Abstract
Introduction
The current standard for treating operable early stage non-small cell lung cancer is surgical resection and for inoperable cases it is external beam radiotherapy. Lung functions are adversely affected with both the above treatments. CyberKnife treatment limits radiation damage by tracking targets moving with each breath. The effect of CyberKnife treatment on pulmonary function tests has not been well documented.
Methods
Lung cancer patients who underwent CyberKnife treatment and had pre- and post-treatment pulmonary function tests were included. Paired t-tests were conducted. We also conducted subgroup analysis.
Results
Thirty-seven patients were included. Median age was 73 years. No statistical difference between mean pre- and post-CyberKnife pulmonary function tests was found.
Discussion
We observed that CyberKnife better preserves lung function status compared to current standards of care. It has shown to have very minimal side effects.
Introduction
More cancer patients die of lung cancer than of any other cancer.Citation1,Citation2 Early detection and treatment has shown overall improved outcomes in patients with lung cancer.Citation3,Citation4 The current standard of care for early stage non-small cell lung cancer (NSCLC) is invasive local control through surgical resection typically by lobectomy.Citation3 Significant decrease in pulmonary function after lobectomy has been noted in earlier studies.Citation5,Citation6 Win et al found that NSCLC patients who underwent lobectomy “suffered a significant reduction of pulmonary reserve” and lost a great deal of lung function and exercise capacity.Citation6 Functional lung status was measured using pulmonary function tests (PFT) in these studies.
For patients with stage 1 NSCLC who are inoperable or do not want to undergo surgery, external beam radiotherapy is the next best treatment as per the current standards. However, conventional radiotherapy has a high local failure rate of 6.4%–70% and has an estimated five-year overall survival rate of 21% ± 8%.Citation7 Symptomatic radiation pneumonitis is present in 5% to 30% of patients receiving radiotherapy for thoracic malignancies. In addition, 50% to 90% of patients experience declines in pulmonary function test measurements.Citation8–Citation13 The decrease in lung function in both surgical and radiotherapy therapy patients is very significant considering that most lung cancer patients already have poor lung function as most of them also have a history of smoking. Reducing the morbidity of treatment could possibly improve the quality of life in the survivors. There have been significant advances in treatment technology in recent years that will reduce damage to healthy lung tissue during NSCLC treatment by surgery or radiotherapy. One such treatment is CyberKnife.
CyberKnife is a noninvasive, highly specific radiological method of treating cancer tissue with relative preservation of the surrounding healthy tissues. It has been approved and used to treat early stage NSCLC with excellent results. CyberKnife has the unique ability to track dynamic targets that move with breathing. Thus it limits radiation exposure and damage to normal tissue.Citation14 Despite its great promise in treatment of lung cancer, no previous studies have specifically documented CyberKnife’s effect on pulmonary function studies. This study aims to confirm that in treatment of lung cancer, especially early stage, CyberKnife preserves lung function better than the current standard of care. The objective is to compare pre- and post-PFTs of patients treated with CyberKnife for lung cancer and ascertain how much lung function is preserved after the treatment.
Methods and materials
This is an Internal Review Board-approved, retrospective, observational cohort study of patients diagnosed with lung cancer to determine if there are differences in lung function before and after radiosurgery using CyberKnife. Pulmonary function tests were performed on the group before CyberKnife treatment and repeated 3–4 months after treatment.
We included patients diagnosed with primary or metastatic lung cancer who opted for CyberKnife treatment and had pre- and post-treatment pulmonary function tests. We excluded patients who did not fulfill the above criteria.
Abstracted data was entered into a Microsoft Access database and transferred to SPSS statistical software (v 20.0; IBM Corporation, Armonk, NY). Analysis included generation of descriptive statistics to adequately describe the sample. We also conducted paired t-tests to determine differences in pulmonary function data pre- and postoperatively (at 3 to 4 months). In addition, we conducted subgroup analysis based on gender, location, and stage of tumor. We compared eleven parameters of pulmonary function tests including: forced vital capacity (FVC), forced expiratory volume in 1 second (FEV1), FEV1/FVC ratio, forced expiratory flow 25%–75%, forced inspiratory vital capacity, slow vital capacity, inspiratory capacity, expiratory reserve volume, diffusing capacity of the lung for carbon monoxide, diffusion capacity corrected for alveolar volume, and alveolar volume.
Results
Thirty-seven patients were included in the study. The median age of the group was 73 years (). Approximately 49% of the subjects were female, while 51% were males. Three patients were given 5000 cGy in five divided fractions and 34 patients received 6000 cGy in five divided fractions. All the patients had smoking history. Stage 1 cancer was documented in 22 patients, stage 2 in two patients, stage 3 in five patients and stage 4 cancer in eight patients. The location of the tumors is mentioned in .
Table 1 Patient characteristics
Paired t-tests indicated that there was no statistical difference between pre-CyberKnife and post-CyberKnife treatment in terms of mean PFTs for the overall group () and for subgroups based on gender and tumor location.
Table 2 Comparison of pulmonary function tests pre- and post-CyberKnife treatment
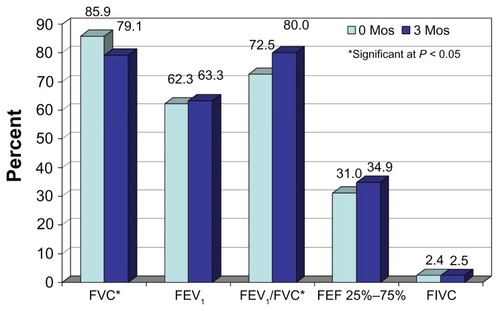
Analysis of subgroups based on stage indicate that stage 4 PFTs were significantly decreased for FVC, but significantly increased for the FEV1/FVC ratio, at 3 months compared to zero months ().
Figure 1 Comparison of mean pulmonary function tests before and 3–4 months after CyberKnife treatment in a stage 4 patient.
Abbreviations: Mos, months; FVC, forced vital capacity; FEV1, forced expiratory volume in 1 second; FEF, forced expiratory flow; FIVC, forced inspiratory vital capacity.
Discussion
CyberKnife treatment has been shown to be very effective for stage 1 NSCLC in multiple studies published in last few years.Citation15–Citation19 In our study, we observed that CyberKnife is successful in preserving lung function status as was measured by pulmonary function tests. This observation supports the emerging role of CyberKnife in lung cancer management.
Our results are in line with the conclusions of Stephans et al, who studied Novalis treatment (another stereotactic body radiation therapy) and found no significant differences in PFT pre- and posttreatment.Citation20 In Novalis treatment usually an abdominal compression devise is used to limit patients’ respiration, increasing patient discomfort. CyberKnife treatment does not need any method to limit breathing because of its tumor-tracking ability. Collins et al reported similar results for FVC and FEV1.Citation19 They also reported other side effects of CyberKnife treatment being pneumothorax and radiation pneumonitis. They did show a decrease in diffusing capacity of the lung for carbon monoxide at 6 months in the treated patients.Citation19 We did not see any such decrease at 3 months. We will continue to collect long-term follow-up data on our patients to determine if any changes in lung function occur longitudinally.
Most of the patients in the study were referred to a radiation oncology department after they were considered not eligible for surgery or the patient opted for radiation treatment. CyberKnife was offered to these patients because of decreased duration of treatment, convenience to the patient, and possibility of decreased damage to normal lung tissue.
The small sample size, nonrandomization, and retrospective nature of our study are certain limitations of our study and interpretation of the results should be made with caution. Prospective randomized trials comparing CyberKnife to conventional radiotherapy, other types of stereotactic body radiation therapies, and surgical treatments could further clarify the role of CyberKnife treatment.
Conclusion
In our study, we observed that CyberKnife was successful in preserving lung functions at 3–4 months, unlike the current standards of care, and also has a better side-effect profile. Compared to other methods of stereotactic body radiotherapy, it is more comfortable, as it does not need any methods or devices to restrict the patient. The CyberKnife has proved to be a safe and effective treatment. Our study is limited by a small sample size and the results should be interpreted with caution. More research is needed in this field.
Authors’ contributions
YHK is the principal author and designed the study. RA is the first author and contributed in data collection, literature search, and manuscript writing. AP, KL, SB, and SV contributed in study design and data collection. PS contributed in data collection and manuscript writing. JC contributed in study design and data analysis.
Authors’ information
YHK is a radiation oncologist at Seton Cancer Institute in Saginaw, Michigan. RA and PS are third year internal medicine residents at Synergy Medical Education Alliance/MSUCHM. AP, KL, SB, and SV are medical students at Michigan State University. JC is a research manager at Synergy Medical Education Alliance/MSUCHM.
Acknowledgments
Rishi Agarwal wishes to thank Dr Babu Paidipaty, a pulmonologist who helped in the understanding of PFTs and was instrumental in manuscript writing. RA also wants to thank Dr Ernie Balcueva who helped in manuscript writing, and Carol Wahl, an administrator at Seton Cancer Institute who was instrumental in data collection.
Disclosure
Dr Kim is a radiation oncologist at Seton Cancer Institute and uses CyberKnife for his patients. The authors report no conflicts of interest in this work.
References
- ParkinDMBrayFFerlayJPisaniPGlobal cancer statistics, 2002CA Cancer J Clin20055527410815761078
- JemalASiegelRXuJWardECancer statistics, 2010CA Cancer J Clin201060527730020610543
- GoldstrawPCrowleyJChanskyKfor the International Association for the Study of Lung Cancer International Staging Committee; Participating InstitutionsThe IASLC Lung Cancer Staging Project: proposals for the revision of the TNM stage groupings in the forthcoming (seventh) edition of the TNM Classification of malignant tumoursJ Thorac Oncol20072870671417762336
- AsamuraHGoyaTKoshiishiYfor Japanese Joint Committee of Lung Cancer RegistryA Japanese Lung Cancer Registry study: prognosis of 13,010 resected lung cancersJ Thorac Oncol200831465218166840
- WangJSAbboudRTWangLMEffect of lung resection on exercise capacity and on carbon monoxide diffusing capacity during exerciseChest2006129486387216608931
- WinTGrovesAMRitchieAJWellsFCCaffertyFLarocheCMThe effect of lung resection on pulmonary function and exercise capacity in lung cancer patientsRespir Care200752672072617521461
- QiaoXTullgrenOLaxISirzénFLewensohnRThe role of radiotherapy in treatment of stage I non-small cell lung cancerLung Cancer200341111112826306
- MarksLBFanMCloughRRadiation-induced pulmonary injury: symptomatic versus subclinical endpointsInt J Radiat Biol200076446947510815626
- AllenAMCzerminskaMJännePAFatal pneumonitis associated with intensity-modulated radiation therapy for mesotheliomaInt J Radiat Oncol Biol Phys200665364064516751058
- KahánZCsenkiMVargaZThe risk of early and late lung sequelae after conformal radiotherapy in breast cancer patientsInt J Radiat Oncol Biol Phys200768367368117350177
- KongFMHaymanJAGriffithKAFinal toxicity results of a radiation-dose escalation study in patients with non–small-cell lung cancer (NSCLC): Predictors for radiation pneumonitis and fibrosisInt J Radiat Oncol Biol Phys20066541075108616647222
- YomSSLiaoZLiuHHInitial evaluation of treatment-related pneumonitis in advanced-stage non–small-cell lung cancer patients treated with concurrent chemotherapy and intensity-modulated radiotherapyInt J Radiat Oncol Biol Phys20076819410217321067
- MaJZhangJZhouSAssociation between RT-induced changes in lung tissue density and global lung functionInt J Radiat Oncol Biol Phys200974378178919084355
- GibbsICLooBWJrCyberKnife stereotactic ablative radiotherapy for lung tumorsTechnol Cancer Res Treat20109658959621070081
- BrownWTWuXFayadFCyberKnife radiosurgery for stage I lung cancer: results at 36 monthsClin Lung Cancer20078848849217922973
- VahdatSOermannEKCollinsSPCyberKnife radiosurgery for inoperable stage IA non-small cell lung cancer: 18F-fluorodeoxyglucose positron emission tomography/computed tomography serial tumor response assessmentJ Hematol Oncol20103620132557
- Van der Voort van ZypNCPrévostJBHoogemanMSStereotactic radiotherapy with real-time tumor tracking for non-small cell lung cancer: clinical outcomeRadiother Oncol200991329630019297048
- CollinsBTEricksonKReichnerCARadical stereotactic radiosurgery with real-time tumor motion tracking in the treatment of small peripheral lung tumorsRadiat Oncol200723917953752
- CollinsBTVahdatSEricksonKRadical CyberKnife radiosurgery with tumor tracking: an effective treatment for inoperable small peripheral stage I non-small cell lung cancerJ Hematol Oncol20092119149899
- StephansKLDjemilTReddyCAComprehensive analysis of pulmonary function Test (PFT) changes after stereotactic body radiotherapy (SBRT) for stage I lung cancer in medically inoperable patientsJ Thorac Oncol20094783884419487961