
Abstract
Aims
The study aims to explore the incidence, risk factors, and prognosis in patients with primary hepatocellular carcinoma (HCC) and synchronous lung metastasis using a large-scale population-based cancer registry database.
Patients and methods
Data of 33,177 HCC patients were retrieved from the Surveillance, Epidemiology, and End Results (SEER) database from 2010 to 2015. Multivariate logistic and Cox regression model analysis were applied for the recognition of risk factors and prognostic factors associated with lung metastasis among HCC patients. The overall survival and cancer-specific survival of HCC patients with initial pulmonary metastasis were estimated by Kaplan– Meier analysis, and the survival curves were compared by log-rank tests.
Results
Total 2,084 (6.28%) HCC patients diagnosed with initial pulmonary metastasis were enrolled for analysis. Male gender, younger age, non-white race, unmarried status, uninsured status, elevated alpha-fetoprotein, larger primary liver tumor size, positive lymph node status, synchronal bone or brain metastasis, and tumor poor pathological differentiation were relevant to higher risk of lung metastasis in HCC cohort. The 1-, 3-, 5-year overall survival and cancer-specific survival rates for HCC lung metastasis patients were 12.8% vs 15.3%, 4.0% vs 5.7%, and 1.6% versus 2.4%, respectively. The median overall and cancer-specific survival time in HCC lung metastasis group were both 3 months, while the corresponding time in HCC lung metastasis-free group were 19 and 25 months (P<0.05). Older age, unmarried status, poor tumor differential grade, and absence of surgery were identified as unfavorable prognosis factors.
Conclusion
The survival of patients with HCC lung metastasis was dismal. Several clinicopathological factors were found to be significantly relevant to the development and prognosis of HCC lung metastasis. These new findings could be useful for a precise and individualized therapeutic schedule.
Introduction
Hepatocellular carcinoma (HCC) is the most frequent subtype of primary liver cancer with high lethality.Citation1 Recent statistical data demonstrated that the 5-year survival rate of HCC is still below 20%.Citation2,Citation3 One of reasons responsible for high mortality is the extrahepatic spread of primary tumor loci with partly elucidated mechanism.Citation4,Citation5 Till now, lung is considered as the most favored organ for HCC metastatic colonization, counting for 51% of all extrahepatic metastasis.Citation6 Result from a large-scale population study showed that the 1-year overall survival (OS) and cancer-specific survival (CSS) was 10% and 12.6% in patients diagnosed with HCC lung metastasis (HCCLM).Citation7
Previously, HCC initiated with lung metastasis was regarded as the late stage of disease with poor survival.Citation1 With the conceptual update in treatment modalities, new attempts, such as simultaneous hepatectomy and pulmonary metastasectomy, have been made by surgeons in selected individuals to achieve a better survival.Citation8–Citation10 In addition, Yang et al elucidated that patients receiving combined treatment had a better survival by analyzing 76 consecutive HCC patients initially presenting with lung metastasis.Citation11 However, primary and secondary prevention strategies also played a pivotal role in cancer remedy. Early recognition of patients with high risk for development of HCCLM and subsequent surveillance should be proposed. A previous article illustrated that HCC <7 cm in diameter had higher risk of forming lung metastasis after primary liver cancer resection.Citation12 Due to a low prevalence of HCCLM, a large-scale population-based study is needed for systematic identification of the morbidity, potential risk factors, and clinical prognosis of initial HCCLM patients.
In the present research, we retrospectively reviewed data from the Surveillance, Epidemiology, and End Results (SEER) database to explore the actual incidence and identify factors contributing to initially diagnosed HCCLM. Furthermore, stratified survival estimates and variables affecting either OS or CSS recognition were also conducted.
Patients and methods
Data source and patient enrollment
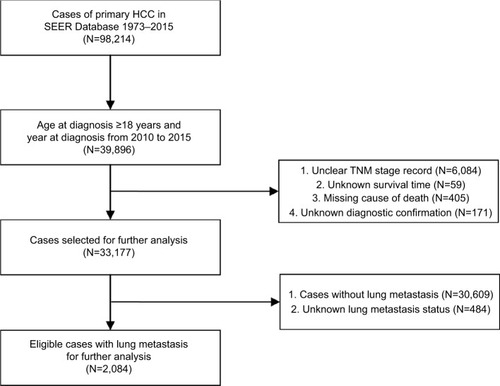
Original data were retrieved from the SEER database maintained by the National Cancer Institute. The SEER program consists of 18 population-based cancer registries, covering ~28% of all population in the USA. The distant metastasis status were collected until 2010 due to the intrinsic reason of the database and the latest revision was released on April 16, 2018. The inclusion criteria were as follows: 1) primary site labeled as “C22.0 Liver” and ICD-O-3 histology/behavior marked with “8,170/3: hepatocellular carcinoma, not otherwise specified,” “8,171/3: hepatocellular carcinoma, fibrolamellar,” “8,172/3: hepatocellular carcinoma, scirrhous,” “8,173/3: hepatocellular carcinoma, spindle cell variant,” “8,174/3: hepatocellular carcinoma, clear cell type,” or “8,175/3: hepatocellular carcinoma, pleomorphic type”; 2) the year at diagnosis from 2010 to 2015; and 3) the age at diagnosis older than 18 years. Individuals who had unclear TNM stage record, unknown survival time, missing cause of death, or unknown diagnostic confirmation were subsequently excluded. For further analysis, cases were grouped by the existence of lung metastasis ().
Figure 1 Flowchart of the enrolled patients in the study according to inclusion and exclusion criterion.
Abbreviations: HCC, hepatocellular carcinoma; SEER, Surveillance, Epidemiology, and End Results.
We obtained the SEER data access permission before the project initiation. The study complied with the Declaration of Helsinki and followed the ethical principles of Huashan Hospital, Fudan University.
Variables definition and stratification
The definition of incidence was the proportion of patients with lung metastasis in the entire HCC patients. We stratified total cohort by age at diagnosis, gender, race, marital status at diagnosis, insurance status, alpha-fetoprotein (AFP) interpretation, maximum of tumor size, 7th AJCC TNM staging, lymph node status, surgery, pathological grade, and other distant site metastasis (brain and bone). Liver metastasis and pathological subtypes were not included for analysis because the records were unable to be distinguished clearly. The variable race comprised of white, black, and others (American Indian/Alaska Native, Asian/Pacific Islander). AFP level was interpreted as elevated, normal, borderline, as well as unknown. Surgery for primary site was classified as no surgery, local tumor destruction, surgery, and unknown. OS was defined as the duration between the surgery and death or the last follow-up, while the CSS was the period between the surgery and the death due to cancer.
Statistical analyses
Data were downloaded by SEER*Stat Software version 8.3.5 (National Cancer Institute, Bethesda, MD, USA). SPSS version 13.0 (IBM Inc., Chicago, IL, USA) was used for statistical analysis, and survival curves were generated using GraphPad Prism version 6.0 (GraphPad-Prism Software Inc., San Diego, CA, USA). Continuous variables were presented as mean±SD or median (minimum, maximum), and the categorical variables were shown as number (percent). Association between categorical data was analyzed using the chi-squared test or Fisher’s exact test, while continuous values using Student’s t-test or Mann–Whitney test, when appropriate. The Kaplan– Meier method and Cox regression analysis were applied to determine prognostic factors associated with OS or CSS. Two tailed P<0.05 was regarded as statistically significant.
Results
Incidence of HCCLM
Among finally enrolled 33,177 patients with HCC from 2010 to 2015, 2,084 patients were initially diagnosed with HCCLM with an incidence rate 6.28% (). No statistical significance could be found between different years. Only 44 (2.1%) individuals with HCCLM received surgery (including local tumor destruction), while remaining 97.8% patients treated conservatively ().
Table 1 Baseline clinical demographics and multivariable logistic regression for analyzing risk factor for initial lung metastasis of primary hepatocellular carcinoma patients in SEER database (2010–2015)
Risk factors for HCCLM
As depicted in , male gender (OR: 1.131, 95% CI: 1.014–1.260, P=0.026), non-white race, unmarried status (OR: 1.313, 95% CI: 1.186–1.454, P<0.001), uninsured status (OR: 1.988, 95% CI: 1.661–2.380, P<0.001), maximum primary liver tumor size over 50 mL (mm), positive lymph node status (OR: 4.326, 95% CI: 3.838–4.875, P<0.001), synchronal bone (OR: 5.495, 95% CI: 4.827–6.255, P<0.001) or brain metastasis (OR: 11.492, 95% CI: 7.892–16.734, P<0.001), and tumor poor pathological differentiation were relevant to higher risk of initial HCCLM. Additionally, patients with HCC older than 40 years or normal AFP level had lower risk of developing lung metastasis ().
Survival and prognostic factors of HCCLM patients
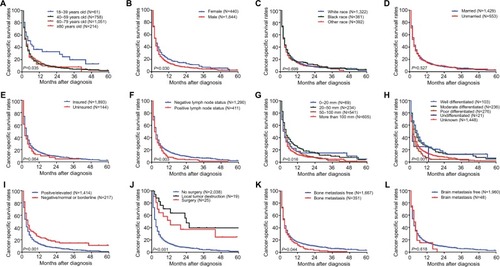
Median OS in HCC lung metastasis-free (HCCLMF) group and HCCLM group were 19 months and 3 months, while the median CSS in the group of HCCLMF and HCCLM were 25 months and 3 months. The 1-, 3-, and 5-year OS rates for HCC patients without or with lung metastasis were 59.8% vs 12.8%, 33.4% vs 4.0%, and 24.1% versus 1.6%, respectively (). In addition, the homologous proportions of CSS were 65.2% vs 15.3%, 41.1% vs 5.7%, and 32.4% versus 2.4% (). Further, log-rank analysis revealed that age at diagnosis, gender, lymph node status, maximum primary tumor size, tumor differentiation, AFP level interpretation, and surgical intervention had impact on HCCLM cohort patients’ OS with statistical significance (P<0.05, ). Besides factors above, bone metastasis was also associated with CSS in HCCLM cohort (P<0.05, ).
Figure 2 Kaplan–Meier analysis of (A) overall survival and (B) cancer-specific survival in hepatocellular carcinoma patients with or without initial lung metastasis.
Abbreviations: LM, lung metastasis; LMF, lung metastasis free.
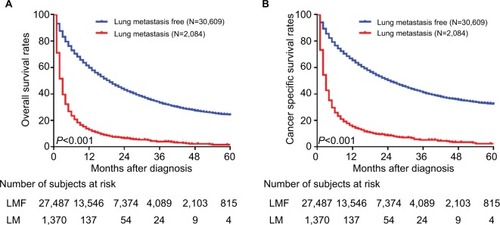
Figure 3 Kaplan–Meier analysis of overall survival in hepatocellular carcinoma patients with initial lung metastasis stratified by (A) age at diagnosis, (B) gender, (C) race, (D) marital status at diagnosis, (E) insurance status at diagnosis, (F) lymph node status, (G) maximum primary tumor size, (H) primary tumor differential grade, (I) alpha-fetoprotein level, (J) surgery for primary tumor, (K) bone metastasis, and (L) brain metastasis.
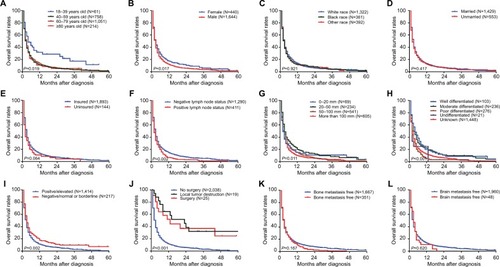
Figure 4 Kaplan–Meier analysis of cancer-specific survival in hepatocellular carcinoma patients with initial lung metastasis stratified by (A) age at diagnosis, (B) gender, (C) race, (D) marital status at diagnosis, (E) insurance status at diagnosis, (F) lymph node status, (G) maximum primary tumor size, (H) primary tumor differential grade, (I) alpha-fetoprotein level, (J) surgery for primary tumor, (K) bone metastasis, and (L) brain metastasis.
Using the univariate and multivariate Cox regression model, age at diagnosis older than 40 years, unmarried status (HR: 1.134, 95% CI: 1.019–1.261, P=0.021), poor differentiation (HR: 1.732, 95% CI: 1.355–2.213, P<0.001) or undifferentiation (HR: 1.732, 95% CI: 1.355–2.213, P<0.001), and surgical intervention (including local tumor destruction and surgery) were identified as worse prognosis factors for OS (). Similarly, these factors were also associated with a higher risk of mortality caused by cancer ().
Table 2 Univariate and multivariate analysis of overall survival in patients with primary hepatocellular carcinoma lung metastasis in SEER database (2010–2015)
Table 3 Univariate and multivariate analysis of cancer-specific survival in patients with primary hepatocellular carcinoma lung metastasis in SEER database (2010–2015)
Discussion
HCCLM is a Gordian knot for clinicians because of its poor survival and limited effective treatment modalities. Previous articles mainly focused on the lung metastasis followed by primary liver tumor resection, while little is known about the simultaneous HCC and lung metastatic tumor. In the current study, the epidemiological result indicated that 6.28% patients with HCC presented with synchronous lung metastasis. Similarly, result from a Chinese cohort revealed that 39 of 862 (4.5%) HCC patients presented with initial lung metastasis.Citation13 However, a national follow-up survey of primary liver cancer in Japan showed that more than two-fifths of HCC patients developed pulmonary metastatic tumor.Citation14 The difference between our result and results from Japan study may be due to the discrepancy of enrolled patients. Our study only focused on the initial HCCLM cases, while Japan group analyzed all pulmonary metastatic cases during HCC progression. But, our result could be underestimated on account of the fact that asymptomatic HCCLM patients are unable to be detected. Strikingly, application of newly effective treatment modalities by clinicians may contribute to a slight increase in OS and CSS compared with data 3 years ago.Citation7
Follow-up analysis identified several risk factors of HCCLM, including younger patient (<40 years), non-white race, unmarried or uninsured status, elevated AFP level, larger primary tumor size, positive lymph node status, synchronal bone or brain metastasis, tumor poor pathological differentiation, and absence of surgery. This result suggested that clinicians should consider the possibility of lung metastasis when visiting HCC patients with above characteristics. Therefore, routine chest radiograph or low-dose computed tomography of lung was considered for these patients. Regrettably, other reported risk factors, such as microvascular invasion and tumor encapsulation, could not be assessed owing to no record in SEER.
Survival estimates elucidated that age below 40 years, female, negative lymph node status, smaller tumor size, better tumor differentiation, normal AFP level, and surgery received may contribute to an optimistic survival. Prognostic factors for HCCLM were further investigated. The HCC patients with characteristics of age at diagnosis older than 40 years, unmarried status, tumor poor differentiation, and existence of surgery had a significantly higher risk of mortality. According to these recognized factors, clinicians could approximately assess the survival and prognosis of HCCLM patients.
Collectively, age at diagnosis, surgery for primary tumor, and tumor differential grade were crucial factors for both risk and prognosis prediction. Although HCC patients younger than 40 years had higher risk for lung metastasis, their OS and CSS appeared the best performance. The underlying causes perhaps were younger patients usually held more positive attitude toward treatment and had better physical status to tolerant various treatment modalities. In addition, the majority of patients did not receive surgery in this study, which most likely led to a lower survival rate compared with the reported data.Citation11 Consistent with previous reports, larger tumor size and positive AFP level predicted high risk for lung tumor colony formation.Citation4,Citation12 Notably, concomitant brain or bone metastasis had no impact on OS among HCCLM patients.
Limitations
First, only patients diagnosed after 2010 are enrolled for analysis because metastatic sites had been recorded until 2010. Second, inevitable bias exists because of absent details of tumor pathology and patient performance status. Third, SEER database represents merely US population, and other countries with high incidence of HCC were unable to be enrolled for global analysis. Last, the research is retrospective and the result still needs prospective trials to confirm a precise conclusion.
Conclusion
Generally, the incidence of initial pulmonary metastasis in HCC patients is 6.28% and the 5-year OS is still poor. Some clinicopathological features, such as age at diagnosis, tumor differential grade, and surgery for primary tumor, are highly predictive of HCCLM and significantly affect patients’ survival. To our knowledge, the study is the first attempt to explore the epidemiological characteristics and identify the associated risk or prognostic factors of HCCLM using a population-based cancer registry database. The conclusion could be useful for a precise and individualized therapeutic schedule.
Acknowledgments
This work was kindly sponsored by the Natural Science Foundation of China (81773089, 81802903) and China National Key Projects for Infectious Disease (2017ZX10203207). The authors also acknowledge the contribution of the SEER program in the establishment and maintenance of the database.
Disclosure
The authors report no conflicts of interests in this work.
References
- FornerAReigMBruixJHepatocellular carcinomaLancet2018391101271301131429307467
- SiegelRLMillerKDJemalACancer statistics, 2018CA Cancer J Clin201868173029313949
- El-SeragHBHepatocellular carcinomaN Engl J Med2011365121118112721992124
- YokooTPatelADLev-CohainNSingalAGYoppACPedrosaIExtrahepatic metastasis risk of hepatocellular carcinoma based on α-fetoprotein and tumor staging parameters at cross-sectional imagingCancer Manag Res2017950351129081671
- LiGCYeQHDongQZRenNJiaHLQinLXTGF beta1 and related-Smads contribute to pulmonary metastasis of hepatocellular carcinoma in mice modelJ Exp Clin Cancer Res2012319323151305
- KatyalSOliverJHPetersonMSFerrisJVCarrBSBaronRLExtrahepatic metastases of hepatocellular carcinomaRadiology2000216369870310966697
- WuWHeXAndayaniDPattern of distant extrahepatic metastases in primary liver cancer: a SEER based studyJ Cancer20178122312231828819435
- KuoTMChangKMChengTIKaoKJClinical factors predicting better survival outcome for pulmonary metastasectomy of hepatocellular carcinomaLiver Cancer20176429730629234633
- HuZLiWHuangPTherapeutic significance and indications of pulmonary metastasectomy for hepatocellular carcinoma following liver resectionInt J Surg201748233128987561
- TakahashiYIkedaNNakajimaJPrognostic analysis of surgical resection for pulmonary metastasis from hepatocellular carcinomaWorld J Surg20164092178218527255943
- YangTLuJHLinCConcomitant lung metastasis in patients with advanced hepatocellular carcinomaWorld J Gastroenterol201218202533253922654451
- IshiiTHatanoEYasuchikaKTauraKSeoSUemotoSHigh risk of lung metastasis after resection of hepatocellular carcinoma more than 7 cm in diameterSurg Today201444101900190524264061
- ZengYZhangXLiuJZhongYWangXCorrelated factors of pulmonary metastasis of hepatocellular carcinomaChin J Dig Surg2013129668671
- IkaiIItaiYOkitaKReport of the 15th follow-up survey of primary liver cancerHepatol Res2004281212914734147