
Abstract
Purpose
This study aimed to evaluate the short- and long-term outcomes of laparoscopic hepatectomy (LH) for colorectal liver metastases (CRLM) in elderly patients.
Patients and methods
Between January 2009 and January 2016, LH was performed for 241 consecutive patients who were ≥60 years old and had CRLM. Based on their age at the LH, the patients were divided into an elderly group (≥70 years old, 78 patients) and a middle-aged group (60–69 years old, 163 patients). The short- and long-term outcomes were compared between the two groups.
Results
Compared to the middle-aged group, the elderly group had higher values for Charlson comorbidity index, proportion of preoperative chemotherapy, and American Society of Anesthesiologists score. No other significant differences were observed in the preoperative characteristics. The elderly group had a higher conversion rate, compared to the middle-aged group, although no significant differences were observed in the surgical procedures, surgical times, intraoperative blood losses, numbers and severities of postoperative 90-day complications, postoperative 90-day mortality rates, pathology results, and other short-term outcomes. Long-term follow-up revealed similar rates of recurrence, disease-free survival, and overall survival in the two groups. Multivariable analysis revealed that age did not independently predict overall survival or disease-free survival.
Conclusion
Similar short- and long-term outcomes were observed after LH for CRLM in elderly and middle-aged patients. Thus, advanced age is not a contraindication for LH treatment in this setting.
Introduction
The westernization of Chinese lifestyle has created recent trends toward decreased physical activity, increased life expectancy, and an increased incidence of colorectal cancer.Citation1 Studies have demonstrated that approximately one-half of colorectal cancers develop liver metastases, and surgical resection is the primary treatment for colorectal liver metastases (CRLM).Citation2–Citation4 A large number of studies have revealed that the 5-year overall survival rate is 30%–60% among patients who undergo radical resection for CRLM, and good long-term survival can be achieved using open hepatectomy for CRLM.Citation5–Citation7 However, ~70% of patients with CRLM are ≥65 years old when they seek treatment, and elderly patients may be less able to tolerate hepatectomy (versus younger patients), which has led some surgeons to reject hepatectomy for elderly patients.Citation5–Citation8
The first reported laparoscopic hepatectomy (LH) was performed in 1992,Citation9 and a growing number of reports have described LH treatment for CRLM.Citation10–Citation15 Compared to open hepatectomy, LH for CRLM leads to lesser intraoperative blood loss, shorter hospital stays, similar or lower incidences of complications, and similar long-term outcomes.Citation10–Citation15 However, the previous studies have not included large numbers of elderly patients, and only a few English reports have described LH treatment for CRLM.Citation16–Citation19 Furthermore, there is a lack of studies comparing short- and long-term outcomes of LH treatment between elderly and middle-aged patients with CRLM. Therefore, the present study aimed to compare the short- and long-term outcomes of LH treatment among elderly and middle-aged patients with CRLM.
Patients and methods
This study complied with the Declaration of Helsinki rules. This retrospective research was approved by the Ethics Committee of First Hospital, JiLin University. The need for informed consent from all patients was waived because this was a retrospective study. All data had no personal identifiers and were kept confidential.
Between January 2009 and January 2016, 241 consecutive patients underwent LH treatment for CRLM and were considered eligible for this retrospective study. The inclusion criteria were as follows: 1) the patient was undergoing their first hepatectomy, 2) the patient had undergone radical resection of colorectal cancer, and 3) complete clinical and follow-up data were available for the patient. The exclusion criteria were as follows: 1) repeat hepatectomy and 2) palliative hepatectomy. Based on their age at the LH, the patients were divided into an elderly group (≥70 years old, 78 patients) and a middle-aged group (60–69 years old, 163 patients). The location, number, diameter, and operability of liver metastatic lesions were preoperatively confirmed in all patients using tumor biomarkers, abdominal computed tomography or magnetic resonance imaging, and other examinations. Positron emission tomography–computed tomography was performed as needed. Lung function tests, electrocardiography, echocardiography, and other examinations were performed to determine the patients’ preoperative cardiopulmonary function. All patients were operated using the totally laparoscopic technique, and intraoperative ultrasonography was performed in all cases. The LH was performed according to a previous report.Citation19 All LHs were carried out by the surgeon Dr Zhenhua Kang. Before this study, he had successfully completed 50 LH surgeries.
The Clavien–Dindo criteria were used to classify the severity of postoperative 90-day complications. Minor complications were defined as grades I–II and major complications as grades III–V. Postoperative 90-day mortality was defined as any death from oncological or non-oncological causes within 90 days after surgery.
After the patients were discharged, follow-ups were performed at outpatient clinics, the patient’s house, community health service centers, and other locations. The follow-ups were performed every 3 months during the first year after surgery, every 4 months during the second year, every 6 months during the third year, and annually thereafter. Patients were referred for in-hospital treatment if tumor recurrence was suspected at any time. The follow-up rate was 100%, as all patients lived near our hospital, and the last follow-up was performed on May 31, 2017.
All the statistical analyses were performed using SPSS, Version 14.0 (SPSS Inc., Chicago, IL, USA). Normally distributed variables were analyzed by Student’s t-tests and presented as mean and SD. Non-normally distributed variables were analyzed by Mann–Whitney U test and presented as medians and ranges. Differences between semiquantitative results were analyzed by Mann–Whitney U tests. Differences between qualitative results were analyzed by chi-square or Fisher’s exact tests, as appropriate. Survival rates were analyzed by the Kaplan–Meier method, and differences between the two groups were analyzed by log-rank test. Multivariable Cox regression analysis was performed to identify the factors predictive of poor disease-free survival and overall survival by using both forward and backward stepwise selection. Explanatory variables with univariate P values ≤0.100 were included in the multivariable analysis. The results are reported as hazard ratios with 95% CIs. A level of 5% was set as the criterion for statistical significance.
Results
The patients’ general preoperative characteristics are shown in . Compared to the middle-aged group, the elderly group had significantly higher values for Charlson comorbidity index, proportion of preoperative chemotherapy, and the American Society of Anesthesiologists score. No other significant differences were observed in the other preoperative characteristics (e.g., gender, body mass index, TNM stage, pre-LH carcinoembryonic antigen levels, and location of liver metastases).
Table 1 Baseline characteristics of the two groups
The patients’ short-term prognoses are shown in . Both groups underwent similar surgical procedures, with most patients undergoing wedge resection or sectionectomy and a few patients undergoing left lateral sectionectomy. No significant inter-group differences were observed in the surgical times, intraoperative blood losses, intraoperative and postoperative blood transfusion rates, or incidences and severities of postoperative complications. The elderly group had a higher rate of conversion to open hepatectomy, and conversion in both groups was primarily related to bleeding. There were no intraoperative deaths in either group, although one patient in the elderly group died within 90 days because of liver failure and one patient in the middle-aged group died after 2 months because of metastasis to the central nervous system. Both groups had similar pathology results.
Table 2 Short-term outcomes of the two groups
The median follow-ups for the elderly and middle-aged groups were 31 and 34 months, respectively, and this difference was not statistically significant (P=0.387). During the follow-ups, 32 patients in the elderly group died because of recurrence (n=29), ischemic stroke (n=1), hemorrhagic stroke (n=1), and sudden cardiac death (n=1), as shown in . Fifty-three patients in the middle-aged group died because of recurrence (n=48) and non-cancer-related diseases (n=5). There were no significant inter-group differences in the recurrence locations, median time to recurrence, or other factors ().
Table 3 The follow-up data of the two groups
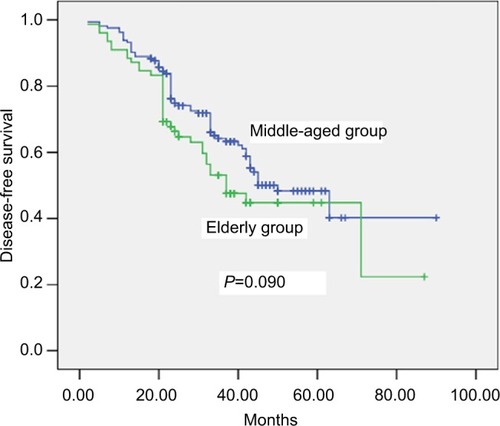
The 5-year overall survival rates for the elderly and middle-aged groups were 52% and 59%, respectively, and this difference was not statistically significant (P=0.139; ). Multivariable analyses revealed that TNM stage, disease-free interval, and number of metastases independently predicted overall survival ( and ). The 5-year disease-free survival rates for the elderly and middle-aged groups were 45% and 49%, respectively, and this difference was not statistically significant (P=0.090; ). Multivariable analyses revealed that disease-free interval and preoperative carcinoembryonic antigen levels independently predicted disease-free survival ( and ). Age did not independently predict overall or disease-free survival.
Table 4 Univariate Kaplan–Meier analysis of overall survival
Table 5 Cox proportional hazards model for overall survival
Table 6 Univariate Kaplan–Meier analysis of disease-free survival
Table 7 Cox proportional hazards model for disease-free survival
Figure 1 Comparison of overall survival rate between elderly and middle-aged groups (P=0.139).
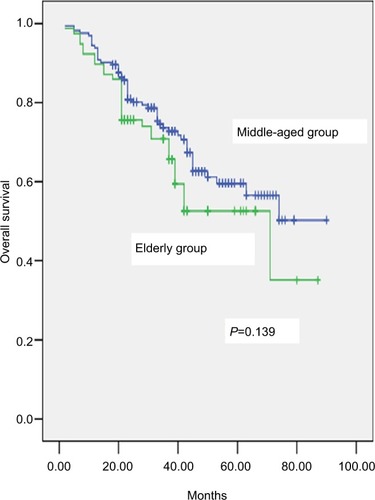
Figure 2 Comparison of disease-free survival rates between elderly and middle-aged groups (P=0.090).
Discussion
Increasing life expectancy is leading to a rise in the surgical treatment of elderly patients with CRLM, and surgical resection of liver metastases is considered safe for these patients. However, elderly individuals have more comorbidities and less cardiopulmonary functional reserve, compared to younger patients, and elderly patients experience relatively high rates of postoperative complications and mortality.Citation5–Citation8 These factors explain the relatively small proportion of elderly patients in the present study, as well as their higher Charlson comorbidity index and American Society of Anesthesiologists score, compared to middle-aged patients. Interestingly, the patients and their families expressed concern regarding the surgery and a desire for non-surgical CRLM treatments.
The liver receives an abundant supply of blood from the hepatic artery and portal vein, and bleeding is common during open hepatectomy.Citation20–Citation23 However, it is difficult to control any bleeding and replicate some of the open procedures during LH, which can necessitate conversion to open hepatectomy in up to 12% of cases.Citation10–Citation15 In the present study, the conversion rate among elderly patients was higher than that among middle-aged patients (7% versus 1%, respectively), and bleeding was the overwhelming reason for conversion to open hepatectomy. These findings may be related to the deterioration of physiological mechanisms (e.g., vascular elasticity) and coagulation function in elderly patients, which makes it difficult to control intraoperative bleeding.Citation24–Citation26 Thus, only open hepatectomy can ensure patient safety. Although we did not detect any obvious differences in the preoperative platelet counts and coagulation test results, coagulation is a very complicated process that may not be completely described using clinical platelet counts and coagulation tests.
The current guidelines categorize LH based on the extent and complexity as minor hepatectomy, major hepatectomy, and difficult hepatectomy.Citation27 Only minor hepatectomy was performed in the present study, and previous reports have also confirmed that LH generally involves minor hepatectomy,Citation5–Citation8 with a few reports showing major and difficult hepatectomy. This is likely because major and difficult hepatectomies are inherently difficult to perform using the open approach, and the laparoscopic approach further complicates the surgery. Thus, patients who require major or difficult hepatectomy for CRLM may not be able to benefit from the advantages of laparoscopic surgery. Nevertheless, recent reports have indicated that laparoscopic major and difficult hepatectomy is safe and feasible,Citation28–Citation31 and our hospital began performing laparoscopic major and difficult hepatectomy in June 2016, based on the accumulated experience with LH. We hope to generate additional data to examine the utility of laparoscopic major and difficult hepatectomy in future studies.
Relatively few elderly patients with CRLM undergo LH because of concerns among surgeons that elderly patients may not be able to tolerate pneumoperitoneum, which can lead to higher intraperitoneal pressure and CO2 retention in the blood. These factors can theoretically lead to cardiopulmonary complications, although none of the elderly patients in the present study experienced severe cardiopulmonary complications. Three elderly patients experienced minor lung infections, based on the Clavien–Dindo criteria,Citation32–Citation35 although they recovered fully after treatment using intravenous antibiotics.
Previous studies have revealed 5-year overall survival rates of 48%–61% and 5-year disease-free survival rates of 43%–58% among elderly patients who underwent hepatectomy for CRLM.Citation36–Citation38 We observed similar outcomes among our elderly patients, and their outcomes were comparable to those of the middle-aged patients. The predominant cause of death among elderly patients was tumor recurrence, with relatively few deaths caused by non-oncological diseases. Therefore, LH appears to be beneficial when indicated for elderly patients with CRLM and to provide good long-term survival, compared to the outcomes for middle-aged patients. Moreover, elderly patients with CRLM have an extremely poor prognosis after receiving non-surgical treatments.
The present study has two important limitations. First, the retrospective design is associated with known risks of bias, and a prospective randomized controlled trial is needed to confirm that LH is safe and effective for elderly patients with CRLM. Second, we only examined data from a single center with a small sample size, and it is possible that our findings may not generalize to other centers and/or patient groups. The fact that the study failed to find statistical significance between the two groups in survival may be due to the small sample size.
Conclusion
The present study results indicate that LH was not associated with elevated rates of postoperative complications or mortality among elderly patients with CRLM, and that their long-term outcomes were comparable to those of middle-aged patients. Therefore, advanced age is not a contraindication for LH treatment of CRLM.
Acknowledgments
We sincerely thank our colleagues who participated in this research.
Disclosure
The authors report no conflicts of interest in this work.
References
- ChenWZhengRZuoTZengHZhangSHeJNational cancer incidence and mortality in China, 2012Chin J Cancer Res201628111127041922
- HeinrichSLangHLiver metastases from colorectal cancer: technique of liver resectionJ Surg Oncol2013107657958422566374
- AkgülÖÇetinkayaEErsözŞTezMRole of surgery in colorectal cancer liver metastasesWorld J Gastroenterol201420206113612224876733
- McNallySJParksRWSurgery for colorectal liver metastasesDig Surg2013304–633734724051581
- MatiasMCasa-NovaMFariaMPrognostic factors after liver resection for colorectal liver metastasisActa Med Port201528335736926421789
- FrankelTLD’AngelicaMIHepatic resection for colorectal metastasesJ Surg Oncol201410912724318723
- ParauATodorNVladLDeterminants of survival after liver resection for metastatic colorectal carcinomaJ BUON2015201687725778299
- MenthaGTerrazSAndresATosoCRubbia-BrandtLMajnoPOperative management of colorectal liver metastasesSemin Liver Dis201333262272
- ReichHMcGlynnFDeCaprioJBudinRLaparoscopic excision of benign liver lesionsObstet Gynecol1991785 Pt 29569581833688
- LuoLZouHYaoYHuangXLaparoscopic versus open hepatectomy for hepatocellular carcinoma: short- and long-term outcomes comparisonInt J Clin Exp Med2015810187721877826770494
- JiangXLiuLZhangQLaparoscopic versus open hepatectomy for hepatocellular carcinoma: long-term outcomesJ BUON201621113514127061541
- EmileSHEvolution and clinical relevance of different staging systems for colorectal cancerMinim Invasive Surg Oncol2017124352
- WuDWuWLiYLaparoscopic hepatectomy for colorectal liver metastases located in all segments of the liverJ BUON201722243744428534367
- SahaySJFazioFCettaFChouialHLykoudisPMFusaiGLaparoscopic left lateral hepatectomy for colorectal metastasis is the standard of careJ BUON20152041048105326416055
- KazaryanAMMarangosIPRøsokBILaparoscopic resection of colorectal liver metastases: surgical and long-term oncologic outcomeAnn Surg201025261005101221107111
- AllardMACunhaASGayetBColorectal Liver Metastases-French Study GroupEarly and long-term oncological outcomes after laparoscopic resection for colorectal liver metastases: a propensity score-based analysisAnn Surg2015262579480226583668
- ZengYTianMLaparoscopic versus open hepatectomy for elderly patients with liver metastases from colorectal cancerJ BUON20162151146115227837616
- SpampinatoMGArvanitakisMPuleoFTotally laparoscopic liver resections for primary and metastatic cancer in the elderly: safety, feasibility and short-term outcomesSurg Endosc20132761881188623247741
- NomiTFuksDKawaguchiYMalFNakajimaYGayetBLaparoscopic major hepatectomy for colorectal liver metastases in elderly patients: a single-center, case-matched studySurg Endosc20152961368137525149638
- HuntingtonJTRoyallNASchmidtCRMinimizing blood loss during hepatectomy: a literature reviewJ Surg Oncol20141092818824449171
- EmileSHAdvances in laparoscopic surgery for colorectal cancer: fluorescence-guided surgeryMinim Invasive Surg Oncol2017125365
- EmileSHLaparoscopic intersphincteric resection for low rectal cancer: technique, oncologic, and functional outcomesMinim Invasive Surg Oncol2017127484
- XieMZhuJHeXLiver metastasis from colorectal cancer in the elderly: is surgery justified?Dig Dis Sci201560123525353526173502
- ChenJBaiTZhangYThe safety and efficacy of laparoscopic and open hepatectomy in hepatocellular carcinoma patients with liver cirrhosis: a systematic reviewInt J Clin Exp Med2015811206792068926884991
- GoussousNShmelevACunninghamSCMinimally invasive surgery for gallbladder cancerMinim Invasive Surg Oncol201713103116
- BuellJFCherquiDGellerDAWorld Consensus Conference on Laparoscopic SurgeryThe international position on laparoscopic liver surgery: the Louisville Statement, 2008Ann Surg2009250582583019916210
- CoelhoFFKrugerJAFonsecaGMLaparoscopic liver resection: experience based guidelinesWorld J Gastrointest Surg20168152626843910
- YoonYSHanHSChoJYAhnKSTotal laparoscopic liver resection for hepatocellular carcinoma located in all segments of the liverSurg Endosc20102471630163720035349
- XiangLXiaoLLiJChenJFanYZhengSSafety and feasibility of laparoscopic hepatectomy for hepatocellular carcinoma in the posterosuperior liver segmentsWorld J Surg20153951202120925585525
- XiaoLXiangLJLiJWChenJFanYDZhengSGLaparoscopic versus open liver resection for hepatocellular carcinoma in posterosuperior segmentsSurg Endosc201529102994300125899815
- LeeWHanHSYoonYSComparison of laparoscopic liver resection for hepatocellular carcinoma located in the posterosuperior segments or anterolateral segments: a case-matched analysisSurgery201616051219122627353634
- XiaoHXiePZhouKClavien-Dindo classification and risk factors of gastrectomy-related complications: an analysis of 1049 patientsInt J Clin Exp Med2015858262826826221408
- ClavienPABarkunJde OliveiraMLThe Clavien-Dindo classification of surgical complications: five-year experienceAnn Surg2009250218719619638912
- WangWShaoMZhangRLong-term outcomes after laparoscopic versus open surgery for elderly patients with rectal cancerInt J Clin Exp Med2016991816018167
- WuDLiYYangZFengXLvZCaiGLaparoscopic versus open gastrectomy for gastric carcinoma in elderly patients: a pair-matched studyInt J Clin Exp Med20169234653472
- WangCLuoWFuZSunMSiHGuoDA propensity score-matched case-control comparative study of laparoscopic and open liver resection for hepatocellular carcinomaJ BUON201722493694128952210
- NaganoYNojiriKMatsuoKThe impact of advanced age on hepatic resection of colorectal liver metastasesJ Am Coll Surg2005201451151616183488
- FiguerasJRamosELópez-BenSSurgical treatment of liver metastases from colorectal carcinoma in elderly patients. When is it worthwhile?Clin Transl Oncol20079639240017594954