
Abstract
Background
The association between Graves’ disease (GD) and thyroid carcinoma remains controversial. This study aimed to investigate incidental thyroid carcinoma (ITC) in surgery-treated hyperthyroid patients with and without GD.
Materials and methods
We searched PubMed and EMBASE for cohort studies investigating ITC in surgery-treated hyperthyroid patients without prediagnosed thyroid carcinoma in accordance with the Meta-Analysis of Observational Studies in Epidemiology guidelines. The last search was updated to January 23, 2018. All statistical tests were performed using Review Manager 5.3 and STATA version 12.0.
Results
Eleven cohort studies involving 10,743 GD and 3,336 non-GD patients were included. The pooled prevalence of ITC was 7.0% (95% confidence interval [CI] 4.5–9.6), and was comparable in surgery-treated GD and non-GD hyperthyroid patients (GD vs non-GD: pooled odds ratio [OR], 1.0; 95% CI: 0.68–1.46; P=0.98). In the subgroup analysis, toxic adenoma and toxic nodular goiter showed no difference when comparing with GD (pooled OR, 0.53; 95% CI: 0.21–1.36; P=0.18 and pooled OR, 1.01; 95% CI: 0.65–1.57; P=0.95, respectively).
Conclusion
Our study demonstrated that GD was not associated with increased risk of ITC in surgery-treated hyperthyroid patients.
Introduction
The prevalence of thyroid carcinoma has rapidly increased over two-fold in the past three decades.Citation1 The hypothetical mechanisms for the disease include exposure to ionizing radiation (especially among children), iodine deficiency and excess, etc.Citation2 Hashimoto’s thyroiditis (HT), a common autoimmune thyroid disease,Citation3–Citation6 was reported to be associated with increased risk of incidental carcinoma.Citation7–Citation9 One explanation for this association was the underlying autoimmunity.Citation10,Citation11
Graves’ disease (GD), also known as toxic diffuse goiter, is another common autoimmune thyroid disease and is considered as the leading cause of hyperthyroidism.Citation12 Although GD is not a traditional risk factor for thyroid cancer,Citation13,Citation14 a recent studyCitation15 showed that the expression levels of specific miRNAs in thyroid tissue from GD patients lay between those with normal thyroid glands and those with papillary thyroid carcinoma (PTC), suggesting the possibility of PTC development in GD patients. A population-based study also indicated a 10-fold increased cancer risk in GD patients.Citation16 However, because the cancer detection by thyroid ultrasound examination and subsequent confirmation of diagnosis were more likely to be conducted in patients with GD compared to euthyroid adults, the conclusion defining GD as a risk factor of PTC cannot be drawn. Therefore, whether GD serves as a risk factor of thyroid carcinoma is still unclear. Three therapeutic options for hyperthyroidism were suggested by the guidelines, namely radio-iodine therapy, medication, and surgery.Citation17,Citation18 Incidental carcinoma could be identified occasionally in surgery-treated GD and non-GD hyperthyroid patients without identified malignancy before surgery.Citation19 However, it remains unclear whether incidental thyroid carcinoma (ITC) is more frequently detected in patients with GD than those with other causes of hyperthyroidism. Thus, the current study aimed to investigate whether GD was associated with the risk of thyroid carcinoma in surgery-treated hyperthyroid patients by conducting a systematic review and comparing the prevalence of ITC between surgery-treated patients with GD and hyperthyroidism of other causes.
Materials and methods
Search strategy
This meta-analysis was planned, performed, and reported in accordance with the Meta-Analysis of Observational Studies in Epidemiology guidelines.Citation20 Electronic databases were used for the literature searching, including EMBASE (from 1949) and PubMed (from 1946). The last search was updated to January 23, 2018. The combination of the keywords is given in the Supplementary materials. The Medical Subject Heading terminology was also used when available. As a supplement, bibliographies of identified studies were searched to make sure all the potentially relevant studies were included. No ethical approval or patient consent was required because all analyses were based on already existing literature.
Inclusion and exclusion criteria
Included studies had to have met the following inclusion criteria: 1) they should be cohort studies, either prospective or retrospective, 2) all patients in the studies underwent surgery due to hyperthyroidism, and 3) the number of ITC in both GD patients and non-GD hyperthyroid patients should be reported. Exclusion criteria were as follows: 1) duplicated studies or publications, 2) studies with incomplete data, 3) studies including any patient with diagnosed or suspected thyroid malignancy before surgery in the analysis, and 4) studies published in languages other than English.
Study selection
Two reviewers (QJ and YL) independently screened the titles and abstracts, and then full texts for eligibility. Discrepancies between the two reviewers’ selections were resolved by discussion with a third author (SL).
Data extraction and quality assessment
The following information was extracted by the three reviewers (QJ, XL, and SL) independently from every eligible study: first author, year of publication, country, ethnicity, surgery method, definition of GD and thyroid carcinoma, age, gender, patient-recruiting window, number of subjects with GD and non-GD hyperthyroidism (patients with toxic adenoma [TA], toxic nodular goiter [TNG]), and the number of thyroid carcinoma in these groups. If available, data on the histological diagnosis and proportion of microcarcinoma in GD and other thyroid diseases were collected. The Newcastle–Ottawa Scale was used for assessing the quality of the included studies.Citation21 All disagreements were resolved through discussion.
Statistical analysis
In this meta-analysis, the prevalence was pooled by meta-analysis using STATA 12.0 (StataCorp LP, College Station, TX, USA). The risk of incidental thyroid cancer was measured by odds ratio (OR) with 95% confidence interval (CI), and pooled using Mantel–Haenszel (M–H) random-effect model due to clinical heterogeneity across studies.Citation22 The overall data were pooled by meta-analysis, and a P-value below 0.05 was considered statistically significant. Between-study heterogeneity was estimated using the chi-squared test (in which P<0.10 was considered to indicate the presence of statistical heterogeneity) and quantified with the I2 statistic (in which I2 ≥50% was considered to indicate significant statistical heterogeneity).Citation23 Subgroup analyses by types of hyperthyroidism and microcarcinoma were also conducted to explore the source of heterogeneity. Five sensitivity analyses were carried out; these were as follows: 1) remove-one assay, 2) alternative pooling method (Peto instead of M–H method), 3) alternative statistical model (fixed effects instead of random effects), 4) exclusion of studies with ambiguous definitions of hyperthyroidism, and 5) exclusion of studies with unclear definitions of GD. Funnel graph, Begg’s test, and Egger’s testCitation24,Citation25 were employed to evaluate the potential publication bias.Citation26 All statistical tests were performed using Review Manager 5.3 (Cochrane Collaboration, Oxford, UK) and STATA version 12.0 (STATA; StataCorp LP).
Results
Study screening and characteristics
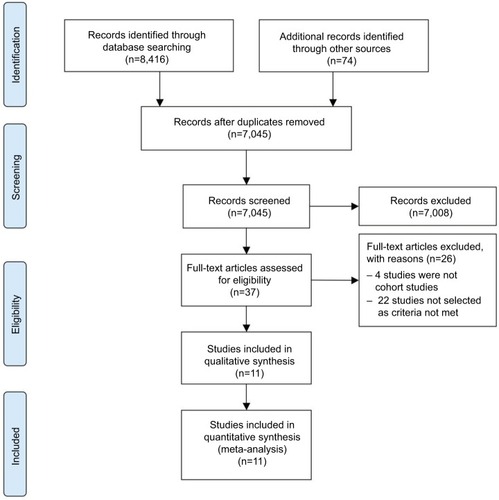
As shown in , a total of 8,416 articles were originally identified, and 74 articles were additionally identified through looking at the references of the screened papers and peer discussion. After title and abstract screening, 37 studies were left for full-text assessment. Eleven studiesCitation27–Citation37 involving 10,743 GD patients and 3,336 patients without GD were included for quantitative analysis and were eligible for further meta-analysis. The baseline characteristics of each included study are summarized in . The mean age of patients from each included study ranged from 39 to 55.7 years. The majority (73–84.5%) of subjects were female. Seven studiesCitation28,Citation30,Citation31,Citation33,Citation34,Citation36,Citation37 had available data on thyroid microcarcinoma, which contributed to 65.59% of the total cancer occurrence. The definitions of GD and hyperthyroidism were based on clinical decisions and symptoms (diagnostic details are shown in Table S1). All definitions of thyroid cancer were based on postsurgical pathological results (histological definitions and classifications can be seen in Table S2). Besides GD, four studiesCitation27,Citation28,Citation34,Citation36 included surgery-treated hyperthyroid patients with TA, while ten studiesCitation28–Citation37 included those with TNG. The indications as well as types of thyroidectomy are also listed in Table S1.
Table 1 Baseline characteristics of included studies
Figure 1 Flow diagram of study selection.
Quality assessment
The Newcastle–Ottawa Scale of included studies ranged from 5 to 8, and the average score was 6.5 (). Three studies were scored at the lowest level (5 in score) mainly due to their failure to provide adequate information on whether all patients were recruited from the same population.Citation29,Citation31,Citation34
Meta-analysis
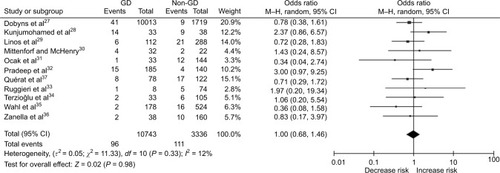
Among the included studies, the prevalence of ITC in surgery-treated hyperthyroid patients ranged from 0.4% to 32.4%, and the pooled prevalence was 7.0% (95% CI 4.5–9.6) (). As shown in , the prevalence of incidental carcinoma in GD and non-GD patients was not significantly different (pooled OR, 1.0; 95% CI: 0.68–1.46; P=0.98).
Figure 2 Forest plot for the overall estimate of the prevalence of thyroid cancer.
Abbreviations: ES, effect size; CI, confidence interval.
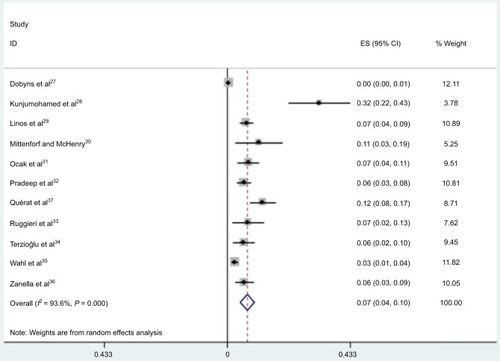
Figure 3 Forest plot for the pooled OR in surgery-treated hyperthyroid patients with and without GD.
Abbreviations: GD, Graves’ disease; OR, odds ratio; CI, confidence interval; M–H, Mantel–Haenszel.
In the subgroup analysis, four studies involving 83 patients reported the ITC in patients with GD and TA, and ten studies compared the prevalence of ITC in GD and TNG (including toxic multinodular goiter and toxic uninodular goiter) patients, detecting no significant difference (pooled OR, 0.53; 95% CI: 0.21–1.36; P=0.18 and pooled OR, 1.01; 95% CI: 0.65–1.57; P=0.95, respectively).
PTC is the most common type of thyroid carcinoma, especially in incidental carcinoma.Citation18 Eight studiesCitation28–Citation31,Citation33,Citation34,Citation36,Citation37 reported incidental PTC with clear definition (including single papillary carcinoma, occult papillary carcinoma, multifocal papillary carcinoma, and papillary microcarcinoma). The overall meta-analysis and subgroup analysis according to the etiology of hyperthyroidism provided similar results regarding the overall risk of ITC (Figure S1).
Publication bias and sensitivity analysis
Funnel plots seemed to be symmetric in our meta-analysis (Figure S2). The Egger’s test (P=0.774) did not detect a statistically significant publication bias.
In order to assess the stability of the result of the current meta-analysis, sensitivity analysis was performed by sequentially excluding one single study each time. Similar results were acquired, suggesting the stability of our meta-analysis (Figure S3.1). As the definitions of either hyperthyroidism or GD were absent in several studies (Table S1), another sensitivity analysis was conducted by excluding studies lacking detailed explanation of hyperthyroidism or GD. The results showed no significant change after excluding undefined hyperthyroidism or GD (pooled OR, 1.16; 95% CI: 0.48–2.81; P=0.74 and pooled OR, 0.91; 95% CI: 0.48–1.73; P=0.77, respectively; shown in Figures S3.2 and S3.3, respectively). Sensitivity analyses using Peto OR and M–H fixed-effect model also confirmed the robustness of the study (Figures S3.4 and S3.5).
Discussion
Our systematic review including 11 cohort studies and over 10,000 participants indicated that the pooled prevalence of ITC was 7.0% (95% CI: 4.5%–9.6%) in surgery-treated hyperthyroid patients. Unlike HT,Citation8 GD did not seem to increase the risk of ITC compared with other hyperthyroid diseases among surgery-treated hyperthyroid patients. Both the subgroup analysis and sensitivity analysis confirmed the conclusion.
Although accumulated studies suggested an increased cancer risk in patients with HT and positive HT-related autoantibodies,Citation8,Citation38,Citation39 our study demonstrated that no increase of ITC risk was detected in surgery-treated patients when compared to those with other causes. A possible explanation is that low or low–normal thyroid-stimulating hormone level could be present in GD patients before the thyrotoxicosis is diagnosed. Studies have proven that long-term suppressed level of thyroid-stimulating hormone (eg, in TA and TNG) significantly reduced the risk of thyroid carcinoma, especially PTC.Citation12,Citation40 This theory might explain the opposite risk of the thyroid malignancy in patients with HT and GD. Meanwhile, our study indicated that thyroid autoimmunity and presence of thyroid autoantibodies, which are common in both GD and HT, might contribute little in the pathogenesis of thyroid malignancy. But direct evidence is required in future investigations.
It must be noted that although ITC could be occasionally detected in hyperthyroid patients when their thyroid glands were removed by surgery, it should not be overtreated. The prevalence of occult papillary carcinoma in autopsy varied from 5.6% to 35.6%,Citation41 indicating PTC as a latent neoplasm. Papillary thyroid microcarcinoma contributed to a very low mortality in the absence of treatment but with active surveillance.Citation42,Citation43 Since GD is not associated with the development of thyroid cancer according to our study, thyroidectomy should not be the first-line treatment in hyperthyroid patients where hyperthyroidism is caused by GD. Also, thyroidectomy should not be done for the purpose of preventing thyroid cancer.
Our subgroup analysis indicated that the risk of ITC was not significantly different among patients with hyperthyroidism caused by TNG/TA and GD. However, TNG and TA are both benign thyroid tumors, with a theoretical potential to turn malignant on occasion. Thus, choosing TNG and TA as the control in our study might have underestimated the malignancy risk of GD.
A recent population-based study in Taiwan indicated a 10-fold increased cancer risk in patients with GD,Citation16 which was inconsistent with our results. The study was not included in our meta-analysis because the treatment modality of the participants was not identified. In this claims database analysis, the patients and controls were not well stratified by the risk of cancers during the matching and adjustment. Most of the controls seemed to be free of a history of thyroid diseases, compared to whom the GD patients in the study were more likely to undergo thyroid ultrasound examinations to find occult masses. A recent meta-analysis by StaniforthCitation44 also reported on the ITC incidence among surgery-treated GD patients, revealing no increased risk of carcinoma. However, this study did not pool all cohort, case–control, and cross-sectional studies in a single analysis, which was considered methodologically inappropriate and might introduce additional bias. One studyCitation27 included in our analysis with a particularly large sample size was absent in theirs. Contributing to the major population in our meta-analysis, this study increased the strength of our study but did not lead to instable results, as can be seen by the sensitive analysis (Figure S3).
Strengths and limitations of this study
The strengths of our study include the comprehensive collection of current evidence of any study design for the topic and the nonselection of studies with patients with suspected malignancy. Some limitations of this meta-analysis must be acknowledged when interpreting our results. First, the definitions of presurgical GD and hyperthyroidism were mainly based on the clinical assessments and were heterogeneous between the included studies. But the multiple sensitivity analyses did not alter the trend of our results. Second, due to the lack of data of nodule presence in GD and the treatment length prior to surgery, related stratified analyses were not feasible. Whether the thyroid carcinoma was found in the nodule or the gland was not clarified among studies. It is difficult in this study to adjust thyroid nodule as a corisk factor of thyroid carcinoma. Meanwhile, although the statistical method did not indicate significant between-study heterogeneity, some clinical heterogeneity could still be undetected.
Conclusion
Our systematic review demonstrated that GD was not associated with increased risk of ITC in surgery-treated hyperthyroid patients. Thus, thyroidectomy is inappropriate for the purpose of preventing thyroid cancer in GD patients. Further long-term cohort study of cancer risk is required in hyperthyroid patients receiving nonsurgical treatment, such as antithyroid drugs or radioactive iodine therapy.
Acknowledgments
The study was supported by grants from the National Natural Science Foundation of China [grant number 81400811 and 21534008], National Basic Research Program of China [grant number 2015CB942800], the Scientific Research Project of Health and Family Planning Commission of Sichuan Province [grant number 130029, 150149, 17PJ063, and 17PJ445], Cholesterol Fund by China Cardiovascular Foundation and China Heart House, and the International Visiting Program for Excellent Young Scholars of SCU.
Author contributions
HT and SL conceived this study. QJ and YL performed the literature search and identification. KR assessed the full-text of included studies. QJ, XL, and SL extracted the data. QJ, LL, JSWK, and XS performed the statistical analysis. QJ, XL, YJ, HT, and SL interpreted the results. QJ, XL, KR, and SL drafted the manuscript. All authors critically revised the manuscript and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
- CarlingTUdelsmanRThyroid cancerAnnu Rev Med20136512513724274180
- DaviesLMorrisLGHaymartMAmerican Association of Clinical Endocrinologists and American College of Endocrinology disease state clinical review: the increasing incidence of thyroid cancerEndocr Pract201521668669626135963
- EisenbergBLHensleySDThyroid cancer with coexistent Hashimoto’s thyroiditis. Clinical assessment and managementArch Surg19891249104510472774906
- OkayasuIFujiwaraMHaraYTanakaYRoseNRAssociation of chronic lymphocytic thyroiditis and thyroid papillary carcinoma. A study of surgical cases among Japanese, and white and African AmericansCancer19957611231223188635037
- SchäfflerAPalitzschKDSeiffarthCCoexistent thyroiditis is associated with lower tumour stage in thyroid carcinomaEur J Clin Invest199828108388449792998
- TamimiDMThe association between chronic lymphocytic thyroiditis and thyroid tumorsInt J Surg Pathol200210214114612075407
- Feldt-RasmussenURasmussenAKAutoimmunity in differentiated thyroid cancer: significance and related clinical problemsHormones (Athens)20109210911720687394
- LeeJHKimYChoiJWKimYSThe association between papillary thyroid carcinoma and histologically proven Hashimoto’s thyroiditis: a meta-analysisEur J Endocrinol2013168334334923211578
- NoureldineSITufanoRPAssociation of Hashimoto’s thyroiditis and thyroid cancerCurr Opin Oncol2015271212525390557
- MedenicaSRadojevicNStojkovicMAutoimmunity and thyrotropin level in developing thyroid malignancyEur Rev Med Pharmacol Sci201519152824282926241536
- WuXLunYJiangHCoexistence of thyroglobulin antibodies and thyroid peroxidase antibodies correlates with elevated thyroid-stimulating hormone level and advanced tumor stage of papillary thyroid cancerEndocrine201446355456024338678
- FioreEVittiPSerum TSH and risk of papillary thyroid cancer in nodular thyroid diseaseJ Clin Endocrinol Metab20129741134114522278420
- HalesIBMcElduffACrummerPDoes Graves’ disease or thyrotoxicosis affect the prognosis of thyroid cancerJ Clin Endocrinol Metab19927538868891517381
- StockerDJBurchHBThyroid cancer yield in patients with Graves’ diseaseMinerva Endocrinol200328320521214605602
- PohlMGrabellusFWormKIntermediate microRNA expression profile in Graves’ disease falls between that of normal thyroid tissue and papillary thyroid carcinomaJ Clin Pathol2017701333927371612
- ChenYKLinCLChangYJCancer risk in patients with Graves’ disease: a nationwide cohort studyThyroid201323787988423421548
- BahnRSBurchHBCooperDSHyperthyroidism and other causes of thyrotoxicosis: management guidelines of the American Thyroid Association and American Association of Clinical EndocrinologistsEndocr Pract201117345652021700562
- RossDSBurchHBCooperDS2016 American Thyroid Association Guidelines for Diagnosis and Management of Hyperthyroidism and Other Causes of ThyrotoxicosisThyroid201626101343142127521067
- WeiSBalochZWLiVolsiVAThyroid carcinoma in patients with Graves’ disease: an institutional experienceEndocr Pathol2015261485325332114
- StroupDFBerlinJAMortonSCMeta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) groupJAMA2000283152008201210789670
- StangACritical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analysesEur J Epidemiol201025960360520652370
- BradburnMJDeeksJJBerlinJARussell LocalioAMuch ado about nothing: a comparison of the performance of meta-analytical methods with rare eventsStat Med2007261537716596572
- HigginsJPThompsonSGQuantifying heterogeneity in a meta-analysisStat Med200221111539155812111919
- TalebiMStudy of publication bias in meta-analysis using trim and fill methodInt J Sci Basic Appl Res2013413136
- EggerMDavey SmithGSchneiderMMinderCBias in meta-analysis detected by a simple, graphical testBMJ199731571096296349310563
- HayashinoYNoguchiYFukuiTSystematic evaluation and comparison of statistical tests for publication biasJ Epidemiol200515623524316276033
- DobynsBMShelineGEWorkmanJBTompkinsEAMcconaheyWMBeckerDVMalignant and benign neoplasms of the thyroid in patients treated for hyperthyroidism: a report of the cooperative thyrotoxicosis therapy follow-up studyJ Clin Endocrinol Metab19743869769984134013
- KunjumohamedFPAl-BusaidiNBAl-MusalhiHNAl-ShereiqiSZAl-SalmiISThe prevalence of thyroid cancer in patients with hyperthyroidismSaudi Med J201536787487726108596
- LinosDAKarakitsosDPapademetriouJShould the primary treatment of hyperthyroidism be surgical?Eur J Surg199716396516579311471
- MittendorfEAMcHenryCRThyroidectomy for selected patients with thyrotoxicosisArch Otolaryngol Head Neck Surg20011271616511177016
- OcakSAktenAOTezMThyroid cancer in hyperthyroid patients: is it different clinical entity?Endocr Regul2014482656824824801
- PradeepPVAgarwalABaxiMAgarwalGGuptaSKMishraSKSafety and efficacy of surgical management of hyperthyroidism: 15-year experience from a tertiary care center in a developing countryWorld J Surg200731230631217219271
- RuggieriMScoccheraFGenderiniMMascaroALuongoBPaoliniAHyperthyroidism and concurrent thyroid carcinomaEur Rev Med Pharmacol Sci19993326526811261738
- TerzioğluTTezelmanSOnaranYTanakolRConcurrent hyperthyroidism and thyroid carcinomaBr J Surg19938010130113028242305
- WahlRAGoretzkiPMeybierHNitschkeJLinderMRöherHDCoexistence of hyperthyroidism and thyroid cancerWorld J Surg1982643853907123975
- ZanellaERulliFSianesiMHyperthyroidism with concurrent thyroid cancerAnn Ital Chir200172329329711765347
- QuératCGermainNDumollardJMEstourBPeoc’hMPradesJMSurgical management of hyperthyroidismEur Ann Otorhinolaryngol Head Neck Dis20151322636625592327
- BüyükaşıkOHasdemirAOYalçınEThe association between thyroid malignancy and chronic lymphocytic thyroiditis: should it alter the surgical approach?Endokrynol Pol201162430330821879469
- JankovicBLeKTHershmanJMClinical Review: Hashimoto’s thyroiditis and papillary thyroid carcinoma: is there a correlation?J Clin Endocrinol Metab201398247448223293329
- SlijepcevicNZivaljevicVMarinkovicJSipeticSDiklicAPaunovicIRetrospective evaluation of the incidental finding of 403 papillary thyroid microcarcinomas in 2466 patients undergoing thyroid surgery for presumed benign thyroid diseaseBMC Cancer2014151330
- ItoYMiyauchiAA therapeutic strategy for incidentally detected papillary microcarcinoma of the thyroidNat Clin Pract Endocrinol Metab20073324024817315032
- LeboulleuxSTuttleRMPaciniFSchlumbergerMPapillary thyroid microcarcinoma: time to shift from surgery to active surveillance?Lancet Diabetes Endocrinol201641193394227550849
- MiyauchiAClinical trials of active surveillance of papillary microcarcinoma of the thyroidWorld J Surg201640351652226744340
- StaniforthJUErdirimanneSEslickGDThyroid carcinoma in Graves’ disease: a meta-analysisInt J Surg20162711812526626367