
Abstract
Objective
Cancer is well known as the most important risk factor for the emergence of pulmonary embolism (PE). The incidence of incidental PE (IPE) has increased with widely use of multi-detector-row computed tomography (CT) technology. Simultaneously, more new cancer patients diagnosed concomitantly with IPE are found. No study has examined the presentation and prognosis of incidental pulmonary embolism (IPE) in gastric cancer patients. The aim of this study was to analyse prognostic factors in patients with advanced gastric cancer complicated with IPE.
Patients and Methods
Ninety patients with histologically confirmed advanced gastric adenocarcinoma diagnosed with IPE were enrolled. Continuous variables were compared using Student’s t-test or the Mann–Whitney U-test if non-normally distributed. The Chi-squared test (or Fisher’s exact test where appropriate) was used to compare categorical variables. The Kaplan–Meier method and the Log rank test were used for survival analysis. Independent prognostic factors for survival were determined using a Cox proportional hazards model. A two-sided P-value < 0.05 was considered statistically significant.
Results
Nineteen patients were diagnosed with IPE concomitantly with gastric cancer. Concurrence of gastric cancer and IPE, lack of anticoagulation therapy, and location of IPE were associated with survival. After adjusting for age and sex, the concurrence of gastric cancer and IPE, lack of anticoagulation, and central IPE independently influenced the survival of advanced gastric cancer patients with IPE. Subgroup analysis of patients with peripheral pulmonary embolisms confirmed that anticoagulant therapy provided a survival benefit.
Conclusion
Concurrence of gastric cancer and IPE may be a prognostic factor for advanced gastric cancer patients with IPE.
Introduction
Pulmonary embolism (PE) is a common complication in patients with cancer.Citation1 A growing body of evidence indicates that cancer patients with PE have shorter survival.Citation2–Citation4 PE can be fatal or cause chronic thromboembolic pulmonary hypertension. The incidence of incidental PE (IPE) has increased with advances in multi-detector-row computed tomography (CT) technology and its increased use in routine staging and follow-up in cancer patients.Citation5–Citation9 Recent retrospective research in cancer patients indicates that the embolic burden in IPE is similar to that in symptomatic PE.Citation10–Citation14 Currently, all major guidelines recommend that the treatment of cancer patients with IPE should refer to the treatment of cancer patients with symptomatic PE.Citation15–Citation17 Interestingly, the 2016 American College of Chest Physicians guideline suggests low-risk patients with isolated subsegmental PE (SSPE) receive no treatment in cases with normal bilateral ultrasonography of the legs (Grade 2C).Citation16 In addition, a cohort study has suggested that there is no difference in overall survival between lung cancer patients with incidental cancer-associated SSPE and those without PE.Citation18
Gastric cancer patients are also at high risk of venous thromboembolism (VTE), with an incidence of 1.3–18.3%.Citation19–Citation22 Furthermore, both Myat Moe et al and den Exter et al found that patients with advanced gastric cancer were more predisposed to developing IPE than patients with other types of cancers.Citation13,Citation23 However, anticoagulant therapy for gastric cancer patients with VTE poses a higher bleeding risk than other cancer types.Citation24–Citation26 In addition, peripheral PEs are more easily discovered using high-resolution CT. How to treat incidental peripheral PE in cancer patients is a central focus of current research. Whether advanced gastric cancer patients with IPE, especially peripheral PE, need anticoagulation therapy is still unknown. There is very little information available pertaining to the relationship between IPE and advanced gastric cancer. The purpose of our study was to explore the clinical characteristics and prognostic factors of patients with advanced gastric cancer complicated by IPE and provide a clinical guideline for the treatment of these patients.
Patients and Methods
Patients
This retrospective study was conducted at the Shandong Cancer Hospital, which is a leading and internationally renowned modern cancer hospital in China. Of the 2563 patients diagnosed with gastric cancer from January 2011 to January 2021, 90 patients with histologically confirmed advanced gastric adenocarcinoma with IPE were enrolled. IPE was defined as PE incidentally detected on a CT scan performed for reasons other than a clinical suspicion of PE. Exclusion criteria were: 1) pulmonary artery obstruction by tumour emboli; 2) lack of medical records; 3) the PE was suspected before the patient received thoracic CT; 4) lack of available CT data; 5) lack of pathological diagnosis of gastric cancer; 6) Eastern Cooperative Oncology Group (ECOG) scores of 3–4 at the diagnosis of IPE; and 7) the patient received no antitumor therapy after the diagnosis of IPE. This study was approved by the institutional ethics committee (IRB No. SDTHEC2021001009).
Clinical Data
Clinical data of all eligible patients were collected from the electronic medical records system, including age, sex, body mass index, pathological type, lymph node metastasis, comorbid conditions, blood laboratory data at the diagnosis of IPE, anti-cancer therapy status at the time of IPE, management of IPE, type and duration of anticoagulation therapy, survival data, date at the diagnosis of gastric cancer, and date of death. Bleeding events were classified as major using the International Society of Thrombosis and Haemostasis criteria. A diagnosis of recurrent VTE during follow-up required objective confirmation. Patients were divided into two groups: those with IPE diagnosed concomitantly with gastric cancer (concurrent group) and those with IPE detected after the diagnosis of gastric cancer (sequential group).
Radiological Evaluation
CT images of each patient were independently reviewed by two senior chest radiologists. PE on CT images was defined as a sharply delineated pulmonary artery-filling defect in at least two consecutive sections located either centrally within the vessel or at acute angles to the interface with the vessel wall.Citation11 IPE was further categorised as central (pulmonary trunk and arteries), lobar, or peripheral (segmental/subsegmental) according to the most proximal clot seen in the pulmonary artery.
Statistical Analysis
SPSS software (version 20, SPSS Inc. Chicago, IL, USA) was used for the statistical analyses, and a two-sided P-value < 0.05 was considered to be statistically significant. Continuous variables were compared using Student’s t-test or the Mann–Whitney U-test if non-normally distributed. The Chi-squared test (or Fisher’s exact test where appropriate) was used to compare categorical variables. The Kaplan–Meier method and the Log rank test were used for survival analysis. Independent prognostic factors for survival were determined using a Cox proportional hazards model.
Results
Clinical Characteristics of Patients with IPE
Of the 2563 patients diagnosed with gastric cancer, only 90 patients with advanced gastric cancer were also diagnosed with IPE and included in the analysis. The baseline characteristics of the patients are summarised in . The median age at the diagnosis of IPE was 63.5 years (range, 37–91 years). Most of the patients were men (68.8%), and more than half had grade III histology (57.7%). Before the diagnosis of IPE, 46.6% of patients received chemotherapy, and 12.2% received surgery,20% received only targeted therapy. The median D-dimer level at the diagnosis of IPE was 8.7 ± 5.7 mg/L. The proportions of central PEs, lobar PEs, and peripheral PEs were 25.5%, 23.3%, and 51.1%, respectively. There were 19 patients who were diagnosed with IPE concomitantly with gastric cancer.
Table 1 Clinical Characteristics of Gastric Cancer Patients with IPE (n = 90)
Only 58 patients received anticoagulant therapy; 52 patients received low molecular weight heparin (LMWH) and 4 patients received LMWH followed by warfarin. The reasons for not administering anticoagulant therapy were as follows: at the physician’s discretion, 21 patients were not treated; 3 patients had contraindications to anticoagulant therapy; 4 patients refused anticoagulant therapy; and the reason was unknown in 4 patients. Only 15 patients were treated with anticoagulant therapy longer than 3 months. The median time between the diagnosis of gastric cancer and the detection of IPE was 74 days (range, 4–868 days). The median survival after the diagnosis of IPE was 290 days (range, 10–2269 days), and the median survival after the diagnosis of gastric cancer was 500 days (range, 10–2360 days).
Factors Associated with Survival in Gastric Cancer Patients with IPE
Univariate analysis found that the significant prognostic factors affecting the survival of advanced gastric cancer patients with IPE were: concurrence of gastric cancer and IPE (median survival, 11.8 months vs 19.2 months, P = 0.018), lack of anticoagulation treatment (median survival, 11.8 months vs 21.2 months, P = 0.002), and localisation of IPE (median survival, central: 11.8 months vs lobar: 14.8 months vs peripheral: 21.13 months, P = 0.031) (). Univariate analysis found that concurrence of gastric cancer and IPE, lack of anticoagulation therapy, and central IPE influenced the survival of advanced gastric cancer patients with IPE. After adjusting for age and sex, multivariate analysis showed that lack of anticoagulation therapy independently influenced the survival of advanced gastric cancer patients with IPE ().
Table 2 Univariate and Multivariate Analyses of Clinicopathologic Factors Associated with the Survival of Advanced Gastric Cancer Patients with IPE
Figure 1 Kaplan-Meier plots of survival based on the localisation of the pulmonary embolism (A), administration of anticoagulation therapy (B), and concurrent or sequential diagnosis of incidental pulmonary embolism (C).
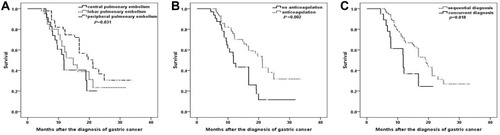
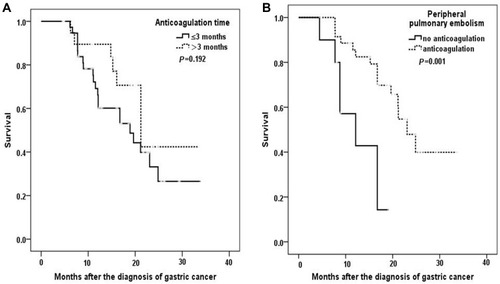
Subgroup analysis of patients receiving anticoagulant therapy showed no noticeable survival differences between patients receiving ≤ 3 months anticoagulant therapy and those receiving > 3 months anticoagulant therapy (median survival 12.13 months vs 23.06 months, P = 0.192). Subgroup analysis of patients with peripheral PE showed that anticoagulant therapy had a survival benefit (median survival, 18.9 vs 21.2 months, P = 0.001) ().
Figure 2 Kaplan-Meier plots of survival in patients receiving anticoagulation therapy based on the duration of anticoagulation therapy (A) and in patients with peripheral pulmonary embolisms based on administration of anticoagulation therapy (B).
Discussion
This study aimed to evaluate the clinical characteristics and survival of advanced gastric cancer patients who were incidentally diagnosed with PE. We found that the concurrence rate of advanced gastric cancer with IPE was 3.51%. This rate is consistent with the recently reported rate of 3.3–3.9% for IPE in cancer patients.Citation28,Citation29 The median time from the diagnosis of gastric cancer to the diagnosis of PE was 74 days. Our results were similar to the results of Khorana et al, who reported a median time from gastric cancer diagnosis to VTE diagnosis of 95 days.Citation30
In our study, approximately 21.1% of patients developed IPE concurrently with advanced gastric cancer. We identified that the concurrent diagnoses of IPE and gastric cancer was an independent predictor of death in advanced gastric cancer patients. Similarly, data from two retrospective studies suggested that the timing of PE presentation is closely related to prognosis in cancer patients with VTE.Citation22,Citation31 Cancer patients simultaneously diagnosed with venous thrombosis may have more aggressive tumour biology and poor prognoses; therefore, these patients should be carefully monitored. The interrelationship between the anticoagulant system and tumour progression and their underlying mechanisms are worthy of further investigation.
Because of the similarities in overall mortality, major bleeding, and recurrent VTE in patients with IPE and those with symptomatic PE, the general consensus is to use the same treatment strategy for both sets of patients.Citation13,Citation32–Citation34 Primarily, on the basis of the results of the CLOT (Randomized Comparison of LMWH versus Oral Anticoagulant Therapy for the Prevention of Recurrent VTE in Patients with Cancer) trial,Citation35–Citation37 evidence-based guidelines recommend at least 6 months of LMWH treatment for patients with VTE and cancer, and that LMWH is preferable to warfarin-based treatment.
In the current study, 58 patients who received anticoagulant therapy had significantly improved survival compared to 32 patients who received no anticoagulant therapy. Therefore, anticoagulant therapy cannot be disregarded for advanced gastric cancer patients with IPE. Nevertheless, no survival differences were found between patients who received ≤ 3 months of anticoagulant therapy and those who received > 3 months of anticoagulant therapy. This may be because only 12 patients (20.6%) received more than 3 months of LMWH treatment. Some previous reports also showed that most patients receive less than 3 months of LMWH treatment and are notably more likely to discontinue treatment in the real world.Citation38,Citation39 This has been attributed to the burden of self-injection and the high cost of LMWH. The latest data shows that direct oral anticoagulants (DOACs) could emerge as an alternative to warfarin and LMWH for the treatment of cancer-associated VTE.Citation25,Citation40 Regrettably, in gastric cancer patients, DOACs carry a higher risk of bleeding than other anticoagulant drugs. It is expected that new, effective, and safe DOACs will be used in the treatment of gastric cancer with VTE in the future.Citation25
Increasing evidence supports that the location of the PE is closely related to prognosis.Citation31,Citation41–Citation43 Our study corroborates these previous reports. It is worth noting that more SSPEs have been discovered due to the advancement of imaging technologies and the application of high-resolution CT.Citation44 The management of incidental SSPE in cancer patients has recently become a focus of controversy.Citation45 A recent systematic literature review pooling patient-level data and a prospective cohort study both reported that patients with incidental cancer-associated SSPE have the same risk of recurrent VTE as patients with more proximal PE, despite having received anticoagulation therapy.Citation46,Citation47 Moreover, the risk of recurrent VTE is 55% in cases of incidental cancer-associated SSPE that is left untreated.Citation47 One another retrospective studies suggest that patients with incidental cancer-associated SSPE might not need anticoagulant treatment.Citation48 In our subgroup analysis, anticoagulant therapy had a survival benefit in patients with peripheral PEs (median survival, 18.9 vs 21.2 months, P = 0.001).
Our study had several limitations. First, due to its retrospective design, some data were lacking. For example, bleeding events, recurrent VTE, and associated deep vein thrombosis were not systematically assessed in patients. Second, the number of patients in this study receiving anticoagulant treatment > 3 months was very small; therefore, we could not evaluate the relationship between the anticoagulation treatment period and survival benefit. Last, although we excluded some patients who received no antitumor treatment or had ECOG scores of 3–4 at the diagnosis of IPE, treatment bias still exists among patients.
In conclusion, IPE is an important event in advanced gastric cancer patients. Concurrence of gastric cancer with IPE and central IPE are important factors affecting the prognoses of these patients. Active anticoagulant therapy might improve survival of advanced gastric cancer patients with IPE. In patients with incidental cancer-associated SSPE, anticoagulant treatment might have survival benefits. Given the limitations of this small retrospective analysis, larger prospective studies are needed to better understand the natural course of IPE and investigate the optimal duration of anticoagulation therapy in advanced gastric cancer patients with IPE.
Disclosure
The authors indicate no potential conflicts of interest.
Acknowledgments
We would like to thank Editage for English language editing.
References
- Lyman GH, Culakova E, Poniewierski MS. Morbidity, mortality and costs associated with venous thromboembolism in hospitalized patients with cancer. Thromb Res. 2018:S112–S118. doi:10.1016/j.thromres.2018.01.028.29703467
- Li Y, Shang Y, Wang W, et al. Lung Cancer and pulmonary embolism: what is the relationship? A review. J Cancer. 2018;9(17):3046–3057. doi:10.7150/jca.26008.30210627
- Re G, Tm P, Petterson TM, et al. Risk factors for incident venous thromboembolism in active cancer patients: a population based case-control study. Thromb Res. 2016;139:29–37. doi:10.1016/j.thromres.2016.01.00226916293
- Alotaibi G, Wu C, Senthilselvan A, et al. Short- and long-term mortality after pulmonary embolism in patients with and without cancer. Vasc Med (London, England). 2018;23(3):261–266. doi:10.1177/1358863X18754692.
- Yao Y, Xu QProgress in the study of cancer-associated venous thromboembolism. Vascular. 2021;29(3):408–414. doi:10.1177/170853812095744332951561
- Browne AM, Cronin CG, English C, NiMhuircheartaigh J, Murphy JM, Bruzzi JF. Unsuspected pulmonary emboli in oncology patients undergoing routine computed tomography imaging. J Thor Oncol. 2010;5(6):798–803. doi:10.1097/JTO.0b013e3181d6153a
- Douma RA, Kok MG, Verberne LM, et al. Incidental venous thromboembolism in cancer patients: prevalence and consequence. Thromb Res. 2010;125(6):e306–e309. doi:10.1016/j.thromres.2010.02.01020223502
- Ritchie G, McGurk S, McCreath C, Graham C, Murchison JT. Prospective evaluation of unsuspected pulmonary embolism on contrast enhanced multidetector CT (MDCT) scanning. Thorax. 2007;62(6):536–540. doi:10.1136/thx.2006.06229917158631
- Tresoldi S, Flor N, Luciani A, et al. Contrast enhanced chest-MDCT in oncologic patients. Prospective evaluation of the prevalence of incidental pulmonary embolism and added value of thin reconstructions. Eur Radiol. 2015;25(11):3200–3206. doi:10.1007/s00330-015-3739-7.25899418
- Chaturvedi S, Sidana S, Elson P, et al. Symptomatic and incidental venous thromboembolic disease are both associated with mortality in patients with prostate cancer. PLoS One. 2014;9(8):e94048. doi:10.1371/journal.pone.0094048.25126949
- Connolly GC, Menapace L, Safadjou S, et al.. Prevalence and clinical significance of incidental and clinically suspected venous thromboembolism in lung cancer patients. Clin Lung Cancer. 2013;14(6):713–718. doi:10.1016/j.cllc.2013.06.003.23891560
- Callejas MF, Errázuriz JI, Castillo F, et al. Incidental venous thromboembolism detected by PET-CT in patients with cancer: prevalence and impact on survival rate. Thromb Res. 2014;133(5):750–755. doi:10.1016/j.thromres.2014.02.00524565275
- den Exter PL, Hooijer J, Dekkers OM, et al. Risk of recurrent venous thromboembolism and mortality in patients with cancer incidentally diagnosed with pulmonary embolism: a comparison with symptomatic patients. J Clin Oncol. 2011;29(17):2405–2409. doi:10.1200/JCO.2010.34.098421555690
- Bozas G, Jeffery N, Ramanujam-Venkatachala D, et al. Prognostic assessment for patients with cancer and incidental pulmonary embolism. Thromb J. 2018;16:8. doi:10.1186/s12959-017-0157-x29445314
- Lyman GH, Khorana AA, Kuderer NM, et al. Venous thromboembolism prophylaxis and treatment in patients with cancer: American Society of Clinical Oncology clinical practice guideline update. J Oncol Pract Am Soc Clin Oncol. 2015;31(17):2189.
- Kearon C, Akl EA, Ornelas J, et al. Antithrombotic therapy for VTE disease: CHEST guideline and expert panel report. Chest. 2016;149(2):315–352.26867832
- Mandalà M, Labianca R. Venous thromboembolism (VTE) in cancer patients. ESMO clinical recommendations for prevention and management. Thromb Res. 2010;S117–S119. doi:10.1016/S0049-3848(10)70028-120433989
- O’connell C, Razavi P, Ghalichi M, et al. Unsuspected pulmonary emboli adversely impact survival in patients with cancer undergoing routine staging multi-row detector computed tomography scanning. J Thrombosis Haemostasis. 2011;9(2):305–311. doi:10.1111/j.1538-7836.2010.04114.x.
- Wada T, Fujiwara H, Morita S, Fukagawa T, Katai H. Incidence of and risk factors for preoperative deep venous thrombosis in patients undergoing gastric cancer surgery. Gastric Cancer. 2017;20(5):872–877. doi:10.1007/s10120-017-0690-028120128
- Kimura Y, Oki E, Ando K, et al. Incidence of venous thromboembolism following laparoscopic surgery for gastrointestinal cancer: a single-center, prospective cohort study. World J Surg. 2016;40(2):309–314. doi:10.1007/s00268-015-3234-y.26316113
- Tanizawa Y, Bando E, Kawamura T, et al. Prevalence of deep venous thrombosis detected by ultrasonography before surgery in patients with gastric cancer: a retrospective study of 1140 consecutive patients. Gastric Cancer. 2017;20(5):878–886. doi:10.1007/s10120-016-0677-2.27987041
- Kang MJ, Ryoo BY, Ryu MH, et al. Venous thromboembolism (VTE) in patients with advanced gastric cancer: an Asian experience. Eur J Cancer. 2012;48(4):492–500. doi:10.1016/j.ejca.2011.11.01622169121
- Myat Moe MM, Redla S. Incidental pulmonary embolism in oncology patients with current macroscopic malignancy: incidence in different tumour type and impact of delayed treatment on survival outcome. Br J Radiol. 2018;91(1088):20170806. doi:10.1259/bjr.20170806.29688026
- Chen DY, Tseng CN, Hsieh M-J, et al. Comparison between non-vitamin K antagonist oral anticoagulants and low-molecular-weight heparin in Asian individuals with cancer-associated venous thromboembolism. JAMA Net Open. 2021;4(2):e2036304. doi:10.1001/jamanetworkopen.2020.36304
- Di Nisio M, Di Nisio M, Mulder F, et al. Clinical impact of bleeding in cancer-associated venous thromboembolism: results from the Hokusai VTE cancer study. Thromb Haemost. 2018;118(8):1439–1449. doi:10.1055/s-0038-166700130060256
- van Es N, van Es N, Bleker S, et al. Clinical impact and course of anticoagulant-related major bleeding in cancer patients. Thromb Haemost. 2018;118(1):174–181. doi:10.1160/TH17-04-027429304537
- Gladish GW, Choe DH, Marom EM, et al. Incidental pulmonary emboli in oncology patients: prevalence, CT evaluation, and natural history. Radiology. 2006;240(1):246–255. doi:10.1148/radiol.240105112916684921
- Bach AG, Schmoll HJ, Beckel C, et al. Pulmonary embolism in oncologic patients: frequency and embolus burden of symptomatic and unsuspected events. Acta Radiol. 2014;55(1):45–53. doi:10.1177/028418511349156923864061
- Dg L, Lohan DG, Keane M, et al. Prevalence and significance of asymptomatic venous thromboembolic disease found on oncologic staging CT. Am J Roentgenol. 2007;189(1):162–170. doi:10.2214/AJR.07.206717579167
- Khorana AA, Yannicelli D, McCrae KR, et al. Evaluation of US prescription patterns: are treatment guidelines for cancer-associated venous thromboembolism being followed? Thromb Res. 2016;145:51–53. doi:10.1016/j.thromres.2016.07.01327485998
- Cha SI, Shin KM, Lim JK, et al. Pulmonary embolism concurrent with lung cancer and central emboli predict mortality in patients with lung cancer and pulmonary embolism. J Thorac Dis. 2018;10(1):262–272. doi:10.21037/jtd.2017.12.3229600056
- Font C, Carmona-Bayonas A, Beato C, et al. Clinical features and short-term outcomes of cancer patients with suspected and unsuspected pulmonary embolism: the EPIPHANY study. Eur Respir J. 2017;49:1.
- van Es N, Bleker, Di Nisio M. Cancer-associated unsuspected pulmonary embolism. Thromb Res. 2014;133:S172–S178. doi:10.1016/S0049-3848(14)50028-X24862140
- den Exter PL, Lj K, van der Hulle T, et al. Embolic burden of incidental pulmonary embolism diagnosed on routinely performed contrast-enhanced computed tomography imaging in cancer patients. J Thrombosis Haemostasis. 2013;11(8):1620–1622. doi:10.1111/jth.12325
- W S, Lee AYY, Carrier M, et al. Low-molecular-weight-heparin versus a coumarin for the prevention of recurrent venous thromboembolism in high- and low-risk patients with active cancer: a post hoc analysis of the CLOT study. J Thromb Thrombolysis. 2019;47(4):495–504. doi:10.1007/s11239-019-01833-w30859370
- Di Nisio M, Lee AY, Carrier M, et al. Diagnosis and treatment of incidental venous thromboembolism in cancer patients: guidance from the SSC of the ISTH. J Thrombosis Haemostasis. 2015;13(5):880–883. doi:10.1111/jth.12883
- Klok FA, Huisman MV. Management of incidental pulmonary embolism. Eur Respir J. 2017;49(6). doi:10.1183/13993003.00282-2016
- Zwicker JI, Bauer KA. How long is long enough? Extended anticoagulation for the treatment of cancer-associated deep vein thrombosis. J Clin Oncol. 2014;32(32):3596. doi:10.1200/JCO.2014.56.518425267753
- Khorana AA, McCrae KR, Milentijevic D, et al. Current practice patterns and patient persistence with anticoagulant treatments for cancer-associated thrombosis. Res Pract Thrombosis Haemostasis. 2017;1(1):14–22. doi:10.1002/rth2.12002
- Rossel A, Robert-Ebadi H, Combescure C, et al. Anticoagulant therapy for acute venous thrombo-embolism in cancer patients: a systematic review and network meta-analysis. PLoS One. 2019;14(3):e213940. doi:10.1371/journal.pone.0213940
- Choi K-J, Cha S-I, Shin K-M, et al. Central emboli rather than saddle emboli predict adverse outcomes in patients with acute pulmonary embolism. Thromb Res. 2014;134(5):991–996. doi:10.1016/j.thromres.2014.08.02725228399
- Gouin B, Blondon M, Jiménez D, et al. Clinical prognosis of nonmassive central and noncentral pulmonary embolism: a registry-based cohort study. Chest. 2017;151(4):829–837. doi:10.1016/j.chest.2016.10.05627876590
- Vedovati MC, Germini F, Agnelli G, et al. Prognostic role of embolic burden assessed at computed tomography angiography in patients with acute pulmonary embolism: systematic review and meta-analysis. J Thrombosis Haemostasis. 2013;11(12):2092–2102. doi:10.1111/jth.12429
- Browne AM, Cronin C, English C, et al. Unsuspected pulmonary emboli in oncology patients undergoing routine computed tomography imaging. J Thor Oncol. 2010;5(6):798–803. doi:10.1097/JTO.0b013e3181d6153a
- Ikesaka R, Carrier M. Clinical significance and management of subsegmental pulmonary embolism. J Thromb Thrombolysis. 2015;39(3):311–314. doi:10.1007/s11239-015-1169-725772115
- Kraaijpoel N, Bleker SM, Meyer G, et al. Treatment and long-term clinical outcomes of incidental pulmonary embolism in patients with cancer: an international prospective cohort study. J Clin Oncol. 2019;37(20):1713–1720. doi:10.1200/JCO.18.0197731116676
- van der Hulle T, den Exter PL, Planquette B, et al. Risk of recurrent venous thromboembolism and major hemorrhage in cancer-associated incidental pulmonary embolism among treated and untreated patients: a pooled analysis of 926 patients. J Thrombosis Haemostasis. 2016;14(1):105–113. doi:10.1111/jth.13172
- Shinagare AB, Okajima Y, Oxnard GR, et al. Unsuspected pulmonary embolism in lung cancer patients: comparison of clinical characteristics and outcome with suspected pulmonary embolism. Lung Cancer. 2012;78(2):161–166. doi:10.1016/j.lungcan.2012.08.00722959241