
Abstract
Background
This population-based study evaluated the overall (OS) and cancer-specific survival (CSS) benefit from palliative radiotherapy (RT) in patients with unresectable intrahepatic cholangiocarcinoma (ICC).
Methods
We queried The Surveillance, Epidemiology, and End Results (SEER) database for the patients with unresectable ICC diagnosed from 1973 to 2013. Propensity score–matched analysis was performed to reduce the impact of the selection bias between the palliative RT group and the nonpalliative RT group. Kaplan–Meier survival curves were used to estimate the survival outcome before and after propensity score matching. OS and CSS were compared between patients with and without palliative RT using univariate and multivariate Cox proportional hazards regression analyses.
Results
A total of 4,027 of 15,803 patients diagnosed with ICC were included in this study. Of those, 847 (21%) patients underwent palliative RT, whereas 3,180 (79%) did not. In the unmatched population, patients treated with palliative RT had improved OS and CSS relative to those treated without palliative RT (adjusted HR =0.9065, 95% CI =0.8360–0.982, P=0.01735) and CSS (adjusted HR =0.8874, 95% CI =0.8160–0.9652, P=0.00532). After propensity score matching, palliative RT was associated with a significantly improved OS (adjusted HR =0.8544, 95% CI =0.7722–0.9453, P=0.00228) and CSS (adjusted HR =0.8563, 95% CI =0.7711–0.9509, P=0.0037).
Conclusion
Palliative RT seems to improve the prognosis of patients with unresectable ICC.
Background
Intrahepatic cholangiocarcinoma (ICC) is a relatively rare gastrointestinal malignancy that originates from the epithelial lining of the intrahepatic biliary tree. Despite a rising incidence, existing data to inform optimal treatment are limited due to the rarity of the disease.Citation1–Citation3
Radical surgical resection is generally considered the only curative treatment for ICC. However, the majority of patients are unresectable due to advanced disease at the time of diagnosis.Citation4,Citation5 For patients with inoperable disease, the overall prognosis remains poor, with the median survival being 7–12 months.Citation6 The results of the Advanced Biliary Cancer Trial demonstrated that cisplatin plus gemcitabine treatment can improve the overall survival (OS) in locally advanced and metastatic biliary tumors.Citation7 Cisplatin plus gemcitabine treatment is generally considered the standard frontline therapy for locally advanced biliary tumors, which is often followed by transarterial chemoembolization, thermal ablation, and external radiotherapy (RT).
Previous studies have suggested that RT can improve the OS in patients with unresectable ICC.Citation6,Citation8–Citation10 On the other hand, some papers reported that RT has no impact on OS rate of patients with unresectable ICC.Citation11 The role of radiation in the management of unresectable ICC remains an important unanswered question. Therefore, we evaluated the OS and cancer-specific survival (CSS) benefit from palliative RT in patients with unresectable ICC.
Methods
The present study was performed using the Surveillance, Epidemiology, and End Results (SEER) 18-Registry (1973–2013 dataset), which represented approximately 28% of cancer cases in the USA. This database documented clinical tumor characteristics including diagnosis, race, sex, marital status, tumor-node-metastasis stage, type of cancer and survival time, and cause-of-death information.
The third edition of the International Classification of Diseases for Oncology (ICD-O-3) was used for the identifi-cation of patients with ICC. Patients with ICC were selected by ICD-O-3 site codes C22.1 or C22.0. The ICD-O-3 histological codes of 8010, 8020, 8040, 8070, 8041, 8140, 8144, 8160, 8161, 8162, 8163, 8260, 8310, 8480, 8490, and 8560 were used to identify ICC.Citation12 We excluded patients without histological diagnostic confirmation or who were diagnosed at autopsy. We also excluded patients with a survival time of <3 months, those with other SEER reportable malignancies if ICC was not the first one, those undergoing tumor resection, patients with distant metastases, and those lacking information about RT.
Propensity score matching
Because of unbalanced baseline characteristics, retrospective studies unavoidably suffer from selection bias. This bias may influence comparison of the survival outcomes between patients treated with and without palliative RT. Propensity score–matching analysis, which is defined as a statistical method to adjust for potential baseline confounding variables, was performed to reduce the impact of the selection bias. A logistic regression model was established for calculating the propensity scores.Citation13 Palliative RT status was considered as the dependent variable, while baseline characteristics such as age at diagnosis, gender, race, tumor grade, marital status, tumor size, and cause of death were considered as predefined covariates. The patients who underwent palliative RT were matched with those who did not undergo this procedure on the basis of a greedy algorithm of nearest neighbor matching at a 1:1 fixed ratio.Citation14
Statistical analysis
The primary outcome was OS; the secondary outcome was CSS. Categorical patient characteristics were compared using the χ2 test. Kaplan–Meier survival curves were used to estimate the survival outcome before and after propensity score matching. The survival difference according to the receipt of palliative RT was compared using a log-rank test. Cox proportional hazard regression models were used to obtain unadjusted and adjusted HR and 95% CI for survival in univariate analysis and multivariate analyses. Sensitivity analysis was performed using random survival forest methodology by repeating computations after substituting unknown data.Citation15 Statistical analyses were performed using R3.2.3 for window (http://www.R-project.org). Propensity score analysis was performed using the MatchIT package.Citation16 Random survival forest survival analysis was performed using the “randomForestSRC” package. A 2-sided P<0.05 was considered statistically significant.
Ethics approval and consent to participate
This study was partly based on the publicly available SEER database, and we received permission of The National Cancer Institute to access the database for the purposes of research only. As this research did not include interaction with humans or use personal identifying information, informed consent was not required.
Results
Patients’ characteristics
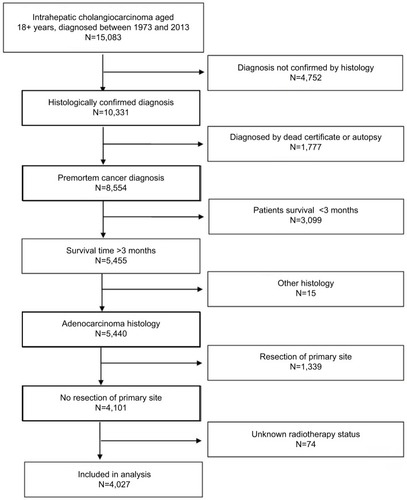
For the present investigation, 4,027 of 15,803 patients diagnosed with ICC were included. Of those, 847 (21%) patients underwent palliative RT, whereas 3,180 (79%) did not. summarizes clinicopathologic characteristics between the 2 groups. The median age was 64 years (range 20–97). depicts the detailed flow chart of patients’ selection for the study cohort.
Table 1 Patient characteristics of the palliative RT and nonpalliative RT groups before and after propensity score matching
Figure 1 Flow chart of patients’ cohort definition.
Survival outcomes in the before matching population
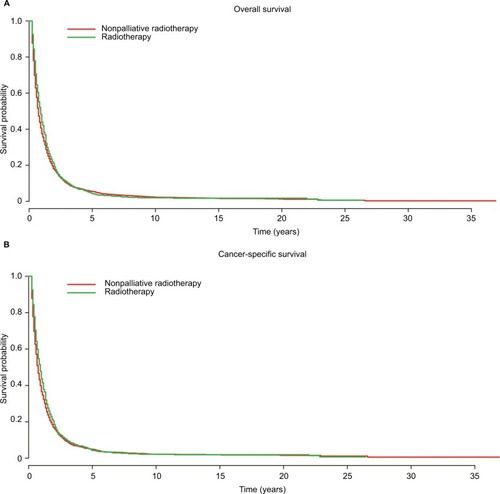
represent Kaplan–Meier curves for OS and CSS survival in patients with and without palliative RT. Patients with palliative RT had a better OS and CSS compared with those not undergoing palliative RT (OS P=0.0138, CSS survival P=0.00453). In univariate analysis, palliative RT was a statistically significant prognostic factor for OS (HR =0.9024, 95% CI =0.832–0.9778, P=0.0122) () and CSS (HR =0.885, 95% CI =0.814–0.9619, P=0.00406) (), respectively. In multivariable Cox proportional analyses, palliative RT was a statistically significant had a significantly protective effect on OS (HR =0.9065, 95% CI =0.8360–0.982, P=0.01735) () and CSS (HR =0.8874, 95% CI =0.8160–0.9652, P=0.00532) ().
Table 2 Prognostic factors for overall survival before and after propensity score–matched analysis
Table 3 Prognostic factors for cancer-specific survival before and after propensity score–matched analysis
Figure 2 Kaplan–Meier analysis of (A) overall and (B) cancer-specific survival of the palliative radiotherapy and nonpalliative radiotherapy groups before propensity score matching.
Adjusting for patient characteristics using propensity score matching
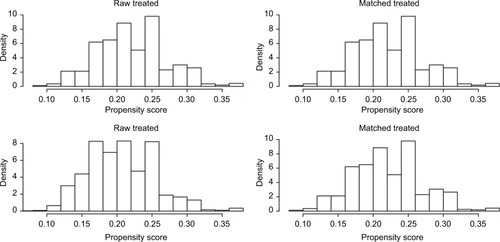
Propensity score–matching analysis was performed to adjust for potential baseline confounding variables including age, marital status, and tumor size. shows the details of the variables before and after propensity score matching, noting that the impact of potential selection bias was reduced. The propensity score for patients in the palliative RT group was 0.22±0.06 compared with 0.21±0.05 for patients in the nonpalliative RT group. After propensity score matching, the score for patients in the palliative RT group was 0.22±0.06, and it was 0.22±0.06 for patients in the nonpalliative RT group. represents the distribution of the propensity scores of the 2 groups before and after propensity score matching.
Figure 3 Distribution of propensity score before and after propensity matching procedure.
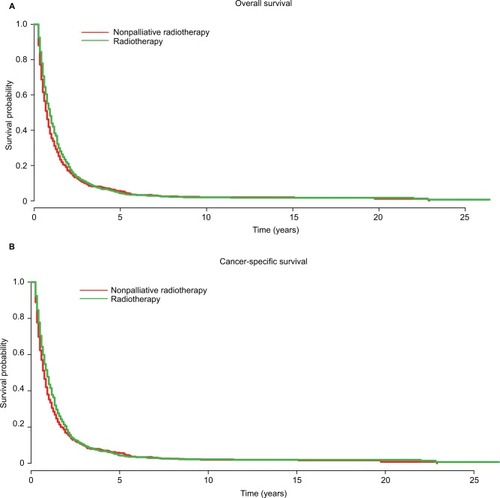
represent Kaplan–Meier curves for OS and CSS after propensity score matching. Patients with palliative RT had a better OS and CSS compared with those not undergoing palliative RT (OS P=0.00864, CSS P=0.0149). In univariate analysis, palliative RT was a statistically significant prognostic factor for OS (HR =0.8725, 95% CI =0.788–0.964, P=0.00791) () and CSS (HR =0.8771, 95% CI =0.7902–0.9737, P=0.0139) () in the matched population. In multivariable Cox analysis, palliative RT was statistically significant and had a significantly protective effect on OS (HR =0.8544, 95% CI =0.7722–0.9453, P=0.00228) () and CSS (HR =0.8563, 95% CI =0.7711–0.9509, P=0.0037) () in the matched population.
Figure 4 Kaplan–Meier analysis of (A) overall and (B) cancer-specific survival of the palliative radiotherapy and nonpalliative radiotherapy groups after propensity score matching.
Sensitivity analysis
The overall study results were not affected by the imputation of unknown data using random survival forest methodology. In sensitivity analysis, palliative RT remained a statistically significant protective factor for OS (HR =0.9114, 95% CI =0.840–0.989, P=0.02596) and CSS (HR =0.8976, 95% CI =0.8245–0.9771, P=0.01260), respectively.
Discussion
Our results suggested that palliative RT may improve OS and CSS of patients with unresectable ICC. Both univariate and multivariable Cox analysis after propensity score matching demonstrated a better prognosis in the patients treated with palliative RT regardless of patient characteristics.
This study is the first analysis based on SEER using propensity score matching to evaluate the effect of palliative RT for unresectable ICC. Similar to our findings, other retrospective studies found palliative RT to have a better prognosis in the patients treated with palliative RT. In a retrospective study series of 84 patients with unresectable ICC, Chen et alCitation9 reported a more favorable prognosis treated with external beam RT. In another SEER-based study, Shinohara et alCitation6 reported a significantly reduced overall mortality in the patients treated with palliative RT. There were only 396 patients who received RT. The median survival time was 7 months as against 3 months for patients not treated with RT (P<0.01). The largest study reported an analysis of the National Cancer Database in 1,636 patients, including 374 patients who received chemotherapy with radiation.Citation10 The authors found the survival benefit from the addition of radiation to chemotherapy using the propensity score–matching method. However, the National Cancer Database, which is a hospital-based registry, more likely suffers from selection bias than a population-based study.Citation17 Conversely, we used SEER which is a population-based database.
On the other hand, a retrospective study using the nationwide SEER registry found no difference in prognosis between unresectable ICC patients who did undergo palliative RT and those who did not.Citation11 However, our results demonstrated a better prognosis in the patients treated with palliative RT. We speculated that this discrepancy might be caused only by selection bias arising from an unbalanced distribution of the baseline characteristics between the 2 groups.
The present study is an analysis of SEER data in 4,027 patients, including 847 patients who underwent palliative RT. To the best of our knowledge, this study is the largest report on patients with unresectable ICC who were treated with palliative RT. To minimize the potential selection bias, propensity score matching was carried out in this population-based investigation. By propensity score matching, any imbalance between the 2 groups could be avoided, imbalance that generated effects similar to random allocation. In addition, we performed sen sitivity analysis by imputation of unknown data using random survival forest methodology. Because our results are consistent, it provides stronger evidence that palliative RT may improve OS and CSS of patients with unresectable ICC.
Many investigators have begun to investigate different strategies of palliative RT for patients with unresectable ICC. Stereotactic body radiation therapy (SBRT) and high-dose hypofractionated proton therapy had been reported to be effective and reasonably safe therapies for unresectable ICC.Citation18,Citation19 Tse et alCitation20 published a Phase I trial of individualized 6-fraction SBRT for unresectable primary liver tumors including 10 patients with unresectable ICC. The median survival of ICC patients was 15 months in their study. Another group also reported a series of 32 patients with unresectable intrahepatic or hilar cholangiocarcinoma, who were treated with SBRT.Citation21 The median OS was 17 months and Grade III toxicity was 12%. Thus, the authors concluded that SBRT is an effective and reasonably safe local therapy. More recently, the Massachusetts General Hospital has reported encouraging outcomes using high-dose hypofractionated proton therapy. The findings of this multi-institutional Phase II Study were impressive, because the local control rate was 94.8% and the OS rate at 2 years was 46.5%.Citation22
There are several limitations to the current study that must be acknowledged. First, information on chemotherapy was not available in the SEER registry. Therefore, it is impossible to making any adjustment for the use of chemotherapy. Because chemotherapy was associated with survival, we could not confirm the survival benefit of palliative RT without considering chemotherapy. Moreover, information on physical condition, liver function, and complications, which are important factors influencing patient survival, were not available in the SEER registry. Second, information about palliative RT, such as the dose, fractionation-specific data, and treatment-related toxicity, could not be ascertained in the SEER registry. Third, because the current study is nonrandomized, it unavoidably suffers from selection bias or from the impact of unknown variables that cannot be reduced in the SEER registry. Finally, OS and CSS were the primary and secondary outcomes in this study. Information such as quality of life and local control are important measures, which were unavailable in the SEER registry. Despite these limitations, this is the first large-scale study to evaluate the effect of palliative RT for unresectable ICC. Although some unknown con-founders were unadjusted, it appears to be impossible that the large beneficial effects of palliative RT are due solely to unknown confounders. The large sample size and the population-based nature reflect the real-world outcome for patients with unresectable ICC.
Conclusion
The present study indicates the potential favorable impact of palliative RT on survival outcome in patients with unresectable ICC. Prospective randomized controlled trials are needed to verify the conclusion of this study.
Data sharing statement
Any request of data and material may be sent to the corresponding author.
Acknowledgments
The authors acknowledge the efforts of the SEER Program tumor registries in the creation of the SEER database.
Disclosure
The authors report no conflicts of interest in this work.
References
- PatelTIncreasing incidence and mortality of primary intrahepatic cholangiocarcinoma in the United StatesHepatology2001336v13531357
- ShaibYHDavilaJAMcGlynnKEl-SeragHBRising incidence of intrahepatic cholangiocarcinoma in the United States: a true increase?J Hepatol200440347247715123362
- McGlynnKATaroneREEl-SeragHBA comparison of trends in the incidence of hepatocellular carcinoma and intrahepatic cholangiocarcinoma in the United StatesCancer Epidemiol Biomarkers Prev20061561198120316775181
- EndoIGonenMYoppACIntrahepatic cholangiocarcinoma: rising frequency, improved survival, and determinants of outcome after resectionAnn Surg20082481849618580211
- ChouFFSheen-ChenSMChenYSSurgical treatment of cholangiocarcinomaHepatogastroenterology1997447607659222685
- ShinoharaETMitraNGuoMMetzJMRadiation therapy is associated with improved survival in the adjuvant and definitive treatment of intrahepatic cholangiocarcinomaInt J Radiat Oncol Biol Phys2008721495150118472359
- ValleJWasanHPalmerDHCisplatin plus gemcitabine versus gemcitabine for biliary tract cancerN Engl J Med20103621273128120375404
- TaoRKrishnanSBhosalePRAblative radiotherapy doses lead to a substantial prolongation of survival in patients with inoperable intrahepatic cholangiocarcinoma: a retrospective dose response analysisJ Clin Oncol201634321922626503201
- ChenYXZengZCTangZYDetermining the role of external beam radiotherapy in unresectable intrahepatic cholangiocarcinoma: a retrospective analysis of 84 patientsBMC Cancer20101049220840777
- JacksonMWAminiAJonesBLRusthovenCGSchefterTEGoodmanKATreatment selection and survival outcomes with and without radiation for unresectable, localized intrahepatic cholangiocarcinomaCancer J201622423724227441741
- AminiNEjazASpolveratoGKimYHermanJMPawlikTMTemporal trends in liver-directed therapy of patients with intrahepatic cholangiocarcinoma in the United States: a population-based analysisJ Surg Oncol2014110216317024676600
- FritzAPercyCJackAInternational Classification of Diseases for OncologyGeneva, SwitzerlandWorld Health Organization2000
- JoffeMMRosenbaumPRInvited commentary: propensity scoresAm J Epidemiol1999150432733310453808
- AustinPCAn introduction to propensity score methods for reducing the effects of confounding in observational studiesMultivariate Behav Res201146339942421818162
- IshwaranHKogalurUBBlackstoneEHLauerMSRandom survival forestsAnn Appl Stat200823841860
- HoDEImaiKKingGStuartEAMatching as nonparametric preprocessing for reducing model dependence in parametric causal inferencePolit Anal200715199236
- van der VeldenJvan LindertACGimbrereCHOostingHHeintzAPEpidemiologic data on vulvar cancer: comparison of hospital with population-based dataGynecol Oncol19966233793838812536
- GoodmanKAWiegnerEAMaturenKEDose-escalation study of single-fraction stereotactic body radiotherapy for liver malignanciesInt J Radiat Oncol Biol Phys201078248649320350791
- BarneyBMOlivierKRMillerRCHaddockMGClinical outcomes and toxicity using stereotactic body radiotherapy (SBRT) for advanced cholangiocarcinomaRadiat Oncol201276722553982
- TseRVHawkinsMLockwoodGPhase I study of individualized stereotactic body radiotherapy for hepatocellular carcinoma and intrahepatic cholangiocarcinomaJ Clin Oncol200826465766418172187
- MahadevanADagogluNManciasJStereotactic body radiotherapy (SBRT) for intrahepatic and hilar cholangiocarcinomaJ Cancer20156111099110426516357
- HongTSWoJYYeapBYMulti-institutional phase II study of highdose hypofractionated proton beam therapy in patients with localized, unresectable hepatocellular carcinoma and intrahepatic cholangiocarcinomaJ Clin Oncol201634546046826668346