
Abstract
Purpose
No consensus has been reached regarding the survival difference between cervical adenocarcinoma (ADC) and adenosquamous carcinoma (ASC) patients. The purpose of this study was to compare survival outcomes and prognostic factors between early-stage ADC and ASC patients.
Patients and Methods
We retrospectively reviewed stage IB-IIA patients with ADC and ASC who underwent radical hysterectomy and postoperative radiotherapy between June 2012 and December 2017.
Results
A total of 125 patients were enrolled in our study (97 with ADC and 28 with ASC). The median follow-up period was 53.4 months. Compared with ASC patients, patients with ADC tended to have a higher proportion of positive pelvic lymph nodes (7.1% and 26.8%, respectively; p = 0.028). The most common site of distant metastasis was the lung, followed by the intestine and colon. The 5-year overall survival (OS), disease-free survival (DFS), pelvic control, and distant control rates for ADC and ASC patients were 83.6% and 92.0% (p = 0.349), 77.5% and 87.7% (p = 0.279), 81.8% and 96.2% (p = 0.121), and 88.3% and 87.7% (p = 0.948), respectively. Parametrial invasion was a prognostic factor for OS. Lymphovascular space involvement was a prognostic factor for DFS.
Conclusion
ADC patients were more likely to have positive pelvic lymph nodes than those with ASC. There was no significant difference in survival outcomes between patients with ADC and ASC.
Introduction
Cervical cancer, one of the leading causes of cancer-related mortality among women, is the fourth largest gynecologic malignant tumor worldwide. Although the incidence has been reduced due to the increasing use of cytologic screening, annual rates of recurrence and death remain high. The main pathologic types of cervical cancer include squamous cell carcinoma (SCC), adenocarcinoma (ADC), and adenosquamous carcinoma (ASC).Citation1 Notably, the morbidity of ADC and ASC is significantly lower than that of SCC. And the incidence of ADC and ASC has increased in recent years.Citation2–Citation4
Controversies persist regarding outcomes and prognostic factors of early International Federation of Gynecology and Obstetrics (FIGO) stage (I–IIA) cervical cancer patients. In terms of prognostic factors, Zhou et alCitation5 identified that FIGO stage, tumor size, and lymph node status were related to overall survival (OS) and disease-free survival (DFS). However, Shu et alCitation6 retrospectively analyzed 1335 IB-IIA cervical cancer patients, including those with SCC, ADC, and ASC, and found that pathologic types, FIGO stage, and tumor size were not significant prognostic factors. Regarding prognosis, several studies have revealed that ADC and ASC patients had poorer OS and DFS than SCC patients.Citation5,Citation7
However, studies focusing on ADC and ASC are limited. No consensus has been reached regarding the differences between the prognosis of ADC and ASC patients. Early studies have shown that compared with ADC patients, ASC patients tended to have a lower 5-year DFS rate and shorter interval of disease recurrence.Citation8,Citation9 However, Zhang et alCitation10 recently compared the outcome between ADC and ASC patients, which showed no significant prognostic difference.
Surgical treatment is the first choice for most patients with early-stage cervical cancer. However, no consensus has been reached regarding the choice of postoperative adjuvant therapy. Song et alCitation11 showed that compared with radiotherapy (RT), concurrent radiochemotherapy (CCRT) may improve DFS. However, several subsequent studies revealed that patients who underwent postoperative CCRT or RT experienced similar survival.Citation12,Citation13 In this study, we compared the outcomes and prognostic factors between early-stage ADC and ASC patients who had received primary radical surgery and postoperative adjuvant RT or CCRT. The results may provide a basis to determine the survival outcomes of ADC/ASC patients and aid the development of individualized adjuvant treatment plans.
Materials and Methods
Patients
We retrospectively reviewed medical records of patients with cervical cancer in our clinical department from June 2012 to December 2017. The inclusion criteria were as follows: histological diagnosis of ADC or ASC, FIGO stage IB-IIA, history of radical hysterectomy with pelvic lymph node (PLN) dissection followed by postoperative RT, and no neoadjuvant RT. Patients with other histological types, such as SCC, neuroendocrine carcinoma, sarcoma and undifferentiated carcinoma, and incomplete clinical and pathological data were excluded. The final sample size of our study was 125, including 97 patients with ADC and 28 patients with ASC.
Clinical and Pathological Characteristics
All patients were staged using the 2009 FIGO staging system. Clinicopathological characteristics were obtained by reviewing medical and pathological reports, including age, FIGO stage, tumor size, parametrial invasion, resection margin, lymphovascular space involvement (LVSI), depth of stromal invasion (DSI), uterine invasion, and PLN status.
Treatment
As the primary treatment, all patients underwent radical hysterectomy with bilateral pelvic lymphadenectomy (including common iliac, internal iliac, external iliac, obturator, and presacral lymph node tissues) with or without para-aortic lymph node resection by either laparoscopy or laparotomy.
Adjuvant RT was started within 4–6 weeks after the primary radical surgery. External beam radiation therapy was administered with intensity modulated radiation therapy. Clinical target volume (CTV) was delineated via computed tomography (CT). The CTV covered the parametrium and upper part of the vaginal and regional lymph node regions, including the internal iliac, external iliac, obturator, presacral, with or without common iliac and para-aortic lymph node regions. A margin of 8 to 10 mm was added to the CTV in all directions to create the planning clinical target volume (PCTV). A dose of 45 Gy in 25 fractions or 50.4 Gy in 28 fractions was delivered to the PCTV. Intracavitary brachytherapy was provided to part of patients with 10–20 Gy in 2–4 fractions.
Cisplatin (40 mg/m2) was administered weekly as the first-line concurrent chemotherapy regimen in most patients for 4–6 cycles. Few patients received paclitaxel plus carboplatin, paclitaxel plus cisplatin, or cisplatin plus 5-fluorouracil every 3 weeks for 2–3 cycles.
Follow-Up
After initial treatment, all patients underwent regular follow-up including physical examination, thinprep cytology test (TCT), abdominal and pelvic ultrasonography. Chest and abdominal CT and pelvic magnetic resonance imaging (MRI) were conducted regularly. Patients who were highly suspected of having recurrence or distant metastasis underwent positron emission tomography (PET)-CT. During follow-up, patients were required to be checked every 3 months in the first 2 years and every 6 months in the next 3–5 years.
Toxicities
Toxicities related to treatment were retrospectively reviewed and graded using the Common Toxicity Criteria for Adverse Events (CTCAE) version 5.0. Adverse events that developed within 90 days from the start of treatment were considered acute toxicities. Those that appeared after 90 days were classified as chronic toxicities.
Statistical Analysis
The variables of concern were the OS and DFS. DFS was defined as the period from the primary surgery to the first recurrence or the most recent follow-up. OS was defined as the period from primary surgery to death from any cause or the most recent follow-up. Patients’ clinicopathological characteristics were compared using the chi-squared test, continuity correction test, or Fisher’s exact test. We used 1:1 propensity score matching to balance the basic characteristics between ADC and ASC patients, including LVSI, pelvic lymph nodes and number of positive PLNs. OS, DFS, pelvic control, and distant control rates were calculated and compared using the Kaplan–Meier method and Log rank tests. Univariate and multivariate Cox regression analyses were used to analyze the prognostic factors. Statistical significance was set at p < 0.05. All statistical analyses were conducted using SPSS (version 23.0, IBM Corporation, Armonk, NY, USA).
Results
Clinicopathological Characteristics
A total of 125 patients were enrolled in this study, comprising 97 patients (77.6%) with ADC and 28 patients (22.4%) with ASC. The clinicopathological characteristics of the patients are displayed in . The number of ADC patients with FIGO stage IB1, IB2, IIA1, and IIA2 were 61 (62.9%), 26 (26.8%), 7 (7.2%), and 3 (3.1%), respectively. Among the patients with ASC, 19 (67.9%), 6 (21.4%), 2 (7.1%), and 1 (3.6%) patients were IB1, IB2, IIA1, and IIA2, respectively. Patients with ADC were more likely to have positive pelvic lymph nodes than those with ASC (26.8% compared to 7.1%, p = 0.028). Other features such as age, FIGO stage, tumor size, LVSI, parametrial invasion, and resection margin were similar between the two groups. For patients with ADC, 20 (20.6%) received neoadjuvant chemotherapy, 18 (18.6%) received postoperative radiation alone, and 79 (81.4%) received postoperative radiation and chemotherapy. The number of patients with ASC who received neoadjuvant chemotherapy, postoperative radiation alone, and postoperative radiation and chemotherapy were 4 (14.3%), 6 (21.4%) and 22 (78.6%), respectively.
Table 1 Clinicopathological Characteristics of ADC and ASC Patients
Survival Outcomes and Failure Patterns
The overall median follow-up duration was 53.4 months (range: 3.5–96.3 months). For ADC patients, median follow-up time was 51.6 months (range: 3.5–95.4 months), and for ASC patients, median follow-up time was 60.5 months (range: 3.8–96.3 months).
During follow-up, 26 patients experienced recurrence, namely 22 with ADC and 4 with ASC. The most common distant metastasis site was the lung (eight patients), followed by the intestine and colon (three patients), and greater omentum or peritoneum (two patients).
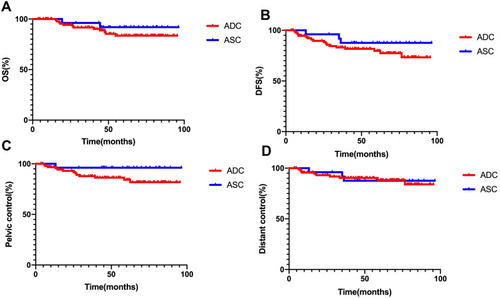
As shown in , for ADC and ASC patients, the 5-year OS, DFS, pelvic control, and distant control rates were 83.6% and 92.0% (p = 0.349), 77.5% and 87.7% (p = 0.279), 81.8% and 96.2% (p = 0.121), and 88.3% and 87.7% (p = 0.948), respectively. The Kaplan–Meier curves of OS, DFS, pelvic control, and distant control rates are shown in .
Table 2 5-Year OS, DFS, Pelvic Control and Distant Control Rate of ADC and ASC Patients
Figure 1 Kaplan-Meier curves of (A) overall survival (OS), (B) disease-free survival (DFS), (C) pelvic control and (D) distant control rates for adenocarcinoma (ADC) and adenosquamous carcinoma (ASC) patients.
Prognostic Factors
According to the univariate analysis (), parametrial invasion was associated with OS (p < 0.001) and DFS (p = 0.018). LVSI and pelvic lymph node status were significant factors for DFS (p = 0.001 and p = 0.001, respectively).
Table 3 Univariate Cox Regression Analysis of Prognostic Factors
Multivariate analysis also indicated that parametrial invasion was an independent prognostic factor for OS (hazard ratio (HR) = 10.288, 95% confidence interval (CI) = 1.687–62.737, p = 0.012), and LVSI was an independent prognostic factor for DFS (HR = 3.094, 95% CI = 1.137–8.416, p = 0.027) (). Histology was not a significant prognostic factor for OS or DFS (p = 0.233 and p = 0.614, respectively).
Table 4 Multivariate Cox Regression Analysis of Prognostic Factors
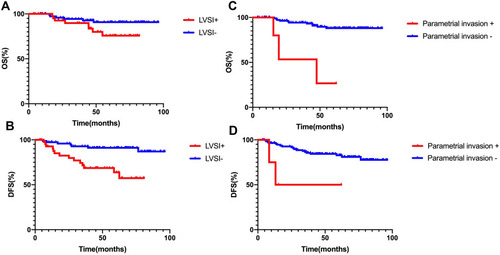
For patients with positive and negative LVSI, the 5-year OS rates were 75.8% and 90.8% (p = 0.073), and the 5-year DFS rates were 63.8% and 91.2% (p < 0.001), respectively. For patients with positive parametrial invasion and negative parametrial invasion, the 5-year OS rates were 26.7% and 88.1% (p < 0.001), and the 5-year DFS rates were 50.0% and 82.8% (p = 0.007), respectively. The Kaplan–Meier curves for OS and DFS are shown in .
Figure 2 Kaplan-Meier curves of overall survival (OS) and disease-free survival (DFS) for patients stratified by lymphovascular space involvement (LVSI) (A and B) and parametrial invasion (C and D).
Propensity Score Matching
We used 1:1 propensity score matching to balance the basic clinicopathological characteristics between patients with ADC and ASC. As a result, 28 patients with ADC were matched to 28 patients with ASC (). There was no significant difference in the basic variables between the two groups after matching.
After propensity score matching, the 5-year OS, DFS, pelvic control, and distant control rates for patients with ADC and ASC were 87.8% and 92.0% (p = 0.562), 87.5% and 87.7% (p = 0.638), 87.5% and 96.2% (p = 0.137), and 96.3% and 87.7% (p = 0.341), respectively ().
Toxicities
The acute and chronic toxicities of the treatments are shown in . Of the 125 patients with ADC or ASC, 39 (31.2%) developed grade 3 acute hematological toxicities, and 15 (12.0%) developed grade 4 acute hematological toxicities. For the digestive system, only one patient had intestinal obstruction classified as grade 3. During follow-up, hydronephrosis occurred in five (4.0%) patients.
Table 5 Acute and Chronic Toxicities of Patients
Discussion
In this study, we compared the clinicopathological characteristics, survival outcomes, and prognostic factors between patients with ADC and ASC. Our results showed that there was no significant difference in OS, DFS, pelvic control, and distant control rates between ADC and ASC patients. Parametrial invasion was an independent prognostic factor for OS, and LVSI was an independent prognostic factor for DFS.
At present, differences in clinicopathological features between ADC and ASC patients still need to be explored. Zhou et alCitation14 found that patients with ADC were more likely to be well and moderately differentiated, while more ASC patients were poorly and undifferentiated. Zhang et alCitation10 recently found that, compared with ADC patients, patients with ASC tended to be older and have higher frequencies of LVSI and serum squamous cell carcinoma antigen (SCC-Ag) greater than 5 ng/mL. However, in our study, the incidence of pelvic lymph node metastasis in patients with ADC was higher than that in patients with ASC. This result emphasizes the need for doctors and researchers to pay closer attention to the drainage field of the pelvic lymph system of ADC patients.
A retrospective study enrolling 318 FIGO stage IB-IIB cervical cancer patients (202 with SCC and 116 with ADC/ASC) treated with radical hysterectomy and postoperative RT or CCRT, discovered that distant metastasis was the major type of failure pattern in both SCC and ADC/ASC groups. Moreover, compared to SCC patients, the distant relapse sites of ADC and ASC patients were more commonly beyond the para-aortic lymph node and supraclavicular lymph node, mainly in the lungs and peritoneum.Citation7 Yang et alCitation15 retrospectively reviewed 247 FIGO stage IB-IIA cervical cancer patients from 2001 to 2011. A total of 48 patients (19.4%) experienced recurrence, including 7 patients (2.8%) with locoregional failure alone, 37 patients (15.0%) with distant metastasis alone, and 4 patients (1.6%) with both. The most common sites of distant metastasis were the lungs (16 patients), para-aortic lymph nodes (13 patients), and colorectum (6 patients). Moreover, a number of studies have demonstrated that, compared with SCC patients, ADC/ASC patients had a higher rate of ovarian metastasis and distant metastasis, such as abdominal carcinomatosis and para-aortic lymph node.Citation16–Citation20 Similarly, in our study, the most common sites of distant metastasis were the lungs, intestine and colon, followed by the great omentum and peritoneum. This suggests that, compared with SCC which mainly spreads through the lymphatic system, ADC/ASC may tend to spread hematologically.Citation7,Citation21
A series of studies have compared the outcomes of patients with SCC and ADC/ASC. Among them, many have demonstrated that the prognosis of ADC and ASC patients is worse than that of SCC.Citation5,Citation7,Citation22,Citation23 However, to date, few studies have compared the survival of patients with ADC and ASC. In early years, Lea et alCitation8 indicated that for low-risk FIGO stage IB1 patients, ASC histology predicted poorer outcome. Similarly, another study concluded that although there was no difference in recurrence rates between ADC and ASC, the median time to recurrence was shorter in patients with ASC.Citation9 Zhang et alCitation10 recently performed a retrospective study of FIGO stage IB-IIA cervical cancer patients (240 with ADC and 130 with ASC). Patients were stratified into low-, intermediate-, and high-risk groups based on clinicopathological features. The results showed that before stratification, the 5-year OS rates for patients with ADC and ASC were 68.1% and 74.7% (p = 0.145), respectively. After stratification, the 5-year OS rates in the low-, intermediate-, and high-risk groups for ADC and ASC patients were 80.8% and 85.4% (p = 0.437), 77.4% and 83.7% (p = 0.647), and 41.9% and 47.8% (p = 0.675), respectively, which was similar to the 5-year DFS rates. Our results showed no significant difference between ADC and ASC patients in 5-year OS or DFS rates before and after propensity score matching. Future studies need to expand the sample size and carry out prospective research.
In this study, compared to patients with negative parametrial invasion, the 5-year OS and DFS rates for patients with positive parametrial invasion were significantly decreased. Huang et alCitation7 analyzed 318 FIGO Stage IB-IIB cervical cancer cases, 202 with SCC and 116 with ADC/ASC. The results showed that parametrial invasion was a prognostic factor for local recurrence and distant metastasis. These results emphasize the importance of parametrial invasion in evaluating the prognosis of cervical cancer patients. This suggests that we should apply multiple clinical approaches, such as gynecological examination and medical imaging, to obtain more accurate staging for cervical cancer. If postoperative pathology demonstrates that parametrial invasion is positive, more aggressive postoperative adjuvant treatments will be necessary.
Notably, parametrial invasion is closely related to up-staging of cervical cancer. However, FIGO stage was not a prognostic factor in this study. In our study, all the patients were staged using the 2009 FIGO staging system, which is a clinical staging system mainly based on physical examination before treatment, supplemented with imaging evaluation. Although patients underwent detailed physical examination by experienced gynecologists, and multiple imaging evaluations before treatment, there were still some limitations. For example, the results could have been influenced if there were minimal infiltrative lesions that could only be identified by postoperative pathology.
The study has a few limitations. First, our study was a retrospective study, which might have had some inherent bias. Second, the sample size might be insufficient and have an imbalance between number of ADC and ASC patients. Third, there is a need to further analyze high-risk and intermediate-risk factors and other pathological grading systems, such as the Silva pattern system of adenocarcinoma. Moreover, high-risk HPV infection and molecular immunity have received notable consideration in the study of cervical cancer. We propose that future research incorporate prospective, multi-center, and large-scale clinical trials.
Conclusion
Our study demonstrated that patients with ADC were more likely to have positive pelvic lymph nodes than those with ASC. There was no significant difference in OS, DFS, pelvic control, and distant control rates between ADC and ASC patients. Parametrial invasion was an independent prognostic factor for OS, and LVSI was an independent prognostic factor for DFS.
Abbreviations
SCC, squamous cell carcinoma; ADC, adenocarcinoma; ASC, adenosquamous carcinoma; FIGO, International Federation of Gynecology and Obstetrics; OS, overall survival; DFS, disease-free survival; RT, radiotherapy; CCRT, concurrent radiochemotherapy; PLN, pelvic lymph node; LVSI, lymphovascular space involvement; DSI, depth of stromal invasion; CTV, clinical target volume; CT, computed tomography; PCTV, planning clinical target volume; TCT, thinprep cytology test; MRI, magnetic resonance imaging; PET, positron emission tomography; CTCAE, Common Toxicity Criteria for Adverse Events; HR, hazard ratio; CI, confidence interval.
Ethics Approval
This protocol was approved by the Institutional Review Board of Peking Union Medical College Hospital. The ethical committee process number is S-K1710. This is a retrospective study and informed consent was unnecessary. The data was anonymized and maintained with confidentiality in this study. This manuscript does not cover any information about patients’ privacy. All procedures in this study were conducted in accordance with the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
- Fujiwara K, Monk B, Devouassoux-Shisheboran M. Adenocarcinoma of the uterine cervix: why is it different? Curr Oncol Rep. 2014;16(12):416. doi:10.1007/s11912-014-0416-y25325935
- Seoud M, Tjalma WA, Ronsse V. Cervical adenocarcinoma: moving towards better prevention. Vaccine. 2011;29(49):9148–9158. doi:10.1016/j.vaccine.2011.09.11521983356
- Missaoui N, Trabelsi A, Landolsi H, et al. Cervical adenocarcinoma and squamous cell carcinoma incidence trends among Tunisian women. Asian Pac J Cancer Prev. 2010;11(3):777–780.21039053
- Wang SS, Sherman ME, Hildesheim A, et al. Cervical adenocarcinoma and squamous cell carcinoma incidence trends among white women and black women in the United States for 1976–2000. Cancer. 2004;100(5):1035–1044. doi:10.1002/cncr.2006414983500
- Zhou J, Zhang WW, Wu SG, et al. The prognostic value of histologic subtype in node-positive early-stage cervical cancer after hysterectomy and adjuvant radiotherapy. Int J Surg. 2017;44:1–6. doi:10.1016/j.ijsu.2017.05.07428583891
- Shu T, Zhao D, Li B, et al. Prognostic evaluation of postoperative adjuvant therapy for operable cervical cancer: 10 years’ experience of National Cancer Center in China. Chin J Cancer Res. 2017;29(6):510–520. doi:10.21147/j.issn.1000-9604.2017.06.0529353973
- Huang YT, Wang CC, Tsai CS, et al. Clinical behaviors and outcomes for adenocarcinoma or adenosquamous carcinoma of cervix treated by radical hysterectomy and adjuvant radiotherapy or chemoradiotherapy. Int J Radiat Oncol Biol Phys. 2012;84(2):420–427. doi:10.1016/j.ijrobp.2011.12.01322365621
- Lea JS, Coleman RL, Garner EO, et al. Adenosquamous histology predicts poor outcome in low-risk stage IB1 cervical adenocarcinoma. Gynecol Oncol. 2003;91(3):558–562. doi:10.1016/j.ygyno.2003.08.02014675676
- Reis RD, Frumovitz M, Milam MR, et al. Adenosquamous carcinoma versus adenocarcinoma in early-stage cervical cancer patients undergoing radical hysterectomy: an outcomes analysis. Gynecol Oncol. 2007;107(3):458–463. doi:10.1016/j.ygyno.2007.07.08017854872
- Zhang X, Lv Z, Xu X, et al. Comparison of adenocarcinoma and adenosquamous carcinoma prognoses in Chinese patients with FIGO stage IB-IIA cervical cancer following radical surgery. BMC Cancer. 2020;20(1):664. doi:10.1186/s12885-020-07148-x32678039
- Song S, Song C, Kim HJ, et al. 20 year experience of postoperative radiotherapy in IB-IIA cervical cancer patients with intermediate risk factors: impact of treatment period and concurrent chemotherapy. Gynecol Oncol. 2012;124(1):63–67. doi:10.1016/j.ygyno.2011.09.03322004904
- Cushman TR, Haque W, Menon H, et al. Postoperative chemoradiotherapy versus radiotherapy alone for elderly cervical cancer patients with positive margins, lymph nodes, or parametrial invasion. J Gynecol Oncol. 2018;29(6):e97. doi:10.3802/jgo.2018.29.e9730207105
- Kim H, Park W, Kim YS, et al. Chemoradiotherapy is not superior to radiotherapy alone after radical surgery for cervical cancer patients with intermediate-risk factor. J Gynecol Oncol. 2020;31(3):e35. doi:10.3802/jgo.2020.31.e3531912685
- Zhou J, Wu SG, Sun JY, et al. Comparison of clinical outcomes of squamous cell carcinoma, adenocarcinoma, and adenosquamous carcinoma of the uterine cervix after definitive radiotherapy: a population-based analysis. J Cancer Res Clin Oncol. 2017;143(1):115–122. doi:10.1007/s00432-016-2246-927646608
- Yang K, Park W, Huh SJ, et al. Clinical outcomes in patients treated with radiotherapy after surgery for cervical cancer. Radiat Oncol J. 2017;35(1):39–47. doi:10.3857/roj.2016.0189327927011
- Shimada M, Kigawa J, Nishimura R, et al. Ovarian metastasis in carcinoma of the uterine cervix. Gynecol Oncol. 2006;101(2):234–237. doi:10.1016/j.ygyno.2005.10.00416300819
- Berek JS, Hacker NF, Fu YS, et al. Adenocarcinoma of the uterine cervix: histologic variables associated with lymph node metastasis and survival. Obstet Gynecol. 1985;65(1):46–52.3966022
- Drescher CW, Hopkins MP, Roberts JA. Comparison of the pattern of metastatic spread of squamous cell cancer and adenocarcinoma of the uterine cervix. Gynecol Oncol. 1989;33(3):340–343. doi:10.1016/0090-8258(89)90524-62722061
- Eifel PJ, Morris M, Oswald MJ, et al. Adenocarcinoma of the uterine cervix. Prognosis and patterns of failure in 367 cases. Cancer. 1990;65(11):2507–2514. doi:10.1002/1097-0142(19900601)65:11<2507::AID-CNCR2820651120>3.0.CO;2-92337867
- Lee KB, Lee JM, Park CY, et al. What is the difference between squamous cell carcinoma and adenocarcinoma of the cervix? A matched case-control study. Int J Gynecol Cancer. 2006;16(4):1569–1573. doi:10.1111/j.1525-1438.2006.00628.x16884367
- Gien LT, Beauchemin MC, Thomas G. Adenocarcinoma: a unique cervical cancer. Gynecol Oncol. 2010;116(1):140–146. doi:10.1016/j.ygyno.2009.09.04019880165
- Hu K, Wang W, Liu X, et al. Comparison of treatment outcomes between squamous cell carcinoma and adenocarcinoma of cervix after definitive radiotherapy or concurrent chemoradiotherapy. Radiat Oncol. 2018;13(1):249. doi:10.1186/s13014-018-1197-530558636
- Landoni F, Maneo A, Colombo A, et al. Randomised study of radical surgery versus radiotherapy for stage Ib-IIa cervical cancer. Lancet. 1997;350(9077):535–540. doi:10.1016/S0140-6736(97)02250-29284774