
Abstract
Purpose
To investigate the prognostic value of combined serum carcinoembryonic antigen (CEA) levels and fibrinogen/albumin ratio (FAR) in patients with resectable gastric cancer (GC).
Introduction
This retrospective study evaluated the CEA, fibrinogen, and albumin levels and other clinicopathological features of GC patients. The prognostic significance of these factors for overall survival (OS) was assessed using Kaplan–Meier curves and univariate and multivariate Cox proportional models.
Patients and Methods
A total of 267 patients were included. The optimal cutoff values of CEA and FAR were 3.2 ng/mL and 0.086, respectively. Patients were stratified into three groups based on this cutoff value: CEA-FAR=0 (CEA <3.2 ng/mL and FAR <0.086), CEA-FAR=1 (CEA ≥3.2 ng/mL or FAR ≥0.086), and CEA-FAR=2 (CEA ≥3.2 ng/mL and FAR ≥0.086).
Results
Higher CEA-FAR was strongly associated with age, tumor size, tumor invasion, lymph node status, and TNM stage (all P<0.05). The OS rates differed significantly between these 3 groups (88.9% vs 65.0% vs 46.9%, P<0.001). Multivariate analysis showed that CEA-FAR was an independent prognostic factor for OS (P<0.001). The area under the curve was larger for CEA-FAR than for either CEA or FAR alone (0.683, 0.644, and 0.669, respectively).
Conclusion
Preoperative CEA-FAR could be a potential blood marker for predicting tumor progression and the prognosis of GC patients. Patients with a higher CEA-FAR should undergo extensive follow-up.
Introduction
Gastric cancer (GC) is among the most common malignant tumors of the digestive tract and has a high risk of recurrence and distant metastasis. In China, GC has the second highest incidence rate and third highest mortality rate among all types of cancer.Citation1 Preoperative evaluation is crucial in the treatment of GC. Therefore, it is crucial to find a simple and convenient preoperative prognostic factor to identify high-risk patients and to guide further treatment.
Fibrinogen, a glycoprotein synthesized by the liver, is produced in response to inflammation or activation of the coagulation system and plays an important role in the coagulation cascade.Citation2 Inflammation is a hallmark of cancer, and malignant tumors compromise the coagulation, anticoagulation, and fibrinolysis systems of the body through various mechanisms, resulting in abnormal coagulation function and fibrinogen elevation.Citation3 Fibrinogen is an acute-phase-response protein that can increase under systemic inflammatory conditions. Previous studies have shown that increased plasma fibrinogen indicates poor prognosis of various cancers including GC.Citation4,Citation5 Malnutrition is a common clinical manifestation of gastrointestinal cancers and is also a prognostic indicator of cancer. Albumin is commonly used to assess nutritional status, and hypoalbuminemia is associated with poor prognosis in several cancers such as lung, gastric, and colon cancers.Citation6 Both an increase in serum fibrinogen and a decrease in albumin are associated with systemic inflammation.Citation4,Citation6 Furthermore, it has been recently reported that the fibrinogen-to-albumin ratio (FAR) can be used as a biomarker to predict the prognosis of various cancers such as hepatocellular carcinoma, breast cancer, and gallbladder cancer;Citation7–Citation9 however, the role of FAR in GC remains relatively unexplored.
Tumor markers can serve as indicators for the diagnosis, treatment, and prognosis of GC. CEA is a common serum marker for malignant gastrointestinal tumors and is important in the diagnosis of GC; CEA expression is also an independent risk factor for poor prognosis in GC.Citation10 We hypothesized that a combination of tumor and patient characteristics can be used to predict the survival of GC patients. Accordingly, this study aimed to evaluate the clinical value of CEA-FAR as a novel prognostic biomarker in GC. Further, we also evaluated the association between CEA-FAR and the clinicopathological features of GC.
Patients and Methods
Patients
This retrospective study evaluated patients with primary GC who underwent radical gastrectomy between June 2012 and June 2016 in the Department of Surgical Oncology, the First Affiliated Hospital, Medical of College, Zhejiang University. The inclusion criteria were: (1) complete patient data (including sex, age, pathological type, tumor-node-metastasis (TNM) stage, and survival); (2) no neoadjuvant chemotherapy or radiotherapy prior to surgery; (3) undergone radical gastrectomy with confirmation of adenocarcinoma by postoperative pathology; (4) no metastasis to the lung, liver, bone, and other organs on preoperative imaging and no distant metastasis found during the surgery. The exclusion criteria were: (1) blood disorders; (2) presence of another cancer; (3) hepatic or renal insufficiency based on abnormal alanine aminotransferase and creatinine levels; (4) palliative surgery or short-circuit operation. This study was approved by the Institutional Review Board of the First Affiliated Hospital, College of Medicine, Zhejiang University, and this study was conducted in accordance with the Declaration of Helsinki. Because informed consent was deemed unnecessary by the ethical committee, the requirement to obtain written informed consent was waived.
Clinical Data
Fasting peripheral blood samples were collected within 1 week prior to surgery and sent to the clinical laboratory for routine blood tests and to assess CEA levels, liver and kidney function, coagulation function, and other indicators. FAR was calculated as previously described,Citation11 and the neutrophil-to-lymphocyte ratio (NLR) was determined by dividing the neutrophil count by the lymphocyte count.
The clinical data of the GC patients, including age, sex, tumor size, location, degree of differentiation, and tumor stage, were collected from the hospital information system. Staging was done according to the TNM classification of the American Joint Committee on Cancer (8th edition).
Survival and Follow-Up
All patients were followed up by telephone and outpatient visits after discharge, with the last follow-up conducted in June 2019. Survival time was calculated from the date of diagnosis to date of death or the last follow-up.
Statistical Analysis
The optimal cutoff values for CEA, FAR, NLR, and other variables were obtained via receiver operating characteristic (ROC) curve analysis. The patients were then divided into 2 groups according to the cutoff. Additionally, the patients were divided into 3 groups according to the CEA-FAR score: CEA-FAR=0 (CEA <3.2 ng/mL and FAR <0.086), CEA-FAR=1 (CEA ≥3.2 ng/mL or FAR ≥0.086), and CEA-FAR=2 (CEA ≥3.2 ng/mL and FAR ≥0.086) (). Chi-square or Fisher’s exact test was used for categorical variables. Kaplan–Meier method was used for survival analysis. Multivariate Cox model was used to analyze the factors influencing survival and the prognosis of GC. Variables found significant on univariate analysis were entered into multivariate analysis. All statistical analyses were performed using SPSS 20.0 software, and P<0.05 was considered statistically significant.
Table 1 Prognostic Scores of CEA, FAR and CEA-FAR
Results
Patient Characteristics
In total, 267 patients (176 (65.9%) men and 91 (34.1%) women) with a median age of 63 years (range, 26–91 years) were included in this study. Their clinicopathological characteristics are summarized in .
Table 2 The Clinicopathological Features of GC Patients
Optimal Cutoff Values of CEA and FAR
The optimal cutoff value of CEA for OS is 3.2 ng/mL (area under curve, AUC=0.644, 95% CI: 0.566–0.723, P<0.001, ). The optimal cutoff value of FAR for OS is 0.086 (AUC=0.669, 95% CI: 0.595–0.742, P<0.001, ). Based on these cutoff values, patients were divided into 2 groups: high CEA (≥3.2 ng/mL, n=91) and low CEA (<3.2 ng/mL, n=176); high FAR (≥0.086, n=73) and low FAR (<0.086, n=194).
Figure 1 Receiver operating characteristics curve analysis of CEA, FAR (A) and CEA-FAR (B) for OS in GC patients.
Note: CEA-FAR: CEA<3.2 and FAR<0.086 represent 0, CEA≥3.2 or FAR≥0.086 represent 1, CEA≥3.2 and FAR≥0.086 represent 2.
Abbreviations: GC, gastric cancer; CEA, carcinoembryonic antigen; FAR, fibrinogen/albumin ratio; OS, overall survival.
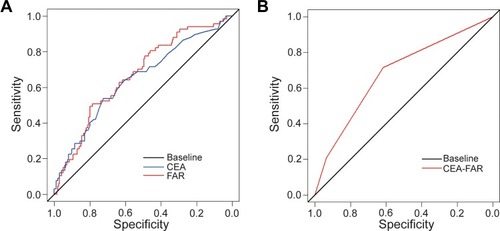
The AUC of CEA-FAR for OS () is 0.683 (95% CI: 0.614–0.751), which is slightly higher than that of FAR (AUC: 0.669 (95% CI: 0.595–0.742), ) and CEA (AUC: 0.644 (95% CI: 0.566–0.723), ). These results suggest that CEA-FAR may be superior to CEA or FAR alone as a prognostic marker of GC.
Relationship of Preoperative CEA and FAR with Clinicopathological Variables
Preoperative CEA and FAR were associated with various clinicopathological variables of GC patients (). High CEA significantly correlated with age (P=0.023), sex (P=0.001), tumor size (P<0.001), tumor invasion (P=0.029), lymph node metastasis (P=0.001), and TNM stage (P=0.004), but not with tumor location and differentiation (all P>0.05). Similarly, preoperative FAR significantly correlated with age (P=0.001), tumor size (P<0.001), differentiation (P=0.032), tumor invasion (P<0.001), lymph node metastasis (P <0.001), and TNM stage (P<0.001), but not with sex and tumor location (all P>0.05).
Prognostic Significance of Preoperative CEA and FAR
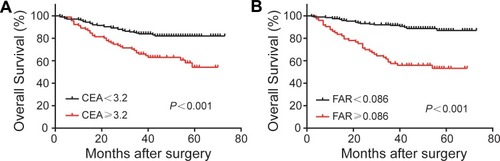
Kaplan–Meier analysis and Log rank tests for the prognostic value of preoperative CEA and FAR showed that the OS rate and median OS time of the low CEA group were significantly higher than those of the high CEA group (82.4 vs 60.4%, 41.0 vs 39.0 months, P<0.001, ). Further, the OS rate and median OS time in the low FAR group were also significantly higher than those in the high FAR group (89.2 vs 54.8%, 41.0 vs 38.0 months, P<0.001, ). Kaplan–Meier analyses for OS based on the preoperative CEA and FAR in different N stages were also conducted (Supplement Figure 1). Only preoperative CEA could predict OS of patients with N0 and N2 stages (Supplement Figure 1A and E). However, pretreatment CEA could not predict OS of patients with N1 and N3 stage (Supplement Figure 1C and G), as well as FAR in all N stages (Supplementary Figure 1B, D, F and H).
Figure 2 Kaplan–Meier survival curves for OS according to CEA (A) and FAR (B) in GC patients.
Abbreviations: OS, overall survival; GC, gastric cancer; CEA, carcinoembryonic antigen; FAR, fibrinogen/albumin ratio.
Prognostic Analysis Based on CEA-FAR
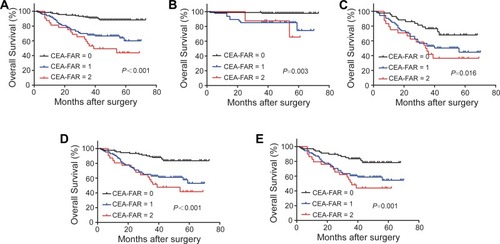
As mentioned above, FAR and CEA are currently used as prognostic markers in GC patients, but whether CEA-FAR has the same prognostic value is still unclear. In this study, the OS was significantly different between the three CEA-FAR groups (CEA-FAR=0, 1, and 2: 88.9%, 65.0%, and 46.9%, respectively; P <0.001, ). In addition, even when patients were stratified based on clinical stage, CEA-FAR appeared to have a predictive value for pathological stage I–II and III when the (). Furthermore, CEA-FAR was a prognostic indictor for OS in advanced GC patients, who represents stage T1 regardless of lymph node involvement () and patients with lymph node metastasis (). We also found significant differences in age (P <0.001), tumor size (P <0.001), tumor invasion (P <0.001), lymph node metastasis (P <0.001), and TNM stage (P <0.001) () between the three groups upon analyzing the relationship between CEA-FAR and clinicopathological features.
Table 3 The Clinicopathological Characteristic Stratified by the CEA-FAR Score
Figure 3 OS based on CEA-FAR in GC patients with stage I–III (A), I–II (B), III (C), advanced GC (D) and lymph node metastasis (E).
Note: CEA-FAR: CEA<3.2 and FAR<0.086 represent 0, CEA≥3.2 or FAR≥0.086 represent 1, CEA≥3.2 and FAR≥0.086 represent 2.
Abbreviations: OS, overall survival; GC, gastric cancer; CEA, carcinoembryonic antigen; FAR, fibrinogen/albumin ratio.
Univariate and Multivariate Survival Analyses
To further identify the predictors of OS after gastrectomy, the clinicopathological variables were evaluated using univariate and multivariate analyses. The univariate analysis revealed that age (HR: 3.307, 95% CI: 1.688–6.478, P=0.001), tumor size (HR: 3.495, 95% CI: 1.871–6.528, P<0.001), FAR (HR: 2.621, 95% CI: 1.618–4.244, P <0.001), CEA level (HR: 2.296, 95% CI: 1.421–3.71, P=0.001), CEA-FAR (CEA-FAR=1: HR: 2.87, 95% CI: 1.636–5.034; CEA-FAR=2: HR: 4.918, 95% CI: 2.463–9.82, P<0.001), and TNM stage (stage II: HR: 5.609, 95% CI: 1.243–25.311, P=0.025; stage III: HR: 20.615, 95% CI: 5.023–84.615, P<0.001) significantly correlated with patient prognosis ().
Table 4 Univariate and Multivariate Analyses of Prognostic Factors in GC Patients
According to the multivariate analysis, CEA-FAR remained as a predictor for outcome (CEA-FAR=1: HR: 1.642, 95% CI: 0.922–2.923, P=0.092; CEA-FAR=2: HR: 2.308, 95% CI: 1.13–4.716, P=0.022). These results show that age (P=0.012), CEA-FAR (P=0.022), and TNM stage (P<0.001) are important prognostic variables associated with poor OS ().
Discussion
This study established the relationships between systemic inflammation, clinicopathological features, and survival in GC patients with resectable tumors. We found that higher FAR was associated with a larger tumor size, poorer differentiation, more severe lymph node metastasis, and more advanced TNM stage. Similarly, high CEA also correlated with increased age, a larger tumor size, more lymph node metastasis, and more advanced TNM stage. Notably, this study reveals for the first time that CEA-FAR is a more effective prognostic marker than either CEA or FAR alone in GC patients undergoing radical gastrectomy. GC patients with CEA-FAR=2 group had worse prognoses than those with CEA-FAR=0, indicating that increased CEA-FAR is related to tumor burden and tumor progression, making it a promising prognostic marker in GC patients.
Elevated FAR was found to be an independent prognostic factor for poor survival in GC patients, which is consistent with findings in previous reports. For example, a study by Hwang et al showed that FAR can predict the survival of breast cancer patients.Citation7 Xu et al also found that elevated FAR is associated with poor prognosis and increased risk of recurrence of hepatocellular carcinoma.Citation9 Collectively, these findings, along with the findings from the present study, show that high FAR has a prognostic importance for various malignant tumors.
Although the reasons underlying the association between increased FAR and poor prognosis is complex and has not been clarified, some mechanisms have been proposed. A hypercoagulable state is closely related to the development of malignant tumors. Fibrinogen decomposes to form fibrin, which provides a scaffold for growth, infiltration, and metastasis of tumor cells.Citation12 Fibrinogen can also act as a ligand for various adhesion molecules, increasing the adhesion and binding between platelets and tumor cells and promoting their infiltration and metastasis.Citation13 Fibrinogen is not only an important component of the coagulation system, but is also an acute phase response protein, making it an indicator of systemic inflammation. Previous studies have shown that fibrinogen plays an important role in inflammatory reactions and the synthesis of pro-inflammatory cytokines.Citation14,Citation15 Fibrinogen mediates the release of pro-inflammatory cytokines, which promotes the proliferation and progression of tumor cells.Citation16 Clinically, Lee et al found that the plasma fibrinogen level was significantly higher in cancer patients than in patients with benign diseases, and fibrinogen levels increased during recurrence or metastasis.Citation17 Pichler et al found that fibrinogen was associated with lymph node metastasis and clinical staging in cancer.Citation18 In lung cancer, tumor cells can produce IL-6 to stimulate secretion of fibrinogen.Citation19 Perisanidis et al proposed that reducing fibrinogen concentration could prolong survival of patients with solid tumors.Citation20
Albumin, which is the most abundant protein in plasma, is commonly used to assess nutritional status in clinical practice. Hypoalbuminemia indicates a poor nutritional status. Malnutrition can lead to the decline of immune function in cancer patients, thus increasing the risk of postoperative complications and tumor progression.Citation21 Previous studies have reported that hypoalbuminemia is associated with disease progression and poor prognosis in patients with colon cancer,Citation22 pancreatic cancer,Citation23 non-small cell lung cancer,Citation24 ovarian cancer,Citation25 and GC.Citation26
Furthermore, this study shows that preoperative CEA is an independent prognostic factor of survival, consistent with previous studies. Zhan et al reported that preoperative CEA elevation is a predictor of OS in early GC.Citation10 Guo et al believe that CEA alone or in combination with CA19-9 and CA72-4 can be used as a predictor of cancer-specific survival and is important in predicting survival and informing treatment decisions in GC.Citation27
Based on these findings, we used the combination of CEA level and FAR (CEA-FAR) as a novel biomarker in GC and found that it is a promising predictor of prognosis. Tumor progression is closely related to both patient and tumor characteristics. Elevated CEA level is associated with tumor invasion and metastasis, while FAR reflects the patient’s inflammatory status, coagulation function, and nutritional status. Here, we confirmed that the combination of CEA and FAR can effectively predict the survival of GC patients, and that its predictive capability is superior to that of either CEA or FAR alone.
However, this study also has some limitations. First, this was a single-center retrospective study and was likely affected by selection bias. Second, we cannot eliminate the potential bias due to the difference in the types of surgery and postoperative chemotherapy regimens. Therefore, the clinical value of preoperative CEA-FAR as a prognostic predictor in GC should be further clarified in larger, multi-center prospective studies.
Conclusion
Preoperative CEA-FAR is an independent prognostic factor of OS in GC patients. Its convenience, low cost, and high repeatability makes it a valuable indicator of prognosis in GC patients. The findings of this study provide a basis for more accurate and individualized treatment.
Acknowledgments
This study was supported by the Medical Health Science and Technology Project of Zhejiang Provincial Health Commission (Grant No. 2017209495).
Disclosure
The authors report no conflicts of interest in this work.
References
- Chen W, Zheng R, Baade PD, et al. Cancer statistics in China, 2015. CA Cancer J Clin. 2016;66(2):115–132. doi:10.3322/caac.2133826808342
- Liang Y, Wang W, Que Y, et al. Prognostic value of the fibrinogen/albumin ratio (FAR) in patients with operable soft tissue sarcoma. BMC Cancer. 2018;18(1):942. doi:10.1186/s12885-018-4856-x30285656
- Wen L, Guo L, Zhang W, et al. Cooperation between the inflammation and coagulation systems promotes the survival of circulating tumor cells in renal cell carcinoma patients. Front Oncol. 2019;9:504. doi:10.3389/fonc.2019.0050431263677
- Wu ZJ, Xu H, Wang R, et al. Cumulative score based on preoperative fibrinogen and pre-albumin could predict long-term survival for patients with resectable gastric cancer. J Cancer. 2019;10(25):6244–6251. doi:10.7150/jca.3515731772657
- Liu X, Liu Z, Lin E, Chen Y, Sun X, Zhou Z. A cumulative score based on preoperative fibrinogen and the neutrophil-lymphocyte ratio to predict outcomes in resectable gastric cancer. Cancer Manag Res. 2018;10:3007–3014. doi:10.2147/CMAR.S17465630214295
- Gupta D, Lis CG. Pretreatment serum albumin as a predictor of cancer survival: a systematic review of the epidemiological literature. Nutr J. 2010;9:69. doi:10.1186/1475-2891-9-6921176210
- Hwang KT, Chung JK, Roh EY, et al. Prognostic influence of preoperative fibrinogen to albumin ratio for breast cancer. J Breast Cancer. 2017;20(3):254–263. doi:10.4048/jbc.2017.20.3.25428970851
- Xu WY, Zhang HH, Xiong JP, et al. Prognostic significance of the fibrinogen-to-albumin ratio in gallbladder cancer patients. World J Gastroenterol. 2018;24(29):3281–3292. doi:10.3748/wjg.v24.i29.328130090008
- Xu Q, Yan Y, Gu S, et al. A novel inflammation-based prognostic score: the fibrinogen/albumin ratio predicts prognoses of patients after curative resection for hepatocellular carcinoma. J Immunol Res. 2018;2018:4925498. doi:10.1155/2018/492549830027102
- Feng F, Tian Y, Xu G, et al. Diagnostic and prognostic value of CEA, CA19–9, AFP and CA125 for early gastric cancer. BMC Cancer. 2017;17(1):737. doi:10.1186/s12885-017-3738-y29121872
- Tan Z, Zhang M, Han Q, et al. A novel blood tool of cancer prognosis in esophageal squamous cell carcinoma: the fibrinogen/albumin ratio. J Cancer. 2017;8(6):1025–1029. doi:10.7150/jca.1649128529615
- Repetto O, De Re V. Coagulation and fibrinolysis in gastric cancer. Ann N Y Acad Sci. 2017;1404(1):27–48. doi:10.1111/nyas.1345428833193
- Palumbo JS, Talmage KE, Massari JV, et al. Platelets and fibrin(ogen) increase metastatic potential by impeding natural killer cell-mediated elimination of tumor cells. Blood. 2005;105(1):178–185. doi:10.1182/blood-2004-06-227215367435
- Luyendyk JP, Schoenecker JG, Flick MJ. The multifaceted role of fibrinogen in tissue injury and inflammation. Blood. 2019;133(6):511–520. doi:10.1182/blood-2018-07-81821130523120
- Jenkins DR, Craner MJ, Esiri MM, DeLuca GC. Contribution of fibrinogen to inflammation and neuronal density in human traumatic brain injury. J Neurotrauma. 2018;35(19):2259–2271. doi:10.1089/neu.2017.529129609523
- Zhang F, Wang Y, Sun P, et al. Fibrinogen promotes malignant biological tumor behavior involving epithelial-mesenchymal transition via the p-AKT/p-mTOR pathway in esophageal squamous cell carcinoma. J Cancer Res Clin Oncol. 2017;143(12):2413–2424. doi:10.1007/s00432-017-2493-428801734
- Lee SE, Lee JH, Ryu KW, et al. Preoperative plasma fibrinogen level is a useful predictor of adjacent organ involvement in patients with advanced gastric cancer. J Gastric Cancer. 2012;12(2):81–87. doi:10.5230/jgc.2012.12.2.8122792520
- Pichler M, Hutterer GC, Stojakovic T, Mannweiler S, Pummer K, Zigeuner R. High plasma fibrinogen level represents an independent negative prognostic factor regarding cancer-specific, metastasis-free, as well as overall survival in a European cohort of non-metastatic renal cell carcinoma patients. Br J Cancer. 2013;109(5):1123–1129. doi:10.1038/bjc.2013.44323922109
- Yamaguchi T, Yamamoto Y, Yokota S, Nakagawa M, Ito M, Ogura T. Involvement of interleukin-6 in the elevation of plasma fibrinogen levels in lung cancer patients. Jpn J Clin Oncol. 1998;28(12):740–744. doi:10.1093/jjco/28.12.7409879291
- Pergialiotis V, Doumouchtsis SK, Perrea D, Vlachos GD. The impact of underweight status on the prognosis of ovarian cancer patients: a meta-analysis. Nutr Cancer. 2016;68(6):918–925. doi:10.1080/01635581.2016.119002127351098
- Yamamoto M, Saito H, Uejima C, et al. Combination of serum albumin and cholinesterase levels as prognostic indicator in patients ith colorectal cancer. Anticancer Res. 2019;39(2):1085–1090. doi:10.21873/anticanres.1321730711999
- Li Z, Xu Z, Huang Y, et al. Prognostic values of preoperative platelet-to-lymphocyte ratio, albumin and hemoglobin in patients with non-metastatic colon cancer. Cancer Manag Res. 2019;11:3265–3274. doi:10.2147/CMAR.S19143231114364
- Hang J, Xue P, Yang H, et al. Pretreatment C-reactive protein to albumin ratio for predicting overall survival in advanced pancreatic cancer patients. Sci Rep. 2017;7(1):2993. doi:10.1038/s41598-017-03153-628592881
- Zhang L, Zhang H, Yue D, et al. The prognostic value of the preoperative albumin to alkaline phosphatase ratio in patients with non-small cell lung cancer after surgery. Thorac Cancer. 2019;10(7):1581–1589. doi:10.1111/1759-7714.1310731161711
- Liu Y, Chen S, Zheng C, et al. The prognostic value of the preoperative c-reactive protein/albumin ratio in ovarian cancer. BMC Cancer. 2017;17(1):285. doi:10.1186/s12885-017-3220-x28431566
- Mao M, Wei X, Sheng H, et al. C-reactive protein/albumin and neutrophil/lymphocyte ratios and their combination predict overall survival in patients with gastric cancer. Oncol Lett. 2017;14(6):7417–7424. doi:10.3892/ol.2017.717929344182
- Guo J, Chen S, Li S, et al. A novel classifier based on three preoperative tumor markers predicting the cancer-specific survival of gastric cancer (CEA, CA19-9 and CA72-4). Oncotarget. 2018;9(4):4814–4822. doi:10.18632/oncotarget.2330729435143