
Abstract
Purpose
To identify potential risk factors of lymph node metastasis and to verify the prognostic significance of the lymph node ratio (LNR) and the total number of lymph nodes examined (NNE) in tracheobronchial adenoid cystic carcinoma (ACC) patients, using a large population-based database.
Patients and methods
From Surveillance, Epidemiology, and End Results database, we identified 263 patients with tracheobronchial ACC in whom complete lymph node data could be obtained. Logistic regression analysis was performed to determine predictive factors of nodal metastasis. X-tile software determined the optimal cut-off points for LNR and NNE. Kaplan– Meier analyses and Cox regression models were adopted for survival analysis.
Results
Of 263 patients, 75 (28.5%) had lymph node involvement. Tumors of bronchial origin (P<0.001) and tumors larger than 30 mm (P<0.001) were associated with a higher likelihood of nodal involvement. Examination of more than ten lymph nodes could avoid understaging and resulted in improved survival; meanwhile, patients with a LNR of 0.07 or less had favorable prognosis.
Conclusion
Patients with tracheobronchial ACC have significant risk of lymph node metastasis. Bronchial ACC and larger tumor size are both risk factors of lymph node metastasis. LNR and NNE may provide a more precise prediction of survival and could be taken into account in future clinical work.
Introduction
Adenoid cystic carcinoma (ACC), mostly found in the salivary gland of the neck and head, is an aggressive and rare malignancy with distinct clinicopathological features.Citation1 ACC in the airway originates from the submucosa glands distributed among the tracheobronchial tree, representing merely 0.04%–0.2% of all pulmonary malignancies.Citation2 Patients usually presented with clinical symptoms of chronic airway obstruction, including cough, chest pain, dyspnea, and hemoptysis, and there was commonly a long interval from the onset of clinical symptoms to final diagnosis.Citation1,Citation3,Citation4 Although researchers have defined this rare disease as an indolent low-grade adenocarcinoma, it has a high tendency for perineural invasion, distant metastasis, and local recurrence.Citation5,Citation6
The rate of nodal metastasis in patients with tracheobronchial ACC ranges from 18.2% to 35.3%, and nodal metastasis was defined as a negative prognostic factor.Citation1,Citation7–Citation11 In the past few years, close attention has been given to lymph node ratio (LNR) and the total number of lymph nodes examined (NNE), both of which were identified as more powerful prognostic factors.Citation12–Citation16 For example, Japanese researchers have reported the superiority of LNR-based subgroup analysis of lymph nodes in surgically treated gastrointestinal cancer.Citation13 In addition, several studies have demonstrated the fact that survival rate increased as more lymph nodes were examined after distal pancreatectomy for pancreatic adenocarcinoma.Citation15 As far as we know, no previous research has evaluated factors predictive of nodal metastasis and the impact of LNR and NNE on survival in patients diagnosed with ACC of the tracheobronchial tree. The goal of our study was to seek potential predictors of nodal metastasis and to determine whether LNR and NNE were associated with prognosis in tracheobronchial ACC, using a large population-based database.
Materials and methods
Surveillance, epidemiology, and end results database
Data were extracted from the US National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) program. Since 1973, SEER database has gradually developed from the previous nine to the current 18 registries which covers ~26% of the US population. The November 2017 update was utilized in our research, providing data on tumor characteristics, patient demographics, and vital status from 1973 to 2015.Citation17 Since none of the protocols involved raw data collection and the patient data were anonymized and openly accessible, Institutional Review Board approval was not needed for our study.
Data acquisition and statistical analysis
From SEER database, all cases with microscopically confirmed ACC in the tracheobronchial tree were selected using the International Classification of Disease for Oncology, Third Edition (ICD-O-3) code 8200/3 and tumor site codes C33.9–C34.9. Patients were eliminated from this analysis if they were diagnosed by autopsy only or death certificate only, did not have active follow-up, or had incomplete lymph node data.
The baseline patient demographics and tumor characteristics were collected including tumor primary site, ethnicity, age at diagnosis, sex, tumor stage, tumor size, treatment modality, NNE, number of positive lymph nodes, cause-specific classification of death, and survival months. Cancer staging criteria has changed greatly in the past decades. TNM stage has been brought into SEER database since 2004. Considering “SEER historic stage” covered the entire study period, we adopted it to group patients in term of tumor stage. LNR was defined as the ratio between the total number of metastatic lymph nodes and the total number of examined lymph nodes.
The SEER*Stat version 8.3.5 (National Cancer Institute, Bethesda, MD, USA) was used to extract clinicopathological data from the SEER database. All statistical analysis was conducted on SPSS version 22 (IBM Corporation, Armonk, NY, USA). X-Tile software (https://medicine.yale.edu/lab/rimm/research/software.aspx) was used to identify the potential cut-off points for LNR and NNE based on minimal P-value method.Citation18 Continuous variables were presented as median (interquartile range), while categorical variables were expressed as frequency (percentage). Univariate and multivariate binary logistic regression analyses were conducted to determine the risk factors of lymph node metastasis. The primary outcome variable was disease-specific survival (DSS), which was defined as the time from cancer diagnosis to death specific to cancer-associated death. Survival curves were plotted using Kaplan–Meier analyses and the difference in survival was determined by log-rank tests. Univariate and multivariate Cox proportional hazards regression methods were performed to identify the prognostic significance of LNR and NNE. All statistical analyses were two-sided, and a P-value <0.05 was considered statistically significant.
Results
Patient characteristics
shows the clinicopathological features of 263 patients who were incorporated in this research. There were 138 women (52.5%) and 125 men (47.5%) with a median age of 55 years (IQR, 47–67). Median tumor size was 30 mm (IQR, 20–42). Race distribution of this cohort was skewed with 214 whites (81.4%), 31 other races (11.8%), and 18 blacks (6.8%). Patients with localized or regional stage disease accounted for 38.8% and 54.1%, respectively, whereas merely 7.1% had distant metastases. Overall, 75 of 263 patients (28.5%) had lymph node metastasis. One hundred and twenty-six patients (47.9%) received surgery with radiotherapy, while 137 (52.1%) were treated with surgical therapy alone. The median follow-up time was 65 months (IQR, 26–110).
Table 1 Patient characteristics
Factors predictive of lymph node metastasis
To identify risk factors of nodal metastasis, we conducted logistic regression analyses (). On univariate analysis, tumors of bronchial origin (OR, 3.209; 95% CI, 1.772–5.821; P<0.001) and larger tumor size (OR, 2.860; 95% CI, 1.602–5.107; P<0.001) were important predictors of lymph node involvement, whereas age, sex, race, and marriage status were not. In a multivariate model, ACCs originating from bronchus (OR, 2.847; 95% CI, 1.553–5.218; P=0.001) and tumors larger than 30 mm (OR, 2.502; 95% CI, 1.381–4.534; P=0.003) were associated with increased risk of lymph node involvement.
Table 2 Univariate and multivariate analyses of risk factors associated with lymph node metastasis
Survival analysis
According to the optimal cut-off analyses using X-tile program, 0.07 was applied as the optimal cut-off value for LNR. Kaplan–Meier analyses demonstrated that patients with a LNR of 0.07 or less had improved DSS compared with those with a LNR of greater than 0.07 (5-year DSS, 81.7% vs 60.9%; median survival, 141 months vs 100 months; P=0.002; ).
Figure 1 Disease-specific survival of patients stratified by (A) LNR, (B) NNE, (C) tumor location, and (D) treatment modality.
Abbreviations: LNR, lymph node ratio; NNE, the total number of lymph nodes examined.
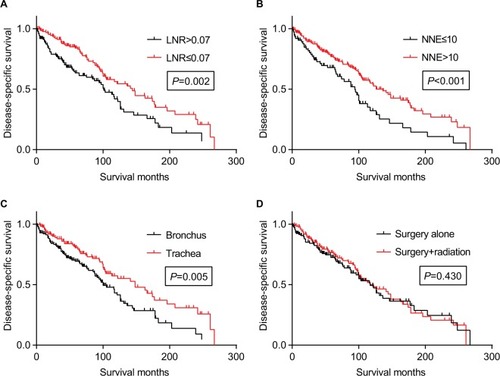
Analyses using X-tile software determined a direct association between increasing NNE and better DSS and identified 10 as the optimal cutoff node count. Patients with >10 dissected lymph nodes were associated with better DSS compared with those with 1–10 dissected lymph nodes (5-year DSS, 75.2% vs 63.8%; median survival, 136 months vs 94 months; P<0.001; ). Moreover, we calculated the lymph node positivity rate in each group. The results demonstrated that the rate of node positivity was 40.8% for patients with >10 dissected lymph nodes, which was higher than patients with 1–10 dissected lymph nodes (27.5%).
As regards to the origin location, bronchial ACC was associated with worse DSS than their tracheal counterpart (5-year DSS, 66.4% vs 78.6%; median survival, 100 months vs 148 months; P=0.005; ). However, patients who received adjuvant radiotherapy did not demonstrate any survival benefit compared with patients who underwent surgery alone (5-year DSS, 72.1% vs 69.8%; median survival, 117 months vs 116 months; P=0.430; ).
shows the prognostic factors associated with DSS according to the Cox regression model. We included age, sex, ethnicity, marital status, tumor location, SEER stage, tumor size, LNR, NNE, and treatment modality to conduct univariate Cox regression analysis. Multivariate Cox regression model identified several negative prognostic factors, including other marital status (HR, 1.719; 95% CI, 1.079–2.740; P=0.023), advanced stage (HR, 2.069; 95% CI, 1.210–3.540; P=0.008 for regional and HR, 2.661; 95% CI, 1.138–6.220; P=0.024 for distant), LNR >0.07 (HR, 1.591; 95% CI, 1.098–2.306; P=0.014), and NNE ≤10 (HR, 1.688; 95% CI, 1.169–2.438; P=0.005).
Table 3 Univariate and multivariate analyses of prognostic factors for disease-specific survival
Discussion
In the past few years, a variety of studies have clarified the prognostic significance of NNE and LNR in a wide range of malignancies, such as gastrointestinal cancer,Citation12,Citation13 kidney cancer,Citation16 and oral cancer.Citation19 Instead of simply classifying patients according to the anatomic site of metastatic lymph nodes, the LNR provides information concerning the total number of metastatic lymph nodes, and at the same time, it provides an assessment of the thoroughness of lymph node dissection. Although it is generally believed that removal of more lymph nodes would contribute to more accurate nodal staging, the efficacy of sampling more lymph nodes remains unclear. Moreover, the impact of LNR on ACC of the tracheobronchial tree still needs to be confirmed. In this study, we identified both NNE and LNR as important predictors of DSS, using a large population-based database. NNE and LNR remained crucial prognosticators, even after controlling for patient demographics features. Our present study of tracheobronchial ACC revealed that dissection of more than ten lymph nodes could avoid understaging and resulted in improved DSS. Furthermore, compared with those with a lower LNR, patients with a LNR greater than 0.07 had decreased DSS.
The overall rate of lymph node involvement in this study was 28.5%, which corresponded to a previous study conducted by Honings et al, who reported a rate of 26% in surgically treated tracheal ACC.Citation20 Unfortunately, current diagnostic procedures are not capable of predicting lymph nodes metastasis, emphasizing the significance of descriptive data to evaluate risk factors of nodal metastasis. Our results showed that tumors of bronchial origin and tumors larger than 30 mm were associated with a higher likelihood of nodal involvement. Megwalu et al analyzed the risk of nodal metastasis in major salivary gland and also demonstrated that larger tumor size was correlated with an increased risk of nodal metastasis.Citation21 In clinical practice, when preoperative imaging examinations reveal the risk factors described earlier, surgeons should maintain a high index of suspicion for lymph node metastasis and manage to perform adequate lymph node dissection. Our current study also noted that the node positivity rate increased as more lymph nodes were harvested, so that the risk of understaging would be reduced in patients with at least ten lymph nodes dissected. Nevertheless, the quality of lymph node dissection not only relies on surgeon’s skill in lymphadenectomy but also depends on pathologist’s proficiency in lymph node examination. Considering an adequate lymph node dissection is influenced by several uncontrollable factors and the method of lymph node examination varies among different medical centers, we suggest that surgeons should work in close collaboration with pathologists to improve the quality of patient’s health care.
In a retrospective study led by Zhao et al, compared with tracheal ACC, ACC originating from bronchus was associated with a higher likelihood of nodal involvement and decreased disease-free survival.Citation22 This is consistent with our series which indicated that tumors of bronchial origin were important predictors of lymph node metastasis and had poor prognosis. Although there was a remarkable difference in prognosis between tracheal and bronchial ACC in univariate analysis, ACC in the bronchus was not an independent prognostic factor when other confounding variables were adjusted in the multivariate model. As previously reported, systematic lymph node dissection was usually avoided in order to protect the blood supply of trachea in patients undergoing surgery for ACC of tracheal origin,Citation23 which would result in inadequate lymph node sampling and potentially influence the survival. We recommend that surgeons should try to capture all of the apparently enlarged lymph nodes, while pathologists are supposed to carefully observe serial sections of the trachea specimens and comprehensively examine for metastatic lymph nodes. Furthermore, the mechanism of tumorigenesis of these two types of ACC may vary noticeably by origin location and future studies regarding the biological behavior of primary airway ACC are essential.
Owing to its low incidence and progression manner, treatment strategies of tracheobronchial ACC remain controversial. Surgical resection is the first choice of therapy whenever possible and an increasing number of studies have addressed the significance of surgery.Citation1,Citation4–Citation6,Citation11,Citation23–Citation26 In light of the fact that this type of tumor is inclined to grow extensively along tracheobronchial tree, radical resection and subsequent tracheobronchoplasty are usually performed during a surgical procedure. As described in several studies, delicate surgical technique and outstanding postoperative care played a vital role in the management of tracheobronchial ACC patients.Citation6,Citation23 Moreover, our team reported the first case of thoracoscopy-assisted circumferential tracheal resection with end-to-end anastomosis for ACC in the trachea and emphasized the significance of collaboration between surgeons and anesthetists.Citation27 Hence, patients are advised to seek help from a tertiary medical center with enough experience in surgical treatment of this disease. Unfortunately, considering the scarcity of this disease, the role of adjuvant radiotherapy remains unclear. Several previous studies demonstrated that adjuvant radiotherapy could provide survival advantage, especially when lymph node metastasis or positive margins existed.Citation28,Citation29 In our study, however, adjuvant radiotherapy did not confer a survival benefit in surgically treated tracheobronchial ACC patients. Meanwhile, other studies also showed no significant elevation in survival rate after adjuvant radiotherapy was carried out.Citation24,Citation26 Thus, recommending adjuvant radiotherapy for surgically treated tracheobronchial ACC patients seems controversial.
The current study also has some limitations, including constraints inherent in the SEER registry and its retrospective design. Detailed information on clinicopathological characteristics such as perineural invasion, margin status, surgical approach, clinical symptoms, physical signs, and dose of radiotherapy are not presented in the SEER program. Patient characteristics such as comorbidities, functional status, and financial ability are also unavailable. Moreover, the total number of examined lymph nodes was correlated with hospital scale and surgeon expertise, but the SEER program only recorded patient’s place of residence, and the levels of hospitals were not reported. And finally, our study results are merely based on bioinformatics study, and an integration of a patient cohort from our institution with a comparison to the SEER data could provide more insight into the research of this very rare disease. Unfortunately, owing to limited number of ACC cases in our institution, we failed to validate the study results from SEER database using our patient cohort. However, unlike prior single-center studies which lacked statistical power, the SEER database made it possible for us to study the prognostic value of NNE and LNR in a rare disease.
Conclusion
Our study reveals that tumors of bronchial origin and larger tumor size are correlated with an increased risk of lymph node involvement in tracheobronchial ACC. In patients undergoing surgery for ACC of the tracheobronchial tree, LNR and NNE are both significant prognostic factors. Examination of more than ten lymph nodes could avoid understaging and result in improved survival; meanwhile, patients with a LNR of greater than 0.07 have poor prognosis. Since LNR and NNE are probably better prognosticators than the nodal staging of the current AJCC TNM staging criteria, in future clinical research, LNR and NNE could be taken into account when stratifying tracheobronchial ACC patients.
Acknowledgments
Our study was supported by the Nature and Science Foundation of Shandong Province (ZR2016HM58). We thank Xinyi Yan for her help in reviewing and editing this article.
Disclosure
The authors report no conflicts of interest in this work.
References
- HuoZMengYWuHAdenoid cystic carcinoma of the tracheobronchial tree: clinicopathologic and immunohistochemical studies of 21 casesInt J Clin Exp Pathol20147117527753525550788
- GaissertHAMarkEJTracheobronchial gland tumorsCancer Control200613428629417075566
- MoranCAPrimary salivary gland-type tumors of the lungSemin Diagn Pathol19951221061227638445
- FalkNWeissferdtAKalhorNMoranCAPrimary pulmonary salivary gland-type tumors: a review and updateAdv Anat Pathol2016231132326645458
- ShimizuJOdaMMatsumotoIAranoYIshikawaNMinatoHClinicopathological study of surgically treated cases of tracheobronchial adenoid cystic carcinomaGen Thorac Cardiovasc Surg2010582828620155344
- MadariagaMLLGaissertHAOverview of malignant tracheal tumorsAnn Cardiothorac Surg20187224425429707502
- ConlanAAPayneWSWoolnerLBSandersonDRAdenoid cystic carcinoma (cylindroma) and mucoepidermoid carcinoma of the bronchus. Factors affecting survivalJ Thorac Cardiovasc Surg1978763369377210333
- MoranCASusterSKossMNPrimary adenoid cystic carcinoma of the lung. A clinicopathologic and immunohistochemical study of 16 casesCancer1994735139013977509254
- MolinaJRAubryMCLewisJEPrimary salivary gland-type lung cancer: spectrum of clinical presentation, histopathologic and prognostic factorsCancer2007110102253225917918258
- KangDYYoonYSKimHKPrimary salivary gland-type lung cancer: surgical outcomesLung Cancer201172225025420884075
- LeeJHJungEJJeonKTreatment outcomes of patients with adenoid cystic carcinoma of the airwayLung Cancer201172224424920828861
- BandoEYonemuraYTaniguchiKFushidaSFujimuraTMiwaKOutcome of ratio of lymph node metastasis in gastric carcinomaAnn Surg Oncol20029877578412374661
- InoueKNakaneYIiyamaHThe superiority of ratio-based lymph node staging in gastric carcinomaAnn Surg Oncol200291273411829427
- IchikuraTOgawaTChochiKKawabataTSugasawaHMochizukiHMinimum number of lymph nodes that should be examined for the International Union Against Cancer/American Joint Committee on Cancer TNM classification of gastric carcinomaWorld J Surg200327333033312607061
- AshfaqAPockajBAGrayRJHalfdanarsonTRWasifNNodal counts and lymph node ratio impact survival after distal pancreatectomy for pancreatic adenocarcinomaJ Gastrointest Surg201418111929193524916590
- YouHYangJLiuQThe impact of the lymph node density on overall survival in patients with Wilms’ tumor: a SEER analysisCancer Manag Res20181067167729670401
- Surveillance. Epidemiology, and End Results (SEER) Program (www.seer.cancer.gov) SEER*Stat Database: Incidence - SEER 18 Regs Research Data, Nov 2017 Sub (1973–2015) <Katrina/Rita Population Adjustment> - Linked To County Attributes - Total U.S., 1969–2016 Counties, released April 2018 based on the November 2017 submission Surveillance Research Program, DCCPS National Cancer Institute
- CampRLDolled-FilhartMRimmDLX-tile: a new bio-informatics tool for biomarker assessment and outcome-based cut-point optimizationClin Cancer Res200410217252725915534099
- OngWZhaoRLuiBPrognostic significance of lymph node density in squamous cell carcinoma of the tongueHead Neck201638Suppl 1E859E86625917601
- HoningsJGaissertHAWeinbergACPrognostic value of pathologic characteristics and resection margins in tracheal adenoid cystic carcinomaEur J Cardiothorac Surg20103761438144420356756
- MegwaluUCSirjaniDRisk of nodal metastasis in major salivary gland adenoid cystic carcinomaOtolaryngol Head Neck Surg2017156466066428168897
- ZhaoYZhaoHFanLShiJAdenoid cystic carcinoma in the bronchus behaves more aggressively than its tracheal counterpartAnn Thorac Surg20139661998200424094522
- YangHYaoFTantaiJZhaoYTanQZhaoHResected tracheal adenoid cystic carcinoma: improvements in outcome at a single institutionAnn Thorac Surg2016101129430026431923
- MaziakDEToddTRJKeshavjeeSHWintonTLVan NostrandPPearsonFGAdenoid cystic carcinoma of the airway: Thirty-two-year experienceJ Thorac Cardiovasc Surg19961126152215328975844
- KanematsuTYohenaTUeharaTTreatment outcome of resected and nonresected primary adenoid cystic carcinoma of the lungAnn Thorac Cardiovasc Surg200282747712027791
- HuMMHuYHeJBPrimary adenoid cystic carcinoma of the lung: Clinicopathological features, treatment and resultsOncol Lett2015931475148125663934
- JiaoWZhuDChengZZhaoYThoracoscopic tracheal resection and reconstruction for adenoid cystic carcinomaAnn Thorac Surg2015991e15e1725555982
- RegnardJFFourquierPLevasseurPResults and prognostic factors in resections of primary tracheal tumors: a multicenter retrospective study. The French Society of Cardiovascular SurgeryJ Thorac Cardiovasc Surg199611148088138614141
- ZhuFLiuZHouYPrimary salivary gland-type lung cancer: clinicopathological analysis of 88 cases from ChinaJ Thorac Oncol20138121578158424389442