Abstract
Background
Radium-223 chloride (223Ra; Alpharadin) is an alpha-emitting radioisotope that targets areas of osteoblastic metastasis and is excreted by the small intestine. When compared with beta-emitters (eg, strontium-89, samarium-153), 223Ra delivers a high quantity of energy per track length with short tissue penetration.
Objective
This review describes the mechanism, radiobiology, and preclinical development of 223Ra and discusses the clinical data currently available regarding its safety and efficacy profile.
Methods
Data from clinical trials including abstracts were collected and reviewed using the PubMed Database, as well as the American Society of Clinical Oncology abstract database.
Conclusion
Current bone-targeted therapies fall into two main categories: antiresorptive agents (eg, zoledronic acid, denosumab), which have been shown to delay skeletal-related events, and radiopharmaceuticals (eg, samarium-153), which may have a role in pain palliation. Historically, neither antiresorptive agents nor radiopharmaceuticals have shown definitive evidence of improved overall survival or other antitumor effects in metastatic castrate-resistant prostate cancer (mCRPC). Radiopharmaceuticals are limited by myelosuppresion, thrombocytopenia, and renal excretion. In a recently reported randomized Phase III trial in men with symptomatic bone-metastatic CRPC who had received or were ineligible for docetaxel chemotherapy, 223Ra treatment resulted in improved overall survival and delayed skeletal-related events. Toxicity consisted of minor gastrointestinal side effects and mild neutropenia and thrombocytopenia that were rarely severe. Pending regulatory approval, 223Ra may represent a unique and distinct option for an important subgroup of patients with mCRPC; future trials should address its use in combination or in sequence with existing and novel agents.
Introduction
Prostate cancer is the most common cancer in men and the second-leading cause of cancer death in men, with 241,740 new diagnoses and 28,170 deaths projected in the US in 2012.Citation1 Advanced prostate cancer has a penchant to metastasize to bone, possibly due to osteomimicry or altered adhesion molecules.Citation2,Citation3 Among patients with metastatic, castrate-resistant prostate cancer (mCRPC) treated with first-line chemotherapy, almost 90% have radiographic evidence of bone metastasis.Citation4,Citation5 Morbidity from complications of osseous metastases, such as pathologic fractures, spinal cord compression, and pain, greatly impairs the quality of life of patients with mCRPC. In addition, pain due to mCRPC is a strong independent prognostic factor for death, and is included in contemporary nomograms for survival in this disease,Citation6–Citation9 thus agents that can reduce pain and suffering due to metastatic prostate cancer may improve not only quality of life but also quantity of life.
Mitoxantrone chemotherapy and several radioisotopes, such as samarium-153 (153Sm) and strontium-89 (89Sr), were the first therapies approved for palliation of bone pain in patients with mCRPC, but without evidence of improvement in overall survival.Citation10,Citation11 Since 2004, four systemic therapies have been approved on the basis of improvements in overall survival, with varying effects on bone pain and skeletal complications.Citation4,Citation5,Citation12–Citation14 These agents, particularly the taxanes docetaxel (Taxotere®; Sanofi-Aventis, Bridgewater NJ), cabazitaxel (Jevtana®; Sanofi-Aventis), and the novel androgen biosynthesis inhibitor abiraterone acetate (Zytiga®; Janssen Biotech, Inc, Horsham, PA), have direct antitumor effects that may result in pain palliation. Contemporaneously, two osteoclast inhibitors (zoledronic acid [Zometa®; Novartis AG, Basel, Switzerland] and denosumab [Xgeva®; Amgen Inc, Thousand Oaks, CA]) have been approved on the basis of delay of skeletal-related events (SREs; pathologic fracture, spine cord compression, and requirement for radiation or surgery to bone), but without improvements in overall survival (OS).Citation15,Citation16 In addition, the novel androgen signaling inhibitor MDV3100 (enzalutamide, Xtandi®; Medivation, Inc, San Francisco, CA) has demonstrated improvements in OS and palliative end points; its approval was granted August 31, 2012, as this article went to press.Citation17–Citation19 Prior to the development of 223Ra (Alpharadin®; Algeta ASA, Oslo, Norway/Bayer AG, Leverkusen, Germany), no specifically bone-targeted therapy has been shown to improve median OS in the population of patients with mCRPC with osseous metastases.
Survival-prolonging systemic therapies currently approved for mCRPC include docetaxel, cabazitaxel, sipuleucel-T (Provenge®; Dendreon, Seattle, WA), abiraterone, and MDV3100 (). However, the effects of these therapies on skeletal complications are not well reported. Pain response is the only SRE that has been routinely reported (), with much fewer data on prevention or delay of SREs. A special case to this has been sipuleucel-T, which is specifically indicated for men with mCRPC who have minimal to no symptoms. As a reference, the palliative chemotherapy regimen of mitoxantrone/prednisone demonstrated a 29% response on the Present Pain Intensity (PPI) scale versus 12% with prednisone alone (P = 0.01), with a duration of 43 versus 18 weeks (P < 0.0001).Citation10 The landmark TAX-327 study showed a pain response of 35% versus 22% (P = 0.01) on the PPI scale for docetaxel/prednisone versus mitoxantrone/prednisone, with a duration of 3.5 versus 4.8 months (P not significant).Citation5 Patients who experienced a pain response in this trial were found to have improved overall survival as compared with those men without such a response.Citation7 In the post-docetaxel mCRPC setting, cabazitaxel/prednisone showed no improvement over mitoxantrone/prednisone on the PPI scale (9.2% vs 7.7%; P = 0.63; duration not reached) in the TROPIC trial.Citation13 In a similar post-docetaxel setting, the COU-AA-301 study demonstrated a 44% versus 27% pain response on the Brief Pain Inventory (BPI) scale for abiraterone/prednisone vs placebo/prednisone, with a time to progression of approximately 8 versus 5 months (25th percentile; P = 0.0056).Citation20 The great variability in pain response for the control arms (7.7% for mitoxantrone/prednisone in the TROPIC study, and 27% for prednisone alone in the COU-AA-301 study) suggests great variability in the reporting methods. Notably, in the COU-AA-301 study, the time to SRE was also delayed to approximately 10 versus 5 months (P = 0.0006). There were previously no other data regarding prevention or delay of SREs with the other survival-prolonging systemic therapies.
Table 1 Overall survival benefit in recent Phase III trials in mCRPC
Table 2 Pain responses in randomized studies of survival prolonging therapies in mCRPC
Bone-targeted osteoclast inhibitors and bone-seeking radiopharmaceuticals have been approved for mCRPC on the basis of prevention or delay of SREs and palliation of pain, respectively. Zoledronic acid, a bisphosphonate that inhibits osteoclasts, significantly delayed the time to SRE versus placebo (approximately 16 versus 11 months, P = 0.009) and also improved pain and analgesia scores.Citation15,Citation21 More recently, a monoclonal antibody to the receptor activator of NF-κB ligand (RANKL), denosumab, has also been approved. In a placebo-controlled Phase III trial, denosumab showed a 3.6-month improvement in time to first SRE over zoledronic acid (20.7 versus 17.1 months; P = 0.0002 [noninferiority], P = 0.008 [superiority]).Citation16 Of note, neither zoledronic acid nor denosumab demonstrated improvements in prostate-specific antigen (PSA) levels, overall disease progression, or overall survival. Thus, while these are bone-targeted agents, they may have a greater effect on bone health and quality than on the tumor microenvironment, which supports metastatic cancer and promotes treatment resistance. An ideal tumor microenvironment–targeting agent would thus not only prevent symptomatic deterioration but also improve upon disease-related outcomes, particularly OS.
In addition to osteoclast inhibitors, therapeutic radioisotopes that have a predilection to accumulate in bone turnover sites can be administered. These radiopharmaceuticals emit either alpha or beta particles. An alpha particle, which is ejected from a heavy nucleus during alpha decay, consists of two neutrons and two protons (ie, a helium nucleus).Citation22 A beta particle is an electron released from a nucleus containing excess neutrons during beta decay, in which one neutron is converted to a proton, an electron, and a neutrino.Citation22 Both α- and β-particles can deliver damaging radiation locally to cancerous cells. The most commonly used radiopharmaceuticals, both β-emitters, currently approved in the US for treatment of bone metastases are 89Sr (Metastron®; GE Healthcare, Arlington Heights, IL) and 153Sm (Quadramet®; EUSA Pharma, Oxford, UK). There are key differences in the physical properties of these radioisotopes, which have important clinical implications (). 89Sr is a pure β-emitter with a long half-life (50 days), whereas 153Sm has a much shorter half-life (1.9 days) and is also a γ-emitter, which allows posttreatment scintigraphic imaging. In addition, 89Sr emits higher-energy beta particles, resulting in greater tissue penetration and consequently higher bone marrow toxicity. Multiple randomized trials have been conducted with 89Sr and 153Sm in patients with mCRPC.Citation23–Citation29 There was no demonstration of improvement in overall survival in Phase III trials, although palliative benefits were seen that formed the basis of US FDA approval. One recent meta-analysis concluded that, although there is some evidence that these beta-emitting radioisotopes might provide a small benefit with complete reduction in pain over 1–6 months and no increase in analgesic use, severe adverse effects (mainly leukopenia and thrombocytopenia) are relatively frequent.Citation11 Nonetheless, 153Sm can be administered in repeat doses, once hematologic toxicities have recovered, for persistent pain.Citation30 Other limitations to 89Sr and 153Sm include the fact that they are renally excreted; this is not ideal in patients with genitourinary cancers. Overall, 89Sr and 153Sm might provide some palliative of pain, at the potential expense of significant hematologic toxicities and without demonstrated OS benefit. Ongoing work of these agents in combination with chemotherapy may optimize their efficacy.Citation31–Citation34
Table 3 Properties of selected radiopharmaceuticals for treatment of bone metastases in mCRPC
In comparison to beta-emitting radioisotopes, radium- 223 (223Ra; Alpharadin®, Algeta) is an α-emitter that delivers radiation with a higher biologic effect to a more localized area. In a large randomized Phase III trial, 223Ra has recently demonstrated improvements in OS, time to first SRE, and biochemical parameters, with a remarkably tolerable adverse-event profile, in men with bone-metastatic CRPC.Citation35 While 223Ra has not yet been approved for use in the US, and there is little experience in the US with the use of this agent, it represents the first bone-targeted therapeutic radiopharmaceutical to demonstrate a survival benefit, which has been the benchmark for recent FDA approvals in this disease setting. An expanded access trial of 223Ra in men with mCRPC with bone metastases is planned.Citation36 Many questions have arisen as to the appropriate sequencing of existing and novel therapies with 223Ra and if/how to combine 223Ra with these systemic therapies. This manuscript will review the preclinical and clinical development of 223Ra, and comment on its potential role and use in the armamentarium of therapy for mCRPC.
Radiobiology, mechanism of action, and preclinical development of 223Ra
Bone-seeking therapeutic radiopharmaceuticals are unique among anticancer therapies in that they actually target the stroma rather than the tumor itself: the target is calcium hydroxyapatite in bone. Ionizing radiation can thus be selectively delivered to areas of increased osteoblastic activity, allowing the targeting of multiple metastases simultaneously, including both symptomatic as well as asymptomatic lesions. As mentioned above, the commonly used clinically available radiopharmaceuticals are β-emitters, with 89Sr and 153Sm the most well studied.Citation37 Following injection of 89Sr, radiation doses are delivered to the osseous target lesions at low dose rates.Citation38 Between 16 weeks and 1 year, absorbed doses in the 20–40 Gy range are deposited as a steadily declining dose rate.Citation39,Citation40 Because of its higher dose rate and the shorter range (ie, tissue penetration), 153Sm may have an improved therapeutic index compared with that of 89Sr ().Citation38 Due to its relatively shorter half-life, repeated administration of 153Sm is feasible for persistent or recurrent bone pain provided adequate hematologic function returns; however, effects on bone marrow remain a limitation.Citation30 This suggests that an agent with less depth of tissue penetration but similar or higher biologic effect is needed to facilitate repeated dosing. One potential reason for difficulty demonstrating antitumor and survival benefits with β-emitters could be related to this dosing limitation.
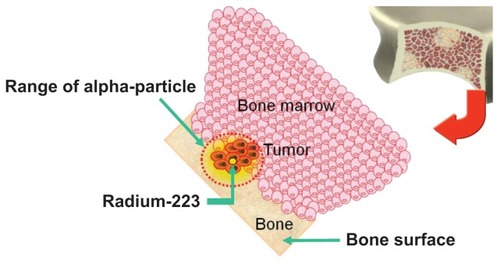
Cationic radium is a calcium mimetic (located in the same column of the periodic table as calcium), and as such naturally targets areas of bone turnover without the need for a carrier. (Recall that the bone stores 99% of the human body’s calcium and 85% of the phosphorous. Blood levels of calcium and bone resorption/formation are both tightly regulated by various hormones.Citation41) For example, Radium-224 (224Ra) has been used extensively for treatment of ankylosing spondylitis, a chronic inflammatory disease of the axial skeleton characterized by new bone formation.Citation42223Ra has a half-life of 11.4 days, produces four alpha particles from decay through short-lived daughter radionuclides, and has advantages over 224Ra in terms of the decay chain.Citation43223Ra was selected for biomedical applications based on its favorable decay chain and half-life.Citation43 In contrast to β-emitters, which have a low linear energy transfer (LET) and track lengths of up to several millimeters, α-emitters deliver a much more densely ionizing (high LET) radiation with an immense quantity of energy per track length and much shorter tissue penetration (<100 μm, or 2–10 cell diameters). The key physical differences in selected α- and β-emitters are summarized in , and the mechanism of action of 223Ra is summarized in . Because alpha-particle irradiation induces mostly double-stranded DNA breaks, cellular repair mechanisms may be less effective.Citation44 Lesions with clones of tumor cells remaining dormant in G0 of the cell cycle may be eradicated by high LET radiation from α-emitters.Citation38,Citation45 In addition, the limited penetration depth also results in lower radiation dose to the marrow and other adjacent normal tissues.
Figure 1 Mechanism of action for the targeting of osseous metastases by 223Ra. Reprinted with permission from Algeta ASA, from 2012 ASCO GU Symposium presentation.
Abbreviation:223Ra, radium-223.
Radiation safety precautions associated with 223Ra therapy are minimal. Following therapy with 223Ra, the risk of radiation exposure to others is very small, with the main recommendation being to maintain good hygiene. While 153Sm and 89Sr are excreted primarily by the kidneys, the major route of excretion of 223Ra is through the feces, with only a small fraction of renal excretion; this reduces the chances of contamination. The patient’s external radiation exposure to others is low enough to allow patients to be immediately released under 10 CFR 35.75 following 223Ra administration.
Preclinical studies of 223Ra demonstrated its potential to be bone marrow–sparing, with promising antitumor activity and favorable biodistribution. In mice, bone uptake of 223Ra compared with 89Sr was similar; however, estimates of dose to marrow cavities showed that 223Ra could be less toxic to bone marrow than β-emitters.Citation46 In a nude rat model of osseous metastases resistant to chemotherapy and biphosphonates, rats treated with 223Ra had superior symptom-free survival.Citation47 A biodistribution study in a dog with bone cancer injected with 223Ra showed elimination via intestinal clearance, with low activity in the intestinal wall that was similar to other soft tissues.Citation38 In addition, examination of these canine specimens using α-track microautoradiography demonstrated some concentration of the α-emitter on the surfaces of trabecular bone and a very high accumulation in the osteoblastic bone matrix.
Clinical evaluation of 223Ra
Phase I studies
Based on the promising preclinical results, a Phase I dose-escalation and safety study was conducted in 25 men and women with prostate (n = 15) and breast (n = 10) cancers (AT1-BC-1).Citation43 Five patients were treated with a single dose of 223Ra at each of the following dose levels and followed for 8 weeks: 46, 93, 163, 213, or 250 kBq/kg. Subjects were followed for 8 weeks. The patients were observed for dose-limiting toxicity (defined as platelets < 20 × 109/L or neutrophils < 0.5 × 109/L) and adverse events (AEs). In addition, the blood-clearance profile of 223Ra was evaluated at 10 minutes and at 1, 4, 24, and 48 hours and 7 days postinjection. Gamma camera scintigraphy was performed in six patients, using the 271 keV peak of the 219Rn daughter to indicate the position of its mother nuclide; this required long acquisition times due to the low number of events. Pain was assessed using the European Organization for Research and Treatment of Cancer QLQ-C 30 questionnaire at baseline, 1, 4, and 8 weeks.
Overall, 223Ra was well-tolerated, and no dose-limiting hematologic toxicity was observed.Citation43 Reversible myelosuppression was observed, with nadir counts occurring 2–4 weeks after administration of 223Ra. There was a trend towards increased myelosuppression at higher dose levels. Interestingly, there was more neutropenia than thrombocytopenia (in contrast to β-emitters, with which thrombocytopenia is often more frequent). There was no anemia above grade 2 or thrombocytopenia above grade 1 observed. Grade 3 leukopenia and neutropenia were only seen at the ≥163 kBq/kg doses in the same two patients, in addition to one isolated instance of leukopenia. The most common AEs were: transient diarrhea (40% of subjects); bone pain, including “flare” (36%); fatigue (25%); nausea (25%); and vomiting (25%). Whereas transient diarrhea was observed at all dose levels, nausea and vomiting occurred at the higher dose levels. AEs were generally mild, reversible, and manageable with supportive care (ie, antidiarrheal medication).
Blood radioactivity levels decreased from 12% of the initial at 10 minutes postinjection to 6% at 1 hour and <1% after 24 hours. By gamma scintigraphy, 223Ra appeared to accumulate in osteoblastic metastases, correlating well with conventional diagnostic 99mTc-MDP bone scans. Serum alkaline phosphatase decreased in both groups of patients, but was greatest in the patients with prostate cancer (−52.1 ± 14.8, mean ± standard deviation) and significantly different between the groups (P = 0.0028). The 16 patients with an elevated serum alkaline phosphatase at baseline (of which eleven had prostate cancer) had a particularly robust decline, which was significantly different than patients with normal-range alkaline phosphatase at baseline. Pain palliation was noted in more than half of the patients, with 52% reporting improvement at 1 week, 60% at 4 weeks, and 56% at 8 weeks. Of note, a “flare” response (transient increase in bone pain) was observed in about one-fifth of patients (seven of 25) during the first week of treatment. This was the first clinical trial of an α-emitter for treatment of cancer patients with osseous metastases.
Because of a very tolerable toxicity profile (including mild myelosuppression and gastrointestinal side effects), pharmaco-dynamic effects consistent with the hypothesized mechanism of action (decline in serum alkaline phosphatase and correlation of gamma scintigraphy with bone scans), and evidence of clinical benefit (improved pain scores compared with baseline in up to 60%), 223Ra was deemed to be promising for further study. Also of note, survival in this Phase I study was observed to be greater than 20 months (with >20 months’ follow-up), which compared favorably to a contemporary Scandinavian randomized trial with 89Sr in a similar population.Citation48 An additional Phase Ib study (BC1-05) of six patients with advanced prostate cancer demonstrated the feasibility of repeat dosing of 223Ra, but has only been reported in abstract form.Citation38,Citation49 Finally, a separate Phase Ib study (BC1-08) in men with progressive CRPC and two or more bone metastases on bone scan (n = 10) did not reach the maximum tolerated dose with escalation up to 200 kBq/kg and demonstrated targeting of osseous lesions, rapid blood clearance, and excretion through the small intestine followed by transit through the large intestine.Citation50
Phase II studies
Two randomized, multicenter Phase II studies in patients with mCRPC have been published. In the first double-blind, placebo-controlled study (BC1-02), patients were randomized to be given either four intravenous injections of 223Ra at 50 kBq/kg or placebo every 4 weeks.Citation51 In the second double-blind, dose-response study (BC1-04), patients were randomized to a single intravenous injection of 223Ra at 5, 25, 50, or 100 kBq/kg.Citation52
The first study (BC1-02) aimed to evaluate the effects of repeated 223Ra dosing in men with symptomatic CRPC.Citation51 Patients were required to have multiple osseous metastatic lesions or one painful lesion with two consecutive rising PSA values. In addition, all patients had bone pain requiring external-beam radiotherapy (EBRT) and either had bilateral orchiectomy or else were maintained on a luteinizing hormone-releasing hormone agonist during the study. Patients were randomized to receive either four consecutive monthly injections of 223Ra at 50 kBq/kg or saline. EBRT was given to the most painful bony lesion starting no later than 7 days after the first injection. The primary end points were the mean change in bone alkaline phosphatase (ALP) from baseline to 4 weeks after the last injection and time to occurrence of SREs. Secondary end points included evaluation of safety, serum markers of bone turnover, PSA, and overall survival.
Sixty-four patients were enrolled from eleven centers in Sweden, Norway, and the UK: 33 patients were randomized to EBRT with 223Ra and 31 patients to EBRT with placebo.Citation51 No difference in EBRT dose fractionation at baseline was observed between the groups. Hematological toxicity was minimal, with no thrombocytopenia observed in the 223Ra arm compared with one event in a placebo-arm patient. Grade ≥ 2 neutropenia occurred in three patients treated with 223Ra compared with none treated with placebo. No patient discontinued 223Ra because of treatment-emergent AEs, and there were more serious AEs in the placebo arm. The only statistically significant difference in AEs between the arms was constipation in twelve patients treated with 223Ra (mild– moderate in all but one case) versus two with placebo.
In addition to a tolerable safety profile, evidence of biologic effects and efficacy were demonstrated.Citation51 The median change in bone ALP from baseline to 4 weeks after the last study injection was −65.6% in the 223Ra group compared with 9.3% in the placebo group (P < 0.0001). Median time to first SRE was 14 weeks in the 223Ra arm versus 11 weeks in the placebo arm (P = 0.257), with a hazard ratio (HR) of 1.75 (95% confidence interval [CI], 0.96–3.19; P = 0.065) favoring 223Ra when adjusted for baseline covariates. The median relative change in PSA from baseline to 4 weeks after the last injection was −23.8% in the 223Ra group versus +44.9% in the placebo group (P = 0.003). Confirmed PSA responses by PSA Working Group criteriaCitation53 (≥50% decline) were observed in eleven of 31 (35%) patients on the 223Ra arm and five of 28 (18%) on the placebo arm (P = 0.153), with median time to PSA progression of 26 weeks and 8 weeks, respectively, on each arm (P = 0.048). Notably, censoring for concomitant treatments did not substantially change the overall results. The median overall survival was 65.3 weeks for the 223Ra group versus 46.4 weeks for placebo (P = 0.066), with an adjusted HR of 2.12 (95% CI, 1.13–3.98; P = 0.020) favoring 223Ra. These survival results have been updated and remain similar with longer follow-up.Citation54 Post hoc analyses showed OS of all patients to be 102.4 versus 42.6 weeks (P < 0.001) for posttreatment normalized versus nonnormalized from baseline ALP values, respectively; patients on the 223Ra arm had OS of 102.1 versus 42.5 weeks (P < 0.001) for posttreatment normalized versus nonnormalized from baseline ALP values, respectively.Citation55 In summary, this randomized, placebo-controlled study showed that repeat dosing of 223Ra every 4 weeks is well tolerated in men with mCRPC and has a significant effect on bone ALP 4 weeks after finishing treatment, in addition to potential beneficial efficacy in terms of SREs, PSA, and overall survival end points.
The second study (BC1-03), a double-blind, randomized, dose-ranging study, was designed to examine the effect of a single injection of 223Ra at 5, 25, 50, or 100 kBq/kg in patients with progressive mCRPC and pain.Citation52 Patients were required to have testosterone levels < 50 ng/dL after castration therapy, a score of ≥2 on the BPI,Citation56 progression of disease based on rising PSA levels, and sites of clinical pain correlating with multifocal osteoblastic disease on bone scintigraphy. The primary end point was the change in “pain index” (derived from a combination of the Visual Analogue Scale and analgesic consumption categorized according to the World Health Organization [WHO] analgesic ladderCitation57) at weeks 2, 4, 8, 12, and 16. Secondary end points included change from baseline in the BPI severity index and functional index, overall survival, duration of pain relief, relative change in bone ALP and PSA, and assessment of AEs.
One hundred patients were randomized and treated at 16 centers in Sweden, Germany, France, and the UK.Citation52 Over half of patients had >20 bone lesions or a superscan, 81% had performance status of 0–1, 36% had prior docetaxel, and 48% had a baseline WHO level of analgesia of 3; median baseline Visual Analogue Scale was 42 mm. A statistically significant dose response for pain index was observed at week 2 only (P = 0.035). At week 8, the percentage of pain responders was 40%, 63%, 56% and 71% on the 5, 25, 50, and 100 kBq/kg arms, respectively. The BPI data also showed a significant dose response at week 8 for the Pain Severity Index (P = 0.040). In a post hoc analysis of pain responders, pain decreased by a mean of −30, −31, −27, and −28 mm (P = 0.008, P = 0.0005, P = 0.002, and P < 0.0001). Furthermore, these responders showed an improvement in the BPI functional interference index in all groups. There were no differences in AEs among the dose groups, with the most frequent nonhematologic AEs being nausea, fatigue, vomiting, diarrhea, constipation, bone pain, urinary tract infection, and peripheral edema. In the two highest-dose groups, there appeared to be slightly greater reductions in platelet, leukocyte, and neutrophil counts. Nadir counts generally occurred at 2 weeks postinjection and subsequently returned to baseline. Changes in bone ALP were significant only in the 100-kBq/kg dose group at weeks 4 and 8 (P < 0.0001 and P = 0.0067, respectively), whereas PSA increased from baseline to week 16 in all dose groups. The median overall survival for the study population was 50 weeks and did not significantly differ among groups.
Overall, this study focusing on the pain-relieving effects of a single injection of 223Ra in escalating doses demonstrated an early dose response at week 2 and a maximum of 71% pain response at week 8 at the highest dose level. A well-tolerated safety profile was observed, although there were no effects on PSA levels and only a significant effect on bone ALP at the highest dose level. Notably, there may have been a problem with dropout bias, as 17 patients had dropped out by week 8 and there was differential dropout in the low- versus high-dose groups (eleven versus six patients).
A third randomized, double-blind dose-finding Phase II study of 223Ra (BC1-04) has only been reported in abstract form.Citation54,Citation57 Patients were randomized to 25, 50, or 80 kBq/kg every 6 weeks for 12 weeks (three total doses). The primary end point was PSA response (≥50% decline from baseline). Bone markers, SREs, AEs, and survival were also evaluated. Sixty-one percent of patients had an elevated ALP at baseline. In these patients, normalization of ALP was associated with a significantly better survival compared with those who did not have normalization of ALP.
Phase III study
The results of the international, randomized, double-blind Alpharadin in Symptomatic Prostate Cancer (ALSYMPCA) Phase III trial were recently presented.Citation35 Eligible patients had confirmed symptomatic CRPC, two or more bone metastases, no known visceral metastases, and were either docetaxel-pretreated or unfit for docetaxel. Patients were randomized 2:1 to either 223Ra injections at 50 kBq/kg with best standard of care or saline injections with best standard of care. Six injections were given at 4-week intervals. “Best supportive care” could include secondary hormonal therapies (antiandrogens, androgen biosynthesis inhibitors, steroids) or EBRT, but not cytotoxic chemotherapy or radioisotopes. Subjects were stratified according to total ALP, bisphosphonate use, and prior docetaxel treatment. The primary end point was overall survival, with secondary end points of time to first SRE, time to total ALP progression, total ALP response, total ALP normalization, time to PSA progression, safety, and quality of life. The trial was designed with 90% power to detect an HR of 0.76 with a two-sided alpha of 0.05. Data from a planned interim analysis after 314 events from 809 randomized patients were presented. The trial was stopped based on the recommendation of an independent data-monitoring committee, due to early evidence of benefit in terms of overall survival (predetermined boundary crossed).
From June 2008 through February 2011, the investigators randomized 541 patients to 223Ra and 268 patients to placebo (intention-to-treat group).Citation35 The baseline characteristics between the arms appeared well matched, with baseline Eastern Cooperative Oncology Group (ECOG) ≤1 in 86%, 6–20 metastases in 44%, and >20 metastases/superscan in 40%, and WHO ladder cancer pain index ≥ 2 in 54% on the 223Ra arm. About 58% had received prior docetaxel. Median total ALP was 213 μg/L, and PSA was 159 μg/L on the 223Ra arm. Median overall survival was significantly improved in the 223Ra group compared with placebo: 14.0 versus 11.2 months (HR 0.695 [95% CI, 0.552–0.875]; P = 0.00185). In addition, time to first SRE was significantly improved in the 223Ra arm: 13.6 versus 8.4 months (HR 0.610 [95% CI, 0.461–0.807]; P = 0.00046). Significant improvements in the biochemical end points of time to total ALP progression (HR 0.163 [95% CI, 0.121–0.221]; P < 0.00001), time to PSA progression (HR 0.671 [95% CI, 0.546–0.826]; P = 0.00015), total ALP response (43% vs 3%; P < 0.001), and total ALP normalization (33% vs 1%; P < 0.001) were also observed.
Overall, 223Ra appeared to be quite well tolerated. Notably, there were fewer AEs in the 223Ra group than the placebo group as measured by all-grade AEs (88% vs 94%), grade 3 or 4 AEs (51% vs 59%), serious AEs (43% vs 55%), and discontinuation due to AEs (13% vs 20%). The incidence of grade 3 or 4 neutropenia in the 223Ra group was 2% versus 1% in the placebo arm. Grade 3 or 4 thrombocytopenia was observed in 4% of subjects on the 223Ra arm versus 2% on the placebo arm. All-grade AEs and grade 3 or 4 anemia were similar between arms. In terms of all-grade nonhematologic AEs, diarrhea (22% vs 13%) and vomiting (17% vs 13%) appeared to be more frequent in the 223Ra group, whereas nausea (34% vs 32%) and constipation (18% vs 18%) appeared similar between groups.
Subgroup analysis demonstrated survival benefits across most clinically important patient subgroups, regardless of current use of bisphophonates, prior use of docetaxel, or ECOG performance status.Citation35 One interesting result was that the HR appeared better in patients currently using bisphosphonates compared with those not on bisphosphonates. There is some biologic rationale for this effect, since the mechanism of action for bisphosphonates is inhibition of osteoclast activity.Citation59 In theory, this decreased osteoclastic activity could result in 223Ra having increased effect at sites of osteoblastic activity, due to longer binding times.Citation35 It remains to be seen whether this effect would also be seen with denosumab, a monoclonal antibody against RANKL, but one might expect similar results. It would also be interesting to evaluate 223Ra with agents known to elicit osteoblastic responses on bone scan, such as abiraterone acetate.Citation60
More detailed results of the impact of 223Ra on SREs were presented recently as well.Citation61 In contrast to other trials of bone-targeted agents,Citation16 no skeletal surveys were routinely performed during the ALSYMPCA trial; all imaging was performed only as clinically indicated.Citation35 SRE components included pathologic bone fracture, spinal cord compression, EBRT, and surgical intervention. In addition to delaying time to first SRE (as mentioned above), 223Ra significantly delayed time to all SRE components except surgical intervention.Citation61 EBRT was the most common SRE component: 23% vs 27% for the 223Ra and placebo arms, respectively (HR 0.65 [95% CI, 0.48–0.87]; P = 0.0038). Pathologic bone fracture was observed in 4% vs 7%, respectively (HR 0.45 [95% CI, 0.24–0.86]; P = 0.013). Of particular interest, spinal cord compression occurred in 3% of patients on the 223Ra arm compared with 6% on placebo (HR 0.44 [95% CI, 0.22–0.88]; P = 0.016). Although not common, this dreaded complication results in significant morbidity in men with advanced prostate cancer.Citation62 This is the first study to demonstrate a significant effect on delay of spinal cord compression in this population.
At the time of this writing, no quality-of-life or pain-response data from the ALSYMPCA trial have been reported. Ideally, a therapy that prolongs OS and delays SREs, besides having biochemical effects, should do so with minimal compromise of quality of life and with improvements in pain. These results are eagerly awaited in order to confirm the benefit of 223Ra in terms of patient-reported outcomes.
Critical appraisal and potential role of 223Ra in therapy of mCRPC
The pivotal Phase III randomized double-blind placebo controlled ALSYMPCA trial of 223Ra demonstrated a highly significant OS improvement in docetaxel-pretreated or docetaxel-unfit men with symptomatic bone-metastatic CRPC and a very tolerable side-effect profile. A large number of men in the US with mCRPC are unfit for systemic chemotherapy due to toxicity concerns or comorbidities, and many men with mCRPC decline chemotherapy and all eventually fail first-line docetaxel. 223Ra is pending regulatory approval in the US and abroad; however, based on recent FDA approvals in mCRPC based on overall survival benefits,Citation5,Citation12–Citation14 approval of 223Ra appears likely. Although time to first SRE was not the primary end point of the ALSYMPCA trial, the effects of 223Ra on delaying SREs are important, and this end point has led to the regulatory approval of other bone-targeted agents even in the absence of beneficial effects on overall survival and disease progression.Citation15,Citation16 Based on eligibility criteria from this pivotal trial, it is likely that the label will be broad, encompassing both men with symptomatic bone-metastatic CRPC who have failed docetaxel and those who are not candidates for docetaxel chemotherapy.
The population of the ALSYMPCA trial was defined somewhat differently compared with prior trials in mCRPC. Because docetaxel/prednisone was the first therapy proven to extend survival in men with mCRPC and therefore became the first-line standard of care, many contemporary trials have focused on either “pre-docetaxel” or “post-docetaxel” populations. More recent trials have also focused on “asymptomatic or minimally symptomatic” patients (eg, IMPACT,Citation12 COU-AA-302,Citation63 PREVAILCitation64). However, this is the first Phase III study of a survival-prolonging therapy to concentrate on the symptomatic, bone-metastatic subpopulation of mCRPC patients. Therefore, 223Ra represents a unique treatment option in this subgroup. 223Ra occupies a unique niche in that it prolongs OS, is a bone-targeted agent that delays SREs, and is also a radiopharmaceutical that might be expected to provide pain palliation (Phase III data not yet reported).
223Ra has not been compared head-to-head against other approved therapies in mCRPC. However, with this caveat and based on what is known from the fairly extensive study of 223Ra in this population to date, the following observations can be made.
Efficacy of 223Ra
A large and significant improvement in OS was observed when compared with placebo in men with mCRPC and symptomatic bony metastases. The concurrent demonstration of benefit in terms of delayed SREs and improvement in all biochemical end points (ie, PSA, total ALP), which would be expected with a therapy of 223Ra’s mechanism of action, adds to the robustness of this finding.
Subgroup analysis demonstrates that OS improvement was consistent across multiple clinically relevant subgroups. Importantly, these benefits were seen in prespecified groups (strata), including total ALP < 220 U/L and ≥220 U/L; current bisphosphonate use (yes/no); or prior use of docetaxel (yes/no).
The population of patients in the ALSYMPCA trial included both docetaxel-unfit and docetaxel-pretreated men. This makes cross-trial comparisons more difficult, since eligibility criteria for trials in mCRPC have historically focused on either chemonaive or chemo-pretreated populations. Men who are unfit for docetaxel-based chemotherapy may have a poorer survival relative to those who are chemotherapy candidates.Citation65
The reason for the choice of treatment with six total injections (or until progression of disease) is not clear, and could be an area for future study.
Overall survival ():
○ Cytotoxic chemotherapy: The absolute median OS difference of 2.8 months observed on the ALSYMPCA trial compares favorably with the 2.9-month difference seen in the chemonaive (but docetaxel-fit) population in the TAX-327 studyCitation66 and the 2.4-month difference in the docetaxel-pretreated population in the TROPIC study.Citation13 However, it should be noted that both of these latter two trials used an active comparator (mitoxantrone plus prednisoneCitation10).
○ AR-directed therapies: Trials with androgen receptor (AR)-directed therapies, such as abirateroneCitation14 and MDV3100,Citation17 in docetaxel-pretreated populations have demonstrated median OS differences of 4.6 and 4.8 months, respectively. Notably, these trials used the less active comparator of placebo plus prednisone. However, there is a strong rationale for combining these agents with 223Ra based on the allowance of these classes of agents in the ALSYMPCA trial and the nonoverlapping toxicity profiles. Therefore, evaluation of combination versus sequential therapy with these agents should be encouraged.
○ Radiopharmaceuticals: None of the currently FDA-approved radiopharmaceuticals (eg, 89Sr, 153Sm) have demonstrated an OS benefit in a randomized Phase III study in men with mCRPC.Citation11
○ Antiresorptive agents: None of the currently FDA-approved osteoclast inhibitors (eg, zoledronic acid, denosumab) have demonstrated OS benefits over placebo. However, their use with 223Ra is likely to be beneficial without overlapping toxicity based on the Phase III evidence to date.
Skeletal-related events ():
○ Cytotoxic chemotherapy: There is insufficient evidence to demonstrate that docetaxel and cabazitaxel prevent or delay SREs, although they are known to result in pain palliation and to prolong time to pain progression, disease progression, and overall survival.
○ AR-directed therapies: Abiraterone has demonstrated delay in time to first SRE (25th percentile, 301 vs 150 days; P < 0.0001) in the COU-AA-301 trial.Citation20 Time to first SRE was a secondary end point in the AFFIRM trial of MDV3100 (NCT00974311), but this result has not yet been reported.Citation17
○ Radiopharmaceuticals: There is insufficient evidence to demonstrate that 89Sr or 153Sm prevent or delay SREs.Citation11
○ Antiresorptive agents: Zoledronic acid delays SREs compared with placebo, and denosumab is superior to zoledronic acid in delaying SREs in men with mCRPC. Notably, subgroup analysis of the ALSYMPCA trial suggested that bisphosphonates may potentiate the activity of 223Ra; a similar effect would be expected with denosumab, though there is a lack of data regarding this.
Pain palliation was demonstrated in Phase III trials of docetaxel and abiraterone, but not cabazitaxel (). A key indication for the use of radioisotopes for men with mCRPC has been pain palliation, although there is likely only a small benefit in complete reduction of pain over 1–6 months and no increase in analgesic use ().Citation11 Data on pain palliation from the 223Ra Phase III ALSYMPCA trial have not been reported; however, the Phase I and II experience with 223Ra would suggest a benefit in terms of pain palliation.
Safety and toxicity profile
The most common nonhematologic side effects of 223Ra in the ALSYMPCA trial include diarrhea, nausea, vomiting, and constipation. Notably, nausea and constipation did not appear to be more frequent on the 223Ra arm versus placebo. Two percent or fewer of these nonhematologic, gastrointestinal side effects were grade 3 or 4. Overall, only about 10% of patients on the 223Ra arm had grade ≥ 3 AEs, fewer than on the placebo arm.
Neutropenia and thrombocytopenia are side effects of 223Ra and occurred overall in 4% and 8%, respectively, of patients in the ALSYMPCA trial. Grade 3 or 4 neutropenia and thrombocytopenia were observed in 2% and 4%, respectively.
In contrast with other radioisotopes, 223Ra appears to have much less myelosuppression. This property allows consecutive doses to be administered safely, and may be the basis for its more substantial antitumor effects and OS compared with β-emitters. Additionally, with 223Ra, neutropenia predominates over thrombocytopenia, which is the inverse of the pattern seen with β-emitters.
Judged against cytotoxic chemotherapies, 223Ra is likely to have a significantly better toxicity profile in terms of myelosuppression and gastrointestinal and other side effects. In an extreme example, in the TROPIC trial of cabazitaxel, grade 3 or 4 diarrhea was observed in 6.2% and grade 3 or 4 neutropenia in 81.7% (febrile neutropenia 7.5%).
In comparison to AR-directed therapies, 223Ra has a distinct toxicity profile but may be similarly tolerable. Patients treated with abiraterone acetate have demonstrated side effects related to mineralocorticoid excess due to the drug’s mechanism of action, such as fluid retention, hypertension, and hypokalemia.Citation14 The most common side effect overall and grade 3 or 4 side effect observed with MDV3100 was fatigue, with patients rarely experiencing seizures (0.6%; all grade ≥ 3).Citation17
Antiresorptive agents are likely to be used in combination with 223Ra, as in the Phase III trial, and side effects generally appear to be nonoverlapping.
Data on quality of life with 223Ra from the ALSYMPCA trial are eagerly awaited.
In comparison to β-emitters, which are renally excreted, 223Ra is eliminated via the small intestine. This could be an important advantage in patients with mCRPC.
Long-term safety data with 223Ra are lacking. However, there is extensive experience with 224Ra in patients with ankylosing spondylitis.Citation42 An increased risk for later cancers has been observed, but only in individuals treated with 224Ra as children and, importantly, not in those treated as adults.Citation67 In comparison, there have been reports of acute leukemia with 89Sr but not 153Sm.Citation68
Future directions
Emerging therapies aimed at preventing skeletal morbidity in men with prostate cancer have recently been reviewed in detail.Citation69 Notable bone-targeted therapies in clinical development for mCRPC include SRC-targeted therapies (dasatinib), and MET-targeted therapies. While the oral endothelin (ETA) receptor antagonists atrasentan and zibotentan (ZD4054) were not successful in Phase III trials when combined with docetaxel in mCRPC, it is possible that these agents may combine favorably with other bone-targeted strategies. The oral SRC tyrosine kinase inhibitor dasatinib (Sprycel; Bristol- Myers Squibb, New York, NY) is being evaluated in a Phase III mCRPC trial of docetaxel/prednisone with dasatinib or placebo (NCT00744497),Citation70 with results anticipated in 2012. Finally, the multitargeted tyrosine kinase inhibitor XL-184 (cabozantinib), which inhibits MET, VEFGR2, RET, and Kit, has shown impressive results in a Phase II studyCitation71 and will enter Phase III testing soon.Citation72,Citation73
Table 4 Skeletal-related event (SRE) delay in recent Phase III trials of bone-targeted therapies in bone-metastatic mCRPC
Table 5 Radiopharmaceuticals in selected randomized trials in men with prostate cancer
Beta emitters have been combined with chemotherapy in several studies, including two randomized studies, demonstrating the possible feasibility and safety of this approach.Citation31–Citation34 For example, one recent Phase I study by Morris et al demonstrated that docetaxel and 153Sm could be administered at full doses over repeated cycles.Citation31 Given the improved toxicity profile with 223Ra over β-emitters, it seems likely that 223Ra could be combined with chemotherapy as well. This concept is currently being investigated in a Phase I/II trial of 223Ra with docetaxel chemotherapy in men with bone metastasis from CRPC (NCT01106352).Citation74 As a synergistic interaction between androgen-deprivation therapy and radiotherapy that increases apoptosis is known to exist in prostate cancer,Citation75 it is conceivable that this synergy could exist between 223Ra and the newer AR-directed therapies (eg, abiraterone, MDV3100) as well. Finally, it is possible that 223Ra and bone-targeted agents in development could have complementary mechanisms of action. All of these remain important research questions that should be addressed in the near future.
Conclusion
The overall risk-to-benefit ratio of 223Ra appears quite favorable. The available data demonstrate that 223Ra has activity in men with symptomatic bone-metastatic CRPC who are either docetaxel-unfit or docetaxel-pretreated. The significant improvement in median OS is an acceptable surrogate of clinical benefit, and is bolstered by delay of SREs and improvement in biochemical end points. These benefits are in the range observed with other approved therapies in this setting. When examined in the context of 223Ra-associated toxicity, these benefits appear well worth the risk in the subpopulation of patients included in the ALSYMPCA trial. Side effects were mild and predominantly gastrointestinal (diarrhea and vomiting). Myelosuppression was minimal, with rare grade ≥ 3 neutropenia and thrombocytopenia. Toxicities appear to be less than those with cytotoxic chemotherapies and are similarly mild, though distinct, when compared to AR-directed therapies. Significantly less myelosuppression is observed with 223Ra compared with β-emitters. The effects of 223Ra on quality of life and pain palliation from the randomized Phase III trial have not been reported. In clinical practice, it is likely that 223Ra would be used in conjunction with antiresorptive agents. Compared with approved cytotoxic chemotherapies, AR-directed therapies, and other radioisotopes, 223Ra could occupy a unique niche in the treatment of mCRPC.
Disclosure
Consultant or advisory roles: Michael R Harrison, Exelixis; Andrew J Armstrong, Sanofi, Bayer, Dendreon, Amgen, Medivation, Janssen, Active Biotech, Bristol-Myers Squibb; Daniel J George, Astellas, Aveo, Bayer, Dendreon, Exelixis, Genentech, Medivation, Novartis, Pfizer, Sanofi, Viamet. Honoraria (speaking): Andrew J Armstrong, Sanofi, Dendreon, Amgen; Daniel J George, Amgen, Dendreon, Novartis, Pfizer, Sanofi. Research funding: Michael R Harrison, Exelixis; Andrew J Armstrong, Sanofi-Aventis, Dendreon, Medivation, Janssen, Active Biotech, Imclone/Eli Lilly, Novartis, Bristol-Myers Squibb; Daniel J George, Exelixis, Genentech, GSK, Millennium, Novartis, Pfizer. Terence Z Wong reports no conflicts of interest in this work.
References
- SiegelRNaishadhamDJemalACancer statistics, 2012CA Cancer J Clin2012621102922237781
- JossonSMatsuokaYChungLWZhauHEWangRTumor-stroma co-evolution in prostate cancer progression and metastasisSemin Cell Dev Biol2010211263219948237
- ArmstrongAJMarengoMSOlteanSCirculating tumor cells from patients with advanced prostate and breast cancer display both epithelial and mesenchymal markersMol Cancer Res201198997100721665936
- PetrylakDPTangenCMHussainMHDocetaxel and estramustine compared with mitoxantrone and prednisone for advanced refractory prostate cancerN Engl J Med2004351151513152015470214
- TannockIFde WitRBerryWRDocetaxel plus prednisone or mitoxantrone plus prednisone for advanced prostate cancerN Engl J Med2004351151502151215470213
- ArmstrongAJGarrett-MayerESYangYCde WitRTannockIFEisenbergerMA contemporary prognostic nomogram for men with hormone-refractory metastatic prostate cancer: a TAX327 study analysisClin Cancer Res200713216396640317975152
- ArmstrongAJGarrett-MayerEOu YangYCProstate-specific antigen and pain surrogacy analysis in metastatic hormone-refractory prostate cancerJ Clin Oncol200725253965397017761981
- ArmstrongAJGarrett-MayerEde WitRTannockIEisenbergerMPrediction of survival following first-line chemotherapy in men with castration-resistant metastatic prostate cancerClin Cancer Res201016120321120008841
- HalabiSVogelzangNJKornblithABPain predicts overall survival in men with metastatic castration-refractory prostate cancerJ Clin Oncol200826152544254918487572
- TannockIFOsobaDStocklerMRChemotherapy with mitoxantrone plus prednisone or prednisone alone for symptomatic hormone-resistant prostate cancer: a Canadian randomized trial with palliative end pointsJ Clin Oncol1996146175617648656243
- RoqueIFMMartinez-ZapataMJScott-BrownMAlonso-CoelloPRadioisotopes for metastatic bone painCochrane Database Syst Rev20117CD00334721735393
- KantoffPWHiganoCSShoreNDSipuleucel-T immunotherapy for castration-resistant prostate cancerN Engl J Med2010363541142220818862
- de BonoJSOudardSOzgurogluMPrednisone plus cabazitaxel or mitoxantrone for metastatic castration-resistant prostate cancer progressing after docetaxel treatment: a randomised open-label trialLancet201037697471147115420888992
- de BonoJSLogothetisCJMolinaAAbiraterone and increased survival in metastatic prostate cancerN Engl J Med2011364211995200521612468
- SaadFGleasonDMMurrayRA randomized, placebo-controlled trial of zoledronic acid in patients with hormone-refractory metastatic prostate carcinomaJ Natl Cancer Inst200294191458146812359855
- FizaziKCarducciMSmithMDenosumab versus zoledronic acid for treatment of bone metastases in men with castration-resistant prostate cancer: a randomised, double-blind studyLancet2011377976881382221353695
- ScherHIFizaziKSaadFEffect of MDV3100, an androgen receptor signaling inhibitor (ARSI), on overall survival in patients with prostate cancer postdocetaxel: Results from the phase III AFFIRM studyJ Clin Oncol201230Suppl 5 Abstr LBA1
- de BonoJFizaziKSaadFPrimary, secondary, and quality-of-life endpoint results from the phase III AFFIRM study of MDV3100, an androgen receptor signaling inhibitorJ Clin Oncol201230Suppl Abstr 4519
- Enzalutamide (XTANDI Capsules) [webpage on the Internet]Silver Spring, MDUS Food and Drug Administration2012 [updated September 4, 2012]. Available from: http://www.fda.gov/Drugs/InformationOnDrugs/ApprovedDrugs/ucm317997.htmAccessed December 12, 2012
- LogothetisCDe BonoJSMolinaAEffect of abiraterone acetate (AA) on pain control and skeletal-related events (SRE) in patients (pts) with metastatic castration-resistant prostate cancer (mCRPC) post docetaxel (D): Results from the COU-AA-301 phase III studyJ Clin Oncol201129Suppl Abstr 4520
- SaadFGleasonDMMurrayRLong-term efficacy of zoledronic acid for the prevention of skeletal complications in patients with metastatic hormone-refractory prostate cancerJ Natl Cancer Inst2004961187988215173273
- AdamADixonAKAllisonDJGraingerRGGrainger and Allison’s Diagnostic Radiology: a Textbook of Medical Imaging5th edEdinburghChurchill Livingstone2008
- LewingtonVJMcEwanAJAckeryDMA prospective, randomised double-blind crossover study to examine the efficacy of strontium-89 in pain palliation in patients with advanced prostate cancer metastatic to boneEur J Cancer19912789549581716935
- BuchaliKCorrensHJSchuererMSchnorrDLipsHSydowKResults of a double blind study of 89-strontium therapy of skeletal metastases of prostatic carcinomaEur J Nucl Med1988147–83493512460352
- PorterATMcEwanAJPoweJEResults of a randomized phase-III trial to evaluate the efficacy of strontium-89 adjuvant to local field external beam irradiation in the management of endocrine resistant metastatic prostate cancerInt J Radiat Oncol Biol Phys19932558058138478230
- QuiltyPMKirkDBolgerJJA comparison of the palliative effects of strontium-89 and external beam radiotherapy in metastatic prostate cancerRadiother Oncol199431133407518932
- OosterhofGORobertsJTde ReijkeTMStrontium(89) chloride versus palliative local field radiotherapy in patients with hormonal escaped prostate cancer: a phase III study of the European Organisation for Research and Treatment of Cancer, Genitourinary GroupEur Urol200344551952614572748
- SerafiniANHoustonSJRescheIPalliation of pain associated with metastatic bone cancer using samarium-153 lexidronam: a double-blind placebo-controlled clinical trialJ Clin Oncol1998164157415819552068
- SartorOReidRHHoskinPJSamarium-153-Lexidronam complex for treatment of painful bone metastases in hormone-refractory prostate cancerUrology200463594094515134985
- SartorOReidRHBushnellDLQuickDPEllPJSafety and efficacy of repeat administration of samarium Sm-153 lexidronam to patients with metastatic bone painCancer2007109363764317167764
- MorrisMJPandit-TaskarNCarrasquilloJPhase I study of samarium-153 lexidronam with docetaxel in castration-resistant metastatic prostate cancerJ Clin Oncol200927152436244219364960
- TuSMMillikanREMengistuBBone-targeted therapy for advanced androgen-independent carcinoma of the prostate: a randomised phase II trialLancet2001357925333634111210994
- SciutoRFestaAReaSEffects of low-dose cisplatin on 89Sr therapy for painful bone metastases from prostate cancer: a randomized clinical trialJ Nucl Med2002431798611801708
- FizaziKBeuzebocPLumbrosoJPhase II trial of consolidation docetaxel and samarium-153 in patients with bone metastases from castration-resistant prostate cancerJ Clin Oncol200927152429243519364971
- ParkerCHeinrichDO’SullivanJMOverall survival benefit and safety profile of radium-223 chloride, a first-in-class alpha- pharmaceutical: results from a phase III randomized trial (ALSYMPCA) in patients with castration-resistant prostate cancer (CRPC) with bone metastasesJ Clin Oncol201230Suppl 5 Abstr 8
- BayerRadium-223 Chloride (Alpharadin) in Castration-Resistant (Hormone-Refractory) Prostate Cancer Patients with Bone MetastasesClinicalTrialsgov [website on the Internet]Bethesda, MDUS National Library of Medicine2012 [updated September 20, 2012]. Available from: http://clinicaltrials.gov/show/NCT01516762. NLM identifier: NCT01516762Accessed November 1, 2012
- PerezCAPrinciples and Practice of Radiation Oncology4th edPhiladelphiaLippincott Williams & Wilkins2004
- BrulandØSNilssonSFisherDRLarsenRHHigh-linear energy transfer irradiation targeted to skeletal metastases by the alpha-emitter 223Ra: adjuvant or alternative to conventional modalities?Clin Cancer Res20061220 Pt 26250s6257s17062709
- BlakeGMGrayJMZivanovicMAMcEwanAJFlemingJSAckeryDMStrontium-89 radionuclide therapy: a dosimetric study using impulse response function analysisBr J Radiol1987607156856923620827
- BreenSLPoweJEPorterATDose estimation in strontium-89 radiotherapy of metastatic prostatic carcinomaJ Nucl Med1992337131613231613572
- ASBMR educational materials [webpage on the Internet]Bone curriculum Available from: http://depts.washington.edu/bonebio/ASBMRed/ASBMRed.htmlAmerican Society of Bone and Mineral Research [updated 2008]Accessed July 26, 2012
- TiepoltCGruningTFrankeWGRenaissance of 224 Ra for the treatment of ankylosing spondylitis: clinical experiencesNucl Med Commun2002231616611748439
- NilssonSLarsenRHFossaSDFirst clinical experience with alpha-emitting radium-223 in the treatment of skeletal metastasesClin Cancer Res200511124451445915958630
- RitterMACleaverJETobiasCAHigh-LET radiations induce a large proportion of non-rejoining DNA breaksNature19772665603653655859634
- HallEJGiacciaAJRadiobiology for the Radiologist6th edPhiladelphiaLippincott Williams & Wilkins2006
- HenriksenGFisherDRRoeskeJCBrulandOSLarsenRHTargeting of osseous sites with alpha-emitting 223Ra: comparison with the beta-emitter 89Sr in miceJ Nucl Med200344225225912571218
- HenriksenGBreistolKBrulandOSFodstadOLarsenRHSignificant antitumor effect from bone-seeking, alpha-particle-emitting (223)Ra demonstrated in an experimental skeletal metastases modelCancer Res200262113120312512036923
- SmelandSEriksteinBAasMSkovlundEHessSLFossaSDRole of strontium-89 as adjuvant to palliative external beam radiotherapy is questionable: results of a double-blind randomized studyInt J Radiat Oncol Biol Phys20035651397140412873686
- NilssonSBalteskardLFossaSDPhase I study of Alpharadin2 (223Ra), and a-emitting bone-seeking agent in cancer patients with skeletal metastasesEurJ Nucl Med Mol Imaging200431S2S290 Abstract 370
- CarrasquilloJADonoghueJAOPandit-TaskarNPhase I pharmacokinetic (PK) and biodistribution study of radium-223 chloride in patients with castration resistant prostate cancer (CRPC) metastatic to boneJ Clin Oncol20102815s Abstr 4680
- NilssonSFranzenLParkerCBone-targeted radium-223 in symptomatic, hormone-refractory prostate cancer: a randomised, multicentre, placebo-controlled phase II studyLancet Oncol20078758759417544845
- NilssonSStrangPAksnesAKA randomized, dose-response, multicenter phase II study of radium-223 chloride for the palliation of painful bone metastases in patients with castration-resistant prostate cancerEur J Cancer201248567868622341993
- BubleyGJCarducciMDahutWEligibility and response guidelines for phase II clinical trials in androgen-independent prostate cancer: recommendations from the Prostate-Specific Antigen Working GroupJ Clin Oncol199917113461346710550143
- NilssonSFranzénLParkerCAlpha-emitting radium-223: Two years follow up from a randomized phase II study in patients with bone metastases from hormone refractory prostate cancerEur J Cancer Suppl20097411 Abstract P-7018
- NilssonSO’Bryan-TearCGBolstadBLoknaAParkerCAlkaline phosphatase (ALP) normalization and overall survival in patients with bone metastases from castration-resistant prostate cancer (CRPC) treated with Radium-223 (Alpharadin™)J Clin Oncol201129Suppl Abstr 4620
- CleelandCSRyanKMPain assessment: global use of the Brief Pain InventoryAnn Acad Med Singapore19942321291388080219
- Palliative Care: Symptom Management and End-of-Life CareGenevaWorld Health Organization2004 Available from: http://www.who.int/3by5/publications/documents/en/genericpalliativecare082004.pdf. Accessed
- AlgetaASAA Dose Finding Study of Radium-223 for Prostate Cancer Patients with Bone MetastasesClinicalTrialsgov [website on the Internet]Bethesda, MDUS National Library of Medicine2012 [updated September 8, 2010]. Available from: http://clinicaltrials.gov/ct2/show/NCT00337155. NLM identifier: NCT00337155Accessed November 1, 2012
- FleischHBisphosphonates: mechanisms of actionEndocr Rev1998191801009494781
- RyanCJShahSEfstathiouEPhase II study of abiraterone acetate in chemotherapy-naive metastatic castration-resistant prostate cancer displaying bone flare discordant with serologic responseClin Cancer Res201117144854486121632851
- SartorAOHeinrichDHelleSIRadium-223 chloride impact on skeletal-related events in patients with castration-resistant prostate cancer (CRPC) with bone metastases: A phase III randomized trial (ALSYMPCA)J Clin Oncol201230Suppl 5 Abstr 9
- LoblawAMiteraGMalignant extradural spinal cord compression in men with prostate cancerCurr Opin Support Palliat Care20115320621021725245
- RyanCJSmithMRDe BonoJSInterim analysis (IA) results of COU-AA-302, a randomized, phase III study of abiraterone acetate (AA) in chemotherapy-naive patients (pts) with metastatic castration-resistant prostate cancer (mCRPC)J Clin Oncol201230Suppl Abstr LBA4518
- Medivation IncA Safety and Efficacy Study of Oral MDV3100 in Chemotherapy-Naive Patients with Progressive Metastatic Prostate Cancer (PREVAIL)ClinicalTrialsgov [website on the Internet]Bethesda, MDUS National Library of Medicine2012 [updated October 11, 2012]. Available from: http://clinicaltrials.gov/show/NCT01212991. NLM identifier: NCT01212991Accessed November 1, 2012
- ItalianoAOrtholanCOudardSDocetaxel-based chemotherapy in elderly patients (age 75 and older) with castration-resistant prostate cancerEur Urol20095561368137518706755
- BertholdDRPondGRSobanFde WitREisenbergerMTannockIFDocetaxel plus prednisone or mitoxantrone plus prednisone for advanced prostate cancer: updated survival in the TAX 327 studyJ Clin Oncol200826224224518182665
- NekollaEAKellererAMKuse-IsingschulteMEderESpiessHMalignancies in patients treated with high doses of radium-224Radiat Res1999152Suppl 6S3S710564925
- KossmanSEWeissMAAcute myelogenous leukemia after exposure to strontium-89 for the treatment of adenocarcinoma of the prostateCancer200088362062410649256
- SaylorPJLeeRJSmithMREmerging therapies to prevent skeletal morbidity in men with prostate cancerJ Clin Oncol201129273705371421860001
- Bristol-Myers SquibbRandomized Study Comparing Docetaxel Plus Dasatinib to Docetaxel Plus Placebo in Castration-Resistant Prostate Cancer (READY)ClinicalTrialsgov [website on the Internet]Bethesda, MDUS National Library of Medicine2012 [updated October 5, 2012]. Available from: http://clinicaltrials.gov/ct2/show/NCT00744497. NLM identifier: NCT00744497Accessed November 1, 2012
- HussainMSmithMRSweeneyCCabozantinib (XL184) in metastatic castration-resistant prostate cancer (mCRPC): Results from a phase II randomized discontinuation trialJ Clin Oncol201129Suppl Abstr 4516
- Exelixis Study of Cabozantinib (XL184) Versus Prednisone in Men with Metastatic Castration-resistant Prostate Cancer Previously Treated with Docetaxel and Abiraterone or MDV3100 (COMET-1)ClinicalTrials gov [website on the Internet]Bethesda, MDUS National Library of Medicine2012 [updated October 2, 2012]. Available from: http://clinicaltrials.gov/ct2/show/NCT01605227. NLM identifier: NCT01605227Accessed November 1, 2012
- Exelixis Study of Cabozantinib (XL184) Versus Mitoxantrone Plus Prednisone in Men with Previously Treated Symptomatic Castration-resistant Prostate Cancer (COMET-2)ClinicalTrialsgov [website on the Internet]Bethesda, MDUS National Library of Medicine2012 [updated October 11, 2012]. Available from: http://clinicaltrials.gov/ct2/show/NCT01522443. NLM identifier: NCT01522443Accessed November 1, 2012
- AlgetaASAA Study of Alpharadin® with Docetaxel in Patients with Bone Metastasis From Castration-Resistant Prostate Cancer (CRPC)ClinicalTrialsgov [website on the Internet]Bethesda, MDUS National Library of Medicine2012 [updated May 11, 2012]. Available from: http://clinicaltrials.gov/ct2/show/NCT01106352. NLM identifier: NCT01106352Accessed November 1, 2012
- DeWeeseTLSongDYCurrent evidence for the role of combined androgen suppression and radiation in the treatment of adenocarcinoma of the prostateUrology200055216917410688072
- Quadramet® (samarium Sm 153 lexidronam injection) [prescribing information]Langhorne, PAEUSA Pharma (USA) Inc2009
- Metastron™ (strontium-89 chloride injection) [prescribing information]Arlington Heights, ILGE Healthcare2006