
Abstract
Background and objective
The risk of malignancy from “atypia of undetermined significance/follicular lesion of undetermined significance” (AUS/FLUS) is estimated to lie between 5% and 15%; however, some authors suggest that the risk of malignancy in AUS/FLUS depends upon specific clinical situations. This was a retrospective study which aimed to determine the incidence and risk of thyroid cancer (TC) based upon selected ultrasound features from patients with thyroid nodules (TN) classified as AUS/FLUS.
Methods
Univariate and multivariate logistic regression analyses were used to identify significant associations between ultrasound features and the risk of TC.
Results
Of 127 patients with TN classified as AUS/FLUS who underwent thyroidectomy, 114 (89.8%) had benign disease while 13 (10.2%) had TC. Univariate analysis identified several significant predictors for TC (all p<0.05), including microcalcifications, hypoechogenicity, the prevalence of irregular margins, a taller rather than a wide form, high vascularity, and fast tumor growth. Multivariate analysis further showed that microcalcifications (odds ratio =21.37; p=0.024) and fast growth (odds ratio =22.70; p=0.021) were significant and independent factors associated with the risk of developing TC.
Conclusion
Microcalcifications and fast growth of the TN could therefore be used as predictive factors for the development of TC in patients with AUS/FLUS.
Introduction
The category referred to as “atypia of undetermined significance and follicular lesion of undetermined significance” (AUS/FLUS) was included in The Bethesda System for Reporting Thyroid Cytology (TBSRTC) and collectively for a third category of this classification which is known as “Bethesda III.”Citation1 This is a rather heterogeneous group of thyroid lesions with borderline cellularity. Generally, the use of this TBSRTC classification during diagnosis minimizes the number of unnecessary thyroid surgeries and helps to avoid the unclear, long, and descriptive reports of material obtained from fine-needle aspiration biopsy (FNAB) procedures. TBSRTC therefore improves communication between cytologists, pathologists, endocrinologists, radiologists, and surgeons.
The risk of malignancy in the AUS/FLUS category is estimated to lie in the range of 5%–15%;Citation2 however, some authors suggest that the risk of malignancy in this third category depends upon the specific clinical situation.Citation3
The fourth category of the TBSRTC includes “follicular neoplasm (FN) and suspicious for a FN.” The risk of malignancy in this particular group lies in the range of 15%–30%.Citation1 This category is used to diagnose nodules that might appear as cancer during routine histopathological examinations. Thus, the borderline between the third and fourth categories of the TBSRTC classification is not clear-cut.
Some studies that have adopted terminology and criteria from the Bethesda classification have revealed high concordance in ultrasound-guided fine-needle aspiration cytology with almost 95% of samples interpreted in a satisfactory manner. Approximately 55%–74% of these patients were defined as being definitively benign, while ~2%–5% were defined as being definitively malignant.Citation4 The authors of this previous study classified the rest of the samples as “cytologically indeterminate.” This group contains the AUS/FLUS category, in which 2%–18% of patients have lesions, 2%–25% had FN in nodules, and 1%–6% were suspicious for malignancy. In a previous meta-analysis, Bongiovanni revealed significant variability in the probability of malignancy for each category of the Bethesda system.Citation4 This was compatible with the range predicted by TBSRTC classification, but with the exception of the third category (AUS/FLUS), for which the risk of malignancy in some studies was significantly higher than predicted.Citation4,Citation5 In a further study, Hagag et alCitation6 observed that palpable nodules had the same risk of malignancy as nonpalpable lesions when diagnosed by ultrasound examination. However, ultrasonography has been used to evaluate the risk of malignancy in thyroid nodules (TNs) and is considered to represent a decision-making tool for an indication of ultrasound-guided FNAB (UG-FNAB).
The most common ultrasound characteristics for thyroid malignancy are microcalcifications, hypoechogenicity, irregular margins, and a tall rather than a wide shape as measured on a transverse view. However, a recent study noted that the most specific characteristics for thyroid carcinoma are microcalcifications, irregular margins, and mentioned shape.Citation7 Kwak et alCitation8 used multivariable analyses to show that the risk of cancer is higher for nodules with either microlobulated margins or microcalcifications than for hypoechoic solid nodules without these features. The same authors noticed that macrocalcifications localized in the nodule with microcalcifications had the same oncological value as microcalcifications alone.
According to some studies which have adopted the TBSRTC classification, the risk of malignancy in the third and fourth category is ~15%,Citation1 in the third category 5%–15% and in the fourth category from 15% to 30%. The recommended clinical management for patients of the third category is to repeat the diagnostic procedure (FNAB), while in the fourth category, the usual recommended management is lobectomy or thyroidectomy.Citation1 Thus, the risk of malignancy in patients assigned to one of these 2 different categories might remain at the same level, although the recommendations for clinical management are completely different.
According to these observations, a very interesting question is very evident: are there any clinical characteristics of the TNs classified as AUS/FLUS, which form additional and helpful suggestions for repeat biopsy or surgery? Given the nuances of ultrasound pattern for different TNs, as well as the different cytological diagnoses of these lesions, we set out to evaluate whether malignancy risk stratification, based upon a multitude of ultrasound features, may help in determining the appropriate course of clinical management. In the absence of ultrasound features associated with a higher risk of malignancy in biopsied nodules categorized as AUS/FLUS in the TBSRTC classification, we could ascertain whether such lesions require further observation. On the other hand, the presence of these ultrasound patterns may allow us to direct patients with such nodules toward lobectomy or thyroidectomy. Moreover, the ability to distinguish between malignant TNs from benign ones in the AUS/FLUS category is extremely important, because, as some authors say, more tailored and minimally invasive treatment may be required.Citation9
Materials and methods
Our study protocol was approved by the Bioethics Committee of Wroclaw Medical University (Reference number: KB-783/2017). We obtained verbal consent from the participants instead of written consent because the data were analyzed anonymously and retrospectively on the basis of medical records. The process used to obtain verbal consent was deemed to be acceptable and was approved by the Bioethics Committee of Wroclaw Medical University. The authors did not have access to any identifying patient information and did not have any direct access to the study participants.
We retrospectively reviewed all FNAB reports and histopathological diagnoses from 4,296 patients who were admitted and received surgery for thyroid tumors in The First Department and Clinic of General, Gastroenterological and Endocrine Surgery between January 1, 2008 and December 31, 2016. All analyzed FNAB results were reported using TBSRTC classification and patients defined as the third category of TBSRTC (“Bethesda III”) were evaluated. All patients admitted and surgically treated in our department received ultrasound examination of the thyroid gland and lymph nodes of the neck prior to treatment. We evaluated three thyroid ultrasound examinations of each patient which were performed 24, 12 and 1 month before hospital admission and surgical treatment. All ultrasound results which qualified for the study (categorized as AUS/FLUS) were retrospectively analyzed. All ultrasound patterns of biopsied nodules assigned to the third category (AUS/FLUS) of the TBSRTC system were evaluated and compared to the final histopathological diagnoses.
Statistical analysis
All statistical analyses were carried out using Statistica 13.0 software (StatSoft, Tulsa, OK, USA). Descriptive data were presented as numbers and percentages (for qualitative variables) or means, SD, and 95% CIs for quantitative variables. The distribution of the data was analyzed by the Shapiro–Wilk normality test. Differences between the 2 study groups were analyzed by the χ2 test, by Fisher’s exact test, or by the Student’s t-test for independent samples.
The stepwise method of multivariate logistic regression analysis was used to determine independent predictive factors that were associated with the presence of thyroid cancer (TC). Odds ratios (ORs) and 95% CIs were calculated. A p≥0.1 was considered an exclusion criterion for our univariate logistic regression analysis.
Because of the small number of cancer cases, p-values arising from logistic regression analyses were confirmed by Fisher’s exact test (using 2-way contingency tables). A 2-tailed p-value of <0.05 was considered statistically significant for all other analyses.
Results
A total of 4,296 individuals were retrospectively reviewed. In this group of patients, 127 (2.95%) had TNs with a diagnosis of AUS/FLUS cytology. There were 105 (82.7%) females and 22 (17.3%) males with a mean age of 51.0±15.0 years. Resected nodules were classified histopathologically as follows: 57 (44.88%) patients had benign thyroid goiter, 12 (9.44%) patients had thyroiditis, 45 (35.43%) patients had adenoma, and 13 (10.23%) patients were diagnosed with TC. Radical surgery was performed in 9 (96.85%) patients, and a second round of surgery was required in 4 (3.14%) individuals with TC (). The characteristics of the total study group are shown in .
Table 1 Demographic, clinical, and operative indications of patients with TN Bethesda category III
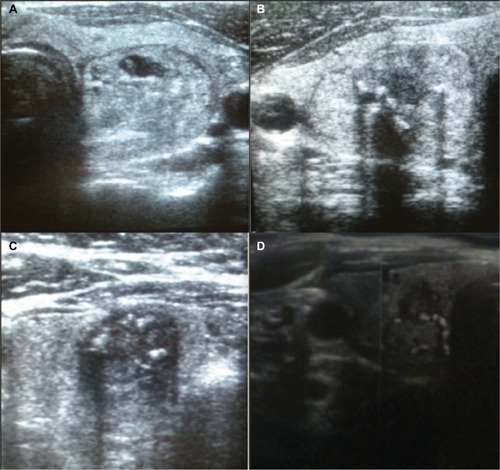
Figure 1 Sonographic patterns of malignant TNs classified by cytology as in the AUS/FLUS category of TBSRTC.
Notes: (A) Solid, partially hypoechoic nodule with irregular margins, (B) microcalcifications, hyper- and hypoechoic nodule with irregular margins, (C) microcalcifications, hypoechoic nodule with irregular margins, and (D) hypoechoic nodule with high intranodular vascularity and irregular margins.
Abbreviations: AUS/FLUS, atypia of undetermined significance/follicular lesion of undetermined significance; TBSRTC, The Bethesda System for Reporting Thyroid Cytology; TN, thyroid nodule.
Demographic, clinical, and operative characteristics of the patient subgroups
A total of 127 (100%) patients with TNs assigned to category III of the TBSRTC classification (AUS/FLUS, “Bethesda III”) were divided into 2 subgroups: 114 (89.8%) patients with benign disease of the TNs and 13 (10.2%) patients with TC. The comparative characteristics of these two patient subgroups are shown in . There were no significant differences in terms of gender or age between these 2 subgroups (p>0.05). However, the rates of radical thyroid resection and necessity for reoperation were significantly higher in patients with cancer than in patients with benign thyroid disease (p<0.0001 for both).
Ultrasound features of the two subgroups of patients are shown in . There were statistically significant differences in the rates of microcalcifications, echogenicity, nodule proportions, and tumor growth rate when comparing patients with benign thyroid disease and those with TC (p<0.0001 for all). There was a tendency toward a significant difference in the rate of tumor vascularity when comparing the 2 patient subgroups (p=0.052).
Table 2 Ultrasound features of patients with Bethesda category III TNs
Ultrasound features as independent predictors for the risk of TC
Logistic regression analysis was used to investigate the association of gender, age, and ultrasound features with the risk of TC. The results are presented in . In univariate logistic regression analysis, microcalcifications, hypoechogenicity, irregular margins, a tall rather than wide nodule proportion, high vascularity, and fast tumor growth were all significantly related to the risk of cancer. Then, a multivariate logistic regression model showed that the risk of TC significantly increased with intranodular microcalcifications () and fast tumor growth (p<0.05 for both). There was also a tendency for an association between tumors which were formed in a way that that were taller than they were wide and the risk of cancer (p=0.052).
Table 3 Univariate and multivariate logistic regression analysis of the association between risk of TC (noncancer group vs cancer group) and demographic and ultrasound parameters in patients of Bethesda category III
Discussion
Ultrasonography of the TNs is the most effective diagnostic tool for predicting malignancy and selecting these lesions for further evaluation.Citation10 UG-FNAB is the most cost-effective procedure that provides useful diagnostic information relating to further clinical management.Citation11 The clinical and practical purpose of this diagnostic tool is to reduce the number of unnecessary “diagnostic” surgical procedures in patients with benign nodules and detects those individuals in whom the risk of malignancy is high.
In 2007, the National Cancer Institute (NCI) hosted “The NCI Thyroid FNA State Science Conference” in Bethesda (Maryland), After this meeting, “The Bethesda Thyroid Atlas Project” was created and finally, the TBSRTC was formed.Citation12 This classification contains 6 categories of thyroid cytology, and each of these categories has an implied risk of malignancy ranging from 0% to 3% (category II) to as high as 97%–99% (category VI). Following UG-FNAB, the use of TBSRTC reduced the number of unnecessary thyroid surgeries in patients with benign nodules, but also increased the number of patients qualifying for surgery due to malignant progression. However even this global and well-prepared classification is associated with clinical dilemmas. The TBSRTC classification has been used in our own clinic ever since 2007. Between 2008 and 2016, the classification served as a basic presurgical diagnostic criterion.
According to the TBSRTC classification, the third category is associated with a 5%–15% risk of cancer, and the usual clinically recommended management is to repeat UG-FNAB.¹ In our patients, of the 127 (2.95%; 127/4,296) individuals classified in the AUS/FLUS category, 13 were diagnosed with thyroid carcinoma and 114 with benign disease; thus, the risk of malignancy in our study group was estimated to be 10.2%. However, in our patients, the diagnosis of AUS/FLUS category was estimated in 127 (2.95%) individuals (127/4,296). Some authors recommend that the AUS/FLUS category should not constitute >7% of all TBSRTC reports.Citation13 For example, Guo et alCitation14 estimated that 3% of their study group (8/236) could be categorized as AUS/FLUS; however, other studies have claimed that 2%–18% of thyroid lesions are associated with the AUS/FLUS category.Citation4
Generally, the most well-known and suspicious ultrasound features for the malignancy of TNs include hypoechogenicity, irregular margins, microcalcifications, and a taller than wide shape.Citation10 Some authors suggest, however, that no single ultrasound pattern can represent a strong predictor for the risk of thyroid malignancy and that the combined use of a multitude of such features may provide higher diagnostic accuracy.Citation15 In our present study, we observed statistically significant differences in the rates of microcalcifications, echogenicity, nodule proportions, and tumor growth rate between patients with benign thyroid disease and those with TC. A tendency for significant difference was also observed for the rate of tumor vascularity between patient subgroups. We also noticed that 52% of TNs within the AUS/FLUS category showed high intranodular vascularity (, ). However, Moon et alCitation16 suggested that this ultrasound pattern can be seen in 31% of benign TNs compared with 17% of malignant ones. Other studies suggest that microcalcifications and increased intranodular vascularity might be predictive for malignancy,Citation17 but others were unable to confirm these observations.Citation18 In our present study, 77% of patients in the AUS/FLUS category and with a final histopathological diagnosis of malignancy were shown to have high vascularity. However, in the group of cases in the AUS/FLUS category but with a benign final histopathological diagnosis, high vascularity was also observed in over 49% of individuals. This is why some authors have claimed that high intranodular vascularity is very useful in predicting TC,Citation19 while others suggest that high vascularity does not predict thyroid malignancy.Citation20 Chng et alCitation10 assessed the higher number of malignant TNs with irregular margins, hypoechogenicity, and a taller than wide shape. However, these authors also noticed that the size of the nodule, microcalcifications, and intranodular vascularity were not significantly different when compared between malignant and benign thyroid lesions. Chng et alCitation10 added that irregular margins had the highest positive predictive value for malignancy, because all of the nodules with this sonographic pattern were malignant in their study. The same observations were reported by Maia et alCitation18 in a group of 80 patients with “indeterminate thyroid cytology” and surgically treated in a single institution. These authors reported that irregular margins had the highest positive predictive value for malignancy. In a meta-analysis by Brito et al,Citation17 a taller than wide shape was estimated to the one ultrasound feature which has the highest diagnostic OR for predicting malignancy of the TNs when compared to other sonographic patterns. In our present study, we observed a tendency for association between taller than wide forms of tumor and the risk of cancer.
In accordance with the observations of other authors,Citation21,Citation22 we did not identify significant differences in either age or gender between patients with benign and malignant nodules.
Some authors describe a wide range in the risk of malignancy (6%–48%) in specimens categorized as AUS/FLUS.Citation13,Citation23,Citation24 This suggests that the criteria used for this classification are inconsistent. Furthermore, previous authors have stated that the risk of malignancy in the AUS/FLUS category depends upon the clinical and cytological features of the TN cells and accounts for 38% for patients defined as “atypia, rule out papillary carcinoma.”Citation23 These authors also stated that different types of follicular atypia have different risks of malignancy and this discrepancy should be communicated by the cytologist and clinicians.
Some authors have confirmed that the vast majority of malignant TNs are solid, and that this was observed in 82%–91% of all TCs.Citation8 Other authors suggest that the presence of microcalcifications, even in a partially cystic TN, definitely increases the risk of malignancy.Citation25 Besides this general agreement, that a purely cystic nodule (without a solid component) has a very low suspicion of malignancy and should be treated as a benign lesion with no need to UG-FNAB,Citation17 in our study we had 2 patients with this type of ultrasound feature. These patients underwent biopsy and provided results which qualified for the AUS/FLUS category. The main indication for surgery in these patients was not the cytology diagnosis of the nodules or ultrasound patterns, but cosmetic reasons. In the histopathology diagnosis, these nodules were classified as a benign colloid goiter.
The incidence and risk of malignancy in the AUS/FLUS category is not very low. Nodules qualifying for the AUS/FLUS category of the TBSRTC system with a high suspicion of malignancy in the ultrasound patterns should undergo diagnostic or therapeutic surgery to either refute or confirm malignancy. However, in the absence of sonographic features associated with malignancy, another appropriate form of clinical management might be observation. Microcalcifications and fast tumor growth could be used as predictive factors for the development of TC in patients with TNs which qualify for the AUS/FLUS category.
Author contributions
All authors contributed toward data analysis, drafting and critically revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
- CibasESAliSZThe Bethesda system for reporting thyroid cytopathologyAm J Clin Pathol2009132565866519846805
- AliSZCibasESThe Bethesda System for Reporting Thyroid CytopathologyNew YorkSpringer2009
- Van der LaanPAMarquseeEKraneJFUsefulness of diagnostic qualifiers for thyroid fine-needle aspirations: with atypia of undetermined significanceAm J Clin Pathol2011136457257721917679
- BongiovanniMSpitaleAFaquinWCMazzucchelliLBalochZWThe Bethesda system for reporting thyroid cytopathology: a meta-analysisActa Cytol201256433333922846422
- OhoriNPSchoedelKEVariability in the atypia of undetermined significance/follicular lesion of undetermined significance diagnosis in the Bethesda system for reporting thyroid cytopathology: sources and recommendationsActa Cytol201155649249822156456
- HagagPStraussSWeissMRole of ultrasound guided fine-needle aspiration biopsy in evaluation of nonpalpable thyroid nodulesThyroid199889899959848711
- HaugenBRAlexanderEKBibleKCAmerican Thyroid Association Management Guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: The American Thyroid Association Guidelines Task Force on thyroid nodules and differentiated thyroid cancerThyroid2016261113326462967
- KwakJYHanKHYoonJHThyroid imaging reporting and data system for US features of nodules: a step in establishing better stratification of cancer riskRadiology2011260389289921771959
- WuWGongXZhouQChenXChenXUltrasound-guided percutaneous microwave ablation for solid benign thyroid nodules: comparison of MWA versus control groupInter J Endocrinol201720179724090
- ChngCLKurzawinskiTRBealeTValue of sonographic features in predicting malignancy in thyroid nodules diagnosed as follicular neoplasm on cytologyClin Endocrinol2015835711716
- KaliszewskiKZubkiewicz-KucharskaAWojtczakBStrutyńska-KarpińskaMZaleska-DorobiszULeśkówEUltrasound guided fine-needle aspiration biopsy of thyroid nodules: does radiologist assistance decrease the rate of unsatisfactory biopsies?Adv Clin Exp Med20162519310026935503
- RenukaIVSaila BalaGAparnaCKumariRSumalathaKThe Bethesda system for reporting thyroid cytopathology: interpretation and guidelines in surgical treatmentIndian J Otolaryngol Head Neck Surg201264430531124294568
- SinghRSWangHHEliminating the “Atypia of Undetermined Significance/Follicular Lesion of Undetermined Significance” category from the Bethesda system for reporting thyroid cytopathologyAm J Clin Pathol2011136689690222095375
- GuoAKaminohYForwardTSchwartzFLJenkinsonSFine needle aspiration of thyroid nodules using the Bethesda system for reporting thyroid cytopathology: an institutional experience in a rural settingInter J Endocrinol201720179601735
- MoonWJJungSLLeeJHBenign and malignant thyroid nodules: US differentiation–multicenter retrospective studyRadiology2008247376277018403624
- MoonHJKwakJYKimMJSonEJKimEKCan vascularity at power Doppler US help predict thyroid malignancy?Radiology2010255126026920308462
- BritoJPGionfriddoMRAl NofalAThe accuracy of thyroid nodule ultrasound to predict thyroid cancer: systematic review and meta-analysisJ Clin Endocrinol Metab20149941253126324276450
- MaiaFFMatosPSPavinEJVassalloJZantut-WittmannDEValue of ultrasound and cytological classification system to predict the malignancy of thyroid nodules with indeterminate cytologyEndocr Pathol2011222667321547508
- BruneseLRomeoAIorioSA new marker for diagnosis of thyroid papillary cancer: B-flow twinkling signJ Ultrasound Med20082781187119418645077
- StaculFBartolottoMDe GobbisFUS, colour-Doppler US and fine-needle aspiration biopsy in the diagnosis of thyroid nodulesRadiol Med2007112575176217657415
- CastroMREspirituRPBahnRSPredictors of malignancy in patients with cytologically suspicious thyroid nodulesThyroid201121111191119822007937
- CaloPGMedasFSanta CruzRFollicular nodules (Thy3) of the thyroid: is total thyroidectomy the best option?BMC Surg2014612
- RenshawAADoes a repeated benign aspirate change the risk of malignancy after an initial atypical thyroid fine-needle aspiration?Am J Clin Pathol201013478879220959662
- NayarRIvanovicMThe indeterminate thyroid fine-needle aspiration: experience from an academic center using terminology similar to that proposed in the 2007 National Cancer Institute Thyroid Fine Needle Aspiration State of the Science ConferenceCancer2009117319520219382174
- KimDWLeeEJInHSKimSJSonographic differentiation of partially cystic thyroid nodules: a prospective studyAJNR Am J Neuroradiol201031101961196620634308