
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Purpose
The effects of age, period, and cohort on mortality rates of bladder cancer in China remained vague. This study aimed to analyze the secular trends of bladder cancer mortality in China and estimate the independent effects of age, period, and cohort.
Methods
Data for bladder cancer mortality from 1991 to 2015 was obtained from the WHO Mortality Database and China Health Statistical Yearbook. The age-period-cohort model was used to estimate the effect of age, period, and cohort. The intrinsic estimator method was used to solve the nonidentification problem of collinearity among age, period, and cohort.
Results
The age-standardized mortality rates of total residents (2.33–1.87/100,000), male (3.45–2.89/100,000), and female (1.24–0.82/100,000) showed decreasing trends, which was more obvious in males than in females. Age effects increased consistently with age in all age groups (coefficients: −2.02 to 1.91 in the total population, −2.06 to 2.02 in males and −2.04 to 1.81 in females). Cohort effects decreased overall (coefficients: 0.96 to −1.62 in the total population, 1.11 to −1.66 in males and 0.78 to −1.46 in females). Period effects were not found in China.
Conclusion
Although a decreasing mortality was observed, the bladder cancer burden in China will likely increase in the next few years due to population aging, environmental pollution, and food safety. The findings suggested that preventive measures should be taken corresponding to the changes in age-and cohort-related factors in the population.
Introduction
As one of the most common cancer of the urinary system, bladder cancer is the 9th most common cancer and 14th leading cause of cancer deaths worldwide, with an estimated 430,000 new cases and 165,100 deaths in 2012.Citation1 Bladder cancer incidence and mortality rates have decreased slightly in most developed countries.Citation2 Incidence and mortality rates in general decreased in most Western countries but increased in some Eastern European and developing countries, which leads to the burden of bladder cancer has been increasing.Citation3 These changes could be caused by the exposure to risk factors for bladder cancer, including tobacco consumption, air pollution, urbanization and industrialization, and unhealthy lifestyles, which could be summarized as a cohort effect.Citation4 In addition, the aging population, the development of death registration systems and changes in the ICD also contributed to changes in bladder cancer burden.Citation5 We classified these factors as age effect and period effect. Pou et alCitation6 used the age-period-cohort (APC) model to analyze the effects of age, period, and cohort on the mortality of bladder cancer in Córdoba, a province of Argentina, and suggested that mortality of bladder cancer is influenced by age and cohort.
China has experienced rapid economic growth and social change since the adoption of economic reforms from 1978 onward. As a result of this process, the epidemiological transition and the attendant rise in the chronic disease burden have taken place more rapidly than other countries.Citation7 Bladder cancer is the sixth most common cancer in males and 15th in females according to the National Central Cancer Registry (NCCR) of China 2015 annual report.Citation8 The incidence and mortality rates in China have increased graduallyCitation9 and shown different trends between males and femalesCitation10 over the past few years. Increasing trends in incidence were observed for bladder cancer from 1973 to 2010 in urban Shanghai.Citation5 Han et alCitation11 and Wen et al Citation12 have examined the time trends of bladder cancer mortality using the data from the NCCR, but these studies did not reveal the effects of age, period, and cohort on bladder cancer mortality trends. Guo et alCitation10 has estimated the bladder cancer cohort effect with generalized additive models using the national data, whereas the study ignored the effects of age and period due to the nonidentification problem of collinearity among age, period, and cohort.
Up until the present day, the effects of age, period, and cohort on bladder cancer mortality trends in China have remained vague. In this study, we examined the secular trends in bladder cancer mortality in China during the period 1991–2015 and analyzed the independent effects of chronological age, time period, and birth cohort simultaneously using the APC model combined with the intrinsic estimator (IE) algorithm, which could solve the nonidentification problem mentioned above.
Methods
Materials
The bladder cancer mortality data accessed is freely available from the WHO Cancer Mortality Database (International Agency for Research on Cancer, Lyon, France) for the period 1991–2000 and the China Public Health Statistical Yearbooks for the period 2002–2015. We replaced data in 2001 with the average of the four neighboring calendar years for 1999–2003 as it was unavailable.Citation13 Data of 31 provinces was reported by the Center for Health Information and Statistics of China, which is an annual disease surveillance system set up in 1973 and based upon a 10% sample of the population.Citation14
Bladder cancer patients aged 35–84 years were included in this study for the following reasons: the group aged ≥85 years did not meet the requirements of the APC models; the intervals of age and cohort need to be consistent; and the bladder cancer mortality of younger groups aged <35 years was approximately zero. Age, period, and cohort models were based on ten 5-year age intervals beginning at age 35 years (35–39, 40–44, 45–49, 50–54, 55–59, 60–64, 65–69, 70–74, 75–79, 80–84) and five 5-year period groups (1991–1995, 1996–2000, 2001–2005, 2006–2010, 2011–2015). Age-standardized mortality rates (ASMRs) were calculated based on the data of the National Population Sampling Survey in 2015.
Methods
The APC model was used to estimate the effect of age, period, and cohort on bladder cancer mortality and the IE method was used to solve the nonidentification problem that the age, period, and cohort were collinear.Citation15 The equation of the multiplicative APC model for mortalities rates is denoted as:
Results
Overall trends of bladder cancer mortality rates
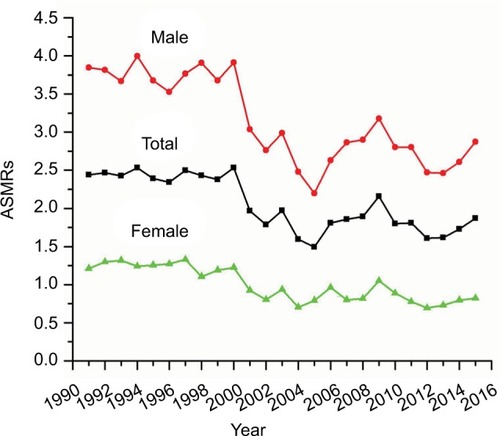
shows the ASMRs of bladder cancer from 1991 to 2015. Decreasing trends was observed in male, female, and total residents. The rate of decrease was more obvious in males than females.
Figure 1 Trends of ASMRs/100,000 population for bladder cancer in China.
Abbreviation: ASMRs, age-standardized mortality rates.
Age-specific bladder cancer mortality rates by time period and cohort
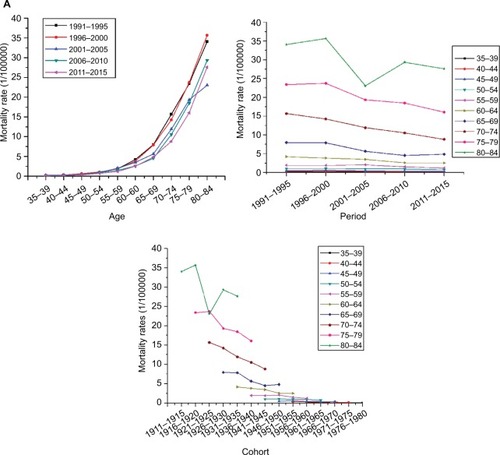
Age-specific bladder cancer mortality rates by period are shown in . Overall bladder cancer mortality rates increased with age and this trend was more obvious in the >65 years age groups. The mortality rate for those aged 80–84 years was nearly 300-fold higher than for those aged 35–39 years in total residents. The multiples were 500 in male residents and 100 in female residents.
Figure 2 Age, period, and cohort-specific mortality rates for bladder cancer/100,000 population in China.
Note: (A) Shows the bladder cancer mortality of total population; (B) shows the bladder cancer mortality of males; and (C) shows the bladder cancer mortality of females.

Period-specific bladder cancer mortality rates by age group
plots period-specific bladder cancer mortality rates by age group. The mortality rates showed stable trends in the ≤64 years age groups and a rapidly decreasing trend in the 65–79 years age groups. In the 80–84 years age group, the mortality rates during the period 2001–2005 were lower than the other periods.
Cohort-specific bladder cancer mortality rates by age group
As shows, the cohort-specific mortality rates of bladder cancer shared analogous trends with period-specific bladder cancer mortality rates. Mortality rates fluctuated slightly in the ≤64 years age groups and the >64 years age groups had a higher risk of mortality than the ≤64 years age groups. Bladder cancer mortality increased with age during the same cohort, especially in cohorts before 1946.
APC model
shows the results of the full APC IE model. The net effects of age, period, and cohort on overall mortality trends can be seen in . The separate effects of age, period, and cohort can be seen in .
Figure 3 Age, period, and cohort effects on bladder cancer mortality in China and the corresponding 95% CIs.
Note: (A) Shows the bladder cancer mortality of total population; (B) shows the bladder cancer mortality of males; and (C) shows the bladder cancer mortality of females.
Abbreviation: APC, age-period-cohort.
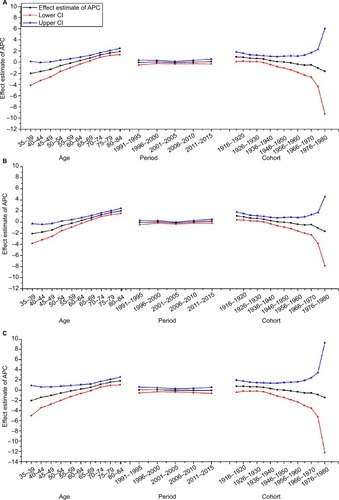
Table 1 APC model analysis of bladder cancer mortality in China by gender
Age effect
The coefficients of age effect increased consistently in all age groups. The age effect was found to be stronger in females than males aged ≤59 years and the age effect was more pronounced in males than females aged >59 years. Therefore, the effect of age on mortality increased faster in the male residents. Furthermore, the population aged ≤49 years showed lower risk among male residents. The high-risk groups are aged >65 years for males and >70 years for females.
Period effect
As shows, the mortality rates of bladder cancer did not change during the observed periods. Therefore, there was no evidence to prove the period was a contributing factor in the trend of mortality rates.
Cohort effect
The cohort effects decreased in the male, female, and total population. In males, the cohort coefficients before 1931 were greater than zero and have statistical significance. This reveals that the population born before 1931 showed a greater risk of death from bladder cancer for male residents. As for females, none of the cohort coefficients had statistical significance. This finding indicates that the cohort is a factor that affects bladder cancer mortality in males only.
Discussion
In this study, bladder cancer mortality data from 1991 to 2015 was obtained to examine the secular trend of bladder cancer mortality in mainland China and APC analysis was used to explored age, period, and cohort effects. The results showed that the ASMRs presented a decreasing trend, which was more obvious in males than females. Furthermore, age effects increased consistently with age in all age groups, cohort effects decreased overall in the total population, and period effects were not observed in this study. These detections not only provide a comprehensive and up-to-date overview of temporal trends in bladder cancer mortality in China over the past 25 years but also produce some evidence for the prevention and control of bladder cancer.
The overall decreasing trends were observed in the total population and population by gender, which was clearer in males, consistent with the results of Guo et alCitation10 and Antoni et al.Citation2 Bladder cancer incidence was influenced by the environmental, industrial, and economic development of China, but the mortality is mainly determined by the treatment. Health care policy with regard to cancer, such as early detection and early diagnosis, is effective for improving treatment quality and reducing the mortality rate of bladder cancer in China. The disparity among genders may be interpreted by differential exposure to carcinogens and genetic and environmental factors, especially tobacco consumption.Citation18 Nonetheless, prospects for bladder cancer burden in China are currently grim and will remain so during the next few years due to population aging, poor air quality, problematic food safety, and massive tobacco consumption.Citation19 Smokers have about 50% increase in the incidence of bladder cancer mortality compared with nonsmokers.Citation20 Therefore, tobacco control, environmental protection, early screening of bladder cancer and the potential impact of lifestyle, diet, inflammation status, or surgical treatment, such as transurethral resection, should be considered to control the mortality of bladder cancer.Citation21,Citation22
The age effect on bladder cancer mortality showed an uptrend in all populations, especially in males. The risk of mortality increased with age, which is analogous to the study of Olfert et al.Citation4 The lengthy latent period may explicate the finding. There is often an interval of several decades between the first exposure to a carcinogen and the clinical appearance of the disease for most human cancers.Citation23 Hence, many cases of bladder cancers are diagnosed and reported in the elderly. Furthermore, that the elderly may experience greater exposure to tobacco smoking and occupational risk factors is another interpretation for this finding. However, population aging in China has been rising owing to a sharp decline in fertility and prolongation of life expectancy. The percentage of people aged ≥65 years increased from 4.91% in 1982Citation24 to 10.47% in 2015,Citation25 so we inferred bladder cancer burden in China will likely increase in the next few years.
Period effects usually indicate the impact of factors with immediate effects on cancer mortality and incidence, such as new diagnoses, improved medical interventions, or a change in ascertaining or coding the cause of mortality. The impact of the period for both males and females is not found in this study. One possible reason is that the study period (1991–2015) was relatively short, just as in the Argentinian study.Citation6 An alternative reason may be that the effect of period on cancer mortality was small because of the highly developed of clinical treatment and screening program.Citation26,Citation27
The effects of the cohort showed a downward trend as a whole. This finding might be explained by the improved nutrition, living conditions, and health care services, which could reduce the risk factor exposure in younger cohorts. It has been confirmed that the status of medical insurance is closely related to chronic disease mortality, ignoring the impact of lifestyle.Citation28 In China, three important medical security systems have been established since the 1990s, and the “Decision of the State Council on Setting up a Basic Medical Insurance System for Staff Members and Workers in Cities and Towns” was enacted in 1998. Furthermore, compared to the elderly cohorts, the younger cohorts had better nutrition and living conditions. The kindred trends were also found in other cancers’ mortality rates, eg, breast cancer, lung cancer, and cervical cancer.Citation26,Citation29,Citation30 This phenomenon might highlight that the Chinese population has greatly benefited from improved nutrition, living conditions, and health care services due to rapid economic development and that this weakened the cohort effects.Citation31
In this study, the APC model combined with the IE algorithm was used to solve the nonidentification problem of collinearity among age, period, and cohort, which produced a more reliable result. However, only 25 years of bladder cancer mortality rates were employed in this study because the disease surveillance system was perfected electronically in 1990s, which may affect the impact of the period on bladder cancer mortality rates. In particular, 2001 data was unavailable and an estimated value was input. Whether different imputation methods had an influence on the results is unclear.
Conclusion
This study clearly and simultaneously estimates the effects of age, period, and cohort on bladder cancer mortality. The findings indicated age and cohort effects exited in China population, which suggested that preventive measures should be taken corresponding to the changes in age-and cohort-related factors in the population.
Disclosure
The authors report no conflicts of interest in this work.
References
- FerlayJSoerjomataramIDikshitRCancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012Int J Cancer20151365E359E38625220842
- AntoniSFerlayJSoerjomataramIZnaorAJemalABrayFBladder cancer incidence and mortality: a global overview and recent trendsEur Urol20177119610827370177
- BourneleDBeisDZebrafish models of cardiovascular diseaseHeart Fail Rev201621680381327503203
- OlfertSMFelknorSADelclosGLAn updated review of the literature: risk factors for bladder cancer with focus on occupational exposuresSouth Med J200699111256126317195421
- BaoPPZhengYWuCXCancer incidence in urban Shanghai, 1973–2010: an updated trend and age-period-cohort effectsBMC Cancer201616128427102013
- PouSAOsellaARDiaz MdelPBladder cancer mortality trends and patterns in Córdoba, Argentina (1986–2006)Cancer Causes Control201122340741521184264
- YangGKongLZhaoWEmergence of chronic non-communicable diseases in ChinaLancet200837296501697170518930526
- ChenWZhengRBaadePDCancer statistics in China, 2015CA Cancer J Clin201666211513226808342
- PangCGuanYLiHChenWZhuGUrologic cancer in ChinaJpn J Clin Oncol201646649750127049022
- GuoPHuangZLYuPLiKTrends in cancer mortality in China: an updateAnn Oncol201223102755276222492700
- HanSJZhangSWChenWQLiCLAnalysis of the status quo and trends: mortality in patients with bladder cancer in ChinaJ Mod Urol201318228232
- WenDGShanBEZhangSWAnalysis of incidence and mortality rates of bladder cancer in registration areas of China from 2003 to 2007Tumor2012324256262
- GuoPLiKTrends in esophageal cancer mortality in China during 1987–2009: age, period and birth cohort analyzesCancer Epidemiol20123629910522226590
- LiMWanXWangYSunYYangGWangLTime trends of esophageal and gastric cancer mortality in China, 1991–2009: an age-period-cohort analysisSci Rep201771679728754910
- YangYSchulhofer-WohlSFuWJLandKCThe intrinsic estimator for Age-Period-Cohort analysis: what it is and how to use itAm J Sociol2008113616971736
- ClaytonDSchifflersEModels for temporal variation in cancer rates. I: Age-period and age-cohort modelsStat Med1987644494673629047
- ClaytonDSchifflersEModels for temporal variation in cancer rates. II: Age-period-cohort modelsStat Med1987644694813629048
- ShariatSFSfakianosJPDrollerMJKarakiewiczPIMerynSBochnerBHThe effect of age and gender on bladder cancer: a critical review of the literatureBJU Int2010105330030819912200
- ChungRYSchoolingCMCowlingBJLeungGMHow does socioeconomic development affect risk of mortality? An age-period-cohort analysis from a recently transitioned population in ChinaAm J Epide-miol20101713345356
- LiuWZhaoXZhongZThe role of tobacco smoke in bladder and kidney carcinogenesis: a comparison of exposures and meta-analysis of incidence and mortality risksEur Urol2016704e104e10526343004
- FerroMDi LorenzoGBuonerbaCPredictors of residual T1 high grade on re-transurethral resection in a large multi-institutional cohort of patients with primary T1 High-Grade/Grade 3 bladder cancerJ Cancer20189224250425430519326
- MatteoFDorinMVFrancescoCHigh-grade T1 on re-trans-urethral resection after initial high-grade T1 confers worse oncological outcomes: results of a multi-Institutional StudyUrol Int2018101171529975950
- LeviFLa VecchiaCAge, cohort and period effects on large bowel cancer incidenceEur J Cancer Prev200211651551712457101
- ZhuJChenJGZhangYHChenYSDingLLTrend on mortality changes for lung cancer during 1972–2011 in Qidong, JiangsuZhonghua Liu Xing Bing Xue Za Zhi2012339933936 Chinese23290806
- WangYWChenHHWuMSChiuHMTaiwanese Nationwide Colorectal Cancer Screening ProgramCurrent status and future challenge of population-based organized colorectal cancer screening: lesson from the first decade of Taiwanese programJ Formos Med Assoc2018117535836428988890
- WangJBaiZWangZYuCComparison of secular trends in cervical cancer mortality in China and the United States: an age-period-cohort analysisInt J Environ Res Public Health201613111148
- VartolomeiMDFerroMCantielloFValidation of neutrophil-to-lymphocyte ratio in a multi-institutional cohort of patients with T1G3 non-muscle-invasive bladder cancerClin Genitourin Cancer201816644545230077463
- BittoniMAWexlerRSpeesCKClintonSKTaylorCALack of private health insurance is associated with higher mortality from cancer and other chronic diseases, poor diet quality, and inflammatory biomarkers in the United StatesPrev Med20158142042626453984
- LiCYuCWangPAn age-period-cohort analysis of female breast cancer mortality from 1990–2009 in ChinaInt J Equity Health20151417626369689
- WangLYuCLiuYLung cancer mortality trends in China from 1988 to 2013: new challenges and opportunities for the governmentInt J Environ Res Public Health201613111052
- FerroMVartolomeiMDRussoGIAn increased body mass index is associated with a worse prognosis in patients administered BCG immunotherapy for T1 bladder cancerWorld J Urol20183849945