
Abstract
Background
Compared with application of bone-modifying agents (BMAs) every 4 weeks, it is unclear whether 12-weekly de-escalated therapy can be used as a substitute strategy.
Methods
A systematic search of PubMed, EMBASE, and the Cochrane Register of Controlled Trials until November 22, 2017, was performed. Randomized controlled trials (RCTs) were included to assess skeletal-related event (SRE) rates, adverse events, and bone turnover biomarkers, comparing 12-weekly de-escalated treatments with standard 4-weekly dosage regimens. Risk ratios (RRs) with 95% CIs were pooled in fixed-effect meta-analyses.
Results
A total of eight citations were eligible comprising 2,878 patients: zoledronate (three studies, 2,650 patients), pamidronate (two studies, 68 patients), and denosumab (three studies, 160 patients). Summary RR (0.98; 95% CI 0.87–1.12; P=0.82) for SRE rates between de-escalated and standard arms was produced when seven low risk of bias trials (695 patients) were pooled, and results without statistical significance also appeared in the analysis of adverse events and bone turnover biomarkers. Due to the limited sample size and methodological differences, the data for skeletal morbidity rates (SMRs), time to first SRE, serum C-telopeptide (sCTx) levels, and hypocalcemia were not combined, but systematic review still obtained similar indistinguishableness.
Conclusion
In this meta-analysis of randomized clinical trials, the results “appeared” to show non-inferiority of the 12-weekly treatment. Due to the difference in available data, the results for bisphosphonates are more solid than for the receptor activator of nuclear factor-κB ligand (RANKL) antibodies.
Introduction
Approximately 70% of the patients with multiple myeloma or advanced malignant tumors (especially with highest prevalence in breast and prostate cancers) are associated with a common clinical problem of bone metastasis.Citation1 Malignant bone diseases caused by bone metastases can severely damage the stability of normal bones and result in life-limiting skeletal-related events (SREs), including pathological fractures and nerve compression, which may require palliative radiotherapy or bone surgery and can also cause hypercalcemia and a decrease in quality of lifeCitation2–Citation5 or even lead to a higher risk of death.Citation6 Bone-modifying agents (BMAs), including bisphosphonates and receptor activator of nuclear factor-κB ligand (RANKL) inhibitor, can inhibit osteoclast-mediated bone resorption.Citation7 This treatment has been tested to reduce the incidence of skeletal morbidity in patients with bone metastasesCitation8–Citation10 and is widely used clinically. However, the best interval of drug delivery is still controversial.
In general, the dosing interval for BMAs is every 3–4 weeks.Citation11 This dose regimen was developed from studies on hypercalcemia patients and co-administration with standard anti-cancer agents, rather than on convincing pharmacodynamics and contrastive studies.Citation12,Citation13 The pharmacokinetic studies found that terminal half-lives of bisphosphonate and denosumab were both longer.Citation14,Citation15 With the prolongation of the overall survival expectancy of the patients with advanced malignant tumors, the toxic effects may increase gradually with the long accumulation periods of BMAs, primarily manifested in jaw osteonecrosis, renal adverse events, hypocalcemia, and bone pain.Citation16 Therefore, increasing attention has been paid to whether de-escalation dosing could provide the same efficacy as the standard dosage regimen while improving adherence and safety.Citation17
We conducted this research to summarize all available evidence from randomized controlled trial (RCT) studiesCitation18–Citation25 regarding the comparison between 12-weekly de-escalation treatments and standard 4-weekly dosage regimens and to provide a quantitative assessment. If de-escalation shows non- inferiority, its clinical application will undoubtedly reduce the cost of medical treatment and the waste of medical resources.
Methods
The present systematic review was in compliance with PRISMA statementCitation26 and has been registered in the PROS- PERO database (CRD42017083426). A complete PRISMA checklist is provided in .Citation27,Citation28
Research question
The research issues are expressed in the framework of population–intervention–comparator–outcomes-study design (PICOS) as “Comparison of the benefit (skeletal morbidity rate [SMR], SRE, time to first SRE) and harm (osteonecrosis of jaw, renal toxicity, bone pain, hypocalcemia) of BMA administration to cancer patients with bone metastases every 12 weeks or every 4 weeks”.
Literature-search strategy
Under the guidance of the comprehensive and systematic search strategy formulated by evidence-based experts, PubMed, EMBASE, and Cochrane Library were independently searched by two investigators (CL and LW) and updated until November 22, 2017. No filters, limits, and publication date or language restrictions were enforced. Complete search strategies are shown in . To test the sensitivity of the search strategy and find any other relevant publications, reference lists of multiple articles and pertinent reviews were checked manually.
Inclusion and exclusion criteria
The article inclusion criteria applied to the stage 1 review (title and abstract reading) were as follows: 1) cancer patients with bone metastasis; 2) randomized clinical trial; and 3) de-escalated treatment (12-weekly) compared with standard treatment (4-weekly) using the same BMAs. Stage 2 review (full-text reading) inclusion criteria for application were as follows: 1) administration contains 4-weekly dose and 12-weekly dose; 2) included at least one end point of the following: SREs, SMR (which was defined as the number of occurrences of any SRE, allowing for only one event in any 3-week interval, divided by the time at risk in years), time to first on-study SRE, adverse events, serious adverse events (SAEs), renal adverse events, osteonecrosis of the jaw, cardiac events, bone pain, radiation to bone, gastrointestinal events, hypocalcemia, or bone turnover marker (urine N-telopeptide [uNTx] or urine N-telopeptide corrected for creatinine [uNTx/Cr] or serum C-telopeptide [sCTx]).
The exclusion criteria were as follows: 1) conference abstracts or 2) not treated with same BMAs or contained different doses in two arms. If data from the same study cohort resulted in more than one publication, data for different outcomes were required to be included, whereas if the results were the same, the most recent or complete report was used to prevent the duplication of data from patients from one cohort.
Data extraction and study quality assessment
Two authors independently performed data extraction and quality assessment, disagreements were resolved by consensus, and a third senior author was consulted when necessary. For all standard research, data collection was performed using a predefined standardized grid (), including the following entries: first author, year of publication, country, study design information, sample size, mean age, patient inclusion criteria, outcomes assessed, duration, industry funded, and study status. Specific outcomes were separately collected and are shown in , including SRE, adverse events, SAEs, renal adverse events, osteonecrosis of the jaw, bone pain, radiation to bone, and bone turnover marker (reduction of uNTx).
Table 1 Characteristics of included studies in the meta-analysis
Table 2 Meta-analysis results for end points
Cochrane Collaboration’s assessment toolCitation29 was used to assess the risk of bias, and special attention was paid to the following items that usually represent the quality of the RCT:Citation30 random sequence generation, allocation concealment, blinded (participants, personnel and outcome assessment), incomplete outcome data, free of selective reporting, and free of other bias.
Data analyses
Meta-analysis was performed where enough data were available. Binary outcomes were synthesized using risk ratio (RR). All summary estimates were reported with point estimates and corresponding 95% CIs. If data were considered unsuitable for meta-analysis based on study characteristics, a narrative approach to summary of study-specific results was employed. The statistical heterogeneity across studies was assessed using the Cochran Q and I2 statistics with significance defined as Q test ≤0.10 or I2 >50%.Citation31 The random- effects model was selected as a result of the existence of significant heterogeneity; if not, the fixed-effect model was performed to combine results. Due to the limitations of available data, sensitivity or subgroup analyses were not executed. The analyses described earlier were implemented through Review Manager 5.3 (Cochrane Collaboration, Oxford, UK).
Results
Search results
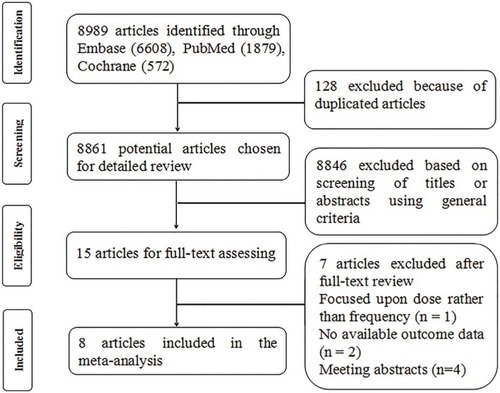
The flow diagram illustrates the identification process of electronic search and study selection based on eligible and excluded trials (). Our systematic literature search identified 8,989 potentially relevant publications; after duplicate removal and the first screening of titles and abstracts, 8,974 were excluded. We had a full review for the remaining 15 records, of which seven articles were excluded: oneCitation32 focused upon zoledronate dose rather than dose frequency, oneCitation33 did not include necessary outcomes, oneCitation34 focused on the comparison with denosumab and bisphosphonate, while not providing separate data from each subgroup, and fourCitation35-38 were published as meeting abstracts without end point data. Eventually, eight publications were identified for the meta-analysis.
Figure 1 Flow chart of article screening and selection process.
Study and patients’ characteristics
The characteristics and data extraction of qualified studies included in the meta-analysis are summarized in and . The age of participants across studies ranged from 55 to 65 years. A total of 2,878 participants from eight RCTs were included. Among the studies, threeCitation18–Citation20 studies evaluated reduced-frequency dosing treatment with zoledronate, twoCitation21,Citation22 with pamidronate, and threeCitation23–Citation25 with denosumab.
Two of the studiesCitation19,Citation24 involved a series of malignancies with bone metastasis including breast cancer, prostate cancer, and multiple myeloma, and the rest were breast cancer as the main research object.Citation18,Citation20–Citation23,Citation25 Two articles,Citation23,Citation25 respectively, reported the results of a study by Lipton et al at different time points (13 and 25 weeks), so the data extracted from the two were considered attributable to the same study. In addition, of all the articles included, two studies were published in 2017,Citation19,Citation20 two in 2013,Citation18,Citation22 one in 2014,Citation21 and three between 2007 and 2009.Citation23–Citation25 In terms of experimental design, the dose and frequency were consistent across studies using zoledronate (4 mg), pamidronate (90 mg), and denosumab (180 mg) every 4 weeks vs every 12 weeks.
Quality assessment
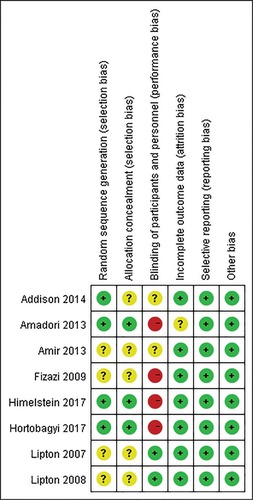
All included articlesCitation18–Citation25 were evaluated for risk bias using the Cochrane Collaboration tools. Four studiesCitation18–Citation20,Citation24 were considered high risk of bias in blinding of the outcome assessment field. Although other articles also showed an uncertain risk of bias in several fields, overall, the majority of RCTs exhibited lower risk of bias ().
Figure 2 Risk of bias assessment.
Note: Green represents low risk of bias; red represents high risk of bias; and yellow represents unclear risk of bias.
Findings – SREs
The included studies reported multiple outcome estimates related to the risk of SREs comparing de-escalated with standard dose, including the SRE rate (the proportion of patients with at least one SRE on study),Citation18–Citation25 the time to first on-study SRE,Citation19,Citation20 and the SMR.Citation18,Citation20
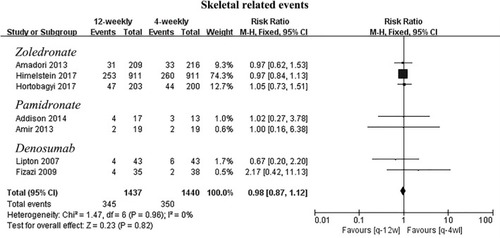
As shown in , data for the SRE rates were available in all the included studies. The combined RRs showed that de-escalated was not superior to the standard arm in SRE rates (RR 0.98; 95% CI 0.87–1.12; P=0.82) with no significant heterogeneity (I2=0%; P=0.96).
Figure 3 Meta-analysis results for skeletal-related events.
Among the ZOOM study,Citation18 the SMR ratio (4-weekly arm vs 12-weekly arm) was 0.97 (95% CI 0.60–1.57; P=0.896). In addition, the mean (SD) SMR was 0.50 (1.50) and 0.46 (1.06) events annually for de-escalated vs the standard arm in the OPTIMIZE-2 study.Citation20 Both findings suggested that the 12-weekly de-escalated was not inferior to the 4-weekly treatment. Regarding the time to first SRE, there was no statistically significant difference between treatment arms (HR 1.06; 95% CI 0.70–1.60; P=0.79) for OPTIMIZE-2.Citation20 Median times to first SRE were also reported by Himelstein et al,Citation19 which were 15.7 vs 16.8 (4-weekly arm vs 12-weekly arm). As a result of the differences in data type, no consolidation analysis for SMR or time to first SRE was conducted.
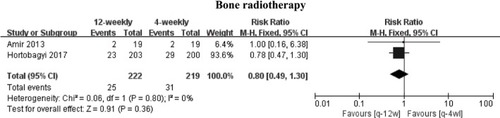
Bone radiotherapy, as one of the important definitions of SRE, was also, respectively, analyzed in two studies (12-weekly arm: 25 events; 4–weekly arm: 31 events).Citation20,Citation22 Differences with no statistical significance between the two arms are shown in the pooled analysis (RR 0.80; 95% CI 0.49–1.30; P=0.36) ().
Figure 4 Meta-analysis results for bone radiotherapy.
Finding – adverse events
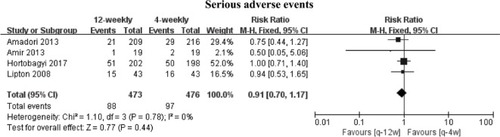
A series of data of side effects and toxicities were analyzed. Overall, AEs occurred in 802 patients (12-weekly arm: 389 events; 4-weekly arm : 413 events) and SAEs occurred in 185 patients (12-weekly arm: 88 events; 4-weekly arm: 97 events). Summary RRs were produced, respectively, RR 0.96 (95% CI 0.89–1.04; P=0.38) for AEs and RR 0.91 (95% CI 0.70–1.17; P=0.44) for SAEs, both were not statistically significant, and high statistical heterogeneity (I2=66%; P=0.05) was observed for AEs ( and ), whereas there was no significant heterogeneity (I2=0%; P=0.78) in SAEs ( and ).
Figure 5 Meta-analysis results for adverse events.
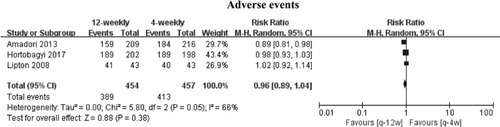
Figure 6 Meta-analysis results for serious adverse events.
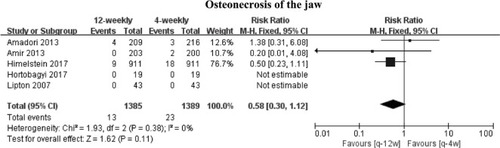
In addition, we conducted a meta-analysis of several common toxic outcomes. The results all showed no statistically significant reductions. Only two studiesCitation18,Citation25 have reported bone pain data, the comparison showed a summary RR of 0.81 (95% CI 0.42–1.55; P=0.52) between de-escalated (15 events) and standard (19 events) arms, and low statistical heterogeneity was found (I2=0%; P=0.71) (). Data for renal adverse events were available from four studies.Citation18–Citation20,Citation22 Similar indifference was found (RR 0.67; 95% CI 0.39–1.16; P=0.15) between de-escalated (21 events) and standard (31 events) arms with low statistical heterogeneity (I2=0%; P=0.55) (). Five studiesCitation18–Citation20,Citation22,Citation23 provided available data for osteonecrosis of the jaw, but only threeCitation18–Citation20 were included in the meta-analysis for the presence of 0 events in both groups.Citation22,Citation23 Comparison showed a summary RR of 0.58 (95% CI 0.30–1.12; P=0.11) between de-escalated (1,385 events) and standard (1,389 events) arms, and low statistical heterogeneity was observed (I2=0%; P=0.38) (). Finally, we did not carry out meta-analysis for hypocalcemia because there was only one set of available data. The researchCitation19 showed that regardless of any grade of hypocalcemia or grade 4 hypocalcemia, no significant differences existed between the 4-weekly group and the 12-weekly group.
Figure 7 Meta-analysis results for bone pain.
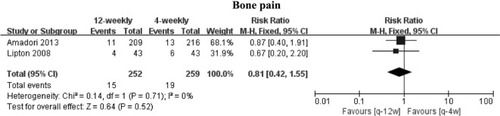
Figure 8 Meta-analysis results for renal adverse events.
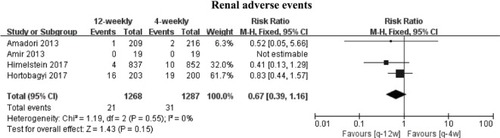
Figure 9 Meta-analysis results for osteonecrosis of the jaw.
Finding – bone turnover biomarkers
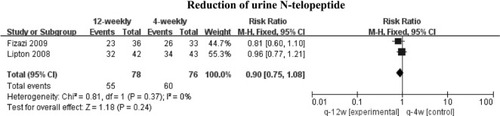
The study of Amadori et alCitation18 provided a significant increase in the N-terminal telopeptide concentration in the 12-weekly group vs 4-weekly group from 6 months (12.2% vs –2.3%; P=0.0111) to 12 months (12.2% vs 0.0%; P=0.0465). However, this open-label result was not reproduced by a double- blind design of Hortobagyi et al.Citation20 When we gathered the other available data,Citation24,Citation25 no statistically significant results (RR 0.90; 95% CI 0.75–1.08; P=0.37) were obtained ().
Figure 10 Meta-analysis results for reduction of urine N-telopeptide.
The research on sCTx also showed different results. Addison’s researchCitation21 based on the REFORM cohort provided a statistically significant greater increase in sCTx (median of 131 vs 17, P=0.034) when comparing treatment group 2 (12-weekly arm) with group 1 (4-weekly arm). However, the observation point was only at baseline and week 12, when sCTx levels were measured for 48 weeks, the outcome changed (73.7% in control arm; 68.4% in de-escalated arm; P=0.64). No statistical analysis was performed for sCTx due to heterogeneity of the data.
Discussion
Dosing intervals have increasingly been questioned, although the standard application of BMAs is once every 4 weeks, which was obtained from studies of hypercalcemia patients who received anticancer agentsCitation39 and has long been guiding clinical practice.Citation10,Citation40 Terminal treatment of cancer patients, especially palliative care, requires a shift from “problem- based, disease-oriented” care to “goal-oriented, integrated” care. The balance between the long-term use of BMA-related side effectsCitation41 and the therapeutic benefits of advanced cancer patients needs deliberation. Thus, increasing interest is focused on the de-escalated treatment strategies. If curative effects of de-escalation treatment to less frequent dosing is concordant with administration of 4-weekly, it can effectively reduce health care costs and relieve medical pressure.Citation42
The primary outcome is health-related quality of life in this research. The results showed that the 12-weekly deescalated treatment regimen is not inferior to the 4-weekly dosage regimen for patients with bone-metastatic cancer, regardless of whether they had completed the standard 1 year of BMA treatment before, which challenged the current guidelines.Citation43–Citation45 The incidence of SRE is a composite frequently used end point of skeletal complications in patients with bone metastases.Citation46,Citation47 We had observed that the average probability of SREs in different experiments was of great disparity. This finding is not only due to the different frequency requirements for imaging but also because of different decision-making models and treatment thresholds among different clinicians. Although the nature of the SRE is uncertain but still plausible, no statistical significance was shown in the final results between study arms. For frequencies of adverse events and toxicity, although limited to different measuring tools, part of the study of small sample data and not sufficient follow-up time, overall, the results showed non-inferiority of the de-escalated treatment. The role of bone turnover biomarkers as a substitute for subsequent SRE risks is increasingly questioned,Citation48 and it is still a common clinical method used because it is simpler and easier.Citation4,Citation49 The results were observed to be different in these studies, but we observed that with the extension of follow-up time and the increase in sample size, the bone turnover biomarker levels tended to not be different between the two groups. In fact, we do not have much hope for a positive outcome for the de-escalated arms; the end is really the same. However, deescalated scheduling is sufficient to satisfy our predefined definition of non-inferiority. Meanwhile, the limitations of data should be taken into consideration, and its clinical feasibility remains to be verified by large sample experiments. At that time, indiscrimination between the two groups may have a substantial impact on medical decisions.
Since 2000, the American Society of Clinical Oncology (ASCO) guidelines have suggested the use of BMAs indefinitely.Citation16 For this long-term treatment model, a larger interval of medication will undoubtedly reduce the cost for patients. Actually, the current guidelines recommend a “one size fits all” approach.Citation50 It is suggested that all patients receive the same dose and frequency of BMAs, regardless of their potential risks or needs, which is obviously unreasonable in the current era of personalized medicine. For example, with different pharmacokinetic and efficacy properties, denosumab, as a new bisphosphonate alternative drug,Citation51 was invariably observed to be marginally more effective than zoledronate in preventing SREs and improving quality of life.Citation52,Citation53 Meanwhile, excellent effectiveness brings a considerable extra cost. The study of Shapiro et alCitation54 has shown that the mean cost of the treatment strategy is nine-fold higher for denosumab than generic zoledronate every 3 months. Therefore, making appropriate treatment strategies is a test to clinicians. What is important is to limit medical waste and economic loss caused by the overuse of the treated individuals while guaranteeing their health and rights.
There are several limitations to this study that should be mentioned, as well. First, the study contained different BMA types and the duration of BMAs used before enrollment and did not always report common clinical end points. Therefore, certain studies tend to play a dominant role in inherently few research samples when carrying out a specific end point summary analysis. Second, the duration of BMAs in these studies is noteworthy, because the life expectancy of partial cancer patients with bone metastases may be close to or shorter than the median length of follow-up of these studies, especially for the special group of elderly patients.Citation55 Additionally, with the aggravation of the disease, the loss of follow-up becomes common. Both may lead to inability to fully evaluate the relationship between exposure and outcome. In addition, our research only included the patients with breast cancer, prostate cancer, and multiple myeloma, although bone metastases are common in many types of cancers.Citation56 Several studies (NCT02051218; NCT00320710; NCT00320710; and NCT02721433) have not included other types of cancer patients as well. Therefore, whether the results can be generalized to other types of cancers is still uncertain and needs further investigation. What has to be further mentioned is that the sample size is very limited, especially for RANKL inhibitor. This may result in the instability, even false positive rate, of the outcomes to a certain extent. Despite these limitations, it is worth noting that there is consistency in all trial results. There were no signs of significant differences between the de-escalation and control arms for different BMAs used and outcome events.
Conclusion
After summarizing and analyzing all available data obtained to date, there appears to be no difference in outcomes between 12-weekly de-escalated therapy and 4-weekly dosage regimen. The longer-interval dose is a better choice, both from a health care resource perspective and a financial perspective. It is important to determine whether each type of cancer can benefit from this and whether the high heterogeneity of SRE risk among different individuals is suitable for unified Clinical Governance. Further precision research is needed in the future to adequately advise clinicians and patients on the optimal dosage regimen of BMAs in various clinical settings.
Acknowledgments
This study was supported by the National Natural Science Foundation of China (grant number: 81473513).
Supplementary materials
Table S1 PRISMA checklist
Table S2 Search strategy
Author contributions
The research project was designed by Cun Liu, Lu Wang, and Changgang Sun; organized by Cun Liu, Lu Wang, Lijuan Liu, Jing Zhuang, Shifeng Tang, Fubin Feng, Jinmei Zhang, and Tingting Zhang; and executed by Cun Liu and Lu Wang. Statistical analysis was designed by Cun Liu, Lu Wang, Tiansong Zhang, Chundi Gao, and Huayao Li; executed by Cun Liu, Lu Wang, Tiansong Zhang, Fubin Feng, Tingting Zhang, and Jia Li; and reviewed and critiqued by Changgang Sun, Lijuan Liu, Chao Zhou, Ruijuan Liu, and Jinmei Zhang. The first draft of the manuscript was written by Cun Liu and Lu Wang, and the manuscript was reviewed and critiqued by Lijuan Liu, Tiansong Zhang, and Changgang Sun. All authors contributed toward data analysis, drafting and critically revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
- HofbauerLCRachnerTDColemanREJakobFEndocrine aspects of bone metastasesLancet Diabetes Endocrinol20142650051224880565
- Clément-DemangeLClézardinPEmerging therapies in bone metastasisCurr Opin Pharmacol201522798625935860
- BrownJECookRJMajorPBone turnover markers as predictors of skeletal complications in prostate cancer, lung cancer, and other solid tumorsJ Natl Cancer Inst2005971596915632381
- BrownJEThomsonCSEllisSPGutcherSAPurohitOPColemanREBone resorption predicts for skeletal complications in metastatic bone diseaseBr J Cancer200389112031203714647134
- Gómez GarcíaSClemonsMAmirERethinking end-points for bone- targeted therapy in advanced cancerEur J Cancer20166310510927299662
- SaadFLiptonACookRChenYMSmithMColemanRPathologic fractures correlate with reduced survival in patients with malignant bone diseaseCancer200711081860186717763372
- GreenJRMüllerKJaeggiKAPreclinical pharmacology of CGP 42’446, a new, potent, heterocyclic bisphosphonate compoundJ Bone Miner Res1994957457518053405
- ColemanREBisphosphonates: clinical experienceOncologist20049Suppl 41427
- ClemonsMGelmonKAPritchardKIPatersonAHBone-targeted agents and skeletal-related events in breast cancer patients with bone metastases: the state of the artCurr Oncol201219525926823144574
- HolenIColemanREBisphosphonates as treatment of bone metastasesCurr Pharm Des201016111262127120166976
- HuttonBAddisonCMazzarelloSDe-escalated administration of bone-targeted agents in patients with breast and prostate cancer-A survey of Canadian oncologistsJ Bone Oncol201322778326909274
- HortobagyiGNTheriaultRLPorterLEfficacy of pamidronate in reducing skeletal complications in patients with breast cancer and lytic bone metastases. Protocol 19 Aredia Breast Cancer Study GroupN Engl J Med199633524178517918965890
- HenryDHCostaLGoldwasserFRandomized, double-blind study of denosumab versus zoledronic acid in the treatment of bone metastases in patients with advanced cancer (excluding breast and prostate cancer) or multiple myelomaJ Clin Oncol20112991125113221343556
- CremersSCPapapoulosSEGelderblomHSkeletal retention of bisphosphonate (pamidronate) and its relation to the rate of bone resorption in patients with breast cancer and bone metastasesJ Bone Miner Res20052091543154716059626
- DoshiSSutjandraLZhengJDenosumab dose selection for patients with bone metastases from solid tumorsClin Cancer Res20121892648265722394983
- van PoznakCSomerfieldMRBarlowWERole of Bone- Modifying Agents in Metastatic Breast Cancer: An American Society of Clinical Oncology-Cancer Care Ontario Focused Guideline UpdateJ Clin Oncol201735353978398629035643
- BouganimNDranitsarisGAmirEClemonsMOptimising the use of bone-targeted agents in patients with metastatic cancers: a practical guide for medical oncologistsSupport Care Cancer201119111687169621785900
- AmadoriDAgliettaMAlessiBEfficacy and safety of 12-weekly versus 4-weekly zoledronic acid for prolonged treatment of patients with bone metastases from breast cancer (ZOOM): a phase 3, open- label, randomised, non-inferiority trialLancet Oncol201314766367023684411
- HimelsteinALFosterJCKhatcheressianJLEffect of Longer- Interval vs Standard Dosing of Zoledronic Acid on Skeletal Events in Patients With Bone Metastases: A Randomized Clinical TrialJAMA20173171485828030702
- HortobagyiGNvan PoznakCHarkerWGContinued Treatment Effect of Zoledronic Acid Dosing Every 12 vs 4 Weeks in Women With Breast Cancer Metastatic to Bone: The OPTIMIZE-2 Randomized Clinical TrialJAMA Oncol20173790691228125763
- AddisonCLPondGRZhaoHEffects of de-escalated bisphosphonate therapy on bone turnover biomarkers in breast cancer patients with bone metastasesSpringerplus2014357725332877
- AmirEFreedmanOCarlssonLRandomized feasibility study of de-escalated (every 12 wk) versus standard (every 3 to 4 wk) intravenous pamidronate in women with low-risk bone metastases from breast cancerAm J Clin Oncol201336543644222781385
- LiptonAStegerGGFigueroaJRandomized active-controlled phase II study of denosumab efficacy and safety in patients with breast cancer-related bone metastasesJ Clin Oncol200725284431443717785705
- FizaziKLiptonAMarietteXRandomized phase II trial of denosumab in patients with bone metastases from prostate cancer, breast cancer, or other neoplasms after intravenous bisphosphonatesJ Clin Oncol200927101564157119237632
- LiptonAStegerGGFigueroaJExtended efficacy and safety of denosumab in breast cancer patients with bone metastases not receiving prior bisphosphonate therapyClin Cancer Res200814206690669618927312
- LiberatiAAltmanDGTetzlaffJThe PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaborationBMJ2009339b270019622552
- KnoblochKYoonUVogtPMPreferred reporting items for systematic reviews and meta-analyses (PRISMA) statement and publication biasJ Craniomaxillofac Surg2011392919221145753
- ShamseerLMoherDClarkeMPreferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanationBMJ2015350g764725555855
- HigginsJPAltmanDGGøtzschePCThe Cochrane Collaboration’s tool for assessing risk of bias in randomised trialsBMJ2011343d592822008217
- ChanKKGlennyAMWeldonJCFurnessSWorthingtonHVWakefordHInterventions for the treatment of oral and oropharyngeal cancers: targeted therapy and immunotherapyCochrane Database Syst Rev20151212CD010341
- SongFSheldonTASuttonAJAbramsKRJonesDRMethods for exploring heterogeneity in meta-analysisEval Health Prof200124212615111523383
- BerensonJRRosenLSHowellAZoledronic acid reduces skeletal-related events in patients with osteolytic metastasesCancer20019171191120011283917
- KuchukIBeaumontJLClemonsMAmirEAddisonCLCellaDEffects of de-escalated bisphosphonate therapy on the Functional Assessment of Cancer Therapy-Bone Pain, Brief Pain Inventory and bone biomarkersJ Bone Oncol20132415415726909286
- BodyJJLiptonAGralowJEffects of denosumab in patients with bone metastases with and without previous bisphosphonate exposureJ Bone Miner Res201025344044619653815
- ColemanREWrightJHoustonSRandomized trial of marker- directed versus standard schedule zoledronic acid for bone metastases from breast cancerJ Clin Oncol20123015 Suppl511
- AmirEFreedmanOCarlssonLP4-16-08: Pilot Randomized Trial of De-Escalated (q12 Weekly) Versus Standard (q3-4 Weekly) Intravenous Bisphosphonates in Women with Low-Risk Bone Metastases from Breast CancerCancer Res20117124 Suppl P4-16-08P4-16-08-P4-16-08
- TempletonAJStalderLAlbiges SauvinLPrevention of symptomatic skeletal events with denosumab administered every 4 weeks versus every 12 weeks: A noninferiority phase III trial (SAKK 96/12, REDUSE)Ann Oncol201425Suppl 4iv540iv541
- BodyJFizaziKStegerGGEffects of denosumab on bone turnover: Results from two randomized phase 2 trials in patients with solid tumorsAnn Oncol200819S8viii275viii276
- KimmelDBMechanism of action, pharmacokinetic and pharmacodynamic profile, and clinical applications of nitrogen-containing bisphosphonatesJ Dent Res200786111022103317959891
- KuchukIMazzarelloSButterfieldKAppletonAAddisonCLClemonsMOral care and the use of bone-targeted agents in patients with metastatic cancers: A practical guide for dental surgeons and oncologistsJ Bone Oncol201321384626909271
- MariottiABisphosphonates and osteonecrosis of the jawsJ Dent Educ200872891992918676801
- XieJDienerMSorgRWuEQNamjoshiMCost-effectiveness of denosumab compared with zoledronic acid in patients with breast cancer and bone metastasesClin Breast Cancer201212424725822694824
- National Comprehensive Cancer Network (NCCN) [homepage on the Internet]Clinical Practice Guidelines in OncologyBreast Cancer Version 22017Accessed September 6, 2018 https://www.nccn.org/professionals/physician_gls/default.aspx
- National Comprehensive Cancer Network (NCCN) [homepage on the Internet]Clinical Practice Guidelines in OncologyMultiple Myeloma Version 32017 https://www.nccn.org/professionals/physician_gls/default.aspxAccessed September 6, 2018
- National Comprehensive Cancer Network (NCCN) [homepage on the Internet]Clinical Practice Guidelines in OncologyProstatic cancer Version 22017 https://www.nccn.org/professionals/physician_gls/default.aspxAccessed September 6, 2018
- MajorPPCookREfficacy of bisphosphonates in the management of skeletal complications of bone metastases and selection of clinical endpointsAm J Clin Oncol2002256 Suppl 1S10S1812562046
- HussainAAlyADaniel MullinsCQianYArellanoJOnukwughaERisk of skeletal related events among elderly prostate cancer patients by site of metastasis at diagnosisCancer Med20165113300330927730756
- ClampADansonSNguyenHColeDClemonsMAssessment of therapeutic response in patients with metastatic bone diseaseLancet Oncol200451060761615465464
- ColemanRCostaLSaadFConsensus on the utility of bone markers in the malignant bone disease settingCrit Rev Oncol Hematol201180341143221411334
- KuchukIClemonsMAddisonCTime to put an end to the “one size fits all” approach to bisphosphonate use in patients with metastatic breast cancer?Curr Oncol2012195e303e30423144577
- LaceyDLTimmsETanHLOsteoprotegerin ligand is a cytokine that regulates osteoclast differentiation and activationCell19989321651769568710
- ZhangZPuFShaoZThe skeletal-related events of denosumab versus zoledronic acid in patients with bone metastases: A meta-analysis of randomized controlled trialsJ Bone Oncol20179212429123990
- ZhangXHamadehISSongSOsteonecrosis of the Jaw in the United States Food and Drug Administration’s Adverse Event Reporting System (FAERS)J Bone Miner Res201631233634026288087
- ShapiroCLMoriartyJPDusetzinaSCost-Effectiveness Analysis of Monthly Zoledronic Acid, Zoledronic Acid Every 3 Months, and Monthly Denosumab in Women With Breast Cancer and Skeletal Metastases: CALGB 70604 (Alliance)J Clin Oncol201735353949395529023215
- BodyJJColemanRClezardinPInternational Society of Geriatric Oncology (SIOG) clinical practice recommendations for the use of bisphosphonates in elderly patientsEur J Cancer200743585285817258449
- ColemanREMetastatic bone disease: clinical features, pathophysiology and treatment strategiesCancer Treat Rev200127316517611417967