
Abstract
Background
Breast-conserving surgery plus postoperative radiotherapy is the standard surgical treatment mode for early breast cancer. Currently, there are no clear predictive indicators to determine whether a patient can choose breast-conserving surgery, which mainly depends on the surgeon’s clinical experience and subjective judgment. Cone-beam breast computed tomography (CBBCT) reconstructs the breast 3D image from three mutually perpendicular angles, helping surgeons to locate and accurately measure the volume of the tumor, mammary gland, and breast. We used CBBCT to retrospectively measure the tumor-to-gland volume ratio and tumor-to-breast volume ratio in breast cancer cases. Then, we analyzed the correlation between the surgical methods and ratios in breast cancer patients.
Methods
We collected 100 patients undergoing breast-conserving surgery as the study group, and 100 patients undergoing mastectomy as the control group. All patients chose the surgical approach after comprehensive consideration of examination results and assessment of patient condition. Patients underwent CBBCT examination before surgery. We retrospectively measured the volume of tumor, mammary glands and breast, then calculated tumor-to-gland and tumor-to-breast volume ratios.
Results
Tumor volume and the ratios of the two groups statistically differed (P < 0.001), while the mammary gland and breast volume did not (P > 0.05). The average tumor-to-gland volume ratio was 4.32% in the study group and 10.74% in the control group, and the average tumor-to-breast volume ratio was 0.74% in the study group and 1.36% in the control group. In breast-conserving surgery, the 95% reference range of tumor-to-gland ratio is (0, 12.90%), and the 95% reference range of tumor-to-breast ratio is (0, 2.17%).
Conclusion
The tumor-to-gland volume ratio and tumor-to-breast volume ratio measured using CBBCT are correlated with the choice of surgical methods (breast-conserving surgery or mastectomy) for breast cancer patients. This can be used as possible predictor of breast-conserving surgery to help surgeons.
Introduction
In recent decades, the surgical approach toward breast cancer has continuously been developing. Based on medical evidence, we found that for patients with early breast cancer, the survival rate after breast-conserving surgery combined with postoperative radiotherapy is equal to or greater than that of patients undergoing mastectomy.Citation1–Citation4 Both international guidelines and Chinese guidelines suggest that an appropriate tumor-to-breast volume ratio is one of the guidelines for breast-conserving surgery.Citation5 However, there is no clear indication to help surgeons accurately calculate the volume ratio, and to define the appropriate volume ratio range. Therefore, whether a patient can choose breast-conserving surgery mainly relies on the surgeon’s clinical experience and subjective judgment, and lacks a clear predictive index.
Cone-beam breast computed tomography (CBBCT) is a new high-resolution three-dimensional breast computed tomography (CT) imaging technique.Citation6,Citation7 Compared with traditional breast imaging techniques including mammography and MRI, CBBCT has many advantages. CBBCT is a 3D imaging technique with low radiation dose and simple operation. CBBCT can clearly distinguish cancer and benign calcifications, is less susceptible to breast density interference, and has higher sensitivity and specificity than do traditional breast imaging techniques.Citation6,Citation8 It is precisely because CBBCT is a form of 3D stereo imaging that it can visually display tumor location, and help to accurately measure the volume of tumors, glands, and breasts.
Therefore, we wondered whether it is possible to measure tumor-to-gland and tumor-to-breast volume ratios by CBBCT, and predict whether the patient would be suitable for breast-conserving surgery. We collected data from patients with breast cancer who underwent CBBCT before surgery, and measured the tumor-to-gland volume ratio and tumor-to-breast volume ratio by CBBCT. We then assessed whether the ratios were related to the type of surgery the patient accepted. Using this approach, we hoped to identify the best volume ratio range measured by CBBCT as a predictive index for breast-conserving surgery to help breast surgeons make better clinical decisions.
Materials and Methods
Patients and Methods
We retrospectively collected the data of 200 patients with breast cancer who underwent CBBCT examination before operation in our hospital from July 2019 to November 2020. The study group included 100 patients who underwent breast-conserving surgery and the control group included 100 patients who underwent mastectomy. In the study group, 47 patients underwent conventional breast conserving surgery, 40 patients underwent breast-conserving surgery with volume displacement technique (including round block technique, batwing mastopexy, tennis racket technique, and parallelogram mastopexy lumpectomy), and 13 patients received breast-conserving surgery with volume replacement technique (use latissimus dorsi flaps). In the control group, 88 patients underwent simple mastectomy accompanied with sentinel lymph node biopsy and 12 patients underwent modified radical mastectomy.
Inclusion criteria were: a) female; b) diagnosed with operable primary breast cancer; c) patient accepted CBBCT before surgery; d) maximum tumor diameter < 5 cm; and e) breast cancer neoplasm stage 0 and IIIA according to the American Joint Committee on Cancer classification (2017)Citation9 and no metastasis.
Exclusion criteria were: a) being pregnant; b) inflammatory breast cancer; c) Paget’s disease; d) patient underwent neoadjuvant chemotherapy; e) incomplete or technically suboptimal CBBCT examination; f) multicentric tumors; and g) if the decision of mastectomy was based on the patient’s request with no other medical indications.
The age of study group was 32–78 years, with an average age of 51.05 (± 8.29) years. The control group was between 31–72 years old, with an average age of 52.54 (± 9.27) years.
This study was performed with the approval of the Ethics Committee of Guangxi Medical University Cancer Hospital and in accordance with the provisions of the Helsinki Declaration. All participants provided written informed consent. A total of 200 BC medical records were collected.
Imaging Protocol
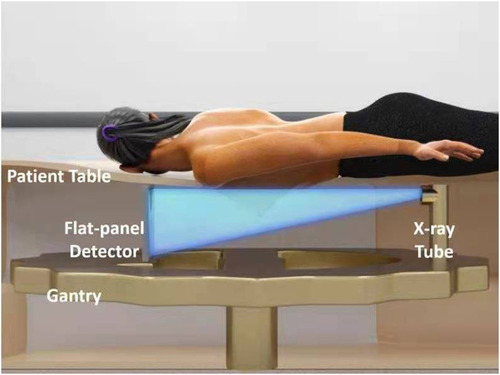
CBBCT uses the KBCT-1000 imaging system produced by Corning (Tianjin) Medical Equipment Co., Ltd. CBBCT collects 397 mm X 298 mm images at a rate of 30 frames per second and a resolution of 1024×768. During the examination, the patient takes the prone position, and the breast naturally droops through a hole in the center of the examination. The X-ray tube and detector scan around the breast to obtain a two-dimensional breast projection image, which reconstructs the three-dimensional image and uploads it to the image processing system and work station (). The quantity of reconstructed images is related to the length of the breast. Under the standard reconstruction mode (0.273 mm3), the maximum breast length that can be reconstructed in a single scan is 16cm. The reconstructed image is isotropic, and the layer thickness is consistent in all directions.
Figure 1 The patient is in the prone position, and the breasts naturally sag through the hole in the center of table. The X-ray tube and detector scan a circle around the breast to obtain a two-dimensional breast projection image. From this a three-dimensional image is reconstructed and uploaded to the image processing system and workstation.
The equipment has passed the US Food and Drug Administration (FDA), China’s State Food and Drug Administration (cFDA), and EU CE certification.
The breast volume is measured semi-automatically. At a work station, imaging doctors use the CBBCT console system to mark the range of tumor, gland, and breast, and the volume is automatically calculated by software. Both doctors were blinded to clinicopathologic and other imaging modality findings. In this study, two senior imaging doctors measured the tumor, gland, and breast volume of the study group and the control group, compared the measured data and calculated the tumor-to-gland volume ratio and tumor-to-breast volume ratio. If the data measured differed they re-measured and discussed the measurements to reach a consensus.
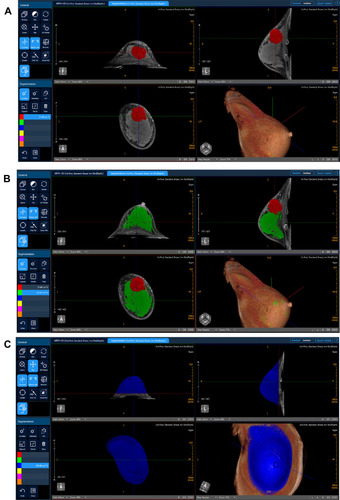
A 49 years old patient underwent breast-conserving surgery () and a 38 years old patient underwent mastectomy (). There are four reconstructed breast images in each figure, which show transverse, sagittal, coronal, and 3D views separately.
Figure 2 This patient, female, 49 years old, with invasive carcinoma of the right breast, underwent breast-conserving surgery. There are four reconstructed breast images in each figures, which show transverse, sagittal, coronal, and 3D views separately. (A) Red mark represents tumor. Tumor volume is 3.25 cm3. (B) Green mark represents gland, and its volume is 92.17 cm3. Tumor-to-gland volume ratio is 3.53%. (C) Blue mark is right breast and its volume is 445.05 cm3. Tumor-to-breast volume ratio is 0.73%.
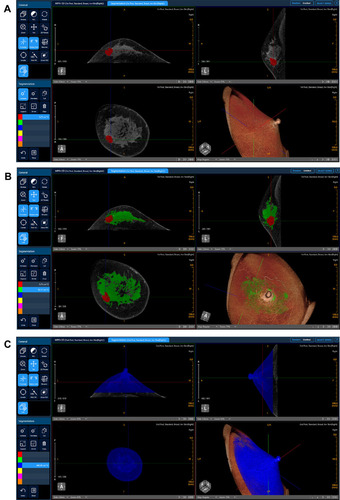
Figure 3 This patient, female, 38 years old, with invasive carcinoma of the right breast, underwent mastectomy. There are four reconstructed breast images in each figures, which show transverse, sagittal, coronal, and 3D views separately. (A) Red mark is tumor and its volume is 21.48 cm3. (B) Green mark is gland and its volume is 132.47 cm3. Tumor-to-gland volume ratio is 16.21%. (C) Blue mark is right breast and its volume is 425.80 cm3. Tumor-to-breast volume ratio is 5.04%.
Statistical Analysis
Statistical analyses were performed using SPSS version 24.0 (IBM, International Business Machines Corp.). The Shapiro–Wilk test was used to determine the data distribution normality. Normally or non-normally distributed data were reported as mean ± standard deviation (SD) or median and interquartile range (IQR), respectively. The Chi-Square test was used to compare age and pathological type. Tumor, gland, and breast volumes, and tumor-to-gland and tumor-to-breast volume ratios were compared between the two groups using the Wilcoxon rank sum test. We set the value for statistical significance at P < 0.05.
Results
A total of 200 patients with breast cancer were included in this study. Characteristics of the patients, including pathological type of tumors and ages, are shown in . The most common pathological type of breast cancer found was invasive ductal carcinoma. The surgical method chosen by the patient was not related to age or (x2 = 6.21, P = 0.184) or pathological type (x2 = 1.73, P = 0.63).
Table 1 Patient Characteristics
The average tumor volume was 2.48 cm3 (range 0.29–11.83 cm3) in the study group and 4.54 cm3 (range 0.79–17.38 cm3) in the control group, and there was statistically significant difference between them (P < 0.001) (). The average gland volume was 73.16 cm3 (range 14.21–250.58 cm3) in the study group and 55.54 cm3 (range 12.21–195.05 cm3) in the control group (P>0.05). The average breast volume was 385.69 cm3 (range 110.28–958.58 cm3) in the study group and 377.04 cm3 (range 64.13–991.30 cm3) in the control group (P > 0.05). The tumor-to-gland volume ratio range was 0.31%~18.95% in the study group and 1.52%~52.70% in the control group, and the tumor-to-breast volume ratio was 0.08%~2.95% in the study group and 0.27%~7.13% in the control group.
Table 2 Assessment of the Differences Between Average Volumes and Ratios (Average Tumor, Gland, Breast Volumes and Tumor-to-Gland Volume Ratio, Tumor-to-Breast Volume Ratio) Between the Two Groups
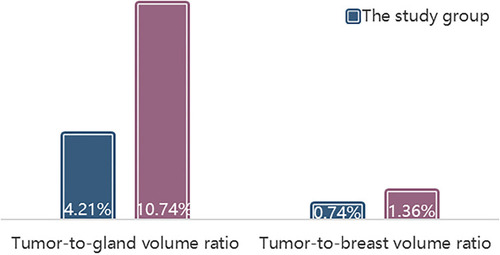
The average tumor-to-gland volume ratio of 10.74% in the control group was significantly higher than that of 4.32% in the study group (P < 0.001), and the average tumor-to-breast volume ratio of 1.36% in the control group was significantly higher than of 0.74% in the study group (P < 0.001) (). Based on the above data, the 95% reference range for the tumor-to-gland ratio of breast-conserving surgery is (0, 12.90%), the 95% reference range for the tumor-to-breast ratio of mastectomy is (0, 2.17%).
Figure 4 Comparison of average tumor-to-gland and tumor-to-breast volume ratios in the two groups.
Discussion
Worldwide, breast cancer is the most common cancer in women and the main cause of cancer death.Citation10 Early stage patients with breast cancer generally adopt standard treatment methods of breast-conserving surgery (BCS) supplemented by postoperative radiotherapy. According to the American Society of Breast Surgeons Performance and Practice Guideline, current indications for BCS are: a biopsy-proven diagnosis of DCIS or invasive breast cancer clinically assessed as resectable with clear margins and with an acceptable cosmetic result. Current contraindications for BCS include multicentric tumor involving two or more quadrants of the breast, diffuse malignant/indeterminate microcalcifications, inflammatory breast cancer, and persistently positive margins of excision. Patients with these situations are recommended to undergo mastectomy.
The breast is a female secondary sexual characteristic that has an important influence on women’s quality of life, self-esteem, and self-confidence. Compared with BCS, the mental state and quality of life of patients with breast cancer who undergo mastectomy are often troubled by their physical appearance.Citation11–Citation14 Before BCS was determined by the NIH (National Institutes of Health) consensus as the standard treatment mode for early breast cancer, patients with early stage breast cancer usually accepted mastectomy. Recently, the results of a randomized controlled trials comparing the efficacy of BCS and mastectomy have shown that BCS and mastectomy have the same survival rate in patients with early breast cancer.Citation1–Citation4 Since then, BCS combined with postoperative radiotherapy has become the internationally recognized first-choice treatment for early breast cancer.
At present, mammography is a clinically recognized and effective breast cancer screening method, but compared with MRI, mammography sensitivity is relatively low and it is easily affected by breast density. However, while MRI improves the diagnostic sensitivity, it also increases the false positive rate of diagnosis. Therefore, the routine use of MRI before BCS remains controversial.Citation15 Compared with ultrasound, CBBCT can eliminate operator subjectivity. Compared with MRI, CBBCT can improve patient comfort, has a short acquisition time, and can better distinguish tumors and calcifications. Owing to the true 3D display, CBBCT can avoid tissue overlap and reduce the false positive rate and radiation dose while improving sensitivity.Citation16–Citation21 Clinically, the choice of surgery for breast cancer patients mainly depends on the surgeon’s analysis of the patient’s specific conditions, which is subjective and sometimes leads to unnecessary mastectomy. CBBCT can make up for this defect. CBBCT dynamically displays cancer through 3D imaging. With the support of software, tumor, gland, and breast volume (cm3) can be accurately measured. Then, doctors can compute the tumor-to-gland and tumor-to-breast volume ratios to provide BCS predictors and help clinicians to make clinical decision. Compared with MRI, CBBCT does not need to use complex calculation methods such as threshold segmentation, and the two ratios can be accurately measured through software, which has more clinical promotion value.Citation22 Moreover, preoperative CBBCT can assess the extent of breast cancer infiltration, helping surgeons to determine the scope of surgery required to achieve negative margins, so as to better conserve breasts and achieve the best cosmetic results.Citation23,Citation24
In this study, we calculated that the 95% medical reference range of the tumor-to-gland ratio for BCS is (0, 12.90%), and the 95% medical reference range of the tumor-to-breast ratio is (0, 2.17%). This means that patients with tumor-to-gland ratios < 12.90%, or tumor-to-breast ratios < 2.17% should consider BCS, and that patients outside of this range should consider mastectomy. In the medical records we have collected, the tumor-to-gland and tumor-to-breast volume ratios of some patients undergoing mastectomy were within this range. However, after comprehensively considering the patient’s TNM staging, breast cancer pathological type, tumor location (quadrants), and tumor-to-nipple distance, these patients underwent mastectomy. Therefore, the tumor-to-gland and tumor-to-breast volume ratios should be used as a clinical reference index, not an absolute standard, to guide the choice of surgery type.
Numerous studies have shown that preoperative measurement of tumor-to-gland and tumor-to-breast volume ratios can provide more accurate clinical data (such as prognosticate HER2 statusCitation25) to help surgeons make surgical decisions, improve the surgical success rate, and preserve breasts for patients to achieve better cosmetic results.Citation26–Citation29 In this study, we performed CBBCT examinations on patients before surgery, measured accurate tumor, gland, and breast volumes, and computed the tumor-to-gland and tumor-to-breast volume ratios. These two ratios can be used as predictors of BCS to guide the selection of surgery type, facilitate discussion, overcome subjective considerations based on rough estimations of breast size, and to provide clinicians with quantifiable reference indicators. Moreover, the two ratios provide a readily intelligible parameter to help patients’ to understand surgical planning and predict postoperative cosmetic effects. The most recent guidelines issued by the European Society of Medical Oncology also pointed out that clinicians should consider tumor size in relation to breast size, when thinking about BCS, mastectomy, or tumor plastic surgery.Citation30
However, our study did have certain limitations. This is a retrospective analysis study that was limited by the short time for the introduction of equipment and the small cohort we collected. It is necessary to continue to collect records for further verification of our results. Additionally, CBBCT examination is relatively expensive, and some patients cannot afford it. Furthermore, measurement of the patient’s tumor, gland, and breast volume are semi-automated, and required imaging doctors to measure each at a workstation. This is time-consuming and cannot be routinely used in clinical practice. Through communication with software engineers, this problem is expected to be resolved by software upgrades and the addition of automatic measurement functions.
In summary, using the tumor-to-gland and tumor-to-breast volume ratios measured by CBBCT as a predictor of BCS can help surgeons to determine the most appropriate surgery type for different patients with breast cancer.
Disclosure
The authors report no conflicts of interest in this work.
Acknowledgments
This work was supported by the National Key R&D Program of China (grants 2017YFC0112600, and 2017YFC0112603) and Guangxi Clinical Research Center for Medical Imaging Construction (Grant No. Guike AD20238096).
References
- van Maaren MC, de Munck L, de Bock GH, et al. 10 year survival after breast-conserving surgery plus radiotherapy compared with mastectomy in early breast cancer in the Netherlands: a population-based study. Lancet Oncol. 2016;17(8):1158–1170. doi:10.1016/S1470-2045(16)30067-527344114
- Veronesi U, Cascinelli N, Mariani L, et al. Twenty-year follow-up of a randomized study comparing breast-conserving surgery with radical mastectomy for early breast cancer. N Engl J Med. 2002;347(16):1227–1232. doi:10.1056/NEJMoa02098912393819
- Litière S, Werutsky G, Fentiman IS, et al. Breast conserving therapy versus mastectomy for stage I-II breast cancer: 20 year follow-up of the EORTC 10801 Phase 3 randomised trial. Lancet Oncol. 2012;13(4):412–419. doi:10.1016/S1470-2045(12)70042-622373563
- Hartmann-Johnsen OJ, Kåresen R, Schlichting E, et al. Survival is better after breast conserving therapy than mastectomy for early stage breast cancer: a registry-based follow-up Study of Norwegian Women Primary Operated Between 1998 and 2008. Ann Surg Oncol. 2015;22(12):3836–3845. doi:10.1245/s10434-015-4441-325743325
- Chinese Anti-Cancer Association CoBCS. Guidelines and standards for the diagnosis and treatment of breast cancer by the Chinese Anti-Cancer Association (2019 Edition). Chin Oncol. 2019;29(08):609–680.
- Wienbeck S, Lotz J, Fischer U. Review of clinical studies and first clinical experiences with a commercially available cone-beam breast CT in Europe. Clin Imaging. 2017;42:50–59. doi:10.1016/j.clinimag.2016.11.01127875762
- Shi L, Vedantham S, Karellas A, et al. Library based x-ray scatter correction for dedicated cone beam breast CT. Med Phys. 2016;43(8):4529. doi:10.1118/1.495512127487870
- Rößler AC, Kalender W, Kolditz D, et al. Performance of photon-counting breast computed tomography, digital mammography, and digital breast tomosynthesis in evaluating breast specimens. Acad Radiol. 2017;24(2):184–190. doi:10.1016/j.acra.2016.09.01727888024
- Giuliano AE, Connolly JL, Edge SB, et al. Breast cancer-major changes in the American joint committee on cancer eighth edition cancer staging manual. CA Cancer J Clin. 2017;67(4):290–303. doi:10.3322/caac.2139328294295
- Bray F, Ferlay J, Soerjomataram I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. doi:10.3322/caac.2149230207593
- Chen CL, Liao MN, Chen SC, et al. Body image and its predictors in breast cancer patients receiving surgery. Cancer Nurs. 2012;35(5):E10–16. doi:10.1097/NCC.0b013e3182336f8b22067694
- Metcalfe KA, Semple J, Quan ML, et al. Changes in psychosocial functioning 1 year after mastectomy alone, delayed breast reconstruction, or immediate breast reconstruction. Ann Surg Oncol. 2012;19(1):233–241. doi:10.1245/s10434-011-1828-721674270
- Dunn LB, Cooper BA, Neuhaus J, et al. Identification of distinct depressive symptom trajectories in women following surgery for breast cancer. Health Psychol. 2011;30(6):683–692. doi:10.1037/a002436621728421
- Rosenberg SM, Dominici LS, Gelber S, et al. Association of breast cancer surgery with quality of life and psychosocial well-being in young breast cancer survivors. JAMA Surg. 2020;155(11):1035–1042. doi:10.1001/jamasurg.2020.332532936216
- Pilewskie M, Olcese C, Eaton A, et al. Perioperative breast MRI is not associated with lower locoregional recurrence rates in DCIS patients treated with or without radiation. Ann Surg Oncol. 2014;21(5):1552–1560. doi:10.1245/s10434-013-3424-524385207
- Korhonen KE, Conant EF, Cohen EA, et al. Breast cancer conspicuity on simultaneously acquired digital mammographic images versus digital breast tomosynthesis images. Radiology. 2019;292(1):69–76. doi:10.1148/radiol.201918202731084481
- O’Connell A, Conover DL, Zhang Y, et al. Cone-beam CT for breast imaging: radiation dose, breast coverage, and image quality. AJR Am J Roentgenol. 2010;195(2):496–509. doi:10.2214/AJR.08.101720651210
- Wienbeck S, Fischer U, Luftner-Nagel S, et al. Contrast-enhanced cone-beam breast-CT (CBBCT): clinical performance compared to mammography and MRI. Eur Radiol. 2018;28(9):3731–3741. doi:10.1007/s00330-018-5376-429594402
- O’Connell AM, Kawakyu-O’Connor D. Dedicated cone-beam breast computed tomography and diagnostic mammography: comparison of radiation dose, patient comfort, and qualitative review of imaging findings in BI-RADS 4 and 5 lesions. J Clin Imaging Sci. 2012;2:7. doi:10.4103/2156-7514.9327422439131
- Xu M, Cheng X, Cheng X, et al. Areas of breast tissue covered in cone beam breast CT imaging. Exp Ther Med. 2017;13(3):913–916. doi:10.3892/etm.2017.409228450919
- O’Connell AM, Karellas A, Vedantham S, et al. Newer technologies in breast cancer imaging: dedicated cone-beam breast computed tomography. Semin Ultrasound CT MR. 2018;39(1):106–113. doi:10.1053/j.sult.2017.09.00129317032
- Cozzi A, Schiaffino S, Della Pepa G, et al. MRI-derived tumour-to-breast volume is associated with the extent of breast surgery. Diagnostics (Basel). 2021;11(2).
- Yue M, Y Z, Liu A, et al. The accuracy of tumor size evaluation on invasive breast cancer based on cone beam breast CT. Chin J Radiol. 2019;(04):286–291.
- Chagpar AB, Butler M, Killelea BK, et al. Does three-dimensional intraoperative specimen imaging reduce the need for re-excision in breast cancer patients? A prospective cohort study. Am J Surg. 2015;210(5):886–890. doi:10.1016/j.amjsurg.2015.05.01826255230
- Zhu Y, Zhang Y, Ma Y, et al. Cone-beam breast CT features associated with HER2/neu overexpression in patients with primary breast cancer. Eur Radiol. 2020;30(5):2731–2739. doi:10.1007/s00330-019-06587-w31900700
- Lagendijk M, Vos EL, Koning AHJ, et al. TUmor-volume to breast-volume RAtio for improving COSmetic results in breast cancer patients (TURACOS); a randomized controlled trial. BMC Cancer. 2017;17(1):336. doi:10.1186/s12885-017-3280-y28514945
- Faermann R, Sperber F, Schneebaum S, et al. Tumor-to-breast volume ratio as measured on MRI: a possible predictor of breast-conserving surgery versus mastectomy. Isr Med Assoc J. 2014;16(2):101–105.24645229
- Vos EL, Koning AH, Obdeijn IM, et al. Preoperative prediction of cosmetic results in breast conserving surgery. J Surg Oncol. 2015;111(2):178–184. doi:10.1002/jso.2378225332158
- Pukancsik D, Kelemen P, Újhelyi M, et al. Objective decision making between conventional and oncoplastic breast-conserving surgery or mastectomy: an aesthetic and functional prospective cohort study. Eur J Surg Oncol. 2017;43(2):303–310. doi:10.1016/j.ejso.2016.11.01028069398
- Cardoso F, Kyriakides S, Ohno S, et al. Early breast cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up†. Ann Oncol. 2019;30(8):1194–1220.31161190