
Abstract
Background
This study aimed to clarify the effect of thoracic drainage fluid (DF) on lung cancer cells in vitro.
Methods
We assessed the influence of DF on the proliferation and migration of lung cancer cells (LTEP-a-2 and A549) using the MTT cell proliferation assay and scratch wound assay. Cell apoptosis was determined by flow cytometric analysis. We also investigated the effect of DF on drug chemosensitivity, assessing viability of LTEP-a-2 and A549 cells.
Results
The proliferative rates of cancer cells in the DF-treated group were significantly higher than those of the control group. Similar results were obtained for cell migration of lung cancer cells. Cells in the DF-treated groups showed a lower percentage of apoptosis than those of the control groups. Chemosensitivity of lung cancer cells to doxycycline and cisplatin (DDP) was lowered by DF.
Conclusion
These findings suggest that DF affects lung cancer cells by promoting proliferation and migration, inhibiting apoptosis, and increasing drug resistance.
Introduction
Lung cancer has the highest incidence and mortality rate among all cancers in China and worldwide.Citation1,Citation2 Currently, surgery is the most important and only method for curing lung cancer. With the improvement of diagnostic and treatment procedures, such as endoscopy, radical surgery, radiochemotherapy, targeted therapy, and other integrated treatments,Citation3,Citation4 more accurate staging and early diagnosis have significantly increased the survival of lung cancer patients.Citation5–Citation7 Also, advances in surgical techniques, such as thoracoscopy, have decreased surgical trauma and incidence of complications in patients, improving their quality of life.Citation8–Citation11
In recent years, many studies on lung cancer surgery have been put forward. With the number of lung cancer patients in China increasing every year, treatment efficiency in large hospitals has become a medical and even a social problem, awaiting resolution. Against this background, the concept of rapid rehabilitation surgery was born. In recent years, this concept has been explored and applied to gastrointestinal, thoracic, and other surgeries, in accordance with clinical diagnosis and treatment models.Citation12–Citation14 Among these is the thoracic surgery domain of lung cancer surgery, where many thoracic surgeons have proposed that the chest tube can be removed earlier after radical lung cancer surgery, especially after thoracoscopic lobectomy, to achieve early postoperative discharge of patients, increase bed turnover, and reduce medical costs. There are many studies showing that early removal of chest tubes does not increase the incidence of complications in patients during the perioperative period, and a small number of studies reported that eliminating the chest tube drainage of 500 mL/day also does not increase complications.Citation15 However, these practices entail reabsorption of excess pleural effusion into the systemic circulation. As malignant tumors are systemic diseases, the presence of chemical substances in plural effusion, and even residual tumor cells, has potential effects on local or systemic recurrence, and development of drug resistance. These effects are still unknown.
Previous studies have found that the drainage fluid (DF) from breast cancer patients promoted proliferation and migration of breast cancer cells, and this effect showed some degree of dose-dependence. One study showed that surgery may have negative effects on malignant tumors.Citation16 Based on this, we designed an experiment to examine the effects of thoracic DF obtained after lung cancer surgery on the biological behavior of lung cancer cells, including chemotherapeutic drug resistance. This provides experimental evidence of the biological characteristics of postoperative DF from various malignancies and may help guide the timing of postoperative tube removal and chemotherapy.
Results
Influence of DF on cell death of LTEP-a-2 and A549 cells
We evaluated the cell death of LTEP-a-2 and A549 cells by MTT assay, taking the untreated cells as reference. The results showed remarkably decreased cell death in the DF-treated group compared to the untreated cells (). The increased survival rates of A549 cells in 0.1%, 0.5%, and 1.0% DF-treated groups were 111.00% (±10.09%), 115.08% (±11.15%), and 114.78% (±11.26%), respectively. These were higher than the untreated group and the differences were statistically significant (P=0.0036, P=0.010, and P=0.011, respectively; and ). Similarly, the survival rates of LTEP-a-2 cells in 0.1%, 0.5%, and 1% DF-treated groups were 160.13% (±34.91%), 158.40% (±19.90%), and 161.31% (±17.33%), respectively, and these were also significantly higher than the untreated group (0.1%, 0.5%, and 1.0% DF, all P<0.001; ).
Figure 1 MTT proliferation assay: DF increases proliferation of LTEP-a-2 and A549 cells.
Notes: (A) Increases proliferation by DF in LTEP-a-2. (B) Increases proliferation by DF in A549. Proliferation of LTEP-a-2 and A549 cells was assessed by MTT proliferation assay, taking the untreated cells as reference. Proliferation was significantly increased in 0.1%, 0.5%, and 1% DF-treated groups compared to the control groups.
Abbreviation: DF, drainage fluid.
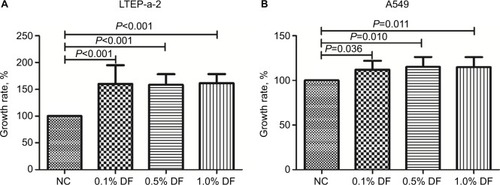
Figure 2 Chemosensitivity test: DF weakened the doxycycline and DDP chemosensitivity of lung cancer cells, taking the control groups as reference.
Notes: In the doxycycline chemosensitivity group, viability of LTEP-a-2 cell groups treated with DF (0.1% and 1%) were higher than those of the control groups at both drug concentration levels (5 and 50 mg/L), and the differences were statistically significant (A). Treatment with DDP produced results similar to those obtained with doxycycline (B). DF similarly weakened chemosensitivity of A549 cells (C and D).
Abbreviations: DDP, cisplatin; DF, drainage fluid; N, negative control.
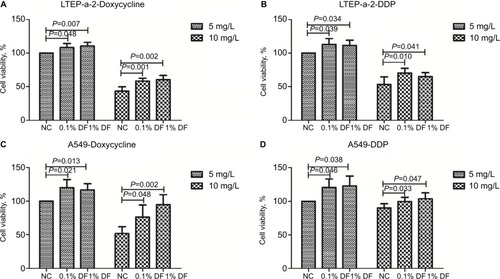
Effect of DF on chemosensitivity
We tested the effect of DF on drug chemosensitivity, assessing the viabilities of LTEP-a-2 and A549 cells (). In the doxycycline chemosensitivity group, the viability of DF-treated (0.1% and 1%) LTEP-a-2 cells was higher than that in the untreated groups for both drug concentration levels (5 and 10 mg/L) and the differences were statistically significant (P=0.047 and P=0.007, respectively, for 5 mg/L doxycycline; P<0.001 and P=0.002, respectively, for 50 mg/L doxycycline; ). Our results with DDP treatment were similar to those obtained for the doxycycline group. Cell viability in DF-treated groups was significantly higher than that in the control group, with statistically significant differences (P=0.039 and P=0.034, respectively, for 5 mg/L DDP; P=0.010 and P=0.041, respectively, for 10 mg/L DDP; ). We observed a similar effect of DF on the drug chemosensitivity of A549 cells ( and ). In the doxycycline group, viability of A549 cells with 0.1% and 1% DF was significantly higher than that in the untreated groups (P=0.021 and P=0.013, respectively, for 5 mg/L doxycycline; P=0.048 and P=0.002, respectively, for 10 mg/L doxycycline, ). We obtained similar results with DDP. Cell viability in DF-treated groups was significantly higher than in control groups (P=0.046 and P=0.038, respectively, for 5 mg/L DDP; P=0.033 and P=0.047, respectively, for 10 mg/L DDP; ).
Flow cytometry analysis
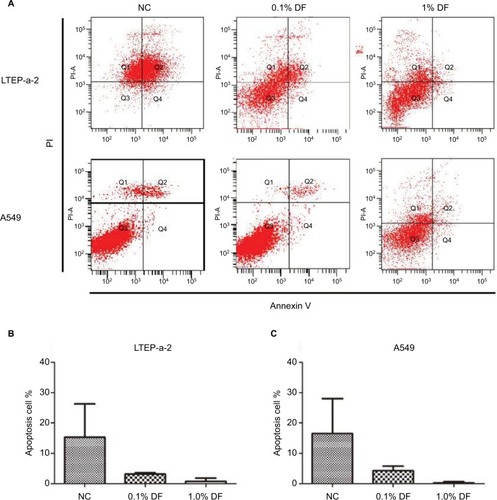
We performed a flow cytometric analysis to determine the percentage of apoptotic cells in each individual group. Cells in the groups treated with 0.1% and 1% DF showed lower apoptosis percentages than those of the control groups ().
Figure 3 Flow cytometry analysis: LTEP-a-2 and A549 cells in the groups treated with 0.1% and 1% DF showed lower percentages of apoptosis than the control groups.
Notes: (A) Representational figures for apoptosis of LTEP-a-2 and A549 cells. (B) Statistical results for apoptosis of LTEP-a-2 cells. (C) Statistical results for apoptosis of A549 cells.
Abbreviations: DF, drainage fluid; NC, negative control; PI, propidium iodide.
Influence of DF on motility of lung cancer cells
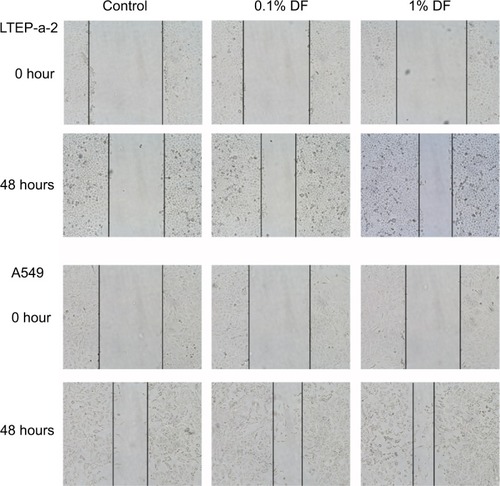
The potential motilities of LTEP-a-2 and A549 cells were evaluated by the scratch wound assay. The results showed that DF tends to stimulate migration of lung cancer cells in both 0.1% and 1% DF groups compared with the control group ().
Figure 4 Scratch wound tests: DF promoted migration of LTEP-a-2 and A549 cells.
Notes: Scratch wounds for LTEP-a-2 and A549 cells at 0 and 48 hours after introducing the wound, and treatment with DF. Scratch fold changes in 0.1% and 1% DF-treated groups were significantly higher than in the control group. The scratch closure change area of cells treated with 1% DF tended to be larger than with 0.1% DF.
Abbreviation: DF, drainage fluid.
Discussion
In this study, we showed that the effects of DF on lung cancer cells include promoted proliferation and migration, inhibited apoptosis, and increased drug resistance. These results were consistent with the findings of previous studies,Citation16–Citation18 which have suggested that DF acts as a form of tumor microenvironment and that its constituent cytokines and other components act to promote malignant biological behavior of tumor cells. In the local primary tumor, these negative effects provide an environment conducive to recurrence of residual tumor cells, while excessive DF absorption and circulation increase the probability of systemic recurrence of the tumor.
In a situation where China’s economy and national income are still not ideal, chemotherapy still remains an important adjuvant treatment for lung cancer as compared with targeted therapy,Citation7,Citation19 which has an indispensable function in the prevention of local and systemic recurrence. Our experimental results showed that DF not only promotes proliferation and inhibits apoptosis of lung cancer cells but also increases drug resistance. This suggests that the presence of local DF after surgery may increase recurrence and decrease the therapeutic efficacy of chemotherapy. Furthermore, DF was found to inhibit both early and late apoptosis in lung cancer cells, providing an environment conducive to the survival and recurrence of residual cancer cells. Therefore, there is still no definite conclusion as to whether chest tubes should be removed soon after surgery.
Previous studies have reported the major components of DF,Citation16 which include cytokines, chemokines, and matrix metalloproteinases. These are influenced by chemotherapy, TNM staging, pathological type, and molecular subtype. Among cytokines, the concentration of IL-6 is the highest, and previous studies have suggested that IL-6 can mediate tumor recurrence and metastasis through STAT3, MMP3, and other relevant pathways.Citation20–Citation23 Therefore, it is conceivable that several complex components of DF can mediate the malignant biological behavior of tumors through a variety of signaling pathways.
More in-depth studies to elucidate the specific underlying mechanisms of the biological effects of DF are warranted. The ability of cells to promote MTT reduction was only evaluated at one time point (48 hours). The MTT reduction is dependent not only on the number of cells but also on the metabolic performer of cells connected with their mitochondrial activity. The results can only improve the mitochondrial functionality or decreased number of cells that died after seeding without affecting the duplication time. Thus, additional assays are required to evaluate the effect of DF on the proliferation rate of cancer cells. The assessment of cell death by apoptosis and the assessment of cell resistance to apoptotic drugs allow limited conclusions. Apoptosis involves the activation of caspases, which is a group of cysteine proteases. The inclusion of the effects on the activity of the initiator and effector caspases should also be considered.
In addition, primary tumor cells from diverse lung cancer patients need to be tested in order to further investigate the drug susceptibility and biological effects of DF. Samples from different types of lung cancers are necessary to understand the differences in chemotherapeutic susceptibility between different clinicopathological types. This research helps improve chemotherapeutic regimens for different lung cancer types and also provides guidance on the best time for chest tube removal. At the same time, the design of rigorous animal experiments and continuous follow-up on the tube removal status and survival of patients are necessary.
Materials and methods
Patients and collection of DF
We obtained 16 DF samples from 16 lung cancer patients who underwent lobectomy. All patients had no known underlying diseases except lung neoplasm. Sixteen DF samples were used for the cell MTT proliferation test, and nine samples were used for the chemosensitivity test in vitro.
Supernatant from centrifuged DF samples was collected under sterile conditions and preserved at −80°C without additives. Written informed consent was obtained from the patients, and the study protocol was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of China Medical University.
Cell incubation
The DF specimens were sterilized and pretreated at 0°C before co-culture assays in vitro. Sixteen DF specimens were used to evaluate the influence of DF on lung cancer cell lines. LTEP-a-2 and A549 lung cancer cell lines were acquired from American Type Culture Collection (ATCC, Manassas, VA, USA). LTEP-a-2 and A549 cells were cultured in RPMI 1640 medium (ATCC) and in F-12K medium (ATCC) supplemented with 10% FBS (Sigma-Aldrich Co., St. Louis, MO, USA). Each experiment was repeated three times.
Cell death test and in vitro chemosensitivity test
We tested the survival potential and drug chemosensitivity of LTEP-a-2 and A549 cells by MTT assay. LTEP-a-2 and A549 cells (5×104/mL for the proliferation test and 10×104/mL for the in vitro chemosensitivity test) were seeded onto 96-well plates in 100 µL complete medium. Lung cells were incubated for 24 hours at 37°C, after which we replaced the medium with new complete medium for both groups. At this point, DF (0.1%, 0.5%, and 1%) samples were added to the treated groups’ medium. Some cells were used for in vitro chemosensitivity tests, which included two concentration levels (5 and 10 mg/L) of doxycycline or DDP. The remaining cells were used for proliferation tests. After 48 hours of incubation at 37°C, 10 µL MTT dye was added to each well and co-cultured with cells for 4 hours. The MTT solution was then removed. Formazan crystals were dissolved by adding 200 µL dimethyl sulfoxide to each well. Absorbance was measured at 570 nm with a microplate reader (Titertek Multiskan PLUS, MK II; Labsystems, McLean, VA, USA). Each experiment was repeated three times.
Flow cytometry analysis
LTEP-a-2 and A549 cells (1×105 cells/well) were seed into 24-well plates and incubated in complete medium overnight. Culture medium was then replaced with new complete medium for both groups, while DF (0.1% and 1%) samples were added to the treated groups’ medium at 37°C for 24 hours. The cells were then washed with PBS and sloughing cells were removed. The recombinant annexin V conjugated to green-fluorescent FITC dye was used to detect the externalization of phosphatidylserine, as a sign of apoptotic cells. The remaining cells were stained with anti-FITC and anti-PI, and the percentages of apoptotic cells in each individual group were determined using flow cytometry analysis. Each experiment was repeated three times.
Scratch wound test
LTEP-a-2 and A549 cells with 90% confluence were plated uniformly in complete medium in 24-well plates. Scratched cells were located at the bottom of the wells after 24 hours of incubation. Cell suspensions were freshly prepared for visualization in PBS. Initial scratch wounds (0 hour) were imaged at once. The medium was replaced, while DF (0.1% and 1%) was added to the treated groups’ medium. Scratch wounds after 48 hours incubation with DF were visualized under a microscope (Leica DM4000B; Leica Microsystems, Wetzlar, Germany). Each experiment was repeated three times.
Statistical analysis
We used IBM SPSS statistical version 22.0 software (IBM Corporation, Armonk, NY, USA). We made statistical figures using PRISM (version 5; GraphPad Software, Inc., La Jolla, CA, USA). The differences among groups were compared by analysis of variance, followed by a Student Newman Keuls post hoc test. P-values <0.05 were considered statistically significant.
Acknowledgments
This study was funded by the Liaoning Natural Science Foundation (No. 20180530020 and 20170520024).
Disclosure
The authors report no conflicts of interest in this work.
References
- ChenWZhengRBaadePDCancer statistics in China, 2015CA Cancer J Clin201666211513226808342
- TorreLABrayFSiegelRLFerlayJLortet-TieulentJJemalAGlobal Cancer statistics, 2012CA Cancer J Clin20156528710825651787
- CetinkayaEUsluerOYılmazAIs endobronchial ultrasound-guided transbronchial needle aspiration an effective diagnostic procedure in restaging of non-small cell lung cancer patients?Endosc Ultrasound20176316216728621292
- Chinese Thoracic Society, Chinese Alliance against Lung CancerChinese expert consensus statement on issues related to small specimen sampling of lung cancerEndosc Ultrasound20176421923028820144
- ChaudharyTChaharASharmaJKKaurKDangAPhytomedicine in the treatment of cancer: a health technology assessmentJ Clin Diagn Res2015912XC04XC0926816981
- Castro-PocasFMAraüjoTPFerreiramlSaraivaMMThe role of endoscopic ultrasound in a case of lung cancer with jaundiceEndosc Ultrasound201674279281
- BurdettSRydzewskaLHMTierneyJFNSCLC Meta-analysis Collaborative GroupPreoperative chemotherapy for non-small-cell lung cancer: a systematic review and meta-analysis of individual participant dataLancet201438399281561157124576776
- Gonzalez-RivasDUniportal thoracoscopic surgery: from medical thoracoscopy to non-intubated uniportal video-assisted major pulmonary resectionsAnn Cardiothorac Surg201652859127134833
- HarrisKModiKKumarADhillonSSEndobronchial ultrasound-guided transbronchial needle aspiration of pulmonary artery tumors: a systematic review (with video)Endosc Ultrasound20154319119726374576
- AswanetmaneePLimsuwatCKabachMAlraiyesAHKheirFThe role of sedation in endobronchial ultrasound-guided trans-bronchial needle aspiration: systematic reviewEndosc Ultrasound20165530030627803902
- DziedzicDPerytASzolkowskaMLangfortROrlowskiTEvaluation of the diagnostic utility of endobronchial ultrasound-guided transbronchial needle aspiration for metastatic mediastinal tumorsEndosc Ultrasound20165317317727386474
- KehletHFast-track colorectal surgeryLancet2008371961579179318328911
- MullerSZalunardoMPHubnerMClavienPADemartinesNZurich Fast Track Study GroupA fast-track program reduces complications and length of hospital stay after open colonic surgeryGastroenterology2009136384284719135997
- DongQZhangKCaoSCuiJFast-track surgery versus conventional perioperative management of lung cancer-associated pneumonectomy: a randomized controlled clinical trialWorld J Surg Oncol20171512028086896
- CerfolioRJBryantASResults of a prospective algorithm to remove chest tubes after pulmonary resection with high outputJ Thorac Cardiovasc Surg2008135226927318242249
- WangDHuKGaoNHigh throughput screening of cytokines, chemokines and matrix metalloproteinases in wound fluid induced by mammary surgeryOncotarget2015630292962931026313265
- Valeta-MagaraAHatamiRAxelrodDPro-oncogenic cytokines and growth factors are differentially expressed in the post-surgical wound fluid from malignant compared to benign breast lesionsSpringerplus2015448326361584
- ZhangYYanDZhangHInfluence of wound fluid on chemotherapy sensitivity in primary breast cancer cellsOncotarget2016740650346504127542254
- BartonMKPatients of all ages with advanced non-small cell lung cancer are not receiving chemotherapyCA Cancer J Clin201565533733826173576
- LesinaMKurkowskiMULudesKSTAT3/SOCS3 activation by IL-6 transsignaling promotes progression of pancreatic intraepithelial neoplasia and development of pancreatic cancerCancer Cell201119445646921481788
- GrivennikovSKarinETerzicJIL-6 and STAT3 are required for survival of intestinal epithelial cells and development of colitis-associated cancerCancer Cell200915210311319185845
- CutlerSJDoeckeJDGhazawiINovel STAT binding elements mediate IL-6 regulation of MMP-1 and MMP-3Sci Rep201771852628819304
- HeGDharDNakagawaHIdentification of liver cancer progenitors whose malignant progression depends on autocrine IL-6 signalingCell2013155238439624120137