
Abstract
Background
Type 2 diabetes mellitus has been proved to be a risk factor of hepatocellular carcinoma, but how diabetes affects incidence of hepatocellular carcinoma among patients with chronic hepatitis B virus infection remains controversial.
Methods
A comprehensive search of Medline and Embase was performed. Incidence of hepatocellular carcinoma in chronic hepatitis B patients was the primary outcome. Pooled HRs and 95% CIs were calculated to assess the correlation between diabetes and incidence of hepatocellular carcinoma.
Results
Five cohort studies and two case–control studies were identified, with a total of 21,842 chronic hepatitis B patients. The diabetes mellitus cohort was found to have increased incidence of hepatocellular carcinoma (pooled HR 1.77, 95% CI 1.28–2.47; fixed effect) and worse overall mortality (pooled RR 1.93, 95% CI 1.64–2.27; fixed effect) in comparison with those without diabetes. In case–control studies, hepatocellular carcinoma cases were found to have an insignificantly elevated diabetes mellitus rate in comparison with the control group.
Conclusion
Type 2 diabetes mellitus is significantly associated with increased risk of hepatocellular carcinoma among patients with chronic hepatitis B virus infection, and aggressive management of diabetes mellitus is strongly suggested.
Introduction
Hepatocellular carcinoma (HCC) is the fifth-most common cancer worldwide, leads to nearly 1 million deaths every year,Citation1 and is the third-most frequent cause of cancer-related death. The incidence of HCC is particularly high in Asia (over 20 in 100,000 men and over ten in 100,000 women) and in Africa, intermediate in southern Europe, and much lower in most developed countries.Citation2 Hepatitis virus infection, mainly hepatitis B virus (HBV) and hepatitis C virus (HCV), has been widely accepted as the major recognized risk factor of HCC globally, accounting for over three-quarters of primary HCC cases.Citation2,Citation3 However, when HBV or HCV is not involved, the etiologic factor of HCC varies, of which diabetes mellitus (DM),Citation4 heavy alcohol drinking,Citation5 smoking,Citation6 obesity,Citation7 and aflatoxinCitation8 are relatively important.
DM, which has been proved to be a risk factor of various kinds of malignancies, is strongly associated with nonalcoholic fatty-liver disease and many other metabolic processes.Citation9 Insulin resistanceCitation10 was believed to play an important role in hepatocarcinogenesis in HBV patients with type 2 DM or even prediabetes.Citation11 The association between DM and HCC risk was indicated to be independent of cirrhosis, though most HCC cases presented with cirrhosis.Citation12 A recent systematic review demonstrated that concurrent DM is strongly associated with increased HCC risk among chronic HCV patients,Citation13 but scanty evidence is available about the correlation between DM and HCC in chronic HBV (CHB) patients. The clinical landscape of HCV is currently facing a great change, such that its cure would be universal for patients for whomever has access to effective therapy, which will definitely result in a decrease in HCC developments. Therefore, HBV infection, alcohol consumption, and metabolic disorders, such as DM and obesity, are supposed to be the leading etiologic factors of HCC in the coming future. There are mixed resultsCitation14–Citation17 of the few studies on the association between DM and the risk of HCC in patients with CHB. As such, we performed this meta-analysis and systematic review of the literature to achieve further understanding of the impact of DM on the risk of developing HCC in patients with CHB.
Methods
Literature-search strategy
A comprehensive search of Medline and Embase was performed to retrieve studies published in English (cutoff date February 5, 2018) using the keywords “diabetes” or “diabetes mellitus, type 2” or “DM”, “hepatitis B” or “HBV”, and “hepatocellular carcinoma” or “HCC” or “liver cancer”. We also examined the reference lists of eligible studies to identify additional articles, in order to guarantee a systemic search. depicts the search strategy in detail.
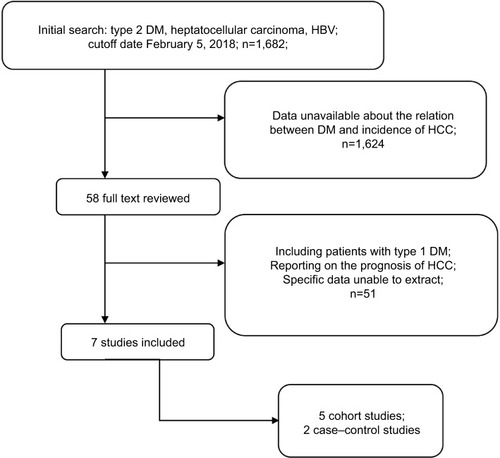
Figure 1 Flow diagram showing the search strategy along with the selection and screening processes for the eligible studies.
Abbreviations: DM, diabetes mellitus; HCC, hepatocellular carcinoma; HBV, hepatitis C virus.
Inclusion and exclusion criteria
Inclusion criteria from the literature search were: studies that focused on the relationship between DM and the risk of HCC: HCC incidence and/or related mortality as outcomes; results of HR/RR/OR and their corresponding 95% CIs for DM and incidence of HCC; and if two or more studies were reported on the same cohort and objectives, either the higher-quality publication or more recent publication was included in the analysis. Studies were excluded if they had not presented data on the relationship between DM and incidence of HCC in patients with HBV infection or specific results were unable to extract. Studies reporting on the effect of DM on the prognosis of HCC or where HCC was not the only outcome (eg, including cholangiocarcinoma) or including patients with type 1 DM were not considered. Reviews, case reports, letters, animal or in vitro studies, conference abstracts, and non-peer-reviewed articles were also excluded from the meta-analysis.
Assessment of quality of articles according to the New-castle–Ottawa Scale, and data extraction were independently performed by YT and SW, as well as the literature search. Quality assessment of both cohort studies and case–control studies included three main characteristics: selection of groups, comparability of cohorts/cases and controls, and outcome/exposure. Studies with seven or more scores were defined as highly qualified.
Data extraction
Incidence of HCC was the main outcome assessed in this meta-analysis, while overall mortality or HCC-related mortality was the secondary main outcome. HR, RR, and OR values with their corresponding 95% CIs were extracted from each study. Other information included (but was not limited to) study design, population characteristics, source of cases and controls, ascertainment of type 2 DM, treatment for HBV infection, anti-HCV status, variables adjusted for in the multivariate regression models, and the measure of association between DM and HCC incidence.
Statistical analysis and exploration of heterogeneity
We used pooled HRs for primary outcomes to assess the relationship between type 2 DM and incidence of HCC in HBV patients. RRs and weighted mean differences, both with corresponding 95% CIs, were computed for binary data and continuous data, respectively. Funnel plots were visually inspected to identify publication bias. Sensitivity analysis was conducted by removing a single study each time and recalculating pooled results of the remaining studies. The χ2 test was used to explore potential heterogeneity with I2 and P-values. I2>50% or P<0.10 was defined as increased heterogeneity and a random-effect modelCitation18 used, while a fixed model was used when P>0.10. Results are presented as P-values and 95% CIs, where appropriate, and two-sided P<0.05 was considered to indicate statistical significance. Meta-analyses were performed using RevMan software (version 5.3.5; Cochrane Collaboration, Copenhagen). Quality of evidence was evaluated using the software GradePro, comprising four levels: high quality, moderate quality, low quality, and very low quality.
Results
The online search initially found 1,682 studies, and 1,624 were excluded after screening of titles and abstracts. A total of 58 full-text articles were reviewed. Finally, two case–control studiesCitation17,Citation19 and five cohort studiesCitation14–Citation16,Citation20,Citation21 were identified, of which six were conducted in AsiaCitation14–Citation17,Citation19,Citation20 and one in New Zealand.Citation21 In all cohort studies, patients diagnosed with HCC before the inception point were excluded. The number of eligible CHB patients ranged from 223 to 6,545, with a total of 21,842. Diagnosis of type 2 DM was obtained from patient self-report, abnormal fasting/random glucose, positive oral glucose tolerance test, and DM management (oral hyperglycemic agent or insulin injection). HCC cases were confirmed with the combination of increased AFP and imaging findings (ultrasound, enhanced computed tomography, or angiography) in five studies,Citation14,Citation15,Citation17,Citation19,Citation21 and positive histology or cytology was also used to define HCC in the two case– control studies.Citation17,Citation19 Two cohort studiesCitation16,Citation20 in Taiwan defined HCC cases according to the national cancer registry alone (). Only Hsiang et alCitation21 reported details of dropouts and withdrawals. In their study, seven patients were lost to follow-up or moved overseas, resulting in a loss to or unavailability for follow-up rate of 3%. Other studies, however, did not provided data about details of follow up.
Table 1 Baseline characteristics of the seven studies included
No statistical differences were found between subjects with and without type 2 DM for average age (mean difference 2.81, 95% CI −2.91 to 8.52), male sex (RR 0.99, 95% CI 0.91–1.08), years of follow-up (mean difference −0.35, 95% CI −1.02 to 0.32), or HBV-treatment rate (RR 1.07, 95% CI 0.73–1.55).
Type 2 DM and risk of HCC in CHB subjects
Of the seven studies included in this meta-analysis, three cohort studiesCitation15,Citation20,Citation21 and one case–control studyCitation17 demonstrated a positive association between type 2 DM and risk of HCC in CHB patients, while other two cohort studiesCitation14,Citation16 and one case–control studyCitation19 failed to find a statistical difference between the two groups. Four in seven studies reported correlations between DM and HCC with HRs,Citation14,Citation16,Citation20,Citation21 two with ORs,Citation17,Citation19 and another with RRs,Citation15 all with corresponding 95% CIs (). All studies had different variables adjusted in multivariate regression analysis ().
Table 2 DM and incidence of HCC risk
Table 3 Factors adjusted in the multivariate regression analysis
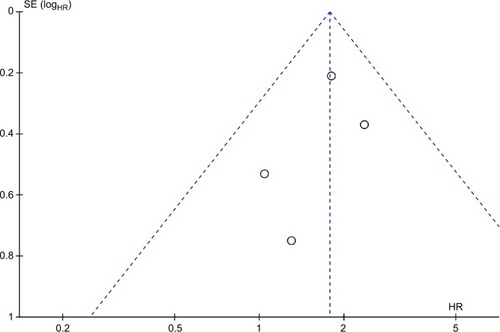
The incidence of HCC in DM cohorts varied from 3.29% to 26.0% in cohort studies, while the rate was 2.02%–13.3% in the non-DM group. The four cohort studies reporting on HRCitation14,Citation16,Citation20,Citation21 found increased incidence of HCC among patients with DM over those without DM among CHB patients (), resulting in a pooled HR of 1.77 (95%CI 1.28–2.47, heterogeneity I2=0; fixed effect). In case–control studies,Citation17,Citation19 an elevated DM rate was indicated in HCC cases in comparison with control groups (12.35% vs 6.53%), but not statistically, with an RR of 2.10 (95% CI 0.84–5.25; random-effect). Among the three studies reporting RRs or ORs, Chen et alCitation15 and Ko et alCitation17 also found significant associations between type 2 DM and risk of HCC in HBV subjects, with an RR of 2.41 (95% CI 1.17–4.95) and an OR of 4.32 (95% CI 1.92–9.70), respectively, but Li et alCitation19 found no significant relationships between DM and risk of HCC when comparing all HCC cases with cross-sectional controls, with an OR of 0.9 (95% CI 0.7–1.2). The publication bias of studies assessing the relation between DM and risk of HCC is shown in .
Figure 2 Forest plot of meta-analysis results comparing the incidence of HCC between patients with DM and those without DM.
Abbreviations: HCC, hepatocellular carcinoma; DM, diabetes mellitus.
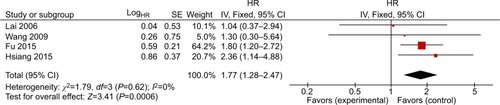
Figure 3 Funnel plot of studies assessing the relationship between DM and risk of HCC.
Abbreviations: DM, diabetes mellitus; HCC, hepatocellular carcinoma.
Analysis of sensibility was carried out by excluding one article at a time to guarantee stability of the meta-analysis. As a result, pooled results remained statistically positive when any of the cohort studies was excluded from the meta-analysis. For example, when Wang et al was excluded, the pooled HR of remaining studies remained at 1.80 (95% CI 1.29–2.53). When it came to heterogeneity, I2 remained at 0 when any study was excluded.
DM, overall mortality, and HCC-related mortality
Two cohort studiesCitation20,Citation21 reported overall mortality between two groups, revealing that subjects with type 2 DM suffered significantly higher overall mortality in comparison with those without DM (), with a pooled RR of 1.93 (95% CI 1.64–2.27, I2=18%; fixed effect). Only Hsiang et alCitation21 reported on HCC-related mortality in patients with CHB, and patients assigned to the DM group had significantly higher HCC-related mortality than those in the non-DM group (27.9 vs 8.8 per 1,000 patient-years, P=0.02). They also demonstrated increased liver-related mortality or orthotopic liver-transplantation rate in the DM group, at 23.4%, compared to the non-DM group, at 9.4% (P=0.009).
Figure 4 Forest plot of results comparing overall mortality between DM and non-DM subjects.
Abbreviations: DM, diabetes mellitus; NDM, non-DM; M–H, Mantel–Haenszel.

Risk of bias and quality evaluation of evidence
We conducted a quality evaluation on all five cohort studies and two case–control studies included, based on the coding manual for cohort-studies and for case–control studies. All studies scored at least 6, and five studies scored 7 or more. The main outcomes and some other results are summarized in . The evidence was considered to be of low quality.
Table 4 Quality evaluation of evidence
Discussion
Chronic hepatitis virus infection, including HBV and HCV,Citation22 has always been widely acknowledged as a major risk factor of primary HCC. DM, as well as other metabolic abnormalities, has been proved to be associated with quite a few kinds of malignancies,Citation23,Citation24 and this association was suggested not to be mediated by body-mass index.Citation25 A recent meta-analysisCitation26 and a systemic reviewCitation13 demonstrated a strong associations between concurrent DM and risk of HCC among chronic HCV patients. While well studied in anti-HCV-positive subjects, the potential relationship of type 2 DM and risk of HCC in the HBV-infected population remains unclear. In addition, with effective treatment for HCV infection, HCV-related HCC cases are expected to decrease worldwide.Citation27 Therefore, HBV infection and metabolic factors, including obesity, DM, and hyperlipidemia, are predicted to account for most of the increase in HCC.
Five cohort studies and two case–control studies were included in the current meta-analysis, with >20,000 individuals enrolled. A recent meta-analysis by Chen et alCitation26 summarized three studies (two reporting with HRs and the other with RRs), revealing a similar risk of HCC in diabetics without DM among CHB patients. However, in the current meta-analysis, we found a significant association between type 2 DM and increasing incidence of HCC among CHB patients, with a pooled HR of 1.77 (95% CI 1.28–2.47) and no heterogeneity detected (I2=0). Previous meta-analyses have failed to find statistical differences between the two groups, possibly due to the small number of studies included and statistical issues, as not all results were presented with HRs. The biological mechanism for how type 2 DM influences HCC development is not well understood and remains controversial. Most researchers have suggested that type 2 DM contributes to HCC development independently or synergetically with other risk factors, such as HBVCitation28 or HCVCitation29,Citation30 infection and alcohol consumption.Citation31
Though relatively uncommon in the setting of HCC, DM is of growing importance, because of its rapidly increasing incidence among adults, as well as nonalcoholic fatty-liver disease, especially in developed countries.Citation9 It has been reported that type 2 DM and/or obesity had the greatest population-attributable fractions (36.6%) and proportion of cases that could be attributed to specific risk factors: to HCC, higher than alcohol-related disorders (23.5%) or HCV (22.4%).Citation32 Insulin resistanceCitation9,Citation33 and hyperinsulinemiaCitation34,Citation35 are believed to be key factors of HCC oncogenesis in diabetics, mostly through the process of inflammation and cellular injury.Citation36–Citation38 While playing an important role in glucose and lipid metabolism, insulin also has pleiotropic effects on regulation of inflammation and cell proliferation. IGF1, the most powerful activator of cellular proliferation, and IRS1 are crucial downstream targets of insulin.Citation36 HCC cells have been found to overexpressCitation39 IGF1 and IRS1, revealing that they are of great importance in the process of HCC development. On the other hand, the inflammatory milieu caused by insulin resistance and nonalcoholic steatohepatitis leads to multiple pathways of inflammatory processes, which in return activated oncogenic signaling pathways, such as PI3K–PTEN–Akt and JAK–STAT.Citation9 Insulin resistance also causes hepatic inflammation and fibrosis by the accumulation of fat within hepatocytes, which produces oxidative stress and results in hepatosteatosis.Citation40 All these activations of pathways are associated with cellular proliferation promotion, increased angiogenesis, and decreased apoptosis, which finally lead to HCC development.
DM was also found to be a poor prognostic factor for overall mortality in the cohort of patients with CHB infection (RR 2.33, 95% CI 1.64–3.31) in the current meta-analysis, which echoed previous studies of worse overall mortality and HCC recurrence after potential curative therapy in patients with DM.Citation41,Citation42 DM has been attributed to increases in both HCC related mortality and mortality from other causes, such as cardiovascular factors.Citation21 Since insulin resistance and hyperinsulinemia are key factors in the process of hepatocarcinogenesis, any other underlying disease or medication that affects the insulin level is a potential risk factor for the progression of HCC. Several studiesCitation21,Citation43,Citation44 have demonstrated higher incidence of HCC among HBV subjects who were treated with insulin or antidiabetic drugs that increase circulating insulin, while metformin, which is supposed to improve insulin sensibility, has been reported to be related to declined HCC risk and mortality.Citation45,Citation46 Therefore, we recommend better management of DM and cautious selection of therapy for DM in CHB patients.
In our meta-analysis, five studies were conducted in Tai-wan. Although they were conducted using different databases in different periods (), it is still difficult to confirm whether the cohort pool used in each study was completely different. Besides, methods used to identify HCC and DM were different in the studies included. Therefore, we think this may be a limitation of our study, and our results should be interpreted with caution.
The major limitation involves the variability of the adjustments within the studies. As is well known, HCC is related to quite a few independent risk factors, of which HBV DNA levels, antiviral therapy, and liver cirrhosis are of great importance. However, specific data about these effecting factors were not available in most of the studies included in this meta-analysis. Three studiesCitation19–Citation21 clearly adjusted for cirrhosis in the multivariate analysis, twoCitation20,Citation21 adjusted for antiviral therapy, and oneCitation19 just excluded patients who accepted antiviral therapy, while only oneCitation21 adjusted sustained viral suppression (HBV viral load <3log IU/mL on at least two occasions 6 months apart). Also, the evaluation of evidence turned out to be of low quality. All seven studies included were observational: five cohort studies and two case–control studies. Many of the researches did not report on the details of follow-up, including precise follow-up years of both groups and loss rate. More well-designed research and randomized controlled trials are needed to confirm further the association between type 2 DM and the risk of HCC. Though the evidence was evaluated as low quality, most studies were designed to minimize potential bias by adjusting for age, sex, and other covariates that were possibly influential ().
Consequently, the findings of type 2 DM significantly related to HCC risk may shed some light on the prevention of HCC. Better management of DM and correlated metabolic factors is strongly recommended, and HBV patients with DM should be tested more frequently, in order to improve early detection of HCC or other malignancies.
Acknowledgments
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
- LombardiAGrimaldiAZappavignaSMissoGCaragliaMHepatocarcinoma: genetic and epigenetic featuresMinerva Gastroenterol Dietol2018641142728398025
- BosettiCTuratiFLa VecchiaCHepatocellular carcinoma epidemiologyBest Pract Res Clin Gastroenterol201428575377025260306
- GüthleMDollingerMMEpidemiología y factores de riesgo de carcinoma hepatocelular. [Epidemiology and risk factors of hepatocellular carcinoma]Radiologe2014547654659 German24973122
- WangPKangDCaoWWangYLiuZDiabetes mellitus and risk of hepatocellular carcinoma: a systematic review and meta-analysisDiabetes Metab Res Rev201228210912221898753
- ChuangSCLeeYCWuGJStraifKHashibeMAlcohol consumption and liver cancer risk: a meta-analysisCancer Causes Control20152691205123126134046
- LeeYCCohetCYangYCStaynerLHashibeMStraifKMeta-analysis of epidemiologic studies on cigarette smoking and liver cancerInt J Epidemiol20093861497151119720726
- CalleEERodriguezCWalker-ThurmondKThunMJOverweight, obesity, and mortality from cancer in a prospectively studied cohort of U.S. adultsN Engl J Med2003348171625163812711737
- WilliamsJHPhillipsTDJollyPEStilesJKJollyCMAggarwalDHuman aflatoxicosis in developing countries: a review of toxicology, exposure, potential health consequences, and interventionsAm J Clin Nutr20048051106112215531656
- NoureddinMRinellaMENonalcoholic fatty liver disease, diabetes, obesity, and hepatocellular carcinomaClin Liver Dis201519236137925921668
- YuJShenJSunTTZhangXWongNObesity, insulin resistance, NASH and hepatocellular carcinomaSemin Cancer Biol2013236 Pt B48349123876851
- HuangYCaiXQiuMPrediabetes and the risk of cancer: a meta-analysisDiabetologia201457112261226925208757
- KasmariAJWelchALiuGLeslieDMcGarrityTRileyTIndependent of cirrhosis, hepatocellular carcinoma risk is increased with diabetes and metabolic syndromeAm J Med20171306746.e174746
- DyalHKAguilarMBartosGDiabetes mellitus increases risk of hepatocellular carcinoma in chronic hepatitis C virus patients: a systematic reviewDig Dis Sci201661263664526703125
- LaiMSHsiehMSChiuYHChenTHType 2 diabetes and hepatocellular carcinoma: a cohort study in high prevalence area of hepatitis virus infectionHepatology20064361295130216729295
- ChenCLYangHIYangWSMetabolic factors and risk of hepatocellular carcinoma by chronic hepatitis B/C infection: a follow-up study in TaiwanGastroenterology2008135111112118505690
- WangCSYaoWJChangTTWangSTChouPThe impact of type 2 diabetes on the development of hepatocellular carcinoma in different viral hepatitis statusesCancer Epidemiol Biomarkers Prev20091872054206019549812
- KoWHChiuSYYangKCChenHHDiabetes, hepatitis virus infection and hepatocellular carcinoma: a case-control study in hepatitis endemic areaHepatol Res201242877478122469194
- DersimonianRLairdNMeta-analysis in clinical trialsControl Clin Trials1986731771883802833
- LiQLiWWYangXType 2 diabetes and hepatocellular carcinoma: a case-control study in patients with chronic hepatitis BInt J Cancer201213151197120222052244
- FuSCHuangYWWangTCHuJTChenDSYangSSIncreased risk of hepatocellular carcinoma in chronic hepatitis B patients with new onset diabetes: a nationwide cohort studyAliment Pharmacol Ther201541111200120925846548
- HsiangJCGaneEJBaiWWGerredSJType 2 diabetes: a risk factor for liver mortality and complications in hepatitis B cirrhosis patientsJ Gastroenterol Hepatol201530359159925250942
- El-SeragHBMasonACRisk factors for the rising rates of primary liver cancer in the United StatesArch Intern Med2000160213227323011088082
- SasazukiSCharvatHHaraADiabetes mellitus and cancer risk: pooled analysis of eight cohort studies in JapanCancer Sci2013104111499150723889822
- Starup-LindeJKarlstadOEriksenSACARING (CAncer Risk and INsulin analoGues): the association of diabetes mellitus and cancer risk with focus on possible determinants - a systematic review and a meta-analysisCurr Drug Saf20138529633224215312
- KingLYKhaliliHHuangESDiabetes mellitus is associated with an increased risk of HCC in a large prospective cohort with long term follow-upHepatology201460281A
- ChenJHanYXuCXiaoTWangBEffect of type 2 diabetes mellitus on the risk for hepatocellular carcinoma in chronic liver diseases: a meta-analysis of cohort studiesEur J Cancer Prev2015242899924809655
- CholankerilGPatelRKhuranaSSatapathySKHepatocellular carcinoma in non-alcoholic steatohepatitis: current knowledge and implications for managementWorld J Hepatol201791153354328469809
- ZhengZZhangCYanJDiabetes mellitus is associated with hepatocellular carcinoma: a retrospective case-control study in hepatitis endemic areaPLoS One2013812e8477624386416
- HungC-HLeeC-MWangJ-HImpact of diabetes mellitus on incidence of hepatocellular carcinoma in chronic hepatitis C patients treated with interferon-based antiviral therapyInt J Cancer2011128102344235220669224
- AraseYKobayashiMSuzukiFEffect of type 2 diabetes on risk for malignancies includes hepatocellular carcinoma in chronic hepatitis CHepatology201357396497322991257
- HassanMMHwangLYHattenCJRisk factors for hepatocellular carcinoma: synergism of alcohol with viral hepatitis and diabetes mellitusHepatology20023651206121312395331
- WelzelTMGraubardBIQuraishiSPopulation-attributable fractions of risk factors for hepatocellular carcinoma in the United StatesAm J Gastroenterol201310881314132123752878
- FarrellGInsulin resistance, obesity, and liver cancerClin Gastroenterol Hepatol201412111711923954644
- BalkauBKahnHSCourbonDEschwègeEDucimetièrePParis Prospective StudyHyperinsulinemia predicts fatal liver cancer but is inversely associated with fatal cancer at some other sites: the Paris prospective studyDiabetes Care200124584384911347741
- BabaHTsuneyamaKHyperinsulinemia rather than hyperglycemia can accelerate the progression of hepatocellular carcinomaHepatology201591 Suppl 1S318S19
- MooreMAParkCBTsudaHImplications of the hyperinsulinaemia-diabetes-cancer link for preventive effortsEur J Cancer Prev199872891079818771
- TanakaSMohrLSchmidtEVSugimachiKWandsJRBiological effects of human insulin receptor substrate-1 overexpression in hepatocytesHepatology19972635986049303488
- LongatoLde La MonteSKuzushitaNOverexpression of insulin receptor substrate-1 and hepatitis Bx genes causes premalignant alterations in the liverHepatology20094961935194319475691
- AmpueroJRomero-GomezMPrevention of hepatocellular carcinoma by correction of metabolic abnormalities: role of statins and metforminWorld J Hepatol2015781105111126052399
- FarrellGCLarterCZNonalcoholic fatty liver disease: from steatosis to cirrhosisHepatology2006432 Suppl 1S99S11216447287
- KawamuraYIkedaKAraseYDiabetes mellitus worsens the recurrence rate after potentially curative therapy in patients with hepatocellular carcinoma associated with nonviral hepatitisJ Gastroenterol Hepatol200823111739174618713301
- TingCTChenRCChenCCLiuMHChuDKuoNWDiabetes worsens the surgical outcomes in cirrhotic patients with hepatocellular carcinomaTohoku J Exp Med20122271738122688467
- TateishiROkanoueTOkitaKP572 insulin use is related to the development of hepatocellular carcinoma at younger age with non-viral etiologyJ Hepatol2014601S260
- BosettiCFranchiMNicotraFInsulin and other antidiabetic drugs and hepatocellular carcinoma risk: a nested case-control study based on Italian healthcare utilization databasesPharmacoepidemiol Drug Saf201524777177826013675
- ZhangXHarmsenWSMettlerTAContinuation of metformin use after a diagnosis of cirrhosis significantly improves survival of patients with diabetesHepatology20146062008201624798175
- DonadonVBalbiMMasMDCasarinPZanetteGMetformin and reduced risk of hepatocellular carcinoma in diabetic patients with chronic liver diseaseLiver Int201030575075820331505