
Abstract
Purpose
This study aimed to investigate the efficacy of preoperative aspartate aminotransferase-to-platelet-ratio index (APRI) score to predict the risk of posthepatectomy liver failure (PHLF) in patients with hepatocellular carcinoma (HCC) after liver resection, and to compare the discriminatory performance of the APRI with the Child–Pugh score, model for end-stage liver disease (MELD) score, and albumin–bilirubin (ALBI) score.
Patients and methods
A total of 1,044 consecutive patients with HCC who underwent liver resection were enrolled and studied. Univariate and multivariate analyses were performed to investigate risk factors associated with PHLF. Predictive discrimination of Child–Pugh, MELD, ALBI, and APRI scores for predicting PHLF were assessed according to area under the ROC curve. The cutoff value of the APRI score for predicting PHLF was determined by ROC analysis. APRI scores were stratified by dichotomy to analyze correlations with incidence and grade of PHLF.
Results
PHLF occurred in 213 (20.4%) patients. Univariate and multivariate analyses revealed that Child–Pugh, MELD, ALBI, and APRI scores were significantly associated with PHLF. Area under the ROC analysis revealed that the APRI score for predicting PHLF was significantly more accurate than Child–Pugh, MELD, or ALBI scores. With an optimal cutoff value of 0.55, the sensitivity and specificity of the APRI score for predicting PHLF were 72.2% and 68.0%, respectively, and the incidence and grade of PHLF in patients with high risk (APRI score >0.55) was significantly higher than in the low-risk cohort (APRI score <0.55).
Conclusion
The APRI score predicted PHLF in patients with HCC undergoing liver resection more accurately than Child–Pugh, MELD, or ALBI scores.
Introduction
HCC is the sixth-most common aggressive malignancy and the second-leading cause of cancer-related deaths worldwide.Citation1 Surgical resection is the most effective curative treatment for patients with resectable HCC and moderate liver-function reserve, providing patients promising survival benefits.Citation2–Citation5 Even though surgical techniques and management have greatly improved over the past few decades, PHLF remains one of the most serious and dreaded complications after hepatectomy in HCC patients, and is a main cause of postoperative death.Citation6–Citation9 Therefore, accurate preoperative prediction of the risk of PHLF in patients with HCC is essential for surgeons to assess the feasibility and safety of liver resection.
Conventional scores, such as Child–Pugh score,Citation10 MELD score,Citation11–Citation13 ALBI score,Citation14 and APRI score,Citation15 are used widely for preoperative assessment of liver-function reserve. Child–Pugh score, which has been merged into clinical management algorithms of HCC patients, is the most used to predict the risk of PHLF;Citation2,Citation3,Citation6 however, it has limitations.Citation10 For example, a serum bilirubin level of 55 μmol/L has the same impact on the score as 550 μmol/L, because of arbitrary thresholds for continuous variables. The most serious deficiency of the Child–Pugh score is that it uses two arbitrary and subjective clinical variables – ascites and hepatic encephalopathy – in its calculation. The MELD score estimates the prognosis of decompen-sated liver-cirrhosis patients, and it has become widely used for organ allocation in liver transplantation and for assessing the 3- to 6-month survival rate in patients with liver failure.Citation11–Citation13 However, the MELD score is not optimal for predicting PHLF after hepatectomy in HCC either, because it was designed for patients with advanced cirrhosis, which most HCC patients do not have.Citation13 The ALBI score has eliminated the arbitrariness and subjectivity of liver-function-reserve assessment in patients with ascites and hepatic encephalopathy, and it has been reported to be superior to Child–Pugh and MELD scores in predicting PHLF and prognosis of HCC patients after liver resection.Citation16–Citation18 However, the ALBI score has no “ceiling effect”, so it is not applicable to assessing liver-function reserve in patients with obstructive jaundice.Citation17 As such, the efficacy of these three conventional scoring systems to predict PHLF before surgery is doubtful.
The APRI score, which is calculated on the ratio of serum AST and platelet count,Citation13 has been reported to predict liver cirrhosis and fibrosis accurately in patients with chronic HBV infection.Citation19 The Asian Pacific Association for the Study of the Liver has proposed that the APRI score is the most cost-effective noninvasive tool to evaluate hepatic cirrhosis and active hepatitis, even to the point of replacing liver biopsy.Citation20 The APRI score has been validated in estimating liver-function reserve and prognosis in patients with HCC,Citation21 but whether it can accurately predict PHLF for patients with HCC who undergo hepatectomy is unknown. We conducted this study to assess the APRI score in predicting the PHLF probability for patients with HCC who have undergone hepatectomy, and to compare its predictive value with that of the Child–Pugh score, MELD score, and ALBI score.
Patients and methods
Patients
All patients with HCC who had received treatment for liver resection with curative intent at the Affiliated Tumor Hospital of Guangxi Medical University between September 2013 and December 2016 were included in this study. The study was approved by the university’s ethics committee in accordance with the Declaration of Helsinki. All patients provided informed consent, and their data were used in this research. Inclusion criteria were: 1) diagnosis of HCC confirmed by histology; 2) no preoperative anticancer treatments for HCC, including transarterial chemoembolization, radiofrequency ablation, and others; 3) no simultaneous malignancies; 4) no preoperative obstructive jaundice; and 5) no preoperative cardiopulmonary, cerebral, or renal dysfunction.
Diagnosis and definitions
Patients were diagnosed initially with HCC staging based of the Barcelona Clinical Liver Cancer staging systemCitation21 and confirmed by histological examination of pathological tissue. The definition of curative liver resection was complete removal of all visible tumor without residual tumor at surgical margins.Citation22 The definition of major liver resection was the removal of three or more Couinaud liver segments.Citation23 The definition of clinically significant portal hypertension was splenomegaly (diameter ≥12 cm) with a platelet count <100×109/L or gastroesophageal varices.Citation24 Patients who had an HBV DNA level >2,000 IU/mL before liver resection were considered to have a high viral load.Citation25–Citation27 According to the criteria proposed by the International Study Group of Liver Surgery, the definition of PHLF is an elevated international normalized ratio (INR) and bilirubin level on or after liver-resection day 5.Citation8 No special treatment was required for patients with grade A PHLF, noninvasive treatment was required for patients with grade B PHLF, invasive procedures were required for patients who developed grade C PHLF.Citation8 The definition of postoperative mortality was death within 90 days after hepatectomy.
Treatments and follow-up
Before surgery, abdominal ultrasonography and contrast-enhanced computed tomography (CT) or magnetic resonance imaging (MRI) was routinely performed to assess tumor status and resectability. Child–Pugh grade and remnant liver volume were calculated to evaluate liver-function reserve. Indications of major or minor hepatectomy for patients with HCC were good health status, Eastern Cooperative Oncology Group score 0–2, good liver-function reserve, with Child–Pugh grade A or B, adequate remnant liver volume measured by volumetric CT or MRI, considered 30% for patients with normal liver status and without distant metastases and 50% for patients with severe liver cirrhosis or other liver disease.Citation17 Surgery started with a right subcostal incision, and the incision was extended to the left subcostal region if necessary. The surgeons examined the abdominal cavity to confirm the extent of local disease, extrahepatic metastases, and peritoneal seeding. They then ligated and divided the corresponding hepatic pedicle, hepatic vein, and short veins. During the liver resection, Pringle’s maneuver was used to block blood inflow to the liver when necessary, with each clamp time <15 minutes, followed by 5 minutes of clamp-free interval. Hepatectomy was performed with electrosurgical instruments, sometimes in conjunction with a clampcrushing method. Before the abdomen was closed, drains were routinely placed in the subphrenic cavity. All resected surgical specimens were histopathologically examined independently by three pathologists.
After discharge, all patients received regular follow up at 1 month after hepatectomy and then at intervals of 2–3 months in the first year after hepatectomy and every 3–6 months from the second year. At each follow-up visit, routine reexaminations included liver-function test, serum AFP level, HBV, markers and HBV DNA (if the patient had HBV infection), chest radiography, abdominal ultrasonography, and CT or MRI. Based on the extent of disease, liver-function reserve, general health status, and economic conditions, patients with recurrence were treated by liver resection, radiofrequency ablation, percutaneous ethanol injection, transcatheter arterial chemoembolization, or sorafenib.
Calculation of score values
The Child–Pugh score includes total serum bilirubin, pro-thrombin time, albumin, ascites, and hepatic encephalopathy.Citation10 The MELD score was calculated as 3.8×loge (bilirubin [mg/dL]) +11.2×loge (INR)+9.6× loge (creatinine [mg/dL]) +6.4× loge (etiology, cholestatic/alcoholic 0, others 1).Citation11 The ALBI score was calculated as 0.66×log10 (bilirubin [μmol/L] − 0.085 × albumin [g/L]).Citation14 The APRI score was calculated as AST/upper limit of normal/platelet count (expressed as platelets ×109/L) ×100.Citation15 All components of these formulae were tested and analyzed within 1 week before surgery.
Statistical analysis
Continuous data of normally distributed values are expressed as mean ± SD and compared using unpaired two-tailed t-tests. Values with abnormal distribution are expressed as medians (IQR 25–75) and compared using Mann–Whitney tests. Categorical data are shown as frequencies, and proportions were compared using χ2. Univariate logistic analysis was used first to assess factors related to PHLF. Variables with statistical significance were then analyzed by multivariate logistic regression analysis to confirm independent predictors of PHLF. Area under the ROC curve (AUC) was calculated to evaluate the discriminatory performance of Child–Pugh, MELD, ALBI, and APRI scores for predicting PHLF. The cutoff value of the APRI score for predicting PHLF was determined by ROC analysis. APRI scores were then stratified by dichotomy, and correlations between risk cohorts for APRI scores and incidence and grade of PHLF analyzed. Statistical analysis was conducted with SPSS 23.0 (IBM Corporation, Armonk, New York, USA). P<0.05 was considered statistically significant.
Results
Clinicopathological characteristics
A total of 1,189 patients received curative hepatectomy during the study. Of these, 145 patients were excluded for these reasons: 72 patients had histologically proven non-HCC, 61 patients had received anticancer treatments for HCC before hepatectomy, 8 patients had obstructive jaundice, and 4 patients had other simultaneous malignant tumors. Finally, 1,044 patients with HCC who met the inclusion criteria were enrolled in this study ().
Table 1 Baseline characteristics of the included 1,044 patients with HCC and comparison of factors between patients with or without PHLF
Morbidity and mortality
Of the 1,044 HCC patients, PHLF occurred in 20.4% (n=213): 9.67% (n=101) with grade A, 10.06% (n=105) with grade B, and 0.67% (n=7) with grade C PHLF. The postoperative mortality rate was 2.7% (n=28): 20 patients died of PHLF complicated with sepsis or multiple-organ failure, and 8 patients died of cardiopulmonary failure and other reasons.
Independent predictors of PHLF
The results of univariate logistic analysis are presented in . For multivariate analysis, Child–Pugh, MELD, ALBI, and APRI scores were used in different logistic regression models to avoid collinearity. Therefore, the Child–Pugh score (OR 1.524, 95% CI 1.150–2.019; P=0.003), MELD score (OR 1.060, 95% CI 1.012–1.111; P=0.015), ALBI score (OR 2.000, 95% CI 1.204–3.321; P=0.007), and APRI score (OR 2.046, 95% CI 1.542–2.714; P<0.007) were closely related to PHLF (). Furthermore, male sex, HBV DNA ≥2,000 IU/mL, cirrhosis, tumor size, multiple-tumor number, major liver resection, and blood loss≥ 400 mL had a significant influence on prognosis ().
Table 2 Univariate logistic analyses to identify predictors of PHLF in patients with HCC
Table 3 Multivariate logistic analyses to identify predictors of PHLF in patients with HCC
Discriminatory performance of Child–Pugh, MELD, ALBI, and APRI scores for predicting PHLF
The AUC analysis showed that the APRI score (AUC 0.743, 95% CI 0.706–0.780; P<0.001) for predicting PHLF was significantly higher than that of Child–Pugh (AUC 0.562, 95% CI 0.517–0.607; P=0.005), MELD (AUC 0.647, 95% CI 0.606–0.687; P<0.001), and ALBI (AUC 0.662, 95% CI 0.620–0.704; P<0.001) scores in the entire cohort of patients with HCC (). The APRI-score cutoff value of 0.55 had a sensitivity of 72.2% and a specificity of 68.0% for predicting PHLF.
Figure 1 ROC curves of APRI, Child–Pugh, MELD, and ALBI scores for predicting PHLF.
Notes: (A) Entire cohort of patients. (B) Patients positive for HBsAg and HBV DNA >2,000 IU/mL. (C) Patients positive for HBsAg and HBV DNA ≤2,000 (IU/mL). (D) Patients with cirrhosis. (E) Patients without cirrhosis. (F) Patients with major liver resection. (G) Patients with minor liver resection. (H) Patients with intraoperative blood loss ≥400 (mL). (I) Patients with intraoperative blood loss <400 mL. Area under the curve: (A) 0.743 for APRI vs 0.562 for Child–Pugh, 0.647 for MELD, and 0.662 for ALBI; (B) 0.746 vs 0.572, 0.659, and 0.681; (C) 0.699 vs 0.554, 0.614, and 0.661; (D) 0.732 vs 0.585, 0.641, and 0.677; (E) 0.729 vs 0.533, 0.638, and 0.640; (F) 0.718 vs 0.558, 0.634, and 0.648; (G) 0.758 vs 0.563, 0.684, and 0.669; (H) 0.743 vs 0.538, 0.638, and 0.641; (I) 0.729 vs 0.574, 0.656, and 0.667, respectively.
Abbreviation: HBsAg, hepatitis B surface antigen; HBV, hepatitis B virus MELD, model for end-stage liver disease; ALBI, albumin–bilirubin; APRI, aspartate aminotransferase-to-platelet-ratio index; PHLF, posthepatectomy liver failure.
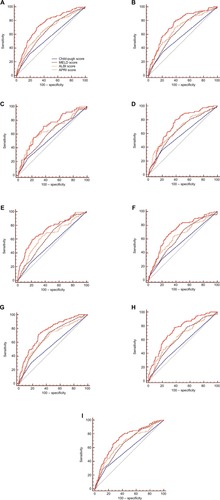
To eliminate subgroups of patients with HCC negatively impacted by APRI score, we stratified HCC patients by HBV DNA load, cirrhosis status, extent of resection, and blood loss. The discriminative performance of Child–Pugh, MELD, ALBI, and APRI scores for predicting PHLF were also compared in subgroups of patients with HCC (). The APRI score for predicting PHLF of patients with HCC among subgroups was also greater than Child–Pugh, MELD, and ALBI scores, and the APRI score had a stronger ability to predict PHLF in patients positive for HBV surface antigen and HBV DNA >2,000 IU/mL, cirrhosis, minor liver resection, or blood loss ≥400 mL.
Correlation between APRI score and incidence and grade of PHLF
With the ROC analysis, the optimal cutoff value of the APRI score for predicting PHLF was 0.55 among all patients. Patients with an APRI score >0.55 were designated the high-risk cohort, and those with an APRI score ≤0.55 were designated the low-risk cohort. Patients in the high-risk cohort had significantly higher incidence and grade of PHLF than those in the low-risk cohort ().
Figure 2 Correlations between risk cohorts of APRI score and incidence and grade of PHLF.
Notes: (A) Entire cohort of patients. (B) Patients positive for HBsAg and HBV DNA >2,000 IU/mL. (C) Patients positive for HBsAg and HBV DNA ≤2,000 IU/mL. (D) Patients with cirrhosis. (E) Patients without cirrhosis. (F) Patients with major liver resection. (G) Patients with minor liver resection. (H) Patients with intraoperative blood loss ≥400 mL. (I) Patients with intraoperative blood loss <400 mL (incidence, P<0.001 for all [χ2-test]; grade, P<0.001 for all [Kruskal-Wallis H-test]).
Abbreviations: HBsAg, hepatitis B surface antigen; HBV, hepatitis B virus; APRI, aspartate aminotransferase-to-platelet-ratio index; PHLF, posthepatectomy liver failure.
![Figure 2 Correlations between risk cohorts of APRI score and incidence and grade of PHLF.Notes: (A) Entire cohort of patients. (B) Patients positive for HBsAg and HBV DNA >2,000 IU/mL. (C) Patients positive for HBsAg and HBV DNA ≤2,000 IU/mL. (D) Patients with cirrhosis. (E) Patients without cirrhosis. (F) Patients with major liver resection. (G) Patients with minor liver resection. (H) Patients with intraoperative blood loss ≥400 mL. (I) Patients with intraoperative blood loss <400 mL (incidence, P<0.001 for all [χ2-test]; grade, P<0.001 for all [Kruskal-Wallis H-test]).Abbreviations: HBsAg, hepatitis B surface antigen; HBV, hepatitis B virus; APRI, aspartate aminotransferase-to-platelet-ratio index; PHLF, posthepatectomy liver failure.](/cms/asset/a469a99a-5f63-4747-9881-1d6279ebf4aa/dcmr_a_12186054_f0002_c.jpg)
Similarly, using the same cutoff value for the APRI score, the incidence and grade of PHLF increased with increasing APRI scores in all the subgroups (). There was a statistically significant positive correlation between high risk and incidence and grade of PHLF (P<0.001 for all).
Discussion
In this study, we compared the APRI score with Child–Pugh, MELD, and ALBI scores in predicting PHLF in patients with HCC who had undergone liver resection. The predictive performance of the APRI score was found to be superior to the other scoring systems. Moreover, the APRI score was superior in predicting PHLF in patient subgroups based on serum HBV DNA load, liver-cirrhosis status, extent of resection, and intraoperative blood loss.
HBV is the most common cause of chronically impaired liver function and liver cirrhosis in Asia-Pacific regions, particularly in mainland China. HBV infection usually accompanies disorders of immunofunction caused by immunological injury,Citation28 which may be accompanied by an attendant risk of PHLF. HBV reactivation often occurs in patients with a high preoperative HBV DNA load, and a high load is a reported risk factor of PHLF.Citation25 Liver cirrhosis is a negative predictor of liver regeneration and recovery of liver function, and it may increase the risk of postoperative ascites and duration of PHLF.Citation6,Citation20 Therefore, accurate preoperative assessment of active HBV and hepatic cirrhosis is critical to reducing the incidence of PHLF. Considering the high degree of accuracy of the APRI score in predicting liver cirrhosis and fibrosis in HBV-infected patients,Citation29 we performed stratified analyses of subgroups of patients according to HBV DNA load and the presence or absence of cirrhosis. We found the APRI score to have better ability than Child–Pugh, MELD, and ALBI scores to predict PHLF in HCC patients with HBV DNA >2,000 IU/mL and cirrhosis. Meanwhile, similar results were found in patients with HBV DNA ≤2,000 IU/mL and no cirrhosis.
Besides poor preoperative liver-function reserve, the surgical procedure itself is an important risk factor for PHLF:Citation6–Citation9 major liver resection and high-volume intraoperative blood loss reportedly increase the risk of PHLF.Citation30,Citation31 In our study, multivariate logistic analysis revealed that major liver resection and blood loss ≥400 mL were correlated with PHLF. After eliminating the influence of these factors, we performed stratified analyses on the extent of resection and volume of intraoperative blood loss. The APRI score was more accurate than Child–Pugh, MELD, and ALBI scores in predicting PHLF in patients with major resection, minor resection, intraoperative blood loss ≥400 mL, and intraoperative blood loss <400 mL.
This study analyzed correlations between risk cohorts for APRI score and the incidence and grade of PHLF. The APRI score had a sensitivity of 72.2% and specificity of 68.0% for predicting PHLF at the optimal cutoff value of 0.55. Like Child–Pugh, MELD, and ALBI scores (–), the APRI score stratified patients with HCC into surgical risk categories. We found that stratified APRI score accurately predicted the incidence and grade of PHLF in HCC patients undergoing curative liver resection. Patients with HCC in the high-risk cohort (APRI score >0.55) had significantly higher incidence and grade of PHLF than those in the low-risk cohort (APRI score ≤0.55). Considering the high incidence and grade of PHLF, patients in the high-risk cohort for APRI score are not suitable for major liver resection. Conversely, with low incidence and grade of PHLF, patients in low-risk cohort for APRI score are moderate candidates for hepatectomy.
The correlation between increased risk of PHLF and increased APRI scores logically is a result of the underlying liver disease, as reflected in the scores. The AST component of the APRI could be increased because of liver stress or damage caused by liver cirrhosis:Citation20 clearance of AST may have been impaired or HBV replication reactivated,Citation30 with release of AST from injured mitochondria.Citation32 The platelet-count component of the APRI could be decreased because of sequestration and destruction of platelets in the enlarging spleen (portal hypertension)Citation33,Citation34 or progressive liver fibrosis, which could reduce hepatocyte production of thrombopoietin and consequent decreased platelet production.Citation35 Low preoperative platelet counts have been associated with an increased risk of PHLF and mortality after hepatectomy.Citation36
We acknowledge that our study has limitations. First, most patients had HBV-related HCC, so the applicability of APRI scores to predicting PHLF in HCC patients with other etiological liver characteristics was not fully assessed. Second, the study was a retrospective analysis and only a preliminary exploration of the predictive value of the APRI score, and thus prospective studies with larger populations should be conducted to ascertain the value of the APRI score for predicting PHLF after hepatectomy for HCC.
Conclusion
Preoperative APRI scores can more accurately predict PHLF than Child–Pugh, MELD, and ALBI scores in patients undergoing liver resection for HCC. Determining the preoperative APRI score to predict PHLF may be useful in guiding surgical treatment of patients with HCC.
Author contributions
RYM and JZY contributed equally to this work. RYM, JZY, LQL, FXW, and GBW made substantial contributions to conception, design, analysis, and interpretation of data, and wrote and revised the manuscript. RYM, ZRL, and XMS collected and analyzed the data. TB and JC helped to collect and analyze the data. All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Abbreviations
| HCC | = | hepatocellular carcinoma |
| PHLF | = | posthepatectomy liver failure |
| APRI | = | aspartate aminotransferase-to-platelet ratio index |
| MELD | = | model for end-stage liver disease |
| ALBI | = | albumin–bilirubin |
| HBV | = | hepatitis B virus |
Acknowledgments
This study was supported by the National Natural Science Foundation of China (81460426 and 81860502) and the National Science Foundation of China Youth Fund Project (81803007).
Supplementary materials
Figure S1 Correlations between patients with Child–Pugh grade A or grade B and incidence and grade of PHLF.
Notes: (A) Entire cohort of patients. (B) Patients positive for HBsAg and HBV DNA >2,000 IU/mL. (C) Patients positive for HBsAg and HBV DNA ≤2,000 IU/mL. (D) Patients with cirrhosis. (E) Patients without cirrhosis. (F) Patients with major liver resection. (G) Patients with minor liver resection. (H) Patients with intraoperative blood loss ≥400 mL. (I) Patients with intraoperative blood loss <400 mL (incidence [C, E, H], P>0.05; others, P<0.05 [χ2 test]; grade [C, E, H], P>0.05; others, P<0.05 [Kruskal–Wallis H-test]).
Abbreviations: HBsAg, hepatitis B surface antigen; HBV, hepatitis B virus; PHLF, posthepatectomy liver failure.
![Figure S1 Correlations between patients with Child–Pugh grade A or grade B and incidence and grade of PHLF.Notes: (A) Entire cohort of patients. (B) Patients positive for HBsAg and HBV DNA >2,000 IU/mL. (C) Patients positive for HBsAg and HBV DNA ≤2,000 IU/mL. (D) Patients with cirrhosis. (E) Patients without cirrhosis. (F) Patients with major liver resection. (G) Patients with minor liver resection. (H) Patients with intraoperative blood loss ≥400 mL. (I) Patients with intraoperative blood loss <400 mL (incidence [C, E, H], P>0.05; others, P<0.05 [χ2 test]; grade [C, E, H], P>0.05; others, P<0.05 [Kruskal–Wallis H-test]).Abbreviations: HBsAg, hepatitis B surface antigen; HBV, hepatitis B virus; PHLF, posthepatectomy liver failure.](/cms/asset/20cf0af7-8e70-45b9-9809-e09ecf935215/dcmr_a_12186054_sf0001_c.jpg)
Figure S2 Correlation between the patients with MELD score >11 or <9 and the incidence and grade of PHLF.
Notes: (A) Entire cohort of patients. (B) Patients positive for HBsAg and HBV DNA >2,000(IU/mL). (C) Patients positive for HBsAg and HBV DNA ≤2,000 (IU/mL). (D) Patients with cirrhosis. (E) Patients without cirrhosis. (F) Patients with major liver resection. (G) Patients with minor liver resection. (H) Patients with intraoperative blood loss ≥400 (mL). (I) Patients with intraoperative blood loss <400 mL (incidence: [F] P<0.05, others P>0.05 [χ2-test]; grade: P<0.001 for all [Kruskal–Wallis H-test].
Abbreviations: HBsAg, hepatitis B surface antigen; HBV, hepatitis B virus; MELD, model for end-stage liver disease; PHLF, posthepatectomy liver failure.
![Figure S2 Correlation between the patients with MELD score >11 or <9 and the incidence and grade of PHLF.Notes: (A) Entire cohort of patients. (B) Patients positive for HBsAg and HBV DNA >2,000(IU/mL). (C) Patients positive for HBsAg and HBV DNA ≤2,000 (IU/mL). (D) Patients with cirrhosis. (E) Patients without cirrhosis. (F) Patients with major liver resection. (G) Patients with minor liver resection. (H) Patients with intraoperative blood loss ≥400 (mL). (I) Patients with intraoperative blood loss <400 mL (incidence: [F] P<0.05, others P>0.05 [χ2-test]; grade: P<0.001 for all [Kruskal–Wallis H-test].Abbreviations: HBsAg, hepatitis B surface antigen; HBV, hepatitis B virus; MELD, model for end-stage liver disease; PHLF, posthepatectomy liver failure.](/cms/asset/ad4233e3-18f1-4175-894f-be2d68c04b68/dcmr_a_12186054_sf0002_c.jpg)
Figure S3 Correlation between the patients with ALBI grade 1 or grade 2–3 and the incidence and grade of PHLF.
Notes: (A) Entire cohort of patients. (B) Patients positive for HBsAg and HBV DNA >2,000 IU/mL. (C) Patients positive for HBsAg and HBV DNA ≤2,000 IU/mL. (D) Patients with cirrhosis. (E) Patients without cirrhosis. (F) Patients with major liver resection. (G) Patients with minor liver resection. (H) Patients with intraoperative blood loss ≥400 mL. (I) Patients with intraoperative blood loss <400 mL (incidence, P<0.001 for all [χ2-test]; grade, P<0.001 for all [Kruskal–Wallis H-test]).
Abbreviation: HBsAg, hepatitis B surface antigen; HBV, hepatitis B virus; ALBI, albumin–bilirubin; PHLF, posthepatectomy liver failure.
![Figure S3 Correlation between the patients with ALBI grade 1 or grade 2–3 and the incidence and grade of PHLF.Notes: (A) Entire cohort of patients. (B) Patients positive for HBsAg and HBV DNA >2,000 IU/mL. (C) Patients positive for HBsAg and HBV DNA ≤2,000 IU/mL. (D) Patients with cirrhosis. (E) Patients without cirrhosis. (F) Patients with major liver resection. (G) Patients with minor liver resection. (H) Patients with intraoperative blood loss ≥400 mL. (I) Patients with intraoperative blood loss <400 mL (incidence, P<0.001 for all [χ2-test]; grade, P<0.001 for all [Kruskal–Wallis H-test]).Abbreviation: HBsAg, hepatitis B surface antigen; HBV, hepatitis B virus; ALBI, albumin–bilirubin; PHLF, posthepatectomy liver failure.](/cms/asset/533e65af-77eb-4630-b925-62f49841578f/dcmr_a_12186054_sf0003_c.jpg)
Disclosure
The authors report no conflicts of interest in this work.
References
- SiegelRLMillerKDJemalACancer statistics, 2017CA Cancer J Clin201767173028055103
- HeimbachJKKulikLMFinnRSAASLD guidelines for the treatment of hepatocellular carcinomaHepatology201867135838028130846
- European Association for the Study of the LiverElectronic address: [email protected]; European Association for the Study of the Liver. EASL clinical practice guidelines: management of hepatocellular carcinomaJ Hepatol201869118223629628281
- OmataMChengALKokudoNAsia-Pacific clinical practice guidelines on the management of hepatocellular carcinoma: a 2017 updateHepatol Int201711431737028620797
- ZhongJHKeYGongWFHepatic resection associated with good survival for selected patients with intermediate and advanced-stage hepatocellular carcinomaAnn Surg2014260232934024096763
- HernaezRSolàEMoreauRGinèsPAcute-on-chronic liver failure: an updateGut201766354155328053053
- SchreckenbachTLieseJBechsteinWOMoenchCPosthepatectomy liver failureDig Surg2012291798522441624
- RahbariNNGardenOJPadburyRPosthepatectomy liver failure: a definition and grading by the International Study Group of liver surgery (ISGLS)Surgery2011149571372421236455
- MelloulEHübnerMScottMGuidelines for perioperative care for liver surgery: enhanced recovery after surgery (ERAS) Society recommendationsWorld J Surg201640102425244027549599
- DurandFVallaDAssessment of the prognosis of cirrhosis: childpugh versus MELDJ Hepatol2005421S100S10715777564
- MalinchocMKamathPSGordonFDPeineCJRankJter BorgPCA model to predict poor survival in patients undergoing transjugular intrahepatic portosystemic shuntsHepatology200031486487110733541
- KamathPSWiesnerRHMalinchocMA model to predict survival in patients with end-stage liver diseaseHepatology200133246447011172350
- WiesnerREdwardsEFreemanRModel for end-stage liver disease (MELD) and allocation of donor liversGastroenterology20031241919612512033
- JohnsonPJBerhaneSKagebayashiCAssessment of liver function in patients with hepatocellular carcinoma: a new evidence-based Approach—the ALBI gradeJ Clin Oncol201533655055825512453
- WaiCA simple noninvasive index can predict both significant fibrosis and cirrhosis in patients with chronic hepatitis CHepatology200338251852612883497
- ChanAWChanRCWongGLNew simple prognostic score for primary biliary cirrhosis: albumin-bilirubin scoreJ Gastroenterol Hepatol20153091391139625753927
- WangYYZhongJHSuZYAlbumin-bilirubin versus Child-Pugh score as a predictor of outcome after liver resection for hepatocellular carcinomaBr J Surg2016103672573427005482
- ChenRCCaiYJWuJMUsefulness of albumin-bilirubin grade for evaluation of long-term prognosis for hepatitis B-related cirrhosisJ Viral Hepat201724323824527862671
- LinZHXinYNDongQJPerformance of the aspartate aminotransferase-to-platelet ratio index for the staging of hepatitis C-related fibrosis: an updated meta-analysisHepatology201153372673621319189
- ShihaGIbrahimAHelmyAAsian-Pacific association for the study of the liver (APASL) consensus Guidelines on invasive and noninvasive assessment of hepatic fibrosis: a 2016 updateHepatol Int2017111130
- BruixJReigMShermanMEvidence-based diagnosis, staging, and treatment of patients with hepatocellular carcinomaGastroenterology2016150483585326795574
- HermanekPWittekindCThe pathologist and the residual tumor (R) classificationPathol Res Pract199419021151238058567
- PolBCampanPHardwigsenJBottiGPonsJLe TreutYPMorbidity of major hepatic resections: a 100-case prospective studyEur J Surg1999165544645310391161
- BerzigottiAReigMAbraldesJGBoschJBruixJPortal hypertension and the outcome of surgery for hepatocellular carcinoma in compensated cirrhosis: a systematic review and meta-analysisHepatology201561252653625212123
- HuangGLauWYShenFPreoperative hepatitis B virus DNA level is a risk factor for postoperative liver failure in patients who underwent partial hepatectomy for hepatitis B-related hepatocellular carcinomaWorld J Surg20143892370237624696061
- AnHJJangJWBaeSHSustained low hepatitis B viral load predicts good outcome after curative resection in patients with hepatocellular carcinomaJ Gastroenterol Hepatol201025121876188221092000
- HungIFPoonRTLaiCLFungJFanSTYuenMFRecurrence of hepatitis B-related hepatocellular carcinoma is associated with high viral load at the time of resectionAm J Gastroenterol200810371663167318616655
- WebsterGIncubation phase of acute hepatitis B in man: dynamic of cellular immune mechanismsHepatology20003251117112411050064
- XiaoGYangJYanLComparison of diagnostic accuracy of aspartate aminotransferase to platelet ratio index and fibrosis-4 index for detecting liver fibrosis in adult patients with chronic hepatitis B virus infection: a systemic review and meta-analysisHepatology201561129230225132233
- RösslerFSapisochinGSongGDefining benchmarks for major liver surgery: a multicenter analysis of 5202 living liver donorsAnn Surg2016264349250027433909
- CywinskiJBAlsterJMMillerCVogtDPParkerBMPrediction of intraoperative transfusion requirements during orthotopic liver transplantation and the influence on postoperative patient survivalAnesth Analg2014118242843724445640
- OkudaMLiKBeardMRMitochondrial injury, oxidative stress, and antioxidant gene expression are induced by hepatitis C virus core proteinGastroenterology2002122236637511832451
- FreedmanRADockterTJLafkyJMPromoting accrual of older patients with cancer to clinical trials: an Alliance for clinical trials in oncology member Survey (A171602)Oncologist20182391016102329674441
- McCormickPAMurphyKMSplenomegalyMKMSplenomegaly, hypersplenism and coagulation abnormalities in liver diseaseBaillieres Best Pract Res Clin Gastroenterol20001461009103111139352
- KurokawaTMurataSOhkohchiNStable liver function during long-term administration of eltrombopag, a thrombopoietin receptor agonist, in patients with chronic liver diseaseTohoku J Exp Med2016240427727927928110
- MaithelSKKneuertzPJKoobyDAImportance of low preoperative platelet count in selecting patients for resection of hepatocellular carcinoma: a multi-institutional analysisJ Am Coll Surg2011212463864821463803