,Citation23,Citation24 The length of ICU stay was also evaluated in three RCTs,Citation21–Citation23 but only two of them reported sufficient mean values with SDs.Citation21,Citation23 In addition, there were three RCTs that reported the continuous data for hospitalization cost, and they were all conducted among Chinese participants.Citation18,Citation20,Citation24
Quality assessment
Complete records for the Jadad scale of each RCT are tabulated in . Finally, all seven RCTs got a Jadad score ≥3 points.Citation18–Citation24 Their mean Jadad score was 3.6 (range 3–5), suggesting that they were of fairly high quality.
Table 4 Quality assessment of eligible RCTs
Overall analysis
Overall morbidity
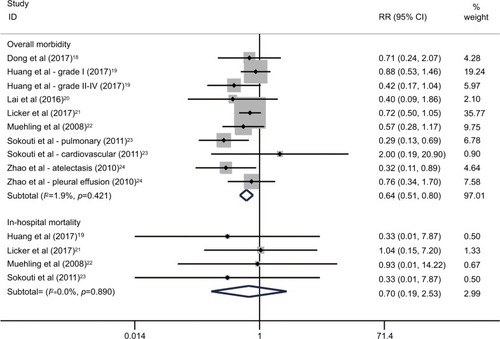
As shown in , the morbidity rates in the ERAS group and the control group ranged 8.3%–36.8% and 20.8%–56.7%, respectively. A fixed-effect model was used based on the low heterogeneity between studies (I2=1.9%; p=0.42). The pooled RR of all seven RCTs was 0.64, with its 95% CI ranging 0.51–0.80, revealing a significant decrease of morbidity rate in patients who received an ERAS program compared to that in patients who received conventional care (; ).Citation18–Citation24
Table 5 Meta-analyses for effects of the ERAS programs on postoperative morbidity and mortality
Figure 3 Overall analyses for effects of the ERAS programs on postoperative morbidity and mortality in patients undergoing lung cancer surgery.
In-hospital mortality
There were three deaths in the ERAS group and five deaths in the control group (). The pooled analysis of four available RCTs used a fixed-effect model (I2=0.0%; p=0.89) and showed no significant difference in the mortality rate between the ERAS group and the control group (RR=0.70; 95% CI=0.19–2.53; p=0.58), as shown in and .Citation19,Citation21–Citation23
Length of hospital stay
With regard to the LOS, we tried to integrate the valid continuous data available from five RCTs, but found a significantly high heterogeneity between studies (I2=86.5%; p<0.001).Citation18–Citation20,Citation23,Citation24 Thus, we canceled meta-analysis of these RCTs, but summarized their results qualitatively.
Among the five RCTs, four indicated that the mean LOS was significantly shortened in the ERAS-treated patients (by 3.20–9.30 days), as shown in .Citation18,Citation19,Citation23,Citation24 Another RCT reported by Lai et alCitation20 emphasized that the length of postoperative stay in ERAS group (6.17±2.91 days) was significantly shorter than that in control group (8.08±2.21 days; p=0.013), although no significant difference was observed in the LOS between these two groups (p=0.072), as shown in .
The remaining two RCTs enrolling 209 European patients reported the LOS as a median with its range.Citation21,Citation22 Both of them showed no difference in the median LOS between the ERAS group and the control group, as shown in .
Length of ICU stay
As for the length of ICU stay, we also qualitatively reviewed three available RCTsCitation21–Citation23 since a considerable heterogeneity was revealed (I2=94.7%; p<0.001).
Both the RCTs reporting the length of ICU stay as mean±SDCitation21,Citation23 suggested that the length of ICU stay was significantly shortened in the patients who received an ERAS program (by 0.33–1.0 days). However, in another RCT reported by Muehling et al,Citation22 there was no difference in the median length of ICU stay between the ERAS group and the control group ().
Total hospitalization cost
As reported in three available RCTs,Citation18,Citation20,Citation24 the mean hospitalization cost in ERAS group and control group ranged 15.60–46.46 and 23.60–45.53 thousand Yuan RMB, respectively. We gave up a meta-analysis of these studies because of a significantly high heterogeneity (I2=92.8%; p<0.001).
Two RCTs based on 109 enrolled patients showed significantly lower hospitalization costs in the ERAS group (differed 7.3–8.0 thousand Yuan RMB).Citation18,Citation24 However, there was no significant difference in hospitalization costs between these two groups in another one smaller RCT ().Citation20
Subgroup analysis
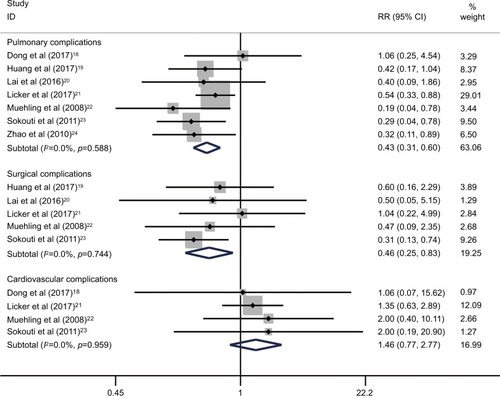
To assess the effects of ERAS programs on postoperative morbidity in detail, we included all seven RCTs in the subgroup of pulmonary complications,Citation18–Citation24 five RCTs in the subgroup of surgical complicationsCitation19–Citation23 and four RCTs in the subgroup of cardiovascular complications.Citation18,Citation21–Citation23
The syntheses of results in all subgroups are summarized in . As shown in , the integrated estimates revealed that both pulmonary complications (RR=0.43; 95% CI=0.31–0.60; p<0.001; I2=0.0%, p=0.59) and surgical complications (RR=0.46; 95% CI=0.25–0.83; p=0.010; I2=0.0%, p=0.74) were significantly decreased in the patients who received an ERAS care. However, no significant improvement was found among the ERAS-treated patients in terms of cardiovascular complications (RR=1.46; 95% CI=0.77–2.77; p=0.25; I2=0.0%, p=0.96), as shown in and .
Figure 4 Subgroup analyses for effects of the ERAS programs on pulmonary, surgical and cardiovascular complications following lung cancer surgery.
Sensitivity analysis
By omitting the individual study sequentially, none of the pooled RRs based on the remaining studies in each group of meta-analysis was out of the estimated range, as shown in the Supplementary materials. No substantial variation was found between adjusted pooled estimates and primary pooled estimates. The strong robustness of our meta-analysis was thus confirmed.
Publication bias
As shown in and the Supplementary materials, these was no significant evidence detected by either Begg’s test or Egger’s test for publication bias within the meta-analyses of postoperative morbidity and mortality. In addition, no publication bias was detected in each subgroup analysis.
Discussion
Summary of evidence
The concept of ERAS was formerly known as the “fast-track surgery”. Since it was firstly introduced by Kehlet and MogensenCitation9 in 1999, a package of ERAS protocols has been proposed by different institutions according to their medical care conditions. In recent years, the ERAS programs have been advocated and utilized in a wide range of surgical specialties, including the orthopedics, urologic and cardiothoracic surgery, although the majority of evidence regarding the benefits of ERAS originated from the colorectal surgery.Citation7,Citation11 Currently, there are up to ~20 elements of perioperative care recognized from the relevant investigations, although the number of these elements varies across different ERAS programs.Citation25
The first consensus ERAS guideline, responding to the need in colorectal surgery, was proposed by the European Society of Clinical Nutrition and Metabolism in 2005.Citation26 Since then, similar guidelines applied to other major procedures have been published for further optimizing the perioperative care of surgical patients.Citation25 With such a background, the ERAS Society, an international nonprofit academic and multidisciplinary organization, was formed in London in 2010, with objectives to improve the perioperative care and enhance the implementation of best practices worldwide.Citation35
However, there is no consensus guideline for thoracic surgery until now. As Nicholson et alCitation12 suggested, a great majority of evidence regarding the application of ERAS in lung surgery was from observational studies, resulting in high bias risks caused from confounding factors. The latest systematic review reported by Fiore et alCitation7 confirmed this viewpoint, since only five observational studies and one RCT were available. The authors concluded that the clinical significance of ERAS programs in lung resections remained controversial because of the scarcity of conclusive evidence.
Key results and interpretations
Given the above reviews, we considered that it might be necessary to make appropriate adjustments to the eligibility criteria. According to prior evidence-based reviews,Citation12,Citation27,Citation28 we modified the following items of eligibility criteria and then utilized them in this systematic review.
First, only RCTs were included in order to guarantee strong evidence intensity and eliminate the methodological restrictions. Second, the target diseases were limited to operable lung cancers to avoid bias risks from different disease patterns. Third, an ERAS program that incorporated more than four care elements covering two or all of three phases of perioperative care was included, as suggested by Nicholson et alCitation12 in their large-scale meta-analysis of 38 RCTs. Finally, we removed the language limitation and allowed non-English articles to be included, although they had to get a Jadad score ≥3 points.
To our knowledge, our study was the first systematic review with meta-analysis to explore the beneficial effects of ERAS programs for patients undergoing lung cancer surgery based on the outcome data from RCTs. This evidence-based review covered all prescribed contents for a standardized PRISMA report. On the basis of modified eligibility criteria, seven RCTs with a mean Jadad score of 3.6 were included in our review.Citation18–Citation24 When pooling the data regarding postoperative morbidity and mortality, low to moderate levels of heterogeneity were observed between studies, indicating the need for a meta-analysis that integrated the appropriate statistics to draw global conclusions.Citation3,Citation29
Therefore, by applying meta-analyses of these RCTs, we discovered that the overall morbidity rate in patients receiving an ERAS program was significantly lower than that in patients managed with conventional care. Besides, the rates of pulmonary and surgical complications were both significantly decreased in ERAS-treated patients. However, no significant effect of ERAS programs was observed on either in-hospital mortality or cardiovascular complications. Sensitivity analyses and publication bias tests were also performed to confirm the stability and accuracy of these pooled estimates. We speculated that the following three possible reasons might be considered when trying to explain this phenomenon.
First, preoperative short-term intensive pulmonary physiotherapy and aerobic training were used as ERAS interventions in three RCTs enrolling 53.3% of all enrolled patients (n=259), in order to improve the functional capacity and cardiopulmonary intolerance before surgery.Citation19–Citation21 Previous evidence had shown that moderate-to-intensive rehabilitation programs could effectively bring physical benefits to surgical patients and prevent the development of pulmonary complications following lung cancer surgery.Citation30 However, their effects on postoperative cardiovascular complications were still controversial. Most of the current studies showed no significant decrease of cardiovascular events after pulmonary resections combined with chest physiotherapy, which was supported by our pooled estimates.Citation21,Citation30
Second, several perioperative care elements implanted in the ERAS programs had the potential to affect the incidence of complications induced by surgical procedures. For instance, poor pulmonary fitness in the high-risk patients, a principal risk factor for alveolar air leaks, could be significantly improved by intensive physiotherapy and physical exercise before surgery.Citation30,Citation31 Thus, patients receiving such interventions were expected to have a lower rate of prolonged air leak. Another example was the formation of bronchial fistula, which could be largely limited by using prophylactic antibiotics and sustainable corticosteroids, because the underlying inflammations might predispose to bronchial stump insufficiency.Citation32 In addition, a “fissureless” technique dealing with the densely fused interlobar fissures intraoperatively in an ERAS program could also significantly decrease the incidences of prolonged air leak and pneumothorax.Citation20 However, all of above care elements appeared not to affect the risk of cardiovascular morbidity directly.
Third, there were only eight deaths in our systematic review, with a mortality rate of 1.6%.Citation19,Citation21–Citation23 Three of them underwent an ERAS program and the other five cases received a traditional pathway, indicating little difference in the in-hospital mortality between groups. We suspected that limited sample size might cause a large decline in the precision of effect size estimations and the analytical power. Thus, the safety of ERAS programs should be further verified by more large-scale multicenter RCTs in the future.
For the secondary outcomes of interest, we gave up summarizing the continuous data regarding the LOS, length of ICU stay and hospitalization cost by quantitative methods due to considerable heterogeneity between relevant studies (I2≥75%). This was not only an issue worth being discussed and interpreted, but also a major limitation that should be acknowledged in our study. First of all, the number of individual ERAS elements differed largely across the RCTs, resulting in a dramatically increased heterogeneity. Most of the ERAS programs were developed based upon the principles from similar works in colorectal and gastric surgical arenas.Citation12,Citation27,Citation28 Without a contemporary consensus on the ERAS interventions for lung cancer surgery, there was a large variation, while many care elements overlapped among the current ERAS programs. On the other hand, the practical execution of some common ERAS interventions might not be standardized. The intensity of preoperative physiotherapy, the usage and dosage of drugs, surgical techniques and the time to remove various catheters were almost dependent on the clinicians’ experiences and institutional policies rather than the consensus ERAS guidelines. This might be another source of heterogeneity.
By applying a qualitative summary, we found that four eligible RCTs enrolling 47.1% of all enrolled patients (n=229) showed a significantly shortened LOS in the ERAS-treated patients.Citation18,Citation19,Citation23,Citation24 Another single-center RCT conducted by Lai et alCitation20 based on 48 high-risk patients also reported that the length of postoperative stay of ERAS group was significantly shorter than that of control group (p=0.013). The remaining two RCTs, including the currently largest RCT (n=151) and the earliest RCT (in 2008), reported a similar LOS between the ERAS group and the control group.Citation21,Citation22 However, the length of ICU stay was significantly shortened in the ERAS-treated patients in the largest RCT (p<0.001).Citation21 Similar results were also reported in a smaller RCT enrolling 60 patients (p=0.017).Citation23
The cost-effectiveness analyses performed in the studies included also demonstrated an economic benefit of the ERAS programs for lung cancer surgery. Among three available RCTs, a significant reduction of hospitalization costs in the ERAS-treated patients was reported in two studies based on a total of 109 patients.Citation18,Citation24 On the contrary, only one smaller RCT (n=48) showed slightly higher hospitalization costs in the ERAS group than that in the control group.Citation20 These three RCTs covering a cost-effectiveness analysis were all conducted among Chinese populations.Citation18,Citation20,Citation24 The majority of current evidence supported that the implementation of an ERAS program for elective lung resections was significantly associated with lower hospitalization costs, which was in favor of the findings from a recent Canadian prospective study recruiting 133 patients.Citation33 In that study, Paci et alCitation33 found that a multidisciplinary ERAS program could contribute to improve the clinical outcomes and save the hospitalization and societal costs. However, in an earlier Chinese prospective study based on 142 high-risk patients, Gao et alCitation34 found that the ERAS group patients had slightly higher hospitalization costs than those of the control group patients. Unfortunately, we were unable to further assess the influence of huge variations in socioeconomic levels and medical care between the eastern and western worlds.
Generalizability
Altogether, this study could be regarded as a substantial update to the recent review reported by Fiore et al.Citation7 Our review optimized the eligibility criteria, and we performed a formal analysis of statistical heterogeneity based on more than six included studies.Citation7,Citation15 Our findings demonstrated the favorable effects of ERAS programs on preventing postoperative complications, shortening the LOS and ICU duration and saving the hospitalization costs based on outcome data from RCTs. These evidence-based results would help to popularize the ERAS protocols for lung cancer surgery and improve the perioperative outcomes.
Limitations
Several limitations must be taken into account regarding the interpretations in our review. First, the number of ERAS care elements varied across the seven included RCTs, resulting in an inherent heterogeneity when evaluating the primary and secondary outcomes. Second, the practical execution of ERAS elements might almost depend on the clinicians’ experiences. Third, our sample size of 486 participants was generally smaller than that in other meta-analyses, which might limit the analytical power. Fourth, some important outcomes, such as the quality of life and readmission rate, were not analyzed due to the lack of supporting data, resulting in a decrease in the integrity of this systematic review. Finally, approximately half of the enrolled patients were from China. Therefore, our findings should be judiciously considered in the clinical settings of other nations.
Conclusion
In conclusion, this systematic review of RCTs demonstrates that the implementation of an ERAS program in lung cancer surgery can significantly decrease the overall morbidity, pulmonary complications, surgical complications and hospitalization costs and shorten the LOS and length of ICU stay, without compromising patients’ safety. A worldwide consensus guideline is urgently required to standardize the ERAS protocols for elective lung resections in the future.
Acknowledgments
Special thanks to the Institution of Medical Statistics, West China School of Public Health, Sichuan University, Chengdu, China for its contributions to statistical analysis. This study was supported by the Foundation of Science and Technology support plan Department of Sichuan Province (2015SZ0158).
Disclosure
The authors report no conflicts of interest in this work.
References
- VázquezSCasalJAfonso AfonsoFJEGFR testing and clinical management of advanced NSCLC: a Galician Lung Cancer Group study (GGCP 048-10)Cancer Manag Res20168112026893581
- JoshiMRizviSMBelaniCPAfatinib for the treatment of metastatic non-small cell lung cancerCancer Manag Res20157758225733926
- LiSWangZHuangJSystematic review of prognostic roles of body mass index for patients undergoing lung cancer surgery: does the ‘obesity paradox’ really exist?Eur J Cardiothorac Surg201751581782828040677
- GhanemSEl BitarSHossriSWeerasingheCAtallahJPWhat we know about surgical therapy in early-stage non-small-cell lung cancer: a guide for the medical oncologistCancer Manag Res2017926727828740431
- ThomasPABerbisJFalcozPEEPITHOR GroupNational perioperative outcomes of pulmonary lobectomy for cancer: the influence of nutritional statusEur J Cardiothorac Surg201445465265924062351
- LiSZhouKWangMLinRFanJCheGDegree of pulmonary fissure completeness can predict postoperative cardiopulmonary complications and length of hospital stay in patients undergoing video-assisted thoracoscopic lobectomy for early-stage lung cancerInteract CardioVasc Thorac Surg Epub2017811
- FioreJFJrBejjaniJConradKSystematic review of the influence of enhanced recovery pathways in elective lung resectionJ Thorac Cardiovasc Surg2016151370815.e626553460
- KehletHWilmoreDWMultimodal strategies to improve surgical outcomeAm J Surg2002183663064112095591
- KehletHMogensenTHospital stay of 2 days after open sigmoidectomy with a multimodal rehabilitation programmeBr J Surg199986222723010100792
- KehletHWilmoreDWEvidence-based surgical care and the evolution of fast-track surgeryAnn Surg2008248218919818650627
- SchatzCEnhanced recovery in a minimally invasive thoracic surgery programAORN J2015102548249226514705
- NicholsonALoweMCParkerJLewisSRAldersonPSmithAFSystematic review and meta-analysis of enhanced recovery programmes in surgical patientsBr J Surg2014101317218824469618
- MoherDLiberatiATetzlaffJPreferred reporting items for systematic reviews and meta-analyses: the PRISMA statementBMJ2009339b253519622551
- OlivoSAMacedoLGGadottiICFuentesJStantonTMageeDJScales to assess the quality of randomized controlled trials: a systematic reviewPhys Ther200888215617518073267
- HigginsJPTGreenSCochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]The Cochrane Collaboration2011 Available from: www.cochrane-handbook.org
- ThomasPABerbisJBasteJMEPITHOR groupPneumonectomy for lung cancer: contemporary national early morbidity and mortality outcomesJ Thorac Cardiovasc Surg20151491738225439468
- BeggCBMazumdarMOperating characteristics of a rank correlation test for publication biasBiometrics1994504108811017786990
- DongQZhangKCaoSCuiJFast-track surgery versus conventional perioperative management of lung cancer-associated pneumonectomy: a randomized controlled clinical trialWorld J Surg Oncol20171512028086896
- HuangJLaiYZhouXShort-term high-intensity rehabilitation in radically treated lung cancer: a three-armed randomized controlled trialJ Thorac Dis2017971919192928839990
- LaiYSuJYangMZhouKCheGImpact and effect of preoperative short-term pulmonary rehabilitation training on lung cancer patients with mild to moderate chronic obstructive pulmonary disease: a randomized trialChin J Lung Cancer20161911746753 Chinese
- LickerMKarenovicsWDiaperJShort-term preoperative h-intensity interval training in patients awaiting lung cancer surgery: a randomized controlled trialJ Thorac Oncol201712232333327771425
- MuehlingBMHalterGLSchelzigHReduction of postoperative pulmonary complications after lung surgery using a fast track clinical pathwayEur J Cardiothorac Surg200834117418018490173
- SokoutiMAghdamBAGolzariSEMoghadaszadehMA comparative study of postoperative pulmonary complications using fast track regimen and conservative analgesic treatment: a randomized clinical trialTanaffos20111031219
- ZhaoGHuangYChenXResearch on fast track surgery application in lung cancer surgeryChin J Lung Cancer2010132102106 Chinese
- SteenhagenEEnhanced recovery after surgery: it’s time to change practice!Nutr Clin Pract2016311182926703956
- FearonKCLjungqvistOVon MeyenfeldtMEnhanced recovery after surgery: a consensus review of clinical care for patients undergoing colonic resectionClin Nutr200524346647715896435
- BeamishAJChanDSBlakePAKarranALewisWGSystematic review and meta-analysis of enhanced recovery programmes in gastric cancer surgeryInt J Surg201519465426004350
- GrecoMCaprettiGBerettaLGemmaMPecorelliNBragaMEnhanced recovery program in colorectal surgery: a meta-analysis of randomized controlled trialsWorld J Surg20143861531154124368573
- ZengZHChenJFLiYXZhangRXiaoLFMengXYInduction regimens for transplant-eligible patients with newly diagnosed multiple myeloma: a network meta-analysis of randomized controlled trialsCancer Manag Res2017928729828744159
- Sebio GarciaRYáñez BrageMIGiménez MoolhuyzenEGrangerCLDenehyLFunctional and postoperative outcomes after preoperative exercise training in patients with lung cancer: a systematic review and meta-analysisInteract Cardiovasc Thorac Surg201623348649727226400
- SinghalSFerrarisVABridgesCRManagement of alveolar air leaks after pulmonary resectionAnn Thorac Surg20108941327133520338378
- LiSJZhouXDHuangJLiuJTianLCheGWA systematic review and meta-analysis-does chronic obstructive pulmonary disease predispose to bronchopleural fistula formation in patients undergoing lung cancer surgery?J Thorac Dis2016871625163827499951
- PaciPMadaniALeeLEconomic impact of an enhanced recovery pathway for lung resectionAnn Thorac Surg2017104395095728778343
- GaoKYuPMSuJHCardiopulmonary exercise testing screening and pre-operative pulmonary rehabilitation reduce postoperative complications and improve fast-track recovery after lung cancer surgery: a study for 342 casesThorac Cancer20156444344926273399
- ERAS Society [homepage] www.erassociety.orgAccessed August 1, 2017