
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Background
To evaluate and compare the efficacy and safety of stereotactic body radiation therapy (SBRT) plus induction chemotherapy and SBRT plus adjuvant therapy.
Methods
Patients with radiographically resectable, biopsy-proven pancreatic cancer were enrolled. Data were prospectively collected from 2012 to 2016. Cox proportional hazards regression was used to identify factors predictive of survival. Propensity score matching analysis was performed to assess the efficacy of SBRT combined with different timing of chemotherapy.
Results
One hundred patients were enrolled with 48 receiving induction chemotherapy and 52 undergoing adjuvant chemotherapy. The median overall survival (OS) and progression-free survival (PFS) were 17.5 months (95% CI: 15.8–19.2 months) and 13.7 months (95% CI: 12.3–15.1 months), respectively. Patients with adjuvant chemotherapy (P <0.001), CA19-9 response (P <0.001) and BED10 (biological effective dose, α/β = 10) ≥ 60 Gy (P = 0.024) had a longer OS, while the former two correlated with PFS. Patients with more positive factors had a superior OS and PFS. After propensity score matching analysis, there were 23 patients from each group included in the analysis. Longer OS (23.1 months versus 15.6, P <0.001) and PFS (18.0 months versus 11.6 months, P <0.001) were found in patients with adjuvant chemotherapy compared with those with induction chemotherapy.
Conclusion
SBRT was safe and effective in early stage pancreatic cancer. Combined with adjuvant chemotherapy, SBRT could be an alternative for patients with resectable pancreatic cancer but not eligible for surgical resection.
Introduction
Pancreatic cancer has been the fourth leading cause of cancer mortality in the United States with a dismal 5-year survival rate of 7%.Citation1 The latest findings also showed that in contrast to the declining trends for the four major cancers, the mortality of pancreatic cancer continues to increase slightly (by 0.3% per year) in men but has leveled off in women.Citation2 Similar trends were found in China with increasing incidences and cancer deaths.Citation3
Although surgical resection has been confirmed as the only strategy for cure, especially for resectable pancreatic cancer, only 15–20% of the patients were amenable to this curative-intent treatment at the initial diagnosis.Citation4,Citation5 The overall 5-year survival rate of those patients even with R0 resection with or without adjuvant therapy is less than 20%.Citation6–Citation10
However, there was no consensus or clinical trials about optimal multimodality treatment for patients with resectable but medically inoperable pancreatic cancer. Due to the limited employment of targeted therapy and immunotherapy for pancreatic cancer, radiotherapy and chemotherapy may be the alternatives if patients are not candidates for surgery. Given the shortcomings of conventional radiotherapy, stereotactic body radiation therapy (SBRT) has become a promising option due to its precise treatment delivery with sharp dose fall-off within adjacent organs at risk, acceptable toxicity and online image verifications. Also the shorter duration of SBRT compared with conventional radiotherapy could avoid delaying delivery of chemotherapy. Therefore, a complete understanding of the feasibility and tolerability of SBRT for early stage, resectable pancreatic cancer would have profound clinical importance. Furthermore, the factors associated with prognosis might suggest the underlying mechanism by which treatment effects occur.
In this study, we sought to compare the efficacy and safety of SBRT plus induction chemotherapy and SBRT plus adjuvant chemotherapy and identify clinical factors associated with survival in a large cohort of patients with early stage, resectable but medically inoperable pancreatic cancer.
Methods
The institutional review board of Changhai Hospital has approved this study. Individual written informed consent was mandatory before treatment. Data were prospectively collected from 2012–2016. A prospective maintained pancreatic cancer database was used to identify all patients who were not amenable to surgery and received SBRT between January 2012 and December 2016. Treatment decisions were made at the discretion of the institutional multidisciplinary pancreatic cancer board, which generally followed National Comprehensive Cancer Network guidelines. Typically, induction chemotherapy plus SBRT was performed for patients without severe local symptoms. SBRT with adjuvant chemotherapy might be given priority for amelioration of local symptoms.
Eligibility
All patients included in this study had resectable pancreatic cancer. Patients’ medical records were firstly reviewed by surgeons for evaluation of the feasibility of surgical resection. Only when they were medically inoperable or declined operations, subsequent radiotherapy and chemotherapy was taken into consideration.
Patients who had completed induction chemotherapy would receive positron emission tomography-computed tomography (PET-CT) to preclude metastasis. Those with metastasis were excluded from the study and received other treatment based on the multidisciplinary approach. Those without metastasis would receive SBRT thereafter.
Staging
Before treatment, comprehensive clinical and radiographic staging, including abdominal computed tomography (CT) or magnetic resonance imaging (MRI) scan, chest CT, and laboratory studies were required. Additionally, histopathological diagnosis with fine-needle aspiration guided by endoscopic ultrasound was required for all patients before treatment. The most recent results of laboratory studies before initiation of treatment were utilized for analysis. The definition of resectable pancreatic cancer was referred to NCCN guidelines.Citation11
Chemotherapy
Chemotherapy regimens were based on NCCN guidelines and determined by a multidisciplinary program. Due to the high incidence of neurological toxicity of nab-paclitaxel and low tolerance of FOLFIRINOX in Chinese patients, the chemotherapy regimen was gemcitabine plus S-1. Additionally, S-1, the prodrug of 5-fluorouracil comprising of tegafur, gimeracil and oteracil, was an option as the regimen. Previous studies have proven that S-1 was not inferior to gemcitabine in terms of overall survival (OS) rates and progression-free survival (PFS) rates with tolerable effects.Citation12–Citation15 Patients were recommended to receive chemotherapy for 6 months and SBRT was initialized with an interval of 2 to 3 weeks before or after chemotherapy. Intravenous administration of gemcitabine (1000 mg/m2) was initiated on days 1, 8, and 15 during each 4-week cycle, which repeated for 6 cycles. S-1 was orally administered at a dose of 80 mg/m2 for 28 days followed by a 14-day rest, which also continued for 6 cycles.
Follow-up
Patients were evaluated initially every 2 to 3 months within one year after treatment and later every 4 to 6 months with CT or MRI scans, physical examinations and CA19-9 for a planned follow-up of 5 years. Any other examinations prompted by new-onset symptoms or at the physician’s discretions were also used to record events.
Definitions and collection of data
The definition of disease recurrence was based on review of the medical records and imaging studies. A new low density mass or growth of the tumor on CT or MRI consistent with recurrent local, regional, or metastatic disease was considered as such and tumor biopsy was rarely performed.Citation16 Differential diagnosis of tumor necrosis induced by SBRT, which may be mistaken for progression, would be performed by three radiologists based on MRI scan. OS was defined from the initial date of treatment to death. PFS was determined from the initial date of treatment to the date of the first recurrence or death. Adverse effects induced by chemotherapy were evaluated by Common Terminology Criteria for Adverse Events (CTCAE) Version 4.0. Radiation-induced acute toxicities were determined by “Acute radiation morbidity scoring criteria” from Radiation Therapy Oncology Group. While late toxicities were evaluated by “Late radiation morbidity scoring schema” from Radiation Therapy Oncology Group/European Organization for Research and Treatment of Cancer.Citation17
A systemic inflammation response index (SIRI) might correlate with survival of patients with pancreatic cancer.Citation18 The value was calculated as:
PNI = 10 × serum albumin (g/dl) + 0.005 × total lymphocyte count (/mm3). Charlson age-comorbidity index (CACI) was originally designed to classify prognostic comorbidity.Citation21 It was identified that CACI was associated with prognosis of patients with pancreatic cancer.Citation22 Pain was quantified by visual analogue scale (VAS).
The recommended upper limit of normal for CA19-9 is 37 U/mL.Citation23 Additionally, a phase I/II study of nab-paclitaxel + gemcitabine that preceded advanced pancreatic cancer reported a significant correlation between decreases in CA19-9 levels of ≥50% versus <50% from baseline and improved survival.Citation24 Therefore, CA19-9 response was defined as the level of CA19-9 decreased by 50% from baseline levels of ≥74 U/mL. Hence, three CA19-9 groups were formed for univariate analysis: CA19-9 levels ≥74 U/mL with response versus CA19-9 levels ≥74 U/mL with no response (including CA19-9 levels within the normal range before SBRT while increased after SBRT) versus CA19-9 levels <74 U/mL (before SBRT and during follow-up). The nadir value of CA19-9 level during the follow-up was utilized for the estimation of CA19-9 decrease. Additionally, it was demonstrated that CA19-9 level less than 200 U/mL was associated with major response for localized pancreatic cancer treated with preoperative therapy.Citation25 Therefore, the serum level of CA19-9 before SBRT was stratified as: <200 U/mL and ≥200 U/mL.
SBRT technique
The protocol was based on our previous studies.Citation26,Citation27 SBRT was delivered via CyberKnife® (Accuray Incorporated, Sunnyvale, CA, USA), an image-guided frameless stereotactic robotic radiosurgery system. A plain CT and a contrast-enhanced pancreatic parenchymal CT were performed and co-registered for treatment planning and target delineations. Before CT simulations, at least three fiducials were implanted using endoscopic ultrasound or CT guidance. Gross tumor volume (GTV) was delineated as a radiographically evident gross disease by contrast CT. Clinical target volume (CTV) encompassing areas of the potential subclinical disease spread was also designated. In most cases, the CTV equaled GTV. A 2–5 mm expansion margin was included to determine the planning target volume (PTV). When the tumor was adjacent to critical organs, the expansion of PTV outside of CTV in this direction should be avoided. Therefore, the margin expansion was allowed to be non-uniform. At least 90% of PTV should be covered by the prescription dose. Normal tissue constraints were according to the American Association of Physicists in Medicine guidelines in TG-101.Citation28
Propensity score matching
To correct for potential imbalances in treatment assignments, we performed propensity score matching, which decreased the differences between SBRT plus induction chemotherapy and SBRT plus adjuvant chemotherapy. We first built a logistic regression model with treatment modality as the dependent variable and all other variables that could potentially influence its prognostic impact as independent variables.
Statistical analysis
Patient characteristics and demographic data were summarized by descriptive statistics. Quantitative outcomes were compared by chi-square test (Fisher’s exact tests). Next, demographic and clinical factors were investigated for their association with OS and PFS using univariate log-rank comparisons and then multivariate proportional hazards regression model. OS and PFS curves were calculated by the Kaplan–Meier method. Median OS and PFS and 95% CIs were reported. Long-term survival of patients with different treatment options was assessed with propensity score matched analysis. Two-sided P values <0.05 were considered statistically significant. Statistical analyses were performed using SPSS version 22.0 (IBM Corporation, Armonk, NY, USA).
Results
Patient characteristics
A total of 100 patients were identified including 48 patients with induction chemotherapy and 52 receiving adjuvant chemotherapy. The median prescription dose of patients with induction chemotherapy and adjuvant chemotherapy was 35 Gy (range: 30–43 Gy/5–8 f) and 39 Gy (range: 30–45 Gy/5–8 f), respectively. Patients treated with adjuvant chemotherapy had higher BED10 (biological effective dose, α/β = 10) than those treated with induction chemotherapy (69.1 Gy versus 59.5 Gy, P <0.001), as well as longer follow-up (21 versus 15 months, P = 0.001). All radiation doses were delivered in 5–8 fractions. Tumors were similarly sized and T1 or T2 in both induction and adjuvant chemotherapy group (2.8 versus 3.0 cm median maximum diameter, P = 0.37). Patients were treated with SBRT plus induction chemotherapy or adjuvant chemotherapy contemporaneously throughout the time range studied ().
Table 1 Baseline patient characteristics
Association of clinical factors with OS
Seventy patients (70.0%) died during the observation period and 30 patients (30.0%) were still alive at their last followup. The median OS was 17.5 months (95% CI: 15.8–19.2 months). Moreover, 1-year and 2-year OS rate was 87.0% and 38.0%, respectively. Before treatment, a level of CA19-9 less than 200 U/mL was found in 57 patients while 43 patients had a level more than 200 U/mL. Among patients with the level of CA19-9 ≥2 upper limit of normal, significant decrease was found in 42 patients while 33 patients had no response or even elevated levels during follow-up. On univariate log-rank comparisons, CA19-9 response, chemotherapy strategies, and BED10 ≥ 60 Gy were predictive factors of OS (). On multivariate regression, patients with CA19-9 response after treatment, adjuvant chemotherapy and BED10 ≥60 Gy had a longer OS (). The number of predictive factors was associated with OS: (0) 12.2 months (95% CI: 11.1–13.3 months); (1) 14.7 months (95% CI: 13.0–16.4 months); (2) 19.7 months (95% CI: 17.3–22.1 months); (3) 23.5 months (95% CI: 21.7–25.3 months); P <0.001 (). Furthermore, patients receiving adjuvant chemotherapy had a longer OS than those with induction chemotherapy: adjuvant chemotherapy: 23.1 months (95% CI: 21.7–24.5 months); induction chemotherapy: 13.9 months (95% CI: 12.7–15.1 months); P <0.001 ().
Table 2 Univariate and multivariate analysis of clinical factors associated with OS
Figure 1 Association with number of positive predictive factors and (A) overall survival and (B) progression-free survival.

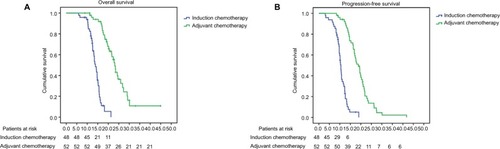
Figure 2 (A) Overall survival and (B) progression-free survival of patients with induction chemotherapy and adjuvant chemotherapy.
Association of clinical factors with PFS
The median PFS was 13.7 months (95% CI: 12.3–15.1 months), while 1-year and 2-year PFS rate was 65% and 16%, respectively. On univariate log-rank comparisons, CA19-9 response, chemotherapy strategies and BED10 ≥60 Gy were also associated with PFS (). On multivariate regression, longer PFS was found in patients with CA19-9 response after treatment and adjuvant chemotherapy (). The number of predictive factors was associated with PFS: (0) 10.1 months (95% CI: 9.0–11.2 months); (1) 16.2 months (95% CI: 13.3–19.1 months); (2) 20.8 months (95% CI: 18.7–22.9 months) P <0.001 (). Additionally, adjuvant chemotherapy correlated with longer PFS compared with induction chemotherapy: adjuvant chemotherapy: 18.8 months (95% CI: 16.7–20.9 months); induction chemotherapy: 10.5 months (95% CI: 9.9–11.1 months); P <0.001 ().
Table 3 Univariate and multivariate analysis of clinical factors associated with PFS
Adjusted survival of induction chemotherapy and adjuvant chemotherapy
Baseline ECOG (Eastern Cooperative Oncology Group), CA19-9 response and BED10 were as independent variables for propensity score matched analysis (). After propensity matching, there were 23 patients of each group included in the analysis. Both an overall survival and a progression survival benefit were found in patients with adjuvant chemotherapy: OS: induction chemotherapy: 15.6 months (95% CI: 14.4–16.8 months), adjuvant chemotherapy: 23.1 months (95% CI: 18.1–28.1 months); P <0.001. PFS: induction chemotherapy: 11.6 months (95% CI: 9.8–13.4 months), adjuvant chemotherapy: 18.0 months (95% CI: 14.5–21.5 months); P <0.001.
Adverse effects of SBRT and chemotherapy
Regarding acute radiation-induced toxicities, only 16 patients had grade 1 to 2 abdominal pain. There were no grade 3 or more acute or late radiation-induced adverse effects. With regard to induction chemotherapy, 11 (22.9%) and 15 patients (31.2%) experienced grade 3 neutropenia and gastrointestinal toxicity, including nausea, vomiting and abdominal pain, respectively. Furthermore, grade 3 neutropenia and gastrointestinal toxicity was found in 13 (25.0%) and 16 (30.8%) patients, respectively. There was no difference of incidences of hematological toxicity between induction chemotherapy group and adjuvant chemotherapy group (P = 0.81) and nor was the incidence of gastrointestinal toxicity (P = 0.96).
Discussion
Although surgical resection was given the first priority for resectable pancreatic cancer, there was no consensus or even reference guides for clinicians on treatment for patients with medically inoperable resectable pancreatic cancer. Therefore, these patients may be amenable to radiotherapy and chemotherapy. This pilot study sought to address the efficacy and tolerability of SBRT with chemotherapy for early stage but medically inoperable pancreatic cancer.
Hallmarks of SBRT include accurate, conformal delivery of high-dose radiation to targets while minimizing doses to organs at risk via precise target localizationCitation29 and steep dose gradients through multiple beam directions,Citation30 rendering SBRT as a potential curative modality for cancer.
Given the growing body of literature of prospective studies evaluating the efficacy of that modality, the median OS in the surgery-only arms ranged between 11 and 20.2 months, while it was 12.5–29.8 months and 9.9–19.4 months in the adjuvant treatment arms and in the neoadjuvant setting, respectively.Citation6,Citation31–Citation39 The median PFS was 5–10.2 months and 8.6–15.2 months in the surgery alone and neoadjuvant or adjuvant group.Citation6,Citation31–Citation39 In addition to conventional radiotherapy, preoperative short-course chemoradiation with proton beam therapy and capecitabine followed by early surgery for resectable pancreatic cancer was investigated.Citation40 The median OS and PFS for the entire group were 17 months and 10 months.Citation40 In our study, the median OS and PFS were 17.5 months and 13.7 months. Therefore, it was identified that SBRT with chemotherapy may not be inferior to surgery with chemotherapy for early stage pancreatic cancer.
The treatment strategy in our study showed that adjuvant chemotherapy was beneficial for OS. After adjustment for dose, patients with adjuvant chemotherapy still had longer OS and PFS than those with induction chemotherapy. The potential mechanism of this correlation might be speculated stimulation of anti-tumor immunity by SBRT, rendering a synergic effect of SBRT and chemotherapy.Citation41,Citation42
In our previous study, it was elucidated that patients receiving BED10 ≥60 Gy achieved better tumor response 6 months after SBRT than those who received BED10 <60 Gy, though no correlation was found between the radiation dose and survival.Citation27 However, it was shown in this study that BED10 ≥60 Gy associated with OS and PFS. Likewise, Krishnan et alCitation43 also reported that BED10 >70 Gy was the predictor of OS. The potential reason may be the difference in patient selection. In the previous study, patients were elderly with advanced or medically inoperable pancreatic cancer with high tumor burdens or large tumor volumes. Hence, SBRT was majorly delivered as the palliative setting, while all patients in this study had resectable pancreatic cancer, indicating that curative radiotherapy should be administered. Nevertheless, patients with better performance status had higher doses, which may result in over-interpretation of prognostic impact of high doses. The limitation of this study was non-randomization. Therefore, the results might be influenced by potential factors though with stringent criteria, which required prospective and randomized studies. Another limitation was the small sample size of the two groups.
Conclusion
In conclusion, SBRT was safe and effective in resectable pancreatic cancer. Adjuvant chemotherapy, CA19-9 response and BED10 ≥60 Gy correlated with OS and the former two were predictive of PFS. We believe that SBRT, due to its short duration and excellent tolerability, combined with adjuvant chemotherapy may be an alternative for patients with early stage and resectable but medically inoperable pancreatic cancer.
Financial support
This study was sponsored by China Health Promotion Foundation (THC2015001) and Youth Fund of Changhai Hospital (CH201709).
Acknowledgments
The authors appreciated Dr Jiuhong Chen for her precise comments and LinkDoc for their constructive advice on patients’ follow-up.
Supplementary material
Table S1 PSM-adjusted patient characteristics
Disclosure
The authors report no conflict of interest in this work.
Reference
- SiegelRLMillerKDJemalACancer statistics, 2016CA Cancer J Clin201666173026742998
- SiegelRLMillerKDJemalACancer statistics, 2017CA Cancer J Clin201767173028055103
- ChenWZhengRBaadePDCancer statistics in China, 2015CA Cancer J Clin201666211513226808342
- SenerSFFremgenAMenckHRWinchesterDPPancreatic cancer: A report of treatment and survival trends for 100313 patients diagnosed from 1985–1995 using the National Cancer DatabaseJ Am Coll Surg199918911710401733
- MyrehaugSSahgalARussoSMStereotactic body radiotherapy for pancreatic cancer: Recent progress and future directionsExpert Rev Anticancer Ther201616552353026999329
- RegineWFWinterKAAbramsRFluorouracil-based chemoradiation with either gemcitabine or fluorouracil chemotherapy after resection of pancreatic adenocarcinoma: 5-year analysis of the U.S. Intergroup/RTOG 9704 phase III trialAnn Surg Oncol20111851319132621499862
- HermanJMSwartzMJHsuCCAnalysis of fluorouracil-based adjuvant chemotherapy and radiation after pancreaticoduodenectomy for ductal adenocarcinoma of the pancreas: Results of a large, prospectively collected database at the Johns Hopkins HospitalJ Clin Oncol200826213503351018640931
- OettleHNeuhausPHochhausAAdjuvant chemotherapy with gemcitabine and long-term outcomes among patients with resected pancreatic cancer: The CONKO-001 randomized trialJAMA2013310141473148124104372
- TsengJFRautCPLeeJEPancreaticoduodenectomy with vascular resection: margin status and survival durationJ Gastrointest Surg20048893594915585381
- HoyerMRoedHSengelovLPhase-II study on stereotactic radiotherapy of locally advanced pancreatic carcinomaRadiother Oncol2005761485315990186
- TemperoMAMalafaMPAl-HawaryMPancreatic adenocarcinoma. Version 2. 2017, NCCN Clinical Practice Guidelines in OncologyJ Natl Compr Canc Netw20171581028106128784865
- UenoHOkusakaTIkedaMTakezakoYMorizaneCAn early phase II study of S-1 in patients with metastatic pancreatic cancerOncology2005682–317117816006754
- UenoHIokaTIkedaMRandomized phase III study of gemcitabine plus S-1, S-1 alone, or gemcitabine alone in patients with locally advanced and metastatic pancreatic cancer in Japan and Taiwan: GEST studyJ Clin Oncol201331131640164823547081
- MorizaneCOkusakaTFuruseJA phase II study of S-1 in gemcitabine-refractory metastatic pancreatic cancerCancer Chemother Pharmacol200963231331918398614
- SudoKYamaguchiTNakamuraKDendaTHaraTIshiharaTYokosukaOPhase II study of S-1 in patients with gemcitabine-resistant advanced pancreatic cancerCancer Chemother Pharmacol201167224925420352216
- KharofaJTsaiSKellyTNeoadjuvant chemoradiation with IMRT in resectable and borderline resectable pancreatic cancerRadiother Oncol20141131414625443499
- CoxJDStetzJPajakTFToxicity criteria of the Radiation Therapy Oncology Group (RTOG) and the European Organization for Research and Treatment of Cancer (EORTC)Int J Radiat Oncol Biol Phys1995315134113467713792
- QiQZhuangLShenYA novel systemic inflammation response index (SIRI) for predicting the survival of patients with pancreatic cancer after chemotherapyCancer2016122142158216727152949
- LeeSHChungMJKimBThe significance of the prognostic nutritional index for all stages of pancreatic cancerNutr Cancer201769351251927967240
- GengYQiQSunMChenHWangPChenZPrognostic nutritional index predicts survival and correlates with systemic inflammatory response in advanced pancreatic cancerEur J Surg Oncol201541111508151426343824
- CharlsonMSzatrowskiTPPetersonJGoldJValidation of a combined comorbidity indexJ Clin Epidemiol19944711124512517722560
- Dias-SantosDFerroneCRZhengHLillemoeKDFernández-Del CastilloCThe Charlson age comorbidity index predicts early mortality after surgery for pancreatic cancerSurgery2015157588188725704415
- FerroneCRFinkelsteinDMThayerSPMuzikanskyAFernandezdelCastilloCWarshawALPerioperative CA19-9 levels can predict stage and survival in patients with resectable pancreatic adenocarcinomaJ Clin Oncol200624182897290216782929
- Von HoffDDRamanathanRKBoradMJGemcitabine plus nab-paclitaxel is an active regimen in patients with advanced pancreatic cancer: A phase I/II trialJ Clin Oncol201129344548455421969517
- CloydJMWangHEggerMEAssociation of clinical factors with a major pathologic response following preoperative therapy for pancreatic ductal adenocarcinomaJAMA Surg2017152111048105628700784
- ZhuXJuXCaoFSafety and efficacy of stereotactic body radiation therapy combined with S-1 simultaneously followed by sequential S-1 as an initial treatment for locally advanced pancreatic cancer (SILAPANC) trial: study design and rationale of a phase II clinical trialBMJ Open2016612e013220
- ZhuXLiFJuXPrognostic role of stereotactic body radiation therapy for elderly patients with advanced and medically inoperable pancreatic cancerCancer Med20176102263227028834410
- BenedictSHYeniceKMFollowillDStereotactic body radiation therapy: the report of AAPM Task Group 101Med Phys20103784078410120879569
- LeksellLThe stereotaxic method and radiosurgery of the brainActa Chir Scand1951102431631914914373
- HartmannGHSchlegelWSturmVKoberBPastyrOLorenzWJCerebral radiation surgery using moving field irradiation at a linear accelerator facilityInt J Radiat Oncol Biol Phys1985116118511923997600
- NeoptolemosJPStockenDDFriessHEuropean Study Group for Pancreatic CancerA randomized trial of chemoradiotherapy and chemotherapy after resection of pancreatic cancerN Engl J Med2004350121200121015028824
- Van LaethemJLHammelPMornexFAdjuvant gemcitabine alone versus gemcitabine-based chemoradiotherapy after curative resection for pancreatic cancer: A randomized EORTC-40013-22012/FFCD-9203/GERCOR phase II studyJ Clin Oncol201028294450445620837948
- NeoptolemosJPStockenDDBassiCEuropean Study Group for Pancreatic CancerAdjuvant chemotherapy with fluorouracil plus folinic acid vs gemcitabine following pancreatic cancer resection: a randomized controlled trialJAMA2010304101073108120823433
- UenoHKosugeTMatsuyamaYA randomised phase III trial comparing gemcitabine with surgery-only in patients with resected pancreatic cancer: Japanese Study Group of Adjuvant Therapy for Pancreatic CancerBr J Cancer2009101690891519690548
- YoshitomiHTogawaAKimuraFPancreatic Cancer Chemotherapy Program of the Chiba University Department of General Surgery Affiliated Hospital GroupA randomized phase II trial of adjuvant chemotherapy with uracil/tegafur and gemcitabine versus gemcitabine alone in patients with resected pancreatic cancerCancer200811392448245618823024
- PalmerDHStockenDDHewittHA randomized phase 2 trial of neoadjuvant chemotherapy in resectable pancreatic cancer: Gemcitabine alone versus gemcitabine combined with cisplatinAnn Surg Oncol20071472088209617453298
- SchmidtJAbelUDebusJOpen-label, multicenter, randomized phase III trial of adjuvant chemoradiation plus interferon Alfa-2b versus fluorouracil and folinic acid for patients with resected pancreatic adenocarcinomaJ Clin Oncol201230334077408323008325
- GolcherHBrunnerTBWitzigmannHNeoadjuvant chemoradiation therapy with gemcitabine/cisplatin and surgery versus immediate surgery in resectable pancreatic cancer. Results of the first prospective randomized phase II trialStrahlenther Onkol2015191171625252602
- ReniMBalzanoGAprileGAdjuvant PEFG (cisplatin, epirubicin, 5-fluorouracil, gemcitabine) or gemcitabine followed by chemoradiation in pancreatic cancer: A randomized phase II trialAnn Surg Oncol20121972256226322237835
- HongTSRyanDPBorgerDRA phase 1/2 and biomarker study of preoperative short course chemoradiation with proton beam therapy and capecitabine followed by early surgery for resectable pancreatic ductal adenocarcinomaInt J Radiat Oncol Biol Phys201489483083824867540
- DemariaSFormentiSCRadiation as an immunological adjuvant: Current evidence on dose and fractionationFront Oncol2012215323112958
- PoppIGrosuALNiedermannGDudaDGImmune modulation by hypofractionated stereotactic radiation therapy: Therapeutic implicationsRadiother Oncol2016120218519427495145
- KrishnanSChadhaASSuhYFocal radiation therapy dose escalation improves overall survival in locally advanced pancreatic cancer patients receiving induction chemotherapy and consolidative chemoradiationInt J Radiat Oncol Biol Phys201694475576526972648