
Abstract
Background
The refractory/relapsed multiple myeloma (RRMM) remains a big clinical challenge, due to its biological and clinical complexity. Leading hematologists have performed many randomized controlled trials (RCTs) worldwide, and their findings were summarized in a recently published network meta-analysis (NMA) but with certain limitations.
Materials and methods
We performed an updated NMA of RCTs related to RRMM treatment, focusing on efficacy measures including the nonresponse rate (NRR), time to progression (TTP), progression-free survival (PFS), and overall survival (OS). The PubMed database was searched. We extended the literature search strategy of a previous NMA to June 30, 2017 and included additional primary RCTs. The surface under the cumulative ranking curve (SUCRA) was calculated to rank the regimens. A weighted-average method was used to rank the regimens by summarizing SUCRAs across different outcome measures.
Results
Finally, a total of 24 RCTs were included in this updated NMA. According to the result, the combination of daratumumab, lenalidomide, and dexamethasone showed better efficacy than other regimens in terms of NRR, TTP, and PFS (NRR: odds ratio [OR] =0.046, 95% credible interval [CrI] =[0.024, 0.085]; TTP: hazard ratio [HR] =0.14, 95% CrI =[0.092, 0.2]; PFS: HR =0.12, 95% CrI =[0.077, 0.18], compared with dexamethasone singlet). The combination of ixazomib, lenalidomide, and dexamethasone showed better efficacy than other regimens in terms of OS (HR =0.30, 95% CrI =[0.17, 0.54], compared with dexamethasone). The combination of daratumumab, lenalidomide, and dexamethasone ranked first in terms of overall efficacy (weighted average of SUCRAs =0.920).
Conclusion
The combination of daratumumab, lenalidomide, and dexamethasone may currently be the most effective regimen in the population of RRMM patients. Triplet regimens containing daratumumab, ixazomib, carfilzomib, or elotumumab plus lenalidomide and dexamethasone can be recommended as first-line therapies for RRMM patients.
Introduction
Since the early 2000s, the introduction of newly developed agents has dramatically improved the outcome of patients with multiple myeloma. However, the refractory/relapsed multiple myeloma (RRMM) remains a big challenge, due to its biological and clinical complexity. In an attempt to find ways to conquer RRMM, world’s leading hematologists have performed many randomized controlled trials (RCTs) worldwide. Recently, two research groups have tried to synthesize the results of these trials by network meta-analysis (NMA), a statistical analysis method by which a thorough comparison and ranking of all included treatment options is made possible.Citation1,Citation2 However, the two previous NMAs have certain limitations. To name a few, in the NMA by van Beurden-Tan et al,Citation1 important outcomes such as overall survival (OS) were left uninvestigated and the ranking information was not provided; and in the other NMA by Botta et al,Citation2 regimens were grouped into categories before comparison, some of which seem inappropriate and may cause bias and confusion. Besides, we found that several new RCTs and updated trial reports are available for a new NMA. Considering the above, we performed the present study to update the evidence and improve its quality using traditional NMA and a self-designed weighted average method to rank the regimens by summarizing results across various efficacy outcome measures.
Materials and methods
Outcome measures
This updated NMA focuses on early and long-term efficacy outcomes, including the nonresponse rate (NRR), time to progression (TTP), progression-free survival (PFS) and OS. Response rate was considered instead of NRR because its outcome event, that is, the absence of objective response to treatment, a negative indicator of treatment efficacy and prognosis, is similar to events of other outcome measures, which allows ranking by summarizing results across all these outcome measures.
Literature search and study selection
The PubMed database was searched. We adopted the literature search strategy described by Botta et al.Citation2 In brief, all possible combinations of the following search terms were used for searching RCTs concerning RRMM patients: “multiple myeloma,” “relapse,” “refractory,” “randomized,” “management,” “regimen,” and “therapy.” No specific filters were used during the search. The time range of the search was between the January 1, 2000 and June 30, 2017.
The following predefined eligibility criteria were used for the study selection: 1) the study should be an RCT; 2) the subjects should be RRMM patients; 3) at least two different regimens were compared in the study, except for those comparing different dosing schemes or modes of administrations; 4) data for at least one of the outcome measures were available. Studies that did not match any of the above criteria were excluded.
Two authors (X.W.L. and X.Q.D.) independently performed the literature search and study selection and discussed with the third author (X.M.) to resolve any discrepancies.
Data extraction and statistical analysis
Two authors (X.W.L. and X.Q.D) independently reviewed the reports. Supplementary materials of the RCTs were included, and the following information was extracted from each study report: name of the first author, year of publication, trial identifications, treatment regimens used for the experimental and control arms, total number of patients, outcome measures investigated, and data for the calculation of effect size for each outcome.
Before NMA, the logarithmic odds ratio (OR) and its standard error were calculated for NRR, and the logarithmic hazard ratio (HR) and its standard error for time-to-event outcomes were original data inputs. Fixed effects Bayesian NMAs were conducted, and forest plots were generated with results shown as the HR and corresponding 95% credible interval (95%CrI). To include all treatments within one network, bortezomib with or without dexamethasone was considered identical and labeled as “bortezomib ± dexamethasone” and thalidomide with or without dexamethasone was considered identical and labeled as “thalidomide ± dexamethasone” as described in van Beurden-Tan et al.Citation1 The dexamethasone monotherapy was set as the common reference regimen. To rank all regimens, the surface under the cumulative ranking curve (SUCRA) was calculated for each outcome as described in Salanti et al Citation3 for a given regimen. A larger SUCRA score indicated better efficacy in terms of a specific outcome measure. For the final ranking regarding the overall efficacy, an arithmetic weighted average of SUCRA scores across NRR, PFS, and OS was calculated. A 20%, 35%, and 45% weight was given to the NRR, PFS, and OS, respectively. These weights were given in accordance with the importance of the outcome measures. We considered the OS the most important, PFS as the surrogate of OS the second most important, and NRR that reflects the early efficacy the least important. There was only one exception, oblimersen plus dexamethasone, for which data on PFS and OS were not available, thus an 80% weight was attributed to TTP. A larger weighted average of SUCRAs indicated a higher rank in terms of overall efficacy. The R software version 3.1.2 and the gemtc package were used to perform all the statistical analyses.
Results
Basic information of included RCTs
After literature search and study selection, a total of 29 trial reports published between 2005 and 2017 were considered eligible to be included in the NMA. As a result, 24 independent studies, with a total of 10,853 subjects and 21 different regimens were included in the present study. Compared with the inclusion results by Botta et al,Citation2 an additional seven referencesCitation4–Citation10 were included, among which four were newly identified studiesCitation4,Citation5,Citation9,Citation10 and three were updated study results.Citation6–Citation8 The basic information of the included references has been summarized in .
Table 1 Basic information of included RCT reports
NMA results
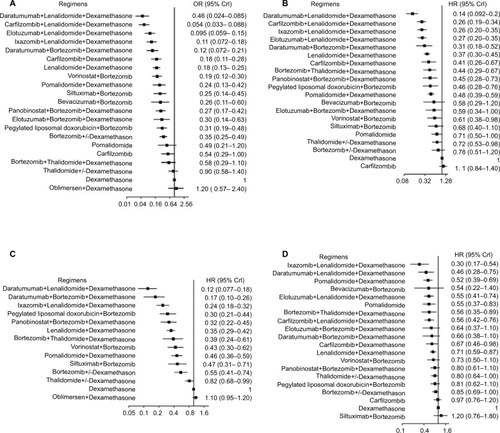
According to the results of NMAs, the combination of daratumumab, lenalidomide, and dexamethasone was the most effective therapy in terms of NRR, TTP, and PFS (NRR: OR =0.046, 95% CrI =[0.024, 0.085]; TTP: HR =0.14, 95% CrI =[0.092, 0.2]; PFS: HR =0.12, 95% CrI =[0.077, 0.18], compared with dexamethasone singlet; ), and the combination of ixazomib, lenalidomide, and dexamethasone is the most effective one in terms of OS (HR =0.12, 95%CrI =[0.17, 0.54]; ).
Figure 1 Forest plots presenting results of network meta-analysis: (A) nonresponse rate, (B) progression-free survival, (C) time to progression, (D) overall survival.
Abbreviations: OR, odds ratio; CrI, credible interval; HR, hazard ratio.
Ranking of regimens by SUCRA
As shown in , the ranking by SUCRA scores for each efficacy outcome was generally consistent with NMA findings. The combination of daratumumab, lenalidomide, and dexamethasone ranked first for NRR (SUCRA =0.984), TTP (SUCRA =0.988), and PFS (SUCRA =0.999). The combination of ixazomib, lenalidomide, and dexamethasone ranked first for OS (SUCRA =0.972).
Table 2 Included regimens, SUCRAs, weighted averages of SUCRAs across NRR, TTP, and OS, and ranks in terms of overall efficacy
In terms of overall efficacy measured by the weighted average of SUCRAs, the combination of daratumumab, lenalidomide, and dexamethasone ranked on top (weighted average =0.920), followed by the combination of ixazomib, lenalidomide, and dexamethasone (weighted average =0.907).
Discussion
Regardless of recent progress in management, RRMM is still an incurable disease, which has been attracting substantial research attention. In the past decades, a large number of RCTs concerning RRMM treatment were published, in which dozens of novel therapeutic regimens were tested and examined. Efforts were made to quantitatively summarize the evidence from RCTs by performing NMA, in order to provide useful and important information for clinical decision-making at minimal cost. However, flawed analyses may result in misleading conclusions. On the other hand, updates of NMAs on a timely basis are the key to keep the evidence “alive.” The present study included the most recently published trials and updates of previous trial reports, thoroughly investigated the efficacy profiles of 21 treatment options, and avoided certain limitations of previous NMAs mentioned above.
According to our results, the combination of daratumumab, lenalidomide, and dexamethasone was most effective in terms of NRR, TTP, and PFS. However, in terms of OS, it was less effective compared with the combination of ixazomib, lenalidomide, and dexamethasone. Ranking by overall efficacy showed that the daratumumab, lenalidomide, and dexamethasone triplet regimen had better performance than other regimens. Interestingly, we noted that the 21 regimens investigated in this NMA can be categorized into three subgroups based on the weighted average of SUCRA scores. The first subgroup includes four regimens (19.0%, weighted average from ~0.8 to ~0.9), which are the most effective ones, with lenalidomide and dexamethasone as the backbone plus one of the four latest agents (daratumumab, ixazomib, carfilzomib, or elotumumab). The second subgroup includes 11 regimens (52.4%, weighted average from ~0.4 to ~0.7), which show moderate efficacy in RRMM patients and are mostly doublet or triplet regimens. The third subgroup includes six regimens (28.6%, weighted average from 0.0 to 0.25), which are mostly singlet or doublet regimens having limited efficacy.
An important advantage of NMA over traditional meta-analysis is the possibility of ranking multiple treatment options. The SUCRA score, derived from the probability that a given treatment has a certain rank and calculated from the posterior distributions of all treatments, is widely used for ranking treatments in Bayesian NMAs. In this study, we applied a weighted averaging strategy to rank the regimens for overall efficacy. We assigned weights to different outcome measures in accordance with their importance. The OS is the “gold standard” outcome measure for the evaluation of long-term anticancer efficacy, the PFS and TTP are widely acknowledged surrogates of OS, and the treatment response associated with early efficacy may differ from long-term outcomes. Therefore, we gave a 20%, 35%, and 45% weight to NRR, PFS/TTP, and OS, respectively. We did not take safety into account, because to date no adequate data were available to include all treatment options in one network for any single adverse event outcome. A systematic review less quantitatively intense may be a good choice for further investigation on safety profiles. We do not recommend any ranking based on a combined quantitative analysis of efficacy and safety, because they are two facets distinct from one another, and it is very difficult to assign a rational and appropriate weight to each outcome.
The present study, similar to its preceding works, also has some limitations. First, although the relative importance of different outcome measures was considered, the appropriateness of the arbitrary assignment of weights needs further verification. Besides, it should acknowledge the limitations of the NMA fully when comparing benefits from the experimental treatments in patient populations that differ in previous treatments, cytogenetic risks, subsequent stem-cell transplantation, maintenance therapy, and so on. Although it could be possible to make adjustment by using approaches such as network meta-regression, the immaturity of methodology, limited number of included trials and frequent missingness in certain study-level variables make it difficult and less reliable.
Conclusion
In conclusion, the combination of daratumumab, lenalido-mide, and dexamethasone may currently be the most effective regimen in the population of RRMM patients. Triplet regimens containing daratumumab, ixazomib, carfilzomib, or elotumumab plus lenalidomide and dexamethasone can be recommended as the first-line therapies for RRMM patients.
Disclosure
The authors report no conflicts of interest in this work.
References
- van Beurden-TanCHYFrankenMGBlommesteinHMUyl-de GrootCASonneveldPSystematic literature review and network meta-analysis of treatment outcomes in relapsed and/or refractory multiple myelomaJ Clin Oncol201735121312131928240968
- BottaDCCCilibertoDRossiMNetwork meta-analysis of randomized trials in multiple myeloma: efficacy and safety in relapsed/refractory patientsBlood Adv20171745546629296961
- SalantiGAdesAEIoannidisJPGraphical methods and numerical summaries for presenting results from multiple-treatment meta-analysis: an overview and tutorialJ Clin Epidemiol201164216317120688472
- San MiguelJWeiselKMoreauPPomalidomide plus low-dose dexamethasone versus high-dose dexamethasone alone for patients with relapsed and refractory multiple myeloma (MM-003): a randomised, open-label, phase 3 trialLancet Oncol201314111055106624007748
- RichardsonPGSiegelDSVijRPomalidomide alone or in combination with low-dose dexamethasone in relapsed and refractory multiple myeloma: a randomized phase 2 studyBlood2014123121826183224421329
- MorganGPalumboADhanasiriSOverall survival of relapsed and refractory multiple myeloma patients after adjusting for crossover in the MM-003 trial for pomalidomide plus low-dose dexamethasoneBr J Haematol2015168682082325403264
- San-MiguelJFHungriaVTYoonSSOverall survival of patients with relapsed multiple myeloma treated with panobinostat or placebo plus bortezomib and dexamethasone (the PANORAMA 1 trial): a randomised, placebo-controlled, phase 3 trialLancet Haematol2016311e506e51527751707
- DimopoulosMALonialSWhiteDElotuzumab plus lenalidomide/dexamethasone for relapsed or refractory multiple myeloma: ELOQUENT-2 follow-up and post-hoc analyses on progression-free survival and tumour growthBr J Haematol2017178689690528677826
- HajekRMassziTPetrucciMTA randomized phase III study of carfilzomib vs low-dose corticosteroids with optional cyclophosphamide in relapsed and refractory multiple myeloma (FOCUS)Leukemia201731110711427416912
- HouJJinJXuYRandomized, double-blind, placebo-controlled phase III study of ixazomib plus lenalidomide-dexamethasone in patients with relapsed/refractory multiple myeloma: China Continuation studyJ Hematol Oncol201710113728683766
- RichardsonPGSonneveldPSchusterMWBortezomib or high-dose dexamethasone for relapsed multiple myelomaN Engl J Med2005352242487249815958804
- RichardsonPGSonneveldPSchusterMExtended follow-up of a phase 3 trial in relapsed multiple myeloma: final time-to-event results of the APEX trialBlood2007110103557356017690257
- DimopoulosMSpencerAAttalMLenalidomide plus dexamethasone for relapsed or refractory multiple myelomaN Engl J Med2007357212123213218032762
- OrlowskiRZNaglerASonneveldPRandomized phase III study of pegylated liposomal doxorubicin plus bortezomib compared with bortezomib alone in relapsed or refractory multiple myeloma: combination therapy improves time to progressionJ Clin Oncol200725253892390117679727
- WeberDMChenCNiesvizkyRLenalidomide plus dexamethasone for relapsed multiple myeloma in North AmericaN Engl J Med2007357212133214218032763
- Chanan-KhanAANiesvizkyRHohlRJPhase III randomised study of dexamethasone with or without oblimersen sodium for patients with advanced multiple myelomaLeuk Lymphoma200950455956519373653
- DimopoulosMAChenCSpencerALong-term follow-up on overall survival from the MM-009 and MM-010 phase III trials of lenalidomide plus dexamethasone in patients with relapsed or refractory multiple myelomaLeukemia200923112147215219626046
- GarderetLIacobelliSMoreauPSuperiority of the triple combination of bortezomib-thalidomide-dexamethasone over the dual combination of thalidomide-dexamethasone in patients with multiple myeloma progressing or relapsing after autologous transplantation: the MMVAR/IFM 2005-04 Randomized Phase III Trial from the Chronic Leukemia Working Party of the European Group for Blood and Marrow TransplantationJ Clin Oncol201230202475248222585692
- HjorthMHjertnerOKnudsenLMThalidomide and dexamethasone vs. bortezomib and dexamethasone for melphalan refractory myeloma: a randomized studyEur J Haematol201288648549622404182
- KropffMBaylonHGHillengassJThalidomide versus dexamethasone for the treatment of relapsed and/or refractory multiple myeloma: results from OPTIMUM, a randomized trialHaematologica201297578479122133776
- DimopoulosMSiegelDSLonialSVorinostat or placebo in combination with bortezomib in patients with multiple myeloma (VANTAGE 088): a multicentre, randomised, double-blind studyLancet Oncol201314111129114024055414
- WhiteDKassimABhaskarBYiJWamstadKPatonVEResults from AMBER, a randomized phase 2 study of bevacizumab and bortezomib versus bortezomib in relapsed or refractory multiple myelomaCancer2013119233934722811009
- San-MiguelJFHungriaVTYoonSSPanobinostat plus bortezomib and dexamethasone versus placebo plus bortezomib and dexamethasone in patients with relapsed or relapsed and refractory multiple myeloma: a multicentre, randomised, double-blind phase 3 trialLancet Oncol201415111195120625242045
- LonialSDimopoulosMPalumboAElotuzumab therapy for relapsed or refractory multiple myelomaN Engl J Med2015373762163126035255
- OrlowskiRZGerchevaLWilliamsCA phase 2, randomized, double-blind, placebo-controlled study of siltuximab (anti-IL-6 mAb) and bortezomib versus bortezomib alone in patients with relapsed or refractory multiple myelomaAm J Heamtol20159014249
- StewartAKRajkumarSVDimopoulosMACarfilzomib, lenalidomide, and dexamethasone for relapsed multiple myelomaN Engl J Med2015372214215225482145
- DimopoulosMAOriolANahiHDaratumumab, lenalidomide, and dexamethasone for multiple myelomaN Engl J Med2016375141319133127705267
- DimopoulosMAMoreauPPalumboACarfilzomib and dexamethasone versus bortezomib and dexamethasone for patients with relapsed or refractory multiple myeloma (ENDEAVOR): a randomised, phase 3, open-label, multicentre studyLancet Oncol2016171273826671818
- JakubowiakAOffidaniMPegourieBRandomized phase 2 study: elotuzumab plus bortezomib/dexamethasone vs bortezomib/dexamethasone for relapsed/refractory MMBlood2016127232833284027091875
- MoreauPMassziTGrzaskoNOral ixazomib, lenalidomide, and dexamethasone for multiple myelomaN Engl J Med2016374171621163427119237
- OrlowskiRZNaglerASonneveldPFinal overall survival results of a randomized trial comparing bortezomib plus pegylated liposomal doxorubicin with bortezomib alone in patients with relapsed or refractory multiple myelomaCancer2016122132050205627191689
- PalumboAChanan-KhanAWeiselKDaratumumab, bortezomib, and dexamethasone for multiple myelomaN Engl J Med2016375875476627557302