
Abstract
Purpose
The purpose of the current study was to analyze the effect of type 2 diabetes mellitus (T2DM) on the short-term outcomes and prognosis of stage I–III colorectal cancer (CRC) undergoing primary surgery.
Methods
Patients who underwent primary CRC surgery were retrospectively collected from Jan 2011 to Jan 2020 in a single clinical center. The short-term outcomes and prognosis were compared between T2DM group and non-T2DM group using propensity score matching (PSM) analysis.
Results
A total of 4250 patients were included in this study. There were 521 patients with T2DM and 3729 patients without T2DM. After 1:1 ratio PSM, there were 519 T2DM patients and 519 non-T2DM patients left in this study. No significant difference was found in baseline information after PSM (p>0.05). T2DM had higher overall complications (p=0.033) after PSM in terms of short-term outcomes. As for prognosis, T2DM group had worse overall survival (OS) in all stages (p=0.044), stage I (p=0.009) and stage II (p=0.021) of CRC and T2DM group had worse disease-free survival (DFS) than non-T2DM group in stage I (p=0.008) of CRC before PSM. However, T2DM did not affect the overall survival (OS) or disease-free survival (DFS) on different stages of CRC after PSM (p>0.05). Moreover, T2DM was not an independent predictor of OS or DFS (p>0.05).
Conclusion
T2DM increased overall complications after primary CRC surgery. However, T2DM might not affect OS and DFS of stage I–III CRC patients.
Introduction
Colorectal cancer (CRC) is the third leading cause of death and the fourth most common cancer in the world.Citation1 More than 900,000 people die every year because of CRC.Citation2 In addition, the number of CRC patients is expected to increase in the future,Citation3 and surgery is still the main treatment for CRC.Citation4,Citation5
Type 2 diabetes mellitus (T2DM) causes a significant burden on patients and society globally,Citation6 and T2DM accounts for increased morbidity and mortality.Citation7 The number of T2DM patients is expected to reach 700 million in 2045.Citation8
Cancer and T2DM are two global public health problems and are also regarded as the world’s major lethal and disabling diseases.Citation9 They share various common risk factors (high blood pressure, obesity, hyperlipidemia) and have a similar etiological mechanism.Citation10,Citation11
As previous studies reported, T2DM could increase the incidence of CRC.Citation12 However, the effect of T2DM on CRC remains controversial.Citation13,Citation14 Furthermore, there have been no propensity score matching (PSM) studies concerning the relationship between CRC and T2DM. Therefore, the purpose of the current study was to analyze the effect of T2DM on the short-term outcomes and prognosis of CRC patients undergoing primary surgery using PSM analysis.
Methods
Patients
Patients who underwent primary CRC surgery were retrospectively collected from Jan 2011 to Jan 2020 in a single clinical center. This study was conducted in accordance with the World Medical Association Declaration of Helsinki. Ethical approval from the First Affiliated Hospital of Chongqing Medical University board was obtained (2021-336) and all the patients signed informed consent.
Inclusion and Exclusion Criteria
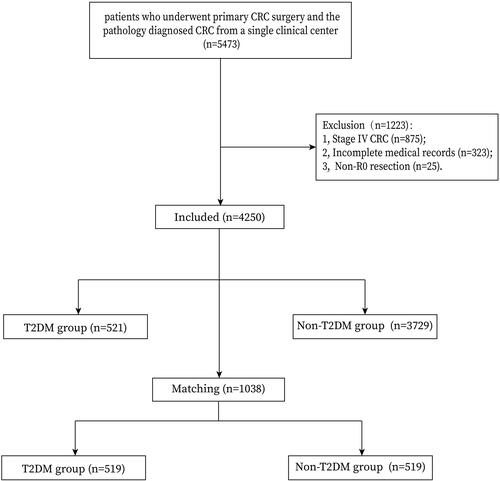
We included the patients who underwent primary CRC surgery and the pathology diagnosed CRC from a database of a single clinical center (n=5473). The exclusion criteria were as follows: 1) stage IV CRC (n=875); 2) incomplete medical records (n=323); and 3) non-R0 resection (n=25). Finally, a total of 4250 patients were included in the current study.
Surgery Management
All patients underwent radical resection according to the clinical guideline and total mesorectal excision or complete mesocolic excision was performed, and the pathology confirmed R0 resection. Patients were regularly followed up every 3 months for the first 3 years and every 6 months for the following 2 years.
Definitions
The tumor node metastasis (TNM) stage was diagnosed according to the AJCC eighth edition.Citation15 Overall survival (OS) was defined as the time from primary CRC surgery to the last follow-up (when patients were alive) or death. Disease-free survival (DFS) was defined as the time from primary CRC surgery to recurrence, death or last follow-up (when patients were alive). The complications were defined according to the Clavien–Dindo classification,Citation16 and major complications were defined as ≥III classification complications.
Data Collection
Patient information was retrospectively collected from inpatient and outpatient system, and the follow-up information was collected from the outpatient system and telephone interviews. The peri-operative information included age, sex, body mass index (BMI), smoking, drinking, family history, hypertension, coronary heart disease (CHD), adjuvant therapy, tumor stage and tumor location. The short-term outcomes included operation time, blood loss, retrieved lymph nodes, hospital stay, overall complications, major complications, postoperative 30-day death, reoperation and anastomotic leakage. The prognosis included OS and DFS.
PSM
To minimize the bias of baseline information, PSM was conducted between T2DM group and non-T2DM group. Nearest neighbor matching was performed without replacement at a 1:1 ratio and a caliper width with a 0.01 standard deviation was specified. The baseline information was matched including age, sex, BMI, smoking, drinking, family history, hypertension, CHD, adjuvant therapy, tumor location and tumor stage.
Statistical Analysis
Continuous variables are expressed as the mean ± SD, and independent-sample t-test was used to compare the difference between T2DM group and non-T2DM group. Frequency variables are expressed as n (%), and Chi-square test or Fisher’s exact test was used. The Kaplan–Meier curve was conducted to compare T2DM on different pathological stages, and Cox regression analyses were performed to identify independent predictive factors for OS and DFS. Data were analyzed using SPSS (version 22.0) statistical software. A bilateral p value <0.05 was considered statistically significant.
Results
Patients
A total of 4250 patients were included in this study according to the inclusion and exclusion criteria. There were 521 patients with T2DM and 3729 patients without T2DM. After 1:1 ratio PSM, there were 519 T2DM patients and 519 non-T2DM patients left in this study. The flow chart of inclusion, exclusion and PSM is shown in .
Figure 1 Flow chart of patient selection.
Baseline Information
Baseline information was compared between T2DM and non-T2DM groups, and T2DM group had an older age (p=0.000), higher BMI (p=0.000), higher portion of hypertension (p=0.000), higher portion of CHD (p=0.000) and lower portion of adjuvant therapy (p=0.011) before PSM. However, no significant difference was found after PSM in terms of age, sex, BMI, smoking, drinking, family history, hypertension, CHD, adjuvant therapy, tumor location or tumor stage (p>0.05) ().
Table 1 Baseline Characteristics Before and After PSM
Short-Term Outcomes
The short-term outcomes including operation time, blood loss, retrieved lymph nodes, hospital stay, overall complications, major complications, postoperative 30-day death, reoperation and anastomotic leakage were compared between T2DM and non-T2DM group. T2DM group had longer hospital stay (p=0.002), higher overall complications (p=0.000) and higher anastomotic leakage (p=0.022) before PSM. After PSM, T2DM had higher overall complications (p=0.033) ().
Table 2 Short-Term Outcomes Before and After PSM
Univariate and Multivariate Analyses of OS
The median follow-up time was 37 (1–114) months, univariate and multivariate analyses were conducted to find the predictors for OS of the 1038 patients after PSM. In univariate analysis, age (p=0.000, HR=2.007, 95% CI=1.486–2.710), BMI (p=0.008, HR=0.658, 95% CI=0.484–0.895), tumor stage (p=0.000, HR=1.556, 95% CI=1.253–1.931), overall complications (p=0.000, HR=1.898, 95% CI=1.407–2.561), major complications (p=0.000, HR=2.940, 95% CI=1.635–5.287) and anastomotic leakage (p=0.007, HR=2.542, 95% CI=1.298–4.979) were predictors; however, T2DM was not a predictor (p=0.764, HR=0.956, 95% CI=0.712–1.283). In multivariate analysis, age (p=0.000, HR=1.843, 95% CI=1.350–2.515), BMI (p=0.029, HR=0.706, 95% CI=0.516–0.965), tumor stage (p=0.000, HR=1.587, 95% CI=1.273–1.979), overall complications (p=0.016, HR=1.496, 95% CI=1.077–2.077) and major complications (p=0.010, HR=2.767, 95% CI=1.270–6.029) were independent predictors for OS ().
Table 3 Univariate and Multivariate Analyses of Overall Survival (After PSM)
Univariate and Multivariate Analyses of DFS
As for DFS, in univariate analysis, age (p=0.000, HR=1.747, 95% CI=1.325–2.303), BMI (p=0.019, HR=0.714, 95% CI=0.538–0.947), tumor stage (p=0.000, HR=1.796, 95% CI=1.447–2.229), overall complications (p=0.001, HR=1.622, 95% CI=1.221–2.155), major complications (p=0.002, HR=2.506, 95% CI=1.398–4.494) and anastomotic leakage (p=0.025, HR=2.154, 95% CI=1.103–4.208) were predictors; however, T2DM was not a predictor (p=0.353, HR=0.878, 95% CI=0.667–1.155). In multivariate analysis, age (p=0.001, HR=1.656, 95% CI=1.245–2.204), tumor stage (p=0.000, HR=1.541, 95% CI=1.258–1.888) and major complications (p=0.015, HR=2.551, 95% CI=1.198–5.431) were independent predictors for DFS ().
Table 4 Univariate and Multivariate Analyses of Disease-Free Survival (After PSM)
Prognosis in Different Tumor Stages
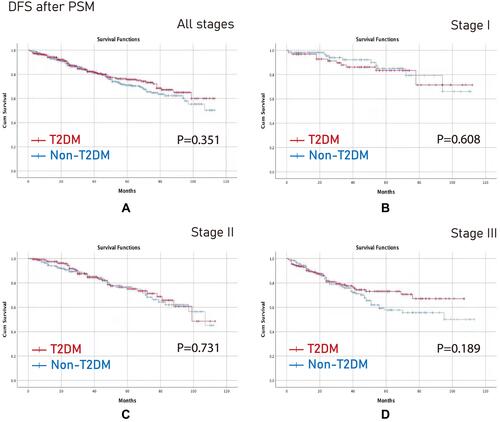
To analyze the effect of T2DM on prognosis on different stages of CRC, the Kaplan–Meier curve was conducted before and after PSM. Before PSM, T2DM group had worse OS in all stages (p=0.044), stage I (p=0.009) and stage II (p=0.021) (), and in terms of DFS, T2DM group had worse DFS than non-T2DM group in stage I (p=0.008) (). However, there were no difference in all stages, stage I, stage II and stage III in terms of OS or DFS after PSM (p>0.05) ( and ).
Figure 2 OS before PSM. (A) All stages; (B) Stage I; (C) Stage II; (D) Stage III.
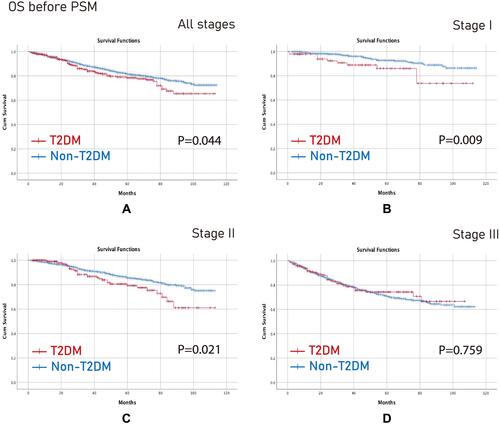
Figure 3 DFS before PSM. (A) All stages; (B) Stage I; (C) Stage II; (D) Stage III.
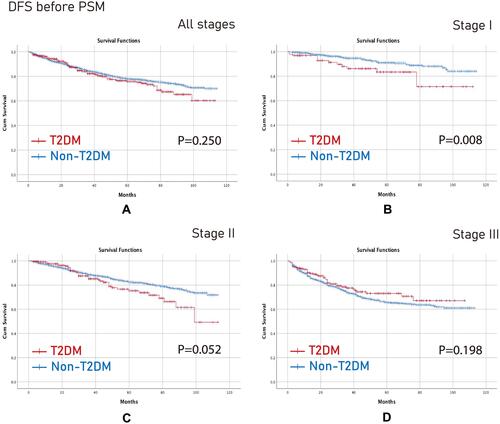
Figure 4 OS after PSM. (A) All stages; (B) Stage I; (C) Stage II; (D) Stage III.
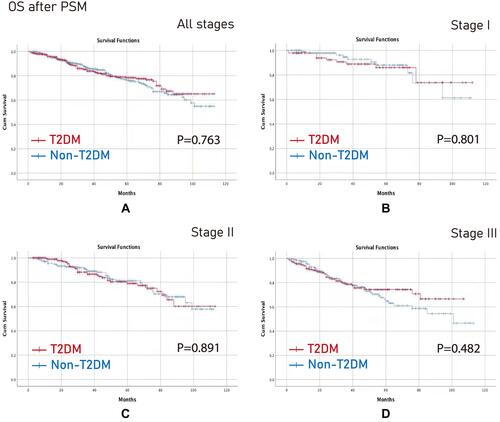
Figure 5 DFS after PSM. (A) All stages; (B) Stage I; (C) Stage II; (D) Stage III.
Discussion
In this study, T2DM had higher overall complications after PSM. As for prognosis, T2DM did not affect the OS or DFS on different stages of CRC after PSM, furthermore, T2DM was not an independent predictor of OS or DFS.
T2DM increased the global medical burden and economic burden,Citation6,Citation7 and furthermore, T2DM could increase the incidence of digestive cancers including esophageal cancer,Citation17 gastric cancerCitation18 and CRC.Citation12 However, there remained controversial about the outcomes of T2DM on CRC. Some studies reported that T2DM affected OS or DFS,Citation13,Citation14 a meta-analysis also reported that CRC patients with concurrent T2DM had worse DFS.Citation19 However, other studies reported its negative influence.Citation20–Citation22
The mechanism of the outcomes between CRC and T2DM remained unclear, but some hypotheses have been reported. T2DM might enhance the chemo-resistance of CRC and hyperglycemic status affected the sensitivity to chemotherapy through multiple regulatory routes.Citation23,Citation24 Epidemiological studies reported metformin improved OS and DFS. Metformin enhanced response to radiotherapy and chemotherapy through synergistic interactions, indicating that it might help induce tumor regression.Citation25,Citation26
PSM analysis is a statistical technique, which can deal with confounding bias and mimic a randomized clinical trial, improving the level of evidence in studies.Citation27 As far as we know, there were no related PSM studies about T2DM and CRC, and this is the first study to analyze the potential effect of T2DM on CRC using PSM.
In this study, we analyzed the differences in surgical outcomes between T2DM group and non-T2DM group. It was found that the T2DM group had higher overall complications before and after PSM. Yap et alCitation28 reported higher overall complications and longer hospital stay in patients with T2DM, and higher complications were reported in another study as well.Citation29 The probable reason was that T2DM had poorer healing or comorbid with cardiovascular diseases.Citation28 Therefore, for surgeons, adequate perioperative management should be done for patients with concurrent CRC and T2DM.
There were many factors that affected the prognosis of CRC, including age, tumor stage, and complications.Citation30–Citation32 In this study, we had the similar findings consistent with previous studies. In this study, T2DM was not a predictive factor in multivariate analysis. Furthermore, we examined T2DM at different stages of CRC to explore the exact impact of T2DM on OS and DFS. T2DM group had worse OS in all stages, stage I and stage II CRC and T2DM group had worse DFS than non-T2DM group in stage I CRC before PSM. We speculated that the possible reason was that patients had a longer OS in early tumor stage, T2DM and its related comorbidities might affect the prognosis. However, in advanced tumor stage, the tumor itself might affect the prognosis.
However, T2DM did not affect the OS or DFS at different stages of CRC after PSM, which represented that T2DM might not affect the prognosis of stage I–III CRC. Possible reasons for the null relationship between T2DM and CRC included duration and severity of T2DM, the type of T2DM medication used might be another reason.Citation21 Further studies are needed in the future.
There were some limitations in this study. First, this was a retrospective single-center study; Second, the course and severity of T2DM were lacking, which might affect the outcome of CRC; Third, metformin use was another factor for T2DM, which needed to be analyzed in the future; Fourth, the follow-up time was relatively short. Therefore, larger sample size and multicenter prospective randomized controlled trials should be conducted in the following experiments.
Conclusion
T2DM increased overall complications after primary CRC surgery. However, T2DM might not affect OS or DFS of CRC patients. Furthermore, T2DM did not affect the prognosis at different stages of CRC after PSM. Therefore, surgeons should be cautious when patients were with concurrent CRC and T2DM.
Disclosure
The authors report no conflicts of interest in this work.
Additional information
Funding
References
- Rawla P, Sunkara T, Barsouk A. Epidemiology of colorectal cancer: incidence, mortality, survival, and risk factors. Prz Gastroenterol. 2019;14(2):89–103. doi:10.5114/pg.2018.81072
- Dekker E, Tanis PJ, Vleugels JLA, Kasi PM, Wallace MB. Colorectal cancer. Lancet. 2019;394(10207):1467–1480. doi:10.1016/S0140-6736(19)32319-0
- Arnold M, Sierra MS, Laversanne M, et al. Global patterns and trends in colorectal cancer incidence and mortality. Gut. 2017;66(4):683–691. doi:10.1136/gutjnl-2015-310912
- Cheng YX, Tao W, Zhang H, Peng D, Wei ZQ. Does liver cirrhosis affect the surgical outcome of primary colorectal cancer surgery? A meta-analysis. World J Surg Oncol. 2021;19(1):167. doi:10.1186/s12957-021-02267-6
- Watanabe T, Momosaki R, Suzuki S, Abo M. Preoperative rehabilitation for patients undergoing colorectal cancer surgery: a retrospective cohort study. Support Care Cancer. 2020;28(5):2293–2297. doi:10.1007/s00520-019-05061-z
- Li Y, Yan Y, Dai H, et al. Mastery of type 2 diabetes prevention and treatment knowledge by general practitioners in Shanghai: a cross-sectional study. BMC Fam Pract. 2021;22(1):189. doi:10.1186/s12875-021-01538-1
- Roy A, Sahoo J, Kamalanathan S, et al. Diabetes and pancreatic cancer: exploring the two-way traffic. World J Gastroenterol. 2021;27(30):4939–4962. doi:10.3748/wjg.v27.i30.4939
- Chatterjee S, Khunti K, Davies MJ. Type 2 diabetes. Lancet. 2017;389(10085):2239–2251. doi:10.1016/S0140-6736(17)30058-2
- Klil-Drori AJ, Azoulay L, Pollak MN. Cancer, obesity, diabetes, and antidiabetic drugs: is the fog clearing? Nat Rev Clin Oncol. 2017;14(2):85–99. doi:10.1038/nrclinonc.2016.120
- Abudawood M. Diabetes and cancer: a comprehensive review. J Res Med Sci. 2019;24:94. doi:10.4103/jrms.JRMS_242_19
- Giovannucci E, Harlan DM, Archer MC, et al. Diabetes and cancer: a consensus report. Diabetes Care. 2010;33(7):1674–1685. doi:10.2337/dc10-0666
- Guraya SY. Association of type 2 diabetes mellitus and the risk of colorectal cancer: a meta-analysis and systematic review. World J Gastroenterol. 2015;21(19):6026–6031. doi:10.3748/wjg.v21.i19.6026
- Zhu B, Wu X, Wu B, et al. The relationship between diabetes and colorectal cancer prognosis: a meta-analysis based on the cohort studies. PLoS One. 2017;12(4):e0176068. doi:10.1371/journal.pone.0176068
- Petrelli F, Ghidini M, Rausa E, et al. Survival of colorectal cancer patients with diabetes mellitus: a meta-analysis. Can J Diabetes. 2021;45(2):186–197.e2. doi:10.1016/j.jcjd.2020.06.009
- Weiser MR. AJCC 8th edition: colorectal cancer. Ann Surg Oncol. 2018;25(6):1454–1455. doi:10.1245/s10434-018-6462-1
- Clavien PA, Barkun J, de Oliveira ML, et al. The Clavien-Dindo classification of surgical complications: five-year experience. Ann Surg. 2009;250(2):187–196. doi:10.1097/SLA.0b013e3181b13ca2
- Xu B, Zhou X, Li X, Liu C, Yang C. Diabetes mellitus carries a risk of esophageal cancer: a meta-analysis. Medicine. 2017;96(35):e7944. doi:10.1097/MD.0000000000007944
- Peng D, Cheng YX, Zhang W. Does Roux-en-Y construction really bring benefit of type 2 diabetes mellitus remission after gastrectomy in patients with gastric cancer? A systematic review and meta-analysis. Diabetes Ther. 2020;11(12):2863–2872. doi:10.1007/s13300-020-00934-7
- Mills KT, Bellows CF, Hoffman AE, Kelly TN, Gagliardi G. Diabetes mellitus and colorectal cancer prognosis: a meta-analysis. Dis Colon Rectum. 2013;56(11):1304–1319. doi:10.1097/DCR.0b013e3182a479f9
- Jullumstrø E, Kollind M, Lydersen S, Edna TH. Diabetes mellitus and outcomes of colorectal cancer. Acta Oncol. 2009;48(3):361–367. doi:10.1080/02841860802637765
- Amshoff Y, Maskarinec G, Shvetsov YB, et al. Type 2 diabetes and colorectal cancer survival: the multiethnic cohort. Int J Cancer. 2018;143(2):263–268. doi:10.1002/ijc.31311
- Ahmadi A, Noroozi M, Pourhoseingholi MA, et al. Effect of metabolic syndrome and its components on survival in colorectal cancer: a prospective study. J Renal Inj Prev. 2015;4(1):15–19. doi:10.12861/jrip.2015.05
- Brown JC, Zhang S, Ou FS, et al. Diabetes and clinical outcome in patients with metastatic colorectal cancer: CALGB 80405 (alliance). JNCI Cancer Spectr. 2019;4(1):pkz078. doi:10.1093/jncics/pkz078
- Ma YS, Yang IP, Tsai HL, et al. High glucose modulates antiproliferative effect and cytotoxicity of 5-fluorouracil in human colon cancer cells. DNA Cell Biol. 2014;33(2):64–72. doi:10.1089/dna.2013.2161
- Saito A, Kitayama J, Horie H, et al. Metformin changes the immune microenvironment of colorectal cancer in patients with type 2 diabetes mellitus. Cancer Sci. 2020;111(11):4012–4020. doi:10.1111/cas.14615
- Cheng HC, Chang TK, Su WC, Tsai HL, Wang JY. Narrative review of the influence of diabetes mellitus and hyperglycemia on colorectal cancer risk and oncological outcomes. Transl Oncol. 2021;14(7):101089. doi:10.1016/j.tranon.2021.101089
- Lonjon G, Boutron I, Trinquart L, et al. Comparison of treatment effect estimates from prospective nonrandomized studies with propensity score analysis and randomized controlled trials of surgical procedures. Ann Surg. 2014;259(1):18–25. doi:10.1097/SLA.0000000000000256
- Yap R, Wilkins S, Staples M, Oliva K, McMurrick PJ. The effect of diabetes on the perioperative outcomes of colorectal cancer surgery patients. PLoS One. 2016;11(12):e0167271. doi:10.1371/journal.pone.0167271
- Tan DJH, Yaow CYL, Mok HT, et al. The influence of diabetes on postoperative complications following colorectal surgery. Tech Coloproctol. 2021;25(3):267–278. doi:10.1007/s10151-020-02373-9
- Kido H, Kato S, Funahashi K, et al. The metabolic parameters based on volume in PET/CT are associated with clinicopathological N stage of colorectal cancer and can predict prognosis. EJNMMI Res. 2021;11(1):87. doi:10.1186/s13550-021-00831-5
- Peng D, Liu XY, Cheng YX, Tao W, Cheng Y. Improvement of diabetes mellitus after colorectal cancer surgery: a Retrospective Study of Predictive factors for type 2 diabetes mellitus remission and overall survival. Front Oncol. 2021;11:694997. doi:10.3389/fonc.2021.694997
- Pang QY, An R, Liu HL. Perioperative transfusion and the prognosis of colorectal cancer surgery: a systematic review and meta-analysis. World J Surg Oncol. 2019;17(1):7. doi:10.1186/s12957-018-1551-y