
Abstract
Introduction:
The prognostic significance of the systemic immune-inflammation index (SII) in breast cancer is unknown. Here, we aimed to explore the connection between pretreatment SII and the survival of patients with triple-negative breast cancer (TNBC).
Methods:
We enrolled 160 TNBC patients treated in our hospital between May 2000 and June 2012. We employed the Kaplan-Meier curve and log-rank test to assess overall survival (OS), disease-free survival (DFS), and distant metastasis-free survival (DMFS). We identified the prognostic significance of SII using the Cox regression model.
Results:
The Kaplan-Meier curve revealed the median OS as 44.2 and 82.4 months in high and low SII TNBC patients, respectively (P<0.001). According to univariate and multivariate analyses, increased SII correlated with poor OS (HR =2.91, 95% CI: 2.00–4.23, P<0.001; HR =2.60, 95% CI: 1.74–3.88, P<0.001). The DFS and DMFS of patients with high SII were 18.8 and 23.8 months, respectively, while those of patients with low SII were 29 and 45.2 months, respectively, (P<0.001). Further univariate analyses showed a significant correlation between SII and DFS and DMFS (P<0.01), while results from multivariate analyses suggested that SII is an independent prognostic factor for DFS (P=0.045), but not for DMFS (P=0.078). The area under the receiver operating characteristics curves for SII to differentiate between long and short OS, DFS, and DMFS were 0.69, 0.60, and 0.64, respectively.
Conclusion:
Our findings may point to SII having an independent prognostic significance in TNBC patients. Prospective in-depth studies, using a larger sample size, are required to further investigate the precise role of SII in TNBC before clinical use.
Introduction
Triple-negative breast cancer (TNBC) is a heterogeneous disease characterized by the negative expression of the human epidermal growth factor receptor 2 (HER2), progesterone receptor, and estrogen receptor.Citation1,Citation2 TNBC usually correlates with pushing margins of invasion, high histological grade, high levels of proliferation, young age, high recurrence and metastases rates, advanced disease,Citation3 and poor clinical outcomes.Citation4,Citation5 So, predicting the prognosis of TNBC patients is particularly vital.
In recent years, liquid biopsy techniques have been widely employed to investigate the diagnostic and prognostic markers for breast cancer and other tumors. For example, circulating tumor cells have an unfavorable prognostic value in breast cancer patients.Citation6,Citation7 Besides, exosomes have been shown to have diagnostic and prognostic values in various tumors.Citation8–Citation10 Gene expression signatures, such as MAD2L1 and BUB1, have prognostic significance in breast cancer patients.Citation11–Citation14 However, the above methods may be limited in clinical use because of the high cost and complexity of measurements. Thus, we would like to focus on the inflammation index, an easily obtained and cheap index, to predict the survival of breast cancer patients.
Cancer-related inflammation has been found to play a significant part in the development and prognosis of cancer.Citation15–Citation17 Some biochemical or hematological markers, such as increase in platelet, lymphocyte, neutrophil, white cell counts, C-reactive protein levels, and hypoalbuminemia, could trigger a systemic inflammatory response.Citation18–Citation21 A combination of these factors has been used to obtain prognostic scores for inflammation, for example, lymphocyte ratio (PLR) for platelet, lymphocyte ratio (NLR) for neutrophil, and the Glasgow Prognostic Score. The adverse role of elevated NLR and PLR has already been studied intensely in various cancers, including non-small cell lung cancer, cervical cancer, gallbladder cancer, ovarian cancer, colorectal cancer, breast cancer, and gastric cancer.Citation19,Citation22–Citation30
The systemic immune-inflammation index (SII) is determined by platelet × neutrophil/lymphocyte, which could be better poised to mirror the sense of balance of the host inflammatory and immune status.Citation31 Though SII has been used before in investigating different cancers, including colorectal cancer, nasopharyngeal cancer, gastric cancer, pancreatic cancer, hepatocellular cancer, and prostate cancer,Citation31–Citation38 it has yet to be applied comprehensively in studies involving breast cancer. Our research evaluated the clinical significance of SII, an easily obtained and cheap index, in TNBC patients.
Materials and methods
Patient selection and data collection
This study is a retrospective investigation sanctioned by the Ethics Committee of China-Japan Union Hospital. All data were anonymous. Written informed consent was obtained from all patients. 160 TNBC patients undergoing treatment at our hospital between May 2000 and June 2012 were enrolled for the test. Patients enrolled had their TNBC histologically confirmation and received surgery accompanied by adjuvant chemotherapy or neoadjuvant chemotherapy. Exclusion criteria: patients suffering from an infectious disease 3 months before enrollment; patients with coronary artery disease, immune disease, inflammatory disease, and hematological diseases; with metastatic or inflammatory breast cancer; or using immunosuppressive or anti-inflammatory drugs (including steroids, rapamycin, anti-lymphocyte, and globulin) before enrollment. 32 patients were excluded based on the above criteria.
Patients received regular follow-up every 3 months following adjuvant treatment until they died or lost follow-up. Follow-up included assessing disease progression, confirming patient death, and lost follow-up. The status of the disease was evaluated using ultrasound imaging, computed tomography (CT), magnetic resonance imaging (MRI), and positron emission computed tomography. September 2018 was set as the deadline for follow-up. Disease-free survival (DFS) time referred to the period from surgical resection to the first disease recurrence, metastasis, lost follow-up, or death. Overall survival (OS) represented the stretch from surgery up till death or lost follow-up. Distant metastasis-free survival (DMFS) covered the spell from surgical resection to the first distant metastasis, lost follow-up, or death.
All patients were exposed to the following treatments: adjuvant and neoadjuvant chemotherapy, breast-conserving surgery and a radical mastectomy, and adjuvant radiotherapy with 50–60 Gy. A 3+ score or a fluorescence in situ hybridization for 1+ and 2+ patients confirmed a positive HER2 status, while an immunohistochemical score of 0 represented a negative status. Progesterone and estrogen receptors were negative and were determined by the immunohistochemistry test to be 1% of the positive invasive tumor nuclei. Data for age, pathology, tumor size, lymph node metastasis, tumor stage [according to the 7th American Joint Committee on Cancer (AJCC) stage],Citation39 lymphovascular invasions, histological grade, and anti-tumor treatment were collected. Data for differential blood counts were collected within the 7 days preceding surgery or neoadjuvant chemotherapy. The counts of platelets, neutrophils, and lymphocytes were extracted from our hospital’s online records. Chemotherapy regimens included paclitaxel + anthracyclines + cyclophosphamide and anthracyclines + paclitaxel.
Statistical analysis
The SPSS 21.0 software (SPSS, Chicago, IL, USA) was used to perform data analysis. SII was determined by platelet × neutrophil/lymphocyte. The median value of SII (557) was used to distinguish between high and low SII. DFS, DMFS, and OS were obtained with the help of the Kaplan-Meier method. The log-rank test was used to compare the differences in DFS, DMFS, and OS between patients from the two groups. Receiver operating characteristics (ROC) curves were employed to evaluate the ability of SII to differentiate between good and reduced survival. Multivariate analyses to identify independent prognostic factors in TNBC patients was carried out using the Cox regression model. Statistical significance was established at P<0.05 for differential results.
Results
Characteristics that are representative of the 160 TNBC patients are displayed in . Results show that the median follow-up time was 61.7 months (5.9–159.0 months). Among the 160 TNBC patients, 143 and 140 of them experienced tumor recurrence and distant metastases, respectively, and 119 of them died. Two patients lost follow-up in DFS, and 1 patient lost it in OS. One-half of the patients (80) had a low SII (≦557), and the other half (80) had a high SII (>557). According to the 7th AJCC, 26 (16.3%), 85 (53.1%), and 49 (30.6%) patients were in stages I, II, and III, respectively. 31 (19.4%) patients underwent breast-conserving surgery, while 129 (80.6%) patients received a radical mastectomy. 39 (24.4%) patients were diagnosed with lobular cancer, while 121 (75.6%) patients had ductal cancer. 12 (7.5%), 93 (58.1%), and 53 (33.1%) TNBC patients suffered from histopathological grades I, II, and III, respectively.
Table 1 Clinicopathologic parameters of 160 TNBC patients
The Kaplan-Meier curve revealed the median OS in TNBC patients with high and low SII to be 44.2 and 82.4 months, respectively, (P<0.001, ). The area under the curve (AUC) of ROC for SII to differentiate between long and short OS was 0.69 (). Results from univariate analyses showed increased SII correlating with poor OS (HR =2.91, 95% CI: 2.00–4.23, P<0.001; ). Furthermore, the T stage, Ki-67, tumor differentiation, surgery type, and N stage correlated with the OS of TNBC patients (P<0.01; ). According to multivariate analyses, elevated SII correlated independently with poor OS (HR =2.60, 95% CI: 1.74–3.88, P<0.001; ).
Table 2 Association between clinicopathologic parameters/SII and OS in TNBC
Figure 1 Kaplan-Meier and ROC curves for 160 TNBC patients. (A) OS as derived by the SII. (B) AUC of SII to differentiate between long and short OS. (C) DFS as derived by the SII. (D) AUC of SII to differentiate between long and short DFS. (E) DMFS as derived by the SII. (F) AUC of SII to differentiate between long and short DMFS.
Abbreviations: ROC, receiver operating characteristic curve; TNBC, triple-negative breast cancer; OS, overall survival; SII, systemic immune-inflammation index; AUC, area under the curve; DFS, disease-free survival; DMFS, distant metastasis-free survival.
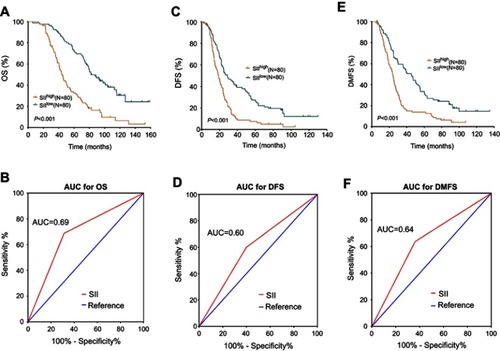
Median DFS in TNBC patients displayed high and low SII to be 18.8 and 29 months, respectively (P<0.001, ). The AUC of ROC for SII to differentiate between long and short DFS was 0.60 (). Univariate analyses showed increased SII correlating with poor DFS (HR =1.88, 95% CI: 1.34–2.65, P<0.001; ). Besides, age, Ki-67, tumor differentiation, N stage, and T stage correlated significantly with poor DFS of TNBC patients (P<0.05; ). According to multivariate analyses, elevated SII correlated independently with poor DFS (HR =1.46, 95% CI: 1.01–2.12, P=0.045; ).
Table 3 Association between clinicopathologic parameters/SII and DFS in TNBC
The median DMFS was 23.8 and 45.2 months in high and low SII TNBC patients, respectively (P<0.001, ). The AUC of ROC for SII to distinguish between long and short DFS was 0.64 (). Univariate analyses showed increased SII correlating with poor DMFS (HR =1.81, 95% CI: 1.28–2.55, P=0.001; ). Moreover, age, Ki-67, T stage, tumor differentiation, and N stage correlated with DMFS of TNBC patients (P<0.05; ). According to multivariate analysis, elevated SII did not correlate independently with poor DMFS (HR =1.40, 95% CI: 0.96–2.03, P=0.078; ).
Table 4 Association between clinicopathologic parameters/SII and DMFS in TNBC
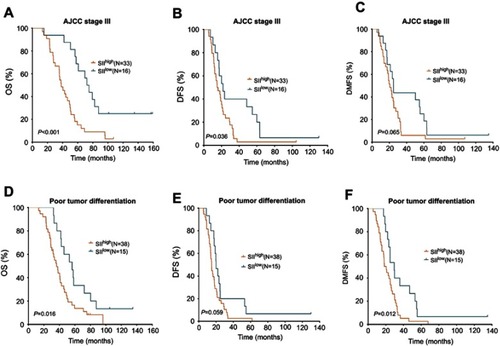
For patients with AJCC stage III, increased SII predicted poorer OS and DFS than decreased SII (P<0.001, =0.036, ) but not DMFS (P=0.065, ). For patients with poor tumor differentiation, elevated SII indicated poor OS and DMFS (P=0.016, =0.012, and ) but not DFS (P=0.059, ).
Figure 2 Kaplan-Meier curves for patients with AJCC stage III and poor tumor differentiation. In patients with AJCC stage III, OS (A), DFS (B), and DMFS (C) as derived by the SII. In patients with poor tumor differentiation, OS (D), DFS (E), and DMFS (F) as derived by the SII.
Abbreviations: AJCC, American Joint Committee on Cancer; OS, overall survival; DFS, disease-free survival; DMFS, distant metastasis-free survival.
Discussion
Our study represents the first study aimed at assessing the clinical significance of SII in TNBC patients. As reported above, increased SII correlated with poor DFS, DMFS, and OS in TNBC patients and its prognostic role carried on into the multivariate analysis, which was consistent with previous findings from investigations of other tumors. According to Huang et al,Citation40 high SII was associated with poor outcomes in the evaluation of the prognostic value of preoperative SII in gastric cancer patients. To date, SII’s role in prognosis has been investigated in different tumors.Citation31–Citation35,Citation37,Citation38,Citation40–Citation42 Hu et alCitation31 were the first researchers to propose SII as having a novel, independent prognostic role in Chinese hepatocellular cancer patients. Patients with elevated SII had higher recurrence and reduced survival rates than patients with decreased SII. Hu et al’s finding has received backing from numerous other investigations. Tong et alCitation38 demonstrated the correlation between SII and tumor response post-treatment and survival in non-small cell lung cancer patients, proving its independent prognostic role. Jiang et alCitation37 showed that elevated SII predicts poor survival for nasopharyngeal cancer patients independently. Our results, in concomitance with all these reports, point to SII having a role to play in major cancer types, including breast cancer.
Accumulating studies have substantiated the association between cancer and the inflammatory system. Counts of the peripheral inflammatory cells, such as monocytes, lymphocytes, and neutrophils, before treatment, have validated the significant link between prognosis and the inflammatory system in different types of cancers.Citation21,Citation28,Citation43–Citation50 As an integrated parameter, the prognostic value of SII in cancers may be explained by the function of platelets, neutrophils, and lymphocytes. Platelets promote tumor angiogenesis and metastases and shield tumor cells from the antitumor immune response.Citation51 Neutrophils are inflammatory and immune parameters that play a part in the proliferation and metastasis of tumors by releasing such inflammatory mediators as neutrophil elastase, interleukin-8, and matrix metalloproteinase-9.Citation52 Contrary to platelets and neutrophils, lymphocytes infiltrate tumors and are associated with better survival in cancer patients, since their immune response can prevent tumor growth and metastasis.Citation53,Citation54
Although our investigation of SII in TNBC patients provided room for optimism, it had its drawbacks. First, we lacked external validation. Second, we could not avoid a selection bias of a retrospective, single-center study. Third, while diseases that impacted SII were excluded, some patients who carried these diseases might still have participated in the research if their medical records were not logged electronically.
Conclusion
We have revealed in our investigation that SII is a potential biomarker that could predict DFS and OS in TNBC, suggesting that SII’s role could be significant in the growth, proliferation, and prognosis of breast cancer cells. Given, therefore, that SII can be obtained easily, it could eventually be introduced in clinical use to identify progressive TNBC if more in-depth studies with little to no nuance are carried out to ascertain its specificity.
Disclosure
The authors report no conflicts of interest in this work.
References
- Brewster AM, Chavez-MacGregor M, Brown P. Epidemiology, biology, and treatment of triple-negative breast cancer in women of African ancestry. Lancet Oncol. 2014;15(13):e625–e634. doi:10.1016/S1470-2045(14)70364-X25456381
- Bianchini G, Balko JM, Mayer IA, Sanders ME, Gianni L. Triple-negative breast cancer: challenges and opportunities of a heterogeneous disease. Nat Rev Clin Oncol. 2016;13(11):674–690. doi:10.1038/nrclinonc.2016.6627184417
- Foulkes WD, Smith IE, Reis-Filho JS. Triple-negative breast cancer. N Engl J Med. 2010;363(20):1938–1948. doi:10.1056/NEJMra100138921067385
- Bosch A, Eroles P, Zaragoza R, Viña JR, Lluch A. Triple-negative breast cancer: molecular features, pathogenesis, treatment and current lines of research. Cancer Treat Rev. 2010;36(3):206–215. doi:10.1016/j.ctrv.2009.12.00220060649
- Criscitiello C, Azim HA Jr., Schouten PC, et al. Understanding the biology of triple-negative breast cancer. Ann Oncol. 2012;23(Suppl 6):vi13–vi18. doi:10.1093/annonc/mds18823012296
- Lu L, Zeng H, Gu X, Ma W. Circulating tumor cell clusters-associated gene plakoglobin and breast cancer survival. Breast Cancer Res Treat. 2015;151(3):491–500. doi:10.1007/s10549-015-3416-125957595
- Chen Q, Yao L, Burner D, et al. Epithelial membrane protein 2: a novel biomarker for circulating tumor cell recovery in breast cancer. Clin Transl Oncol. 2019;21(4):433–442.
- Wang M, Ji S, Shao G, et al. Effect of exosome biomarkers for diagnosis and prognosis of breast cancer patients. Clin Transl Oncol. 2018;20(7):906–911. doi:10.1007/s12094-017-1805-029143228
- Liu C, Xu X, Li B, et al. Single-exosome-counting immunoassays for cancer diagnostics. Nano Lett. 2018;18(7):4226–4232. doi:10.1021/acs.nanolett.8b0118429888919
- Hannafon BN, Trigoso YD, Calloway CL, et al. Plasma exosome microRNAs are indicative of breast cancer. Breast Cancer Res. 2016;18(1):90. doi:10.1186/s13058-016-0753-x27608715
- Wang Z, Katsaros D, Shen Y, et al. Biological and clinical significance of MAD2L1 and BUB1, genes frequently appearing in expression signatures for breast cancer prognosis. PLoS One. 2015;10(8):e0136246. doi:10.1371/journal.pone.013624626287798
- Shen Y, Katsaros D, Loo LW, et al. Prognostic and predictive values of long non-coding RNA LINC00472 in breast cancer. Oncotarget. 2015;6(11):8579–8592. doi:10.18632/oncotarget.328725865225
- Mu L, Tuck D, Katsaros D, et al. Favorable outcome associated with an IGF-1 ligand signature in breast cancer. Breast Cancer Res Treat. 2012;133(1):321–331. doi:10.1007/s10549-012-1952-522297468
- Sparano JA, Gray RJ, Makower DF, et al. Prospective validation of a 21-gene expression assay in breast cancer. N Engl J Med. 2015;373(21):2005–2014. doi:10.1056/NEJMoa151076426412349
- Liu C, Wang Q, Sun B, et al. Low BMI is correlated with increased TGF-beta and IL-10 mRNA levels in the peripheral blood of breast cancer patients. IUBMB Life. 2018;70(3):237–245. doi:10.1002/iub.172129405562
- Mantovani A, Allavena P, Sica A, Balkwill F. Cancer-related inflammation. Nature. 2008;454(7203):436–444. doi:10.1038/nature0720518650914
- Hanahan D, Weinberg RA. Hallmarks of cancer: the next generation. Cell. 2011;144(5):646–674. doi:10.1016/j.cell.2011.02.01321376230
- Ferrucci PF, Ascierto PA, Pigozzo J, et al. Baseline neutrophils and derived neutrophil-to-lymphocyte ratio: prognostic relevance in metastatic melanoma patients receiving ipilimumab. Ann Oncol. 2016;27(4):732–738. doi:10.1093/annonc/mdw01626802161
- Yu X, Wen Y, Lin Y, et al. The value of preoperative glasgow prognostic score and the C-reactive protein to albumin ratio as prognostic factors for long-term survival in pathological T1N0 esophageal squamous cell carcinoma. J Cancer. 2018;9(5):807–815. doi:10.7150/jca.2275529581759
- Russo A, Franchina T, Ricciardi GRR, et al. Baseline neutrophilia, derived neutrophil-to-lymphocyte ratio (dNLR), platelet-to-lymphocyte ratio (PLR), and outcome in non small cell lung cancer (NSCLC) treated with Nivolumab or Docetaxel. J Cell Physiol. 2018;233:6337–6343. doi:10.1002/jcp.v233.10
- Grenader T, Nash S, Plotkin Y, et al. Derived neutrophil lymphocyte ratio may predict benefit from cisplatin in the advanced biliary cancer: the ABC-02 and BT-22 studies. Ann Oncol. 2015;26(9):1910–1916. doi:10.1093/annonc/mdv25326037798
- Kwon BS, Jeong DH, Byun JM, et al. Prognostic value of preoperative lymphocyte-monocyte ratio in patients with ovarian clear cell carcinoma. J Cancer. 2018;9(7):1127–1134. doi:10.7150/jca.2405729675093
- He X, Li JP, Liu XH, et al. Prognostic value of C-reactive protein/albumin ratio in predicting overall survival of Chinese cervical cancer patients overall survival: comparison among various inflammation based factors. J Cancer. 2018;9(10):1877–1884. doi:10.7150/jca.2332029805715
- Liang Y, Wang W, Li J, et al. Combined use of the neutrophil-lymphocyte and platelet-lymphocyte ratios as a prognostic predictor in patients with operable soft tissue sarcoma. J Cancer. 2018;9(12):2132–2139. doi:10.7150/jca.2487129937932
- Shao S, Risch E, Burner D, et al. IFNgamma enhances cytotoxic efficiency of the cytotoxic T lymphocytes against human glioma cells. Int Immunopharmacol. 2017;47:159–165. doi:10.1016/j.intimp.2017.04.00328410529
- Lu L, Bai Y, Wang Z. Elevated T cell activation score is associated with improved survival of breast cancer. Breast Cancer Res Treat. 2017;164(3):689–696. doi:10.1007/s10549-017-4281-x28488141
- Suzuki R, Wei X, Allen PK, et al. Hematologic variables associated with brain failure in patients with small-cell lung cancer. Radiother Oncol. 2018. doi:10.1016/j.radonc.2018.05.026
- Liu C, Wu S, Meng X, et al. Predictive value of peripheral regulatory T cells in non-small cell lung cancer patients undergoing radiotherapy. Oncotarget. 2017;8(26):43427–43438. doi:10.18632/oncotarget.1523828624781
- van Eijck CHJ, Stricker BH, Petrillo A, et al. Systemic-inflammation-based score can predict prognosis in metastatic gastric cancer patients before first-line chemotherapy. Future Oncol. 2018;14(24):2493–2505.
- Huang W, Wang S, Zhang H, Zhang B, Wang C. Prognostic significance of combined fibrinogen concentration and neutrophil-to-lymphocyte ratio in patients with resectable non-small cell lung cancer. Cancer Biol Med. 2018;15(1):88–96. doi:10.20892/j.issn.2095-3941.2017.012429545972
- Hu B, Yang XR, Xu Y, et al. Systemic immune-inflammation index predicts prognosis of patients after curative resection for hepatocellular carcinoma. Clin Cancer Res. 2014;20(23):6212–6222. doi:10.1158/1078-0432.CCR-14-044225271081
- Aziz MH, Sideras K, Aziz NA. et al. The systemic-immune-inflammation index independently predicts survival and recurrence in resectable pancreatic cancer and its prognostic value depends on bilirubin levels. Annals of Surgery. 2018:1. doi:10.1097/SLA.0000000000002660
- Chen L, Yan Y, Zhu L, et al. Systemic immune-inflammation index as a useful prognostic indicator predicts survival in patients with advanced gastric cancer treated with neoadjuvant chemotherapy. Cancer Manag Res. 2017;9:849–867. doi:10.2147/CMAR.S15102629276407
- Yang J, Guo X, Wang M, et al. Pre-treatment inflammatory indexes as predictors of survival and cetuximab efficacy in metastatic colorectal cancer patients with wild-type RAS. Scientific Reports. 2017;7(1):17166. doi:10.1038/s41598-017-17130-629215037
- Fan L, Wang R, Chi C, et al. Systemic immune-inflammation index predicts the combined clinical outcome after sequential therapy with abiraterone and docetaxel for metastatic castration-resistant prostate cancer patients. Prostate. 2018;78(4):250–256. doi:10.1002/pros.2346529285775
- Lolli C, Basso U, Derosa L, et al. Systemic immune-inflammation index predicts the clinical outcome in patients with metastatic renal cell cancer treated with sunitinib. Oncotarget. 2016;7(34):54564–54571. doi:10.18632/oncotarget.1051527409344
- Jiang W, Chen Y, Huang J, et al. Systemic immune-inflammation index predicts the clinical outcome in patients with nasopharyngeal carcinoma: a propensity score-matched analysis. Oncotarget. 2017;8(39):66075–66086. doi:10.18632/oncotarget.1979629029493
- Tong YS, Tan J, Zhou XL, Song YQ, Song YJ. Systemic immune-inflammation index predicting chemoradiation resistance and poor outcome in patients with stage III non-small cell lung cancer. J Transl Med. 2017;15(1):221. doi:10.1186/s12967-017-1326-129089030
- Edge SB, Compton CC. The American Joint Committee On Cancer: the 7th edition of the AJCC cancer staging manual and the future of TNM. Ann Surg Oncol. 2010;17(6):1471–1474. doi:10.1245/s10434-010-0985-420180029
- Huang L, Liu S, Lei Y, et al. Systemic immune-inflammation index, thymidine phosphorylase and survival of localized gastric cancer patients after curative resection. Oncotarget. 2016;7(28):44185–44193. doi:10.18632/oncotarget.992327283904
- Fukuda H, Takagi T, Kondo T, Shimizu S, Tanabe K. Predictive value of inflammation-based prognostic scores in patients with metastatic renal cell carcinoma treated with cytoreductive nephrectomy. Oncotarget. 2018;9(18):14296–14305. doi:10.18632/oncotarget.2450729581844
- Geng Y, Shao Y, Zhu D, et al. Systemic immune-inflammation index predicts prognosis of patients with esophageal squamous cell carcinoma: a propensity score-matched analysis. Sci Rep. 2016;6:39482. doi:10.1038/srep3948228000729
- Yao M, Liu Y, Jin H, et al. Prognostic value of preoperative inflammatory markers in Chinese patients with breast cancer. Onco Targets Ther. 2014;7:1743–1752. doi:10.2147/OTT.S6965725328407
- Pistelli M, De Lisa M, Ballatore Z, et al. Pre-treatment neutrophil to lymphocyte ratio may be a useful tool in predicting survival in early triple negative breast cancer patients. BMC Cancer. 2015;15:195. doi:10.1186/s12885-015-1584-325884918
- Chen Y, Chen K, Xiao X, et al. Pretreatment neutrophil-to-lymphocyte ratio is correlated with response to neoadjuvant chemotherapy as an independent prognostic indicator in breast cancer patients: a retrospective study. BMC Cancer. 2016;16:320. doi:10.1186/s12885-016-2352-827198767
- Kao SC, Pavlakis N, Harvie R, et al. High blood neutrophil-to-lymphocyte ratio is an indicator of poor prognosis in malignant mesothelioma patients undergoing systemic therapy. Clin Cancer Res. 2010;16(23):5805–5813. doi:10.1158/1078-0432.CCR-10-224520956618
- Yamagishi T, Fujimoto N, Nishi H, et al. Prognostic significance of the lymphocyte-to-monocyte ratio in patients with malignant pleural mesothelioma. Lung Cancer. 2015;90(1):111–117. doi:10.1016/j.lungcan.2015.07.01426259877
- Templeton AJ, McNamara MG, Seruga B, et al. Prognostic role of neutrophil-to-lymphocyte ratio in solid tumors: a systematic review and meta-analysis. J Natl Cancer Inst. 2014;106(6):dju124. doi:10.1093/jnci/dju06124875653
- Cannon NA, Meyer J, Iyengar P, et al. Neutrophil-lymphocyte and platelet-lymphocyte ratios as prognostic factors after stereotactic radiation therapy for early-stage non-small-cell lung cancer. J Thorac Oncol. 2015;10(2):280–285. doi:10.1097/JTO.000000000000039925299234
- Song S, Li C, Li S, et al. Derived neutrophil to lymphocyte ratio and monocyte to lymphocyte ratio may be better biomarkers for predicting overall survival of patients with advanced gastric cancer. Onco Targets Ther. 2017;10:3145–3154. doi:10.2147/OTT.S13803928706446
- Franco AT, Corken A, Ware J. Platelets at the interface of thrombosis, inflammation, and cancer. Blood. 2015;126(5):582–588. doi:10.1182/blood-2014-08-53158226109205
- Houghton AM, Rzymkiewicz DM, Ji H, et al. Neutrophil elastase-mediated degradation of IRS-1 accelerates lung tumor growth. Nat Med. 2010;16(2):219–223. doi:10.1038/nm.208420081861
- Mohammed ZM, Going JJ, Edwards J, McMillan DC. The role of the tumour inflammatory cell infiltrate in predicting recurrence and survival in patients with primary operable breast cancer. Cancer Treat Rev. 2012;38(8):943–955. doi:10.1016/j.ctrv.2012.04.01122651904
- Ali HR, Provenzano E, Dawson SJ, et al. Association between CD8+ T-cell infiltration and breast cancer survival in 12,439 patients. Ann Oncol. 2014;25(8):1536–1543. doi:10.1093/annonc/mdu19124915873