
Abstract
Purpose
Minimally invasive surgery (MIS) is performed frequently in early-stage ovarian cancer patients, especially in ovarian clear cell carcinoma (OCCC). The aim of this study was to investigate whether primary laparoscopic surgery influences prognosis in patients with early-stage OCCC.
Patients and Methods
Patients with International Federation of Gynecology and Obstetrics (FIGO) stage I OCCC were retrospectively reviewed in two hospitals between April 2010 and August 2020. Clinical data were abstracted, and patients were followed up until February 2021. Patients were divided into open surgery (laparotomy) and laparoscopy groups, and the Kaplan–Meier method was applied to compare progression-free survival (PFS) and overall survival (OS) between the groups. Statistical differences were determined by the Log rank test.
Results
Eighty-nine patients were included in the study; 20 (22.5%) and 69 (77.5%) patients underwent laparoscopic and open surgery, respectively. The patients’ characteristics were well-balanced except that patients in the laparoscopy group tended to have smaller tumors and lower frequency of omentectomy and lymphadenectomy compared with the open surgery group. The median follow-up duration was 42.6 and 36.5 months in the laparoscopy and open surgery groups, respectively. Nine (10.1%) patients developed recurrence, and 4 (4.5%) died of the disease; all in the open surgery group. The estimated 2-year PFS rates were 100.0% and 90.1%, and the estimated 5-year OS rates were 100.0% and 91.9% in the laparoscopy and open surgery groups, respectively. No significant survival differences were found between the groups.
Conclusion
Survival was not compromised when primary laparoscopic surgery was performed in early-stage OCCC patients. A well-designed randomized controlled trial is warranted.
Introduction
Epithelial ovarian cancer (EOC) is the most lethal gynecologic malignancy and ranks fifth in cancer deaths among women.Citation1 Ovarian clear cell cancer (OCCC), a subtype accounting for approximately 5–25% of all EOCs, is always diagnosed at an early stage and is confined to the ovary as a pelvic mass. Previous studies have shown that OCCC is relatively less aggressive in the early stageCitation2 but may develop chemo-resistance in the advanced stage, leading to a significantly poorer prognosis compared with high-grade serous ovarian cancer.Citation3,Citation4
With developments in minimally invasive techniques, especially the wide use of laparoscopy, more gynecologic oncologists are considering minimally invasive surgery (MIS) in select patients.Citation5 MIS was first applied to assess tumor burden and to evaluate the resectability of advanced-stage ovarian cancer.Citation6 Recent studies have investigated the feasibility of MIS for interval debulking surgery after neoadjuvant chemotherapyCitation7,Citation8 and for secondary cytoreductive surgery in appropriate recurrent ovarian cancer patients.Citation9–Citation12 Additionally, for patients with apparent early-stage ovarian cancer, MIS has been applied for full staging surgery.Citation13–Citation16 However, as the LACC trial suggested that MIS was associated with lower progression-free survival (PFS) and overall survival (OS) compared with laparotomy in early-stage cervical cancer,Citation17 gynecological oncologists began to pay attention to patients’ survival, which may be affected by MIS, especially in ovarian cancers. Furthermore, as OCCC is associated with endometriosis and because most OCCC patients are diagnosed in the early stage, MIS appears to be applied more frequently in this subtype of ovarian cancer.
Herein, we conducted a retrospective study involving consecutive International Federation of Gynecology and Obstetrics (FIGO) stage I OCCC patients. Each patient’s clinical characteristics, treatment, and prognosis data were carefully collected and analyzed. Specifically, we divided the patients into two groups, namely a laparoscopy group and an open surgery group, according to whether primary laparoscopic surgery was performed. We aimed to investigate whether MIS impacts the survival of patients with FIGO stage I OCCC, compared with open surgery.
Patients and Methods
Study Subjects
This was a two-center, retrospective, cohort study conducted in Fudan University Zhongshan Hospital and Zhejiang Cancer Hospital between April 2010 and August 2020. Data for patients who were pathologically confirmed as having OCCC were reviewed and collected. In this study, only patients diagnosed as FIGO stage I OCCC were included. This study was approved by the medical ethics committees of Fudan University Zhongshan Hospital and Zhejiang Cancer Hospital. The need for written informed consent was waived owing to the retrospective anonymized data collection. The private information of all enrolled patients was carefully protected, and the study was conducted in accordance with the guidelines of the Declaration of Helsinki.
Study Protocol
Medical records were abstracted to obtain the patients’ age at diagnosis, preoperative serum cancer antigen 125 (CA125) value, preoperative CA199 value, FIGO stage, type of surgery (open or laparoscopic), tumor size, tumor location, ascites volume, postoperative adjuvant chemotherapy, chemotherapy cycles, PFS, and OS. Patients were followed up every 3 months for the first 2 years, then every 6 months for the next 3 years, and annually, thereafter. The last follow-up date was February 2021.
Definitions
In our study, patients were divided into two groups, namely a laparoscopy group and a laparotomy (open surgery) group. The laparoscopy group was defined as undergoing primary laparoscopic surgery, including full laparoscopic staging surgery and conversion to open surgery. The laparotomy group was defined as undergoing open surgery directly. PFS was defined as the time from the primary surgery to the date of recurrence, and OS was calculated as the time from the primary surgery to the date of death.
Statistical Analysis
The SPSS software package for windows (version 19.0; IBM Corp., Armonk, NY, USA) was used for statistical analysis. Quantitative data were expressed as medians. The Kaplan–Meier method was used to compare survival between the two groups, and the statistical differences were determined by the Log rank test. A p-value < 0.05 was considered statistically significant.
Results
Baseline and Patients’ Characteristics
Eighty-nine patients diagnosed as FIGO stage I OCCC were included in this study. The median age was 51.0 years (range, 32–75 years); 37 (41.6%) patients were diagnosed as FIGO stage IA and 56.2% as stage IC. The median preoperative CA125 and CA199 values were 43.5 U/mL and 20.3 U/mL, respectively. Most (60.7%) patients had a tumor size > 80 mm, and 18.0% had an ascites volume of > 200 mL. Almost all patients (97.8%) had a unilateral tumor except for two cases. After primary staging surgery, 82 (92.1%) patients received platinum-based chemotherapy, and 74 (83.1%) patients received four or more cycles of chemotherapy, while six (6.7%) patients did not undergo chemotherapy.
Overall, 20 (22.4%) patients underwent primary laparoscopy as the primary staging surgery, and 69 (77.6%) patients underwent open surgery directly. As shown in , clinical characteristics, namely age at diagnosis, FIGO stage, preoperative CA125 and CA199 values, tumor location, ascites volume, and chemotherapy cycles were well-balanced between the two groups. Patients with large tumor size (> 8 cm) tended to undergo open surgery (p=0.003).
Table 1 Clinical Characteristics
Surgical Procedures
Surgical procedures for the entire cohort are summarized in . Overall, 80 (89.9%) patients underwent hysterectomy, and 9 (10.1%) patients underwent fertility-preserving surgery. There was no statistically significant difference in the rates of hysterectomy, salpingo-oophorectomy, peritoneal biopsy, and appendectomy. Omentectomy (75.0% versus 100.0%; p < 0.001) and lymphadenectomy (50.0% versus 81.2%; p = 0.009) were less frequent in the laparoscopy group versus the open surgery group, respectively. Of the 66 patients receiving lymphadenectomy, 19 (28.8%) and 3 (4.5%) patients underwent only pelvic or para-aortic lymphadenectomy, respectively, and 44 (66.7%) patients underwent systematic lymphadenectomy. Of the 20 patients who underwent laparoscopic surgery, 10 (50.0%) were converted to laparotomy immediately, and 2 (10.0%) underwent delayed open surgery staging.
Table 2 Surgical Procedures
Prognosis Between the Laparoscopy and Laparotomy Groups
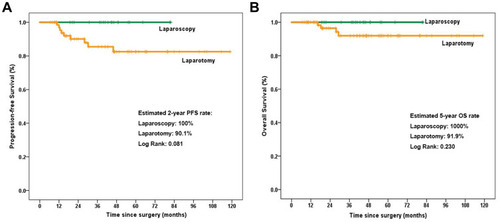
As of February 2021, the median follow-up duration for the entire cohort was 40.7 months (range, 6.6–108.9 months), and 42.6 months and 36.5 months in the laparoscopy and open surgery groups, respectively. Overall, 9 (10.1%) patients developed recurrence, and 4 (4.5%) died of the disease; all were in the open surgery group. As shown in , the estimated 2-year PFS rates were 100.0% and 90.1% in the laparoscopy and open surgery groups, respectively (p = 0.081). There was also no significant difference in OS, with an estimated 5-year OS rate of 100.0% and 91.9% in the laparoscopy and open surgery groups, respectively (p = 0.230) ().
Figure 1 Kaplan–Meier plots for progression-free survival (A) and overall survival (B) between the laparoscopy and laparotomy groups.
Characteristics of the Recurrent Patients
The clinical characteristics of the recurrent patients are listed in . In summary, 7/9 recurrent patients were diagnosed as FIGO stage IC, and 2 were FIGO stage IA. Eight patients received lymph node resection, and one patient did not. All patients underwent six or more cycles of chemotherapy, and the time to recurrence ranged from 10.7 to 45.9 months. Recurrent lesions were found in the pelvic and abdominal peritoneum in three patients, local pelvic recurrence developed in two patients, and retroperitoneal lymph node recurrence developed in two patients. One patient was diagnosed with recurrence according to the presence of ascites. These patients’ treatments and status are listed in .
Table 3 Characteristics of Recurrent Patients
Discussion
Although MIS is widely applied in gynecological surgery, including to diagnose endometriosis, the impact on endometriosis-associated ovarian cancer, including OCCC, which is frequently misdiagnosed as early-stage ovarian endometrioid cyst, remains uncertain. The potential risks of MIS in ovarian cancer may include the following: First, laparoscopy may fail to evaluate tumor disease because of severe dense adhesions, and occult tumor lesions, such as on the posterior surface of the diaphragm that are expected to be identified by palpation during open surgery, may be neglected during MIS.Citation18 Second, MIS may cause intraoperative cancer cell spillage, leading to peritoneal dissemination or port-site metastasis.Citation19–Citation21 Third, we still do not know if carbon dioxide (CO2) pneumoperitoneum changes the tumor environment or the biological behavior of tumor cells; thus, promoting tumor spread or metastasis.
We found no survival differences, when we reviewed previous studies comparing the survival of patients with early-stage ovarian cancer between laparoscopic and open surgery groups; however, the study designs or the included patients differed in the studies.Citation22–Citation28 As shown in , most previous studies included patients with early EOC, and only one study focused on stage IC OCCC patients.Citation25 In Chang et al’s study, 88 patients with stage IC OCCC were included, and 76 (86.4%) and 12 (13.6%) underwent direct exploratory laparotomy staging and laparoscopy, respectively.Citation25 All 12 patients who underwent laparoscopic staging were converted to open surgery after pathological confirmation, and no survival differences were identified between the groups. The authors’ concluded that a laparoscopic diagnosis did not worsen patients’ survival if direct open conversion was performed.
Table 4 References Comparing Survival Between Open Surgery and MIS for Ovarian Cancer Patients with Early Stage
Differing from Chang et al’s study, we included OCCC FIGO stage IA–IC patients and patients who received full laparoscopic staging as well as those who were converted to open surgery. Twenty of 89 patients underwent laparoscopic staging, and 12 (60.0%) were converted to laparoscopic surgery directly or underwent delayed open surgery staging. Our results revealed no tumor recurrence in the laparoscopy group after a median follow-up of 42.6 months. These data may indicate that laparoscopic surgery has no impact on survival in stage I OCCC patients, regardless of whether the surgery was converted to open surgery.
Recently, a large study with a median follow-up of 61 months (range, 13–118 months) investigated the role of MIS for early-stage ovarian cancer patients.Citation29 The authors concluded that grade 3 cancer was the most powerful prognostic factor for recurrence, whereas stage > IC was correlated with shorter PFS, but without reaching statistical significance. Tumor grade, final FIGO stage, and the time of surgical staging (immediate versus delayed) maintained an independent favorable prognostic role for PFS by multivariate analysis. In our study, we did not perform univariate or multivariate analysis for tumor recurrence because of the low recurrence number, and because the follow-up period was too short.
Importantly, we noticed that although no statistical significance was found in most previous studies, a shorter PFS or OS rate was observed in patients receiving direct open surgery staging in many recent studies.Citation25,Citation26 These data may be explained by different baseline characteristics, including preoperative imaging to determine large tumor size, which may lead to a choice of direct open surgery. However, no survival difference was identified between patients with tumor size ≤ 80 mm versus > 80 mm in our study (data not shown). A well-designed, randomized controlled trial should be conducted to resolve this question.
Conclusion
This was a retrospective study comparing survival between early-stage OCCC patients who underwent laparoscopy versus open surgery. Our study concluded that survival was not compromised when primary laparoscopic surgery was performed in FIGO stage I OCCC patients.
Disclosure
All authors report no conflicts of interest for this work.
References
- SiegelRL, MillerKD, JemalA. Cancer statistics, 2020. CA Cancer J Clin. 2020;70(1):7–30. doi:10.3322/caac.2159031912902
- CeppiL, GrassiT, GalliF, et al. Early-stage clear cell ovarian cancer compared to high-grade histological subtypes: an outcome exploratory analysis in two oncology centers. Gynecol Oncol. 2021;160(1):64–70.33077259
- KhaliqueS, LordCJ, BanerjeeS, et al. Translational genomics of ovarian clear cell carcinoma. Semin Cancer Biol. 2020;61:121–131. doi:10.1016/j.semcancer.2019.10.02531698086
- IidaY, OkamotoA, HollisRL, et al. Clear cell carcinoma of the ovary: a clinical and molecular perspective. Int J Gynecol Cancer. 2021;31(4):605–616. doi:10.1136/ijgc-2020-00165632948640
- FagottiA, PerelliF, PedoneL, et al. Current recommendations for minimally invasive surgical staging in ovarian cancer. Curr Treat Options Oncol. 2016;17(1):3. doi:10.1007/s11864-015-0379-826739150
- FagottiA, FerrandinaG, FanfaniF, et al. Prospective validation of a laparoscopic predictive model for optimal cytoreduction in advanced ovarian carcinoma. Am J Obstet Gynecol. 2008;199(6):642.e1–6. doi:10.1016/j.ajog.2008.06.052
- GueliAS, PetrilloM, VizzielliG, et al. Minimally invasive versus standard laparotomic interval debulking surgery in ovarian neoplasm: a single-institution retrospective case-control study. Gynecol Oncol. 2016;143(3):516–520. doi:10.1016/j.ygyno.2016.10.01727769526
- GueliAS, BottoniC, FanfaniF, et al. Minimally invasive interval debulking surgery in ovarian neoplasm (MISSION trial–NCT02324595): a feasibility study. Am J Obstet Gynecol. 2016;214(4):503.e1–503.e6. doi:10.1016/j.ajog.2015.10.922
- FagottiA, PetrilloM, CostantiniB, et al. Minimally invasive secondary cytoreduction plus HIPEC for recurrent ovarian cancer: a case series. Gynecol Oncol. 2014;132(2):303–306. doi:10.1016/j.ygyno.2013.12.02824378877
- FagottiA, CostantiniB, GallottaV, et al. Minimally invasive secondary cytoreduction plus HIPEC versus open surgery plus HIPEC in isolated relapse from ovarian cancer: a retrospective cohort study on perioperative outcomes. J Minim Invasive Gynecol. 2015;22(3):428–432. doi:10.1016/j.jmig.2014.11.00825461683
- GallottaV, GhezziF, VizzaE, et al. Laparoscopic management of ovarian cancer patients with localized carcinomatosis and lymph node metastases: results of a retrospective multi-institutional series. J Minim Invasive Gynecol. 2016;23(4):590–596. doi:10.1016/j.jmig.2016.01.02926872630
- GallottaV, NeroC, LodoliC, et al. Laparoscopic splenectomy for secondary cytoreduction in ovarian cancer patients with localized spleen recurrence: feasibility and technique. J Minim Invasive Gynecol. 2016;23(3):425–428. doi:10.1016/j.jmig.2016.01.00126776676
- GallottaV, GhezziF, VizzaE, et al. Laparoscopic staging of apparent early stage ovarian cancer: results of a large, retrospective, multi-institutional series. Gynecol Oncol. 2014;135(3):428–434. doi:10.1016/j.ygyno.2014.09.00625230214
- GhezziF, MalzoniM, VizzaE, et al. Laparoscopic staging of early ovarian cancer: results of a multi-institutional cohort study. Ann Surg Oncol. 2012;19(5):1589–1594. doi:10.1245/s10434-011-2138-922086443
- ZhangY, FanS, XiangY, et al. Comparison of the prognosis and recurrence of apparent early-stage ovarian tumors treated with laparoscopy and laparotomy: a meta-analysis of clinical studies. BMC Cancer. 2015;15(1):597. doi:10.1186/s12885-015-1604-326307038
- MelamedA, KeatingNL, ClemmerJT, et al. Laparoscopic staging for apparent stage I epithelial ovarian cancer. Am J Obstet Gynecol. 2017;216(1):50.e1–50.e12. doi:10.1016/j.ajog.2016.08.030
- RamirezPT, FrumovitzM, ParejaR, et al. Minimally invasive versus abdominal radical hysterectomy for cervical cancer. N Engl J Med. 2018;379(20):1895–1904. doi:10.1056/NEJMoa180639530380365
- WangP-H. The role of laparoscopy and the value of peritoneal carcinomatosis index in patients with intra-abdominal malignancies who are scheduled to laparotomy. Gynecol Minim Invasive Ther. 2019;8(2):51–52. doi:10.4103/GMIT.GMIT_93_1831143622
- TantitamitT, LeeC-L. Is it the time for laparoscopic management of early-stage ovarian malignancies?Gynecol Minim Invasive Ther. 2018;7(3):93–103. doi:10.4103/GMIT.GMIT_59_1830254949
- LeeCL, KayN. Inhibition of ovarian cancer growth and implantation by paclitaxel after laparoscopic surgery in a mouse model. Am J Obstet Gynecol. 2006;195:1278–1281. doi:10.1016/j.ajog.2006.07.03517014818
- LeeCL, KusunokiS, HuangCY, WuKY, LeePS, HuangKG. Surgical and survival outcomes of laparoscopic staging surgery for patients with stage I ovarian cancer. Taiwan J Obstet Gynecol. 2018;57:7–12. doi:10.1016/j.tjog.2017.12.00229458907
- GhezziF, CromiA, UccellaS, et al. Laparoscopy versus laparotomy for the surgical management of apparent early stage ovarian cancer. Gynecol Oncol. 2007;105(2):409–413. doi:10.1016/j.ygyno.2006.12.02517275077
- ParkJ-Y, KimD-Y, SuhD-S, et al. Comparison of laparoscopy and laparotomy in surgical staging of early-stage ovarian and fallopian tubal cancer. Ann Surg Oncol. 2008;15(7):2012–2019. doi:10.1245/s10434-008-9893-218437497
- DittoA, BoganiG, MartinelliF, et al. Minimally invasive surgical staging for ovarian carcinoma: a propensity-matched comparison with traditional open surgery. J Minim Invasive Gynecol. 2017;24(1):98–102. doi:10.1016/j.jmig.2016.09.01827702704
- ChangHT, ChiuML, WangTY, et al. Effect of chemotherapy, laparoscopy, and cytology on stage IC ovarian clear cell carcinoma: a Long-Term, Single-Center Study. Int J Environ Res Public Health. 2020;17(2):491.
- MerlierM, KerbageY, PieracheA, et al. Impact on prognosis of the surgical route, laparoscopy or laparotomy, for the surgical staging of early stage ovarian cancer—a study from the FRANCOGYN Group. J Clin Med. 2020;9(11):11. doi:10.3390/jcm9113528
- MinigL, SaadiJ, PatronoMG, et al. Laparoscopic surgical staging in women with early stage epithelial ovarian cancer performed by recently certified gynecologic oncologists. Eur J Obstet Gynecol Reprod Biol. 2016;201:94–100. doi:10.1016/j.ejogrb.2016.03.02927086268
- GallottaV, PetrilloM, ConteC, et al. Laparoscopic versus laparotomic surgical staging for early-stage ovarian cancer: a Case-Control Study. J Minim Invasive Gynecol. 2016;23:769–774. doi:10.1016/j.jmig.2016.03.00626995493
- GallottaV, JeongSY, ConteC, et al. Minimally invasive surgical staging for early stage ovarian cancer: a long-term follow up. Eur J Surg Oncol. 2021;47(7):1698–1704. doi:10.1016/j.ejso.2021.01.03333573854