
Abstract
Background
Ribociclib (RIBO) and palbociclib (PALBO), combined with letrozole (LET), have been evaluated as treatments for hormone receptor-positive, human epidermal growth factor receptor 2-negative advanced breast cancer in separate Phase III randomized controlled trials (RCTs), but not head-to-head. Population differences can lead to biased results by classical indirect treatment comparison (ITC). Matching-adjusted indirect comparison (MAIC) aims to correct these differences. We compared RIBO and PALBO in hormone receptor-positive/human epidermal growth factor receptor 2-negative advanced breast cancer using MAIC.
Methods
Patient-level data were available for RIBO (MONALEESA-2), while only published summary data were available for PALBO (PALOMA-2). Weights were assigned to MONALEESA-2 patient data such that mean baseline characteristics matched those reported for PALOMA-2; the resulting matched cohort was used in comparisons. Limited by the results reported in PALOMA-2, progression-free survival (PFS) was the primary comparison. Cox regression models were used to calculate adjusted hazard ratios (HRs) for PFS, before indirect treatment comparison (ITC) was performed with 95% confidence intervals. An exploratory analysis was performed similarly for overall survival using earlier PALBO data (PALOMA-1). Grade 3/4 adverse events were also compared.
Results
Racial characteristics, prior chemotherapy setting, and the extent of metastasis were the most imbalanced baseline characteristics. The unadjusted PFS HRs were 0.556 (0.429, 0.721) for RIBO+LET versus LET alone and 0.580 (0.460, 0.720) for PALBO+LET versus LET alone. MAIC adjustment resulted in an HR of 0.524 (0.406, 0.676) for RIBO+LET versus LET. PFS ITC using unadjusted trial data produced an HR of 0.959 (0.681, 1.350) for RIBO versus PALBO, or 0.904 (0.644, 1.268) with MAIC. Unadjusted overall survival HR of RIBO versus PALBO was 0.918 (0.492, 1.710); while exploratory MAIC was 0.839 (0.440, 1.598). ITC of grade 3/4 adverse events yielded a risk ratio of 0.806 (0.604, 1.076).
Conclusion
MAIC was performed for RIBO and PALBO in the absence of a head-to-head trial: though not statistically significant, the results favored RIBO.
Introduction
Breast cancer is the most prevalent cancer in women and is the second deadliest after lung cancer. An estimated 246,660 new cases of breast cancer were diagnosed in the USA in 2016 and an estimated 40,450 breast cancer deaths occurred. Approximately 12.4% of women will develop breast cancer over the course of their lifetime.Citation1 While breast cancer is detected at an early stage 90% of the time, many cases will progress to advanced or metastatic disease.Citation2,Citation3 Once metastases are detected, the median survival rate is 18–24 months and fewer than 5% of patients are expected to be alive and disease-free after 5 years.Citation4 The most favorable prognosis is conferred to 74% of the patient population who have tumors that express hormonal receptors (HR+) and do not express human epidermal growth factor receptor 2 (HER2 [HER2−]). These tumors are more responsive to therapy than HR− tumors and less aggressive than HER2+ tumors.Citation5
Postmenopausal women with HR+/HER2− advanced breast cancer (ABC) typically receive hormonal therapy (HT) as initial treatment.Citation6 The agents used include selective estrogen receptor antagonists tamoxifen and fulvestrant and aromatase inhibitors: exemestane, letrozole, and anastrozole.Citation7 Considering patients with advanced HR+ tumors, only 20%–40% respond to therapy initially and the majority will ultimately develop resistance.Citation8,Citation9 Subsequently, HT may be used in combination with targeted therapy. Therapies that target pathways involved in resistance can restore or increase sensitivity to HT.Citation6 Everolimus and palbociclib (PALBO) are currently approved by the US Food and Drug Administration for the treatment for HR+/HER2− ABC in combination with aromatase inhibitors. In first- and second-line randomized controlled trials (RCTs), both agents have been shown to improve progression-free survival (PFS) compared with HT alone.Citation10,Citation11
Ribociclib (RIBO), a cyclin-dependent kinase (CDK) 4/6 inhibitor similar to PALBO, was evaluated in a Phase III clinical trial as first-line treatment for postmenopausal women with HR+/HER2− ABC. In the recent MONALEESA-2 trial, patients with HR+ HER2− ABC who received RIBO with letrozole (LET) had better PFS than those who received LET alone: median PFS was not reached in the RIBO arm at data cut-off whereas median PFS was 14.7 months in the placebo arm.Citation12 Patients in the RIBO and LET group experienced a 44% improvement in the risk of progression compared with those who received LET alone.Citation12
Head-to-head comparison is an important tool to demonstrate treatment value and to aid decision-making. Accounting for the time required to perform a randomized trial, new agents may become available before they are compared with the relevant alternatives. Indirect treatment comparison (ITC), the statistical comparison of separate trials with like comparator groups, can provide timely evidence of comparative effectiveness. Guidelines and reviews of the methodologies now support the use of ITC, which is increasingly common.Citation13–Citation15 However, there is an important consideration associated with this method: ITC compares non-randomized treatment groups. Classical ITC can, therefore, generate biased results when trials of variable design with different patient populations are compared. Recent refinements of the ITC methodology have focused on accounting for trial dissimilarities.
Matching-adjusted indirect comparison (MAIC) corrects for baseline differences in patient populations, allowing for indirect comparison with limited bias when patient level data are available for only 1 study. Where individual patient data are available, baseline characteristics can be adjusted and reweighted to match summary statistics for comparator population. The adjusted treatment outcomes may then be compared. This approach has provided strong comparative evidence in the absence of head-to-head studies in various disease settings.Citation14,Citation16–Citation19 RIBO and PALBO are CDK4/6 inhibitors demonstrated to be effective in HR+/HER2− ABC and so their comparison is clinically and economically relevant. As their corresponding trials used the same comparator – LET – and individual patient data were available for RIBO, MAIC was considered an appropriate methodology to examine comparative effectiveness.
Materials and methods
A systematic literature search following the guidelines published by the Cochrane CollaborationCitation22 and the UK’s National Institute for Health and Clinical Excellence (NICE)Citation13 was conducted and identified 2 relevant Phase III RCTs and 1 relevant Phase II RCT: MONALEESA-2Citation12, RIBO and LET (CLEE011A2301 Clinical Study Report, Novartis Data on File); PALOMA-2Citation20, PALBO and LET; and PALOMA-1Citation10, PALBO and LET.Citation10
MONALEESA-2 and PALOMA-2 both reported PFS as the primary endpoint. MONALEESA-2 reported overall survival (OS) as the secondary endpoint at the most recent cut-off (January 4, 2017). PALOMA-2 did not report mature results for OS, whereas the Phase II PALOMA-1 trial did. Hence, this analysis compared PFS results from MONA-LEESA-2 and PALOMA-2 and OS results from MONA-LEESA-2 and PALOMA-1.
ITC and MAIC statistical methods
To ensure the comparability of the trials, transitivity assumptions were tested according to the NICE Decision Support Unit (DSU) Technical Support Document 18 using a Population Average Treatment Effect (PATE) test.Citation13
Classical frequentist ITC was performed using the Bucher (1997)Citation23 method with 95% confidence intervals (CIs). Treatment with LET and placebo was used as the common comparator to evaluate the efficacy of RIBO and LET versus PALBO and LET.
The adjusted baseline characteristics, selected based on feasibility and availability, were: age, race, region, Eastern Cooperative Oncology Group (ECOG) performance status, disease stage at diagnosis, disease-free interval (binary variable <12 months, i.e., de novo), current extent of disease using metastatic sites (visceral versus non-visceral binary variable), number of metastatic sites, and chemotherapy setting at baseline. Variable matching for PFS was performed: as patient level data were available for only the MONALEESA-2 trial, these data were adjusted and reweighted to match PALOMA-2 statistical data. First, the MONALEESA-2 trial population was modified to align its inclusion/exclusion criteria with the PALOMA-2 population. Some patients in the RIBO total intention-to-treat (ITT) dataset were excluded from this analysis based on PALOMA-2 exclusion criteria. In the second step of the MAIC analysis, the RIBO population data were reweighted such that the means/percentages of patient characteristics common to both datasets matched comparator data.
The weights were created by performing a logistic regression on the patient-level RIBO data that included an extra observation representing the comparator’s data (i.e., a patient to whom the mean/percentage summarized values for the comparator’s patient characteristics were attributed). The predicted values (or propensity score) that resulted from the logistic regression were used to weight the RIBO trial data (i.e., adjusted hazard ratios (HRs) were calculated using weighted Cox regression models).
Matching variables for OS using PALOMA-1 followed, although PALOMA-1 was a Phase II study and had slightly different baseline characteristics than PALOMA-2. The number of baseline characteristics reported in the publication was limited and matching could only be performed using a small number of variables. The following variables were available for matching OS in PALOMA-1 versus MONALEESA-2: median age, ECOG. Considering the matching limitations and the low number of OS events that have occurred to date in MONALEESA-2, OS is presented as an exploratory analysis.
Matching-adjusted ITC was performed according to NICE DSU guidelines.Citation13 Analyses were conducted using Stata (Version 13.1; StataCorp LP, College Station, TX, USA). Direct comparison of HRs for RIBO and PALBO was conducted and CIs were measured on a log scale.
Results
Design of the compared studies
The designs of MONALEESA-2 and PALOMA-2 are described in .
Table 1 Comparison of MONALEESA-2, and PALOMA-1 and -2
MONALEESA-2 and PALOMA-2 had different followup periods (~28 versus 23 months). However, the length of the follow-up period is unlikely to affect time-to-event endpoints, such as the HRs for PFS and OS, and was, therefore, not deemed to be a significant transitivity issue. The inclusion criteria for MONALEESA-2 and PALOMA-2/PALOMA-1 were deemed similar and the dosage of LET was identical. However, different stratification variables were used. MONA-LEESA-2 trial population was stratified according to the presence of lung and/or liver metastasis, while PALOMA-2 and PALOMA-1 populations were stratified by disease site and disease-free interval.
Patient characteristics
The designs of the MONALEESA-2 and PALOMA-2/PALOMA-1 trials were similar and were, therefore, considered suitable for comparison. Of the MONALEESA-2 ITT population, 334 patients were treated with RIBO and LET and 334 patients were treated with placebo and LET. In the PALOMA-2 trial, 444 patients were treated with PALBO and LET and 222 were assigned to the placebo and LET group. In the PALOMA-1 trial, 84 patients were treated with PALBO and LET and 81 were assigned to the LET group. Patient baseline characteristics are presented in .
Table 2 Patient characteristics
Site of metastasis, adjuvant chemotherapy, patient age, and primary tumor size are strong prognostic factors in metastatic breast cancer.Citation21 As there was limited deviation in the PATE test, it was concluded that the data were robust enough to perform both an ITC (unmatched) and an MAIC with very little transitivity concern.
PFS
Patient characteristics common to both populations were matched, and the RIBO population was adjusted. presents the levels of baseline characteristics (variables) in each population. The MONALEESA-2 population characteristics are also presented after adjustment to match PALOMA-2.
Table 3 Patient characteristics before and after adjustment (in “levels”)
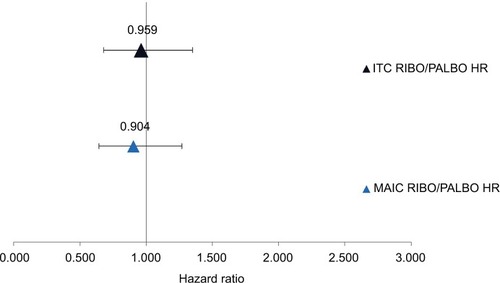
Median PFS was relatively consistent for the LET and placebo groups, with limited deviation from transitivity that would be potentially corrected by ITC and matching. Compared with LET and placebo, the unadjusted PFS HRs were 0.556 (0.429; 0.721) for RIBO and LET and 0.580 (0.460; 0.720) for PALBO and LET. MAIC with the PALOMA-2 population produced a PFS HR of 0.524 (0.407; 0.676) for RIBO and placebo. The unadjusted HR for RIBO versus PALBO was 0.959 (0.681; 1.350) while MAIC produced an HR of 0.904 (0.644; 1.268). depicts these results.
Figure 1 Progression-free survival for RIBO versus PALBO with and without matching adjustment.
Notes: HR <1 favors RIBO, >1 favors PALBO.
Abbreviations: HR, hazard ratio; ITC, indirect treatment comparison; MAIC, matching-adjusted indirect treatment comparison; PALBO, palbociclib; RIBO, ribociclib.
Regarding the statistical fitting of the matching, the estimate had a relatively small R-square value for this type of regression: a pseudo R-square of 0.0251 (prob >χ2=1). Akaike information criterion (AIC) and Bayesian information criterion (BIC) statistics are valuable when comparing models. In this case, the AIC and BIC were 44.58 and 111.78 respectively, which indicates a moderate fit. The relatively large number of matching variables explains the difference in AIC and BIC, which could suggest overmatching. The MONALEESA-2 population was reduced by about 30% in each arm to fit the PALOMA-2. Compared with the ITT population, the effective sample size was 66% for RIBO and 71% for placebo (postexclusion sample sizes were 68% and 73%, respectively), indicating moderate fit.
OS
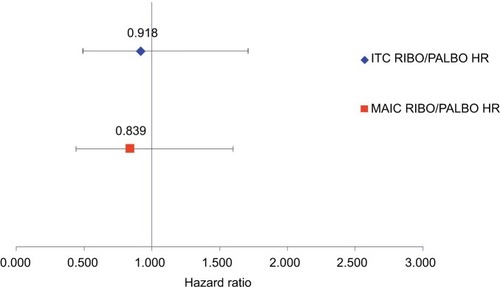
Exploratory unadjusted and adjusted comparisons of OS were performed. As OS data from PALOMA-2 were unavailable, data for PALBO were obtained from the Phase II PALOMA-1 trial. Compared with LET and placebo, the unadjusted OS HRs were 0.746 (0.517; 1.078) for RIBO and LET and 0.813 (0.492; 1.345) for PALBO and LET. MAIC with the PALOMA-1 population produced an OS HR of 0.682 (0.456; 1.021) for RIBO and placebo. The unadjusted HR for RIBO versus PALBO was 0.918 (0.492; 1.710) while MAIC produced an HR of 0.839 (0.440; 1.598). The HR results of this analysis are presented in .
Figure 2 Overall survival for RIBO versus PALBO with and without matching adjustment.
Notes: HR <1 favors RIBO, >1 favors PALBO.
Abbreviations: HR, hazard ratio; ITC, indirect treatment comparison; MAIC, matching-adjusted indirect treatment comparison; PALBO, palbociclib; RIBO, ribociclib.
Grade 3/4 adverse events
The ITC of grade 3/4 adverse events yielded a risk ratio of 0.806 (0.604; 1.076; ), indicating a trend of fewer severe adverse events with RIBO.
Table 4 Indirect treatment comparison of grade 3/4 adverse events
Discussion
An analysis was performed to determine the efficacy of RIBO compared with PALBO for the treatment of HR+/HER2− ABC. This analysis compared PFS and OS in Phase II/III trials of RIBO or PALBO and LET treatment with and without matching adjustment.
In MONALEESA-2, RIBO plus LET was shown to improve PFS versus LET alone.Citation12 The MONALEESA-2 PFS HR for RIBO and LET treatment versus LET alone decreased following matching to the PALOMA-2 trial population data: an HR of 0.556 (0.429; 0.721) became 0.524 (0.406; 0.676). RIBO, therefore, demonstrated improved results in the PALOMA-2 context compared with the MONALEESA-2 context. Upon comparison by classical ITC, RIBO and PALBO were ultimately similar: an HR of 0.959 (0.681; 1.35) for PFS. However, following MAIC, the HR for RIBO compared with PALBO was 0.904 (0.644; 1.268). The unadjusted OS HR of 0.918 (0.517; 1.078) using PALOMA-1 improved to 0.839 (0.440; 1.598) upon exploratory MAIC. Considering comparable populations, RIBO fared better than PALBO. Although not statistically significant, these important results demonstrate that if RIBO and PALBO were compared directly, RIBO may have proved the superior agent.
When assessing therapies in breast cancer, and other diseases with relatively lengthy courses, PFS is a highly relevant outcome. PFS is measured before OS becomes apparent and provides an indication of a disease’s behavior during treatment. PFS has implications for OS and may serve as a proxy for OS in the absence of complete data. MONALEESA-2 is ongoing and the limited number of OS events that have occurred to date would not be expected to accurately represent the total population. No data have been reported for PALOMA-2 OS. Both trials used PFS as the primary outcome measure and, as such, it is the most robust point of comparison for RIBO and PALBO.
In MAIC, patients in 1 population are selected according to their baseline characteristics to replicate a comparator population; this process can be said to break randomization. The implicated variables were not necessarily pre-specified as randomization variables. Simultaneously, a selection bias may result when some baseline characteristics are omitted due to availability. Of additional concern, sample size is reduced during MAIC, which can create a multiplicity bias. Finally, the addition of many variables may result in over-adjustment. Although in this analysis, the statistical fitting and testing performed indicated a moderate fit and, therefore, a limited likelihood of bias, classical and MAIC results proved relatively similar, indicating strong convergence in our findings.
The indirect comparison of RIBO with PALBO, with matching adjustment, predicted how these agents would perform under the same conditions. In our analysis, MAIC suggested 1 of 2 agents that appeared similar by ITC could be the superior choice. We demonstrate, in the absence of a head-to-head clinical trial, that RIBO could compete with or improve upon PALBO results.
Acknowledgments
Parts of this study were featured in a poster presented at the 2017 European Society for Medical Oncology Congress; the abstract is published and is available in the Annals of Oncology (2017) 28 (suppl_5): v74-v108. 10.1093/annonc/mdx365. This study was sponsored by Novartis.
Author contributions
GT made substantial contributions to the conception and design, analyzed and interpreted the data, and critically revised the article. MD acquired and analyzed the data, and contributed to the drafting and revision of the manuscript. DC, AF, and MM made substantial contributions to conception and design, and critically revised the article for important intellectual content. JH contributed to data interpretation and drafting and revising the article. All authors agree to be accountable for all aspects of the work.
Disclosure
DC and MM are employees of Novartis. The authors report no other conflicts of interest in this work.
References
- SiegelRLMillerKDJemalACancer statistics, 2016CA Cancer J Clin201666173026742998
- Early Breast Cancer Trialists’ Collaborative GEffects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: an overview of the randomised trialsLancet200536594721687171715894097
- ClemonsMDansonSHamiltonTGossPLocoregionally recurrent breast cancer: incidence, risk factors and survivalCancer Treat Rev2001272678211319846
- MartinoMBallestreroAZambelliALong-term survival in patients with metastatic breast cancer receiving intensified chemotherapy and stem cell rescue: data from the Italian registryBone Marrow Transplant201348341441822863724
- Breast Cancer Facts & Figures 2015–2016Society ACAtlanta, GAAmerican Cancer Society, Inc.;2015 Available from: https://www.cancer.org/research/cancer-facts-statistics/breast-cancer-facts-figures.htmlAccessed March 28, 2018
- ReinertTBarriosCHOptimal management of hormone receptor positive metastatic breast cancer in 2016Ther Adv Med Oncol20157630432026557899
- Breast Cancer Treatment (PDQ®)–Health Professional VersionBethesda, MDNational Cancer Institute2017
- JohnstonSRNew strategies in estrogen receptor-positive breast cancerClin Cancer Res20101671979198720332324
- Gonzalez-AnguloAMMorales-VasquezFHortobagyiGNOverview of resistance to systemic therapy in patients with breast cancerAdv Exp Med Biol200760812217993229
- FinnRSCrownJPLangIThe cyclin-dependent kinase 4/6 inhibitor palbociclib in combination with letrozole versus letrozole alone as first-line treatment of oestrogen receptor-positive, HER2−negative, advanced breast cancer (PALOMA-1/TRIO-18): a randomised phase 2 studyLancet Oncol2015161253525524798
- BaselgaJCamponeMPiccartMEverolimus in postmenopausal hormone-receptor-positive advanced breast cancerN Engl J Med2012366652052922149876
- HortobagyiGNStemmerSMBurrisHARibociclib as first-line therapy for hr-positive, advanced breast cancerN Engl J Med2016375181738174827717303
- PhillippDAdesAEDiasSPalmerSAbramsKRWeltonNJNICE DSU technical support document 18: methods for population-adjusted indirect comparisons in submissions to NICEUnit DSSheffield2016
- SignorovitchJESikiricaVErderMHMatching-adjusted indirect comparisons: a new tool for timely comparative effectiveness researchValue Health201215694094722999145
- SuttonAAdesAECooperNAbramsKUse of indirect and mixed treatment comparisons for technology assessmentPharmacoeconom-ics2008269753767
- TremblayGLivingsCCroweLKapetanakisVBriggsADetermination of the most appropriate method for extrapolating overall survival data from a placebo-controlled clinical trial of lenvatinib for progressive, radioiodine-refractory differentiated thyroid cancerClinicoecon Outcomes Res2016832333327418847
- SignorovitchJSwallowEKantorEEverolimus and sunitinib for advanced pancreatic neuroendocrine tumors: a matching-adjusted indirect comparisonExp Hematol Oncol2013213224314093
- SignorovitchJEBettsKAReichmannWMOne-year and long-term molecular response to nilotinib and dasatinib for newly diagnosed chronic myeloid leukemia: a matching-adjusted indirect comparisonCurr Med Res Opin201531231532225356603
- SikiricaVFindlingRLSignorovitchJComparative efficacy of guanfacine extended release versus atomoxetine for the treatment of attention-deficit/hyperactivity disorder in children and adolescents: applying matching-adjusted indirect comparison methodologyCNS Drugs2013271194395323975660
- FinnRSMartinMRugoHSPalbociclib and letrozole in advanced breast cancerN Engl J Med2016375201925193627959613
- LargillierRFerreroJMDoyenJPrognostic factors in 1038 women with metastatic breast cancerAnn Oncol200819122012201918641006
- HigginsJPTGreenSCochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]The Cochrane Collaboration2011 Available from http://handbook.cochrane.orgAccessed MArch 28 2018
- BucherHCGuyattGHGriffithLEWalterSDThe results of direct and indirect treatment comparisons in meta-analysis of randomized controlled trialsJ Clin Epidemiol19975066836919250266