
Abstract
Background
Depression and anxiety are prevalent issues amongst individuals suffering from thoracic cancer. Gender differences in coping with thoracic cancer have a serious impact upon the management of emotional distress. The purpose of our study has been to assess sex variations in handling anxiety and depression, including the use of coping mechanisms and their relationship with respect to anxiety and depression.
Methods
This cross-sectional study registered 18 women and 22 men with non-metastatic lung cancer and operated upon. Pre-operatively and at one month post-operatively, the patients were assessed by means of scales (COPE, GAD-7 and PHQ-9).
Results
Post-operatively, the intensity of depression and anxiety was substantially greater in males than in females (p = 0.049, p = 0.042). Male individuals tended to use coping mechanisms of humour (p = 0.009) and restraint (p = 0.029) significantly more frequently than women. Moreover, in women, depression correlated significantly with denial and behavioural deactivation (rho = 0.465, p = 0.029, respectively, rho = 0.562, p = 0.006); whilst anxiety, similarly, correlated with positive interpretation, behavioural deactivation, and use of social-emotional support (rho = 0.484, p = 0.022, respectively, rho = 0.590, p = 0.004 and rho = 0.502, p = 0.017). Furthermore, in males, depression correlated significantly with mental deactivation, use of social-instrumental and social-emotional support (rho = 0.702, p = 0.001, respectively, rho = 0.505, p=0.033, and rho = 0.773 with p < 0.001), whilst anxiety correlated significantly with mental deactivation, denial, and use of social-emotional support (rho = 0.597, p = 0.009, respectively, rho = 0.553 with p = 0.017 and rho = 0.755, p < 0.001).
Conclusion
There were gender divergences in the use of coping mechanisms and the level of post-surgical anxiety and depression. We found significant positive relationships between some coping mechanisms and depression/anxiety. The patient’s gender governs the coping style, which in turn has bearing upon the post-operative evolution.
Introduction
Thoracic cancer comprises non-metastatic lung cancer, lung metastases, esophageal cancer, mediastinal tumours, bone tumours, as well as breast cancer. It is the most diagnosed cancer while also representing the prime cause of cancer death.Citation1 The most prevalent type of thoracic cancer is non-metastatic lung cancer; it is a severe condition habitually accompanied by a considerably reduced life expectancy, regardless of current medical progress.Citation2
Patients, upon being diagnosed with life-threatening ailments – such as cancer – with low life expectancy, undergo severe emotional stress.Citation3
Hence, it comes as no surprise that up to 40% of cancer patients have emotional disorders or experience symptoms of anxiety and depression.Citation4–Citation6
Current medical literature focuses chiefly upon surgery, chemotherapy, or radiotherapy as treatment options for tumours; however, the impact of psychological factors has mostly been overlooked.Citation7 In fact, psychological distress in cancer patients can engender a considerable reduction in their quality of life (QoL)Citation5,Citation8 even with improvements in the field of cancer treatment.Citation9
Distress Management Guideline from the National Comprehensive Cancer Network (NCCN) backs the systematic screening for psychological distress in cancer patients.Citation10,Citation11
Anxiety and depression are regularly encountered in psychological distress, considered as contributing to psychiatric morbidity, following the diagnosis of cancer.Citation12 Most cancer patients experience varying levels of psychological trouble, which shape the evolution of cancer.Citation13
Several studies purport that the extent of depression and anxiety varies considerably in relation to parameters, such as age, gender, and type of cancer.Citation5,Citation14,Citation15
In more than 50% of cases, women, and patients younger than 50 years old, had clinical and sub-clinical forms of anxiety and depression, whilst elderly patients had better emotional tolerance in handling the diagnosis.Citation5,Citation15 The inverse relationship between age and emotional distress in cancer patients can generally be explained by the greater functional impact of the condition upon the everyday life of younger patients and their belief that “they haven’t yet lived their life” compared to older people who may already have an impairment in daily functioning, have longer biographical history behind them and are better prepared cognitively or emotionally to accept the condition. As a matter of fact, immune depression can be brought about by anxiety and depression, negatively impacting the evolution of cancer.Citation15,Citation16
The American Psychiatric Association states that every individual answers differently to the diagnosis of a tumour, whether benign or malignant; while some may exhibit symptoms specific to anxiety or depression, others may suffer from both psychiatric conditions simultaneously.
Since the diagnosis of cancer and post-operative recovery create stressful states, one must turn towards the several coping mechanisms to manage the situation. Based upon their manner of interpreting the circumstances, as well as their coping style, individuals make different cognitive or behavioural attempts at managing novel trials.Citation17
It is widely considered that a pivotal link exists between coping strategies and the presence of anxiety or depression.Citation18–Citation20
Folkman and Lazarus (1984), the founders of the coping and stress theory, outlined coping as
constantly changing cognitive and behavioural efforts to manage specific external and internal demands that are appraised as taxing or exceeding the resources of the person and stress “as exposure to stimuli appraised as harmful, threatening, or challenging, that exceeds the individual’s capacity to cope.Citation17,Citation21
When it comes to coping and gender differences, anterior studies assert that men use problem-focused coping mechanisms predominantly, whilst making lesser use of emotion-focused coping mechanisms/avoidance coping styles, as compared to women, in non-clinical populations.Citation22–Citation25
Only few studies in medical literature – about the oncological population – analyse the distinctions in coping with disease with respect to gender.Citation26–Citation30
Considering the above-mentioned, the current investigation not only assessed the existence of gender differences in anxiety, depression and coping mechanisms used by patients with non-metastatic lung cancer who underwent surgery but also explored the relationship between coping and anxiety/depression.
Materials and Methods
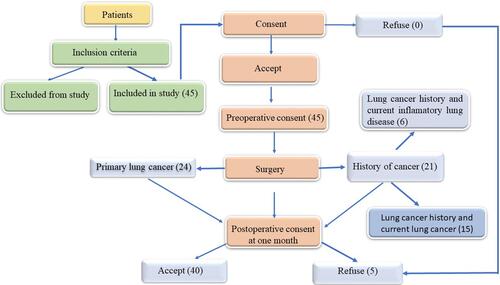
The health archives of the 40 patients identified with thoracic surgical pathology throughout November 2018 and November 2019 were examined pre-operatively and post-operatively. Data were collected from the Department of Thoracic Surgery of the Municipal Emergency Hospital of Timisoara, Romania. From the files, the following patient information was used: registration number, age, gender, address, marital status, education, occupation, smoking status, period and duration of hospital stay, complications, organ involvement, standard laboratory tests and result. All patients gave informed written consent for enrolment in our study ().
Figure 1 Flow diagram.
The study protocol, procedures and informed consent template were approved by the Ethics Committee of the Municipal Hospital of Timisoara and the Ethics Committee of “Victor Babes” University of Medicine and Pharmacy Timisoara.
These 40 patients were diagnosed with lung tumours of differing sizes and intervened surgically upon, using various minimally invasive or classical surgical techniques.
The conditions for inclusion in this study were:
Adult patients older than 18 years old at the time of study inclusion;
Inpatients scheduled at least 24 h before surgery;
Patients diagnosed by chest CT and requiring thoracic surgery for curative purposes
Patients who were aware of the study methods and settled to join and sign the Informed Consent Form (ICF).
The exclusion criteria for patients diagnosed with other invasive methods were:
Tomographically guided transthoracic puncture;
Mediastinoscopy with biopsy;
Fibrobronchoscopy with bronchial biopsy;
Positive cytological examination of the pleural fluid;
Supra-clavicular or latero-cervical ganglion biopsy;
The patient’s refusal to undergo surgery.
Criteria for excluding general patients:
Psychiatric disorders associated with poor memory status (such as psychoses, posttraumatic stress disorder, dissociative disorders or dementias) and compliance;
Severe cognitive deficit;
Metastatic cancer;
Patients known with various pathologies and unfavourable immediate prognosis;
Urgent chest surgery.
On the day of admission, all descriptive data were collected. 1 month after surgery, the patients completed the self-administered psychiatric questionnaires for coping, anxiety, and depression.
COPE Inventory: The COPE questionnaire is a valuable self-reporting means to evaluate the approaches that people utilise in coping with demanding or stressful life events; it was devised by Carver, Scheier, and Weintraub (1989).Citation31 The scale consists of 60 questions having responses graded on a scale of 1 to 4, whereby: 1 – I typically do not do this, 4 – I often do this. The questionnaire appraises 15 forms of coping; each of the 15 coping strategies gauged according to 4 elements. The 15 coping strategies/mechanisms, and the parameters related to each strategy, assessed by the COPE questionnaire are as follows: positive re-interpretation and growth, mental disengagement, venting of emotions, use of instrumental social support, active approach, denial, religious coping, humour, behavioural disengagement, restraint, use of emotional social support, substance use, acceptance, suppression of competing activities and planning. Greater scores denote more common use of the respective coping strategy.
Generalised Anxiety Disorder – 7 questionnaire (GAD-7) was made use of to identify and evaluate the manifestation and degree of anxiety disorder.Citation32 The GAD-7 scores of 0, 1, 2, and 3 correspond to the responses of “not at all”, ‘numerous days’, ‘beyond half the days’, and “nearly each day”, respectively; the scores being totalled for the 7 questions. The GAD-7 scores of 5, 10, and 15 serve as cut-offs for mild, moderate, and severe anxiety, respectively. When 10 is applied as the threshold score, GAD-7 has a specificity of 82% and a sensitivity of 89%.Citation33,Citation34
The Patient Health Questionnaire (PHQ) is a patient-completed adaptation of the PRIME-MD diagnostic method for widespread psychiatric disorders.Citation35 PHQ-9 comprises a segment on depression, weighing parameters (Diagnostic and Statistical Manual of Mental Disorders, 4th Edition) as “0” (never) to “3” (almost every day).Citation36,Citation37 PHQ-9 has 61% sensitivity and 94% specificity in adults. It can establish the existence of depressive distress and the severity of depressive symptoms with its nine items. Statistical processing was affected using SPSSv17. Scores were represented by the median value and the interquartile range (the SPSS software represents the IQR as a difference between the Q3 and Q1). Comparisons between 2 data series of scores were affected using the non-parametric Mann–Whitney U-Test and the correlations between these types of variables were gauged by utilising the non-parametric Spearman correlation. The results were deemed to be of significance for a value of p < 0.05.
Results
We analyzed the questionnaires, with the demographic characteristics of the 40 patients shown in . The differences between the proportions of men and women are non-significant for each demographic characteristic (p values are listed in ).
Table 1 Demographic Characteristics of the Patients
We investigated the 40 patients by comparing PHQ9 and GAD7 between women and men, both pre-operatively and post-operatively at 1 month. PHQ9 values were non-significantly increased in men pre-operatively (Mann–Whitney U-Test, p = 0.861), whilst being significantly increased post-operatively (p = 0.049).
GAD7 values were non-significantly increased in men pre-operatively (Mann–Whitney U-Test, p = 0.697), whilst being significantly increased post-operatively (p = 0.042).
In addition, both pre-operatively and post-operatively, anxiety as well as depression were higher in males than in females, these differences being significant even post-operatively illustrated by the data in . Post-operatively, we correlated the 15 coping mechanisms with GAD7 and PHQ9 separately for men and women as illustrated by the data in .
Table 2 Post-Operative Correlations of Coping Mechanism with PHQ9 and GAD7 Separately in Men and Women
Table 3 Descriptive Statistics for 40 Cancer Patients (18 Males, 22 Females)x
Men
In men, depression significantly positively correlated with mental disengagement, turning towards instrumental social support, and seeking emotional social support.
Moreover, anxiety positively correlated with mental disengagement, denial, and seeking emotional social support.
Women
In women, depression significantly positively correlated with behavioural disengagement as well as denial. In fact, anxiety also exhibited a similar correlation with positive interpretation, behavioural disengagement, and making use of emotional social support.
Considerable differences between the two genders – in terms of the degree of use of coping mechanisms – existed only for humour and restraint, signifying a greater usage of them by males, according to the data presented in . No significant differences were observed between the two sexes with respect to the other coping mechanisms evaluated with the COPE scale, apart from humor and abstinence.
Table 4 Degree of Use of Coping Mechanisms by Genderx
The 15 coping mechanisms ordered by gender and descending COPE score median are represented in .
Table 5 15 Coping Mechanisms Ordered by Gender and Descending COPE Score
Discussion
When considering the general population, it is widely accepted that anxiety and depression are predominant in women as compared to men.Citation38–Citation40
In our study, GAD 7-assessed anxiety and PHQ9-assessed depression, both pre-operatively and post-operatively, were observed to be higher in males than in females; these differences being statistically significant even post-operatively (p = 0.049, for depression; p = 0.042, for anxiety).
Our result is opposite to most existing studies on gender disparities of anxiety and depression in cancer or surgery patients; these had reported a notably higher prevalence or intensity of anxiety and depression in females relative to males, regardless of the cases being of neoplasm or surgery.Citation5,Citation41–Citation44
However, there have been studies on subjects exhibiting somatic disorders, in which the differences by gender were non-significant or the intensity of depression/anxiety was lesser in females.
According to Brezinka’s study involving 231 patients with myocardial infarction having undergone cardiac treatment for rehabilitation, the females exhibited added anxiety compared to men; however, any gender-related disparities in cases of depression were absent.Citation45
A subsequent study (Grace 2005) – which comprised 661 patients suffering from acute coronary syndrome – stated that the depression prevalence was not considerably greater in the female population.Citation46
Nonetheless, our results do concur with the findings of Van’t Spijker et al’s on cancer patients, whereby women were found to exhibit lower rates of emotional distress (anxiety and depression) than men.Citation47
While preceding studies essentially indicate a greater frequency and intensity of depression and anxiety in females, relative to males, the presence of results that do not concur, or sometimes disagree, has been attempted to be justified by numerous hypotheses.
One of these premises would be that females tend to be more open than males and are more amenable to expressing states of anxiety or depression.Citation48
In addition, men have more trouble communicating their feelings or necessity for assistance; they have a propensity to exhibit different symptoms under stress – such as fury, mania, aggression, and so on – which are in fact the symptoms of a depressive state.
The expectation of men to display strength and competitiveness, is in opposition to the possibility of showing emotions which might be perceived as weakness. Hegemonic masculinity can make it harder for men to acknowledge that they have psychological issues and hinders them from seeking help. The aptitude to request assistance when needed still appears to be associated with the female skill set.Citation49
In the face of a cancer diagnosis, including the mandatory therapeutic procedures, though the development of depression and anxiety generally tends to be understood in women, it is commonly ignored in men.Citation50 Considering such patterns, several authors have put forward “male-specific” assessment tools, which are used in the screening for depression in male cancer patients.Citation51
Yet, another premise would be that those men, at the beginning, perceive cancer as less menacing; this is owed, in part, to the high prevalence of prostate cancer, which is known to have a good overall prognosis.Citation5
In our study, we estimate that the anxiety and depression assessed in the patient group are closely correlated with two major stressful events: cancer diagnosis and surgery.
Regarding coping in the non-clinical population, it is deemed that men habitually use problem-focused or instrumental strategies to handle stressful happenings, whilst women are inclined towards the use of methods meant to alter their emotional reactions to stressful circumstances.Citation24,Citation38,Citation52,Citation53
Although most studies back the predominant use of emotion-oriented coping in women compared with men,Citation22,Citation23 some authors have not endorsed this difference among genders.Citation24
Regarding the coping divergences with respect to gender in cancer patients, as we mentioned in the introduction, there are few studies to analyse this aspect so far. In their case, the scales used were very diverse (Ways of Coping Checklist, the Mental Adjustment to Cancer (MAC), Coping Effectiveness Scale, the brief COPE scale), such that the results observed and described are challenging to equate with one another; hence, a satisfactory synthesis of them is complicated to devise.Citation26–Citation30
In our study, significant differences were noted between the two sexes regarding the extent of use of coping mechanisms only for humour and restraint, in the sense of their greater use by males. No significant gender differences were found in the other coping mechanisms evaluated by COPE.
Significantly higher use of humour by men than women in our study concurs with the result obtained by Oppegaard et al in a study based on subjects with lung or gastrointestinal cancer (277 females and 293 males). Using the brief COPE, they noted that women related considerably larger use of positive reframing, religion, instrumental support, self-distraction, denial, and venting, whilst men leaned preferentially towards the directions of humour and substance use.Citation30
Restraint, from COPE, is absent from the scales used in preceding studies but may be considered a form of active coping. In this context, our result would be contrary to previous studies that have reported in men with cancer, a generally greater tendency to use coping mechanisms of avoidance and abandonment.
As stated in his 1994 study, Fife reported that men used avoidant coping more often than women, whilst Goldzweig et al have noted in men, a hopelessness–helplessness coping manner or a fatalistic-acceptant coping disposition.Citation26,Citation27
According to our study, when it comes to the frequency of the types of coping mechanisms used, the religious approach was the principal coping mechanism employed by both sexes, without having any substantial difference between sexes in this regard.
The study by Fife and Jacobs-Lawson concluded that this coping mechanism was considerably more exercised by women than men.Citation26,Citation28
Our result corroborates, in a way, earlier research that reported religious coping as a crucial factor in cancer patients.Citation49,Citation54,Citation55
Overall, studies have claimed the religious approach as empowering, whilst constituting a helpful aspect in the experience of cancer by patients.Citation56,Citation57 Furthermore, it has been linked to diminished levels of depression and anxiety in cancer patients, in addition to improved acceptance of the disease.Citation58–Citation60
Indeed, it comes unanticipated that, by frequency, substance-use as a coping mechanism ranked last in both sexes. In Oppegard’s study, this coping mechanism was much more used by men than women.Citation30
A possible explanation for our result regarding this coping mechanism, would be the recent timing of the surgical intervention undergone by patients constituting the group, with them still being in recovery, as well as the recency of diagnosis announcement. (Surgery had also led to the diagnosis being confirmed and announced).
In men, depression correlated significantly positively with mental disengagement, making use of instrumental social support, and emotional social support, and anxiety also correlated significantly positively with mental disengagement, denial, and use of emotional social support.
In women, depression correlated significantly positively with denial and behavioural disengagement, while anxiety correlated significantly positively with behavioural disengagement, positive interpretation, and use of emotional social support.
Concrete research supports that the use of a particular style of coping varies by gender. The use of a coping style is a reaction to stress and represents a focal parameter that directly contributes to the pathogenesis of depression and anxiety amongst women.Citation61,Citation62
Although coping approaches that belong to the avoidant category – in handling stressful circumstances with secondary appearance of depression/anxiety – are deemed futile in both genders, emotion-focused coping strategies have shown fluctuating results.Citation63
Positive reassessment is tied to diminished negative affects, also forming an adaptive self-adjusting approach that is focused upon emotion.Citation64
Whilst emotion-focused coping may possess several benefits in acting in response to stressors, it also presents the drawback of heralding a psychopathological level with high functional deficiency.Citation65
In our study, positive interpretation, and growth (a mechanism that is included in emotion-focused coping according to the COPE scale adapted to the Romanian population), has shown a significantly positive correlation with anxiety in women, and has therefore proven to be maladaptive. This denotes an individual’s propensity to acquire advantage even from a traumatic situation. Consequently, the result of our study would be in line with studies that show emotion-focused strategies as being correlated with elevated levels of depression/anxiety.Citation42,Citation66,Citation67
In a likewise manner, avoidant coping mechanisms (denial, behavioural and mental disengagement) have also shown association with heightened levels of anxiety and depression in both women and men.
More distinctively, mental disengagement correlated significantly positively with depression and anxiety in men, whilst behavioural disengagement did so with depression and anxiety in women. Nonetheless, denial correlated positively only with anxiety in men and depression in women.
These results concur with those mentioned in existing medical literature on cancer patients, whereby avoidant coping is found to be responsible for elevated levels of depression/anxiety.Citation2,Citation68–Citation70
The use of emotional social support as a coping mechanism correlated significantly positively with both depression and anxiety in the case of men, while correlating with only anxiety in women. It is a method of coping where the individual is inclined to seek understanding, consideration or moral support from friends, relatives, as well as colleagues, so as to lessen distress. Use of instrumental social support was also significantly positively associated with the level of depression in men. In the present instance, it denotes the propensity to seek counsel and information, as well as material assistance required in taking action to improve the situation. Though it is deemed as being a type of active coping, this mechanism, together with the use of emotional-social support, forms part of the social-support coping style, in accordance with the COPE scale version for Romania, the coping style being cited as maladaptive in a few studies on patients suffering from lung cancer or COPD.Citation2,Citation71,Citation72
It should be noted that in our study, no statistically significant negative correlations were observed between the various coping mechanisms analysed with the COPE scale (version adapted to the Romanian population) and anxiety/depression. That is, no coping mechanism approached individually has been shown to be adaptive in the sense of being associated with a low level of anxiety or depression. Probably, the analysis of coping styles separated by sex would have revealed a beneficial association in this regard.
Conclusion
The main findings of our study reveal that there were sex distinctions in the employment of coping mechanisms and the level of post-operative depression and anxiety.
The impact of depression and anxiety is different depending on the patient’s gender. The patient’s gender determines the coping style, which in turn influences the post-operative evolution and the subsequent socio-professional re-insertion.
Also, certain coping mechanisms in both men and women correlated significantly positively with the intensity of depression/anxiety, proving, in this context, maladaptive in the control of these mental states.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of “Victor Babes” University of Medicine and Pharmacy Timisoara, Romania (protocol code no. 24 and date of approval 28.09.2018) and by the Ethics of Municipal Clinical Emergency Hospital of Timisoara (protocol code G-2737 and date of approval 25.09.2018).
Data Sharing Statement
The data presented in this study are available upon request from the corresponding author. The data are not publicly available because the database contains patient personal data.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Disclosure
The authors report no conflicts of interest in this work.
References
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. doi:10.3322/caac.21492
- Oancea C, Suciu C, Timar B, Papava I, Raica M, Burlacu O. The reciprocal relationship between coping mechanisms and lung cancer diagnosis: findings of a prospective study. Cancer Manag Res. 2018;10:33–40. doi:10.2147/CMAR.S148341
- Giese-Davis J, Waller A, Carlson LE, et al. Screening for distress, the 6th vital sign: common problems in cancer outpatients over one year in usual care: associations with marital status, sex, and age. BMC Cancer. 2012;12(1):441. doi:10.1186/1471-2407-12-441
- Caruso R, Nanni MG, Riba MB, Sabato S, Grassi L. The burden of psychosocial morbidity related to cancer: patient and family issues. Int Rev Psychiatry. 2017;29(5):389–402. doi:10.1080/09540261.2017.1288090
- Linden W, Vodermaier A, MacKenzie R, Greig D. Anxiety and depression after cancer diagnosis: prevalence rates by cancer type, gender, and age. J Affect Disord. 2012;141(2–3):343–351. doi:10.1016/j.jad.2012.03.025
- Mitchell AJ, Chan M, Bhatti H, et al. Prevalence of depression, anxiety, and adjustment disorder in oncological, haematological, and palliative-care settings: a meta-analysis of 94 interview-based studies. Lancet Oncol. 2011;12(2):160–174. doi:10.1016/S1470-2045(11
- Tang -L-L, Zhang Y-N, Pang Y, Zhang H-W, Song -L-L. Validation and reliability of distress thermometer in Chinese cancer patients. Chin J Cancer Res. 2011;23(1):54–58. doi:10.1007/s11670-011-0054-y
- Lim HA, Mahendran R, Chua J, Peh CX, Lim SE, Kua EH. The distress thermometer as an ultra-short screening tool: a first validation study for mixed-cancer outpatients in Singapore. Compr Psychiatry. 2014;55(4):1055–1062. doi:10.1016/j.comppsych.2014.01.008
- Hong JS, Tian J. Prevalence of anxiety and depression and their risk factors in Chinese cancer patients. Support Care Cancer. 2014;22(2):453–459. doi:10.1007/s00520-013-1997-y
- Lee H, Jacobsen PB, Ransom S. From the a implementation of NCCN distress management guidelines by member institutions. J Natl Compr Cancer Netw. 2007;5(1):99–103. doi:10.6004/jnccn.2007.0010
- Distress during cancer care.
- Thapa S, Sun H, Pokhrel G, Wang B, Dahal S, Yu S. Performance of distress thermometer and associated factors of psychological distress among Chinese cancer patients. J Oncol. 2020;2020:1–8. doi:10.1155/2020/3293589
- Hasan EM, Calma CL, Tudor A, et al. Coping, anxiety, and pain intensity in patients requiring thoracic surgery. J Pers Med. 2021;11(11):1221. doi:10.3390/jpm11111221
- Runcan R. Anxiety in adolescence: a literature review. in: innovative instruments for community development in communication and education. Trivent Publishing. 2021;113–128. doi:10.22618/TP.PCMS.20216.360008
- Signorelli MS, Surace T, Migliore M, Aguglia E. Mood disorders and outcomes in lung cancer patients undergoing surgery: a brief summary. Future Oncol. 2020;16(16s):41–44. doi:10.2217/fon-2018-0835
- Pitman A, Suleman S, Hyde N, Hodgkiss A. Depression and anxiety in patients with cancer. BMJ. 2018;361. doi:10.1136/bmj.k1415
- Richard S, Folkman S. Stress, Appraisal, and Coping. Springer publishing company; 1984.
- Rand KL, Cripe LD, Monahan PO, Tong Y, Schmidt K, Rawl SM. Illness appraisal, religious coping, and psychological responses in men with advanced cancer. Support Care Cancer. 2012;20(8):1719–1728. doi:10.1007/s00520-011-1265-y
- Walker MS, Zona DM, Fisher EB. Depressive symptoms after lung cancer surgery: their relation to coping style and social support. Psycho-Oncology. 2006;15(8):684–693. doi:10.1002/pon.997
- Mosher CE, Ott MA, Hanna N, Jalal SI, Champion VL. Coping with physical and psychological symptoms: a qualitative study of advanced lung cancer patients and their family caregivers. Support Care Cancer. 2015;23(7):2053–2060. doi:10.1007/s00520-014-2566-8
- Biggs A, Brough P, Drummond S. Part four coping with stress 21 Lazarus and Folkman’s psychological stress and coping theory. J Res Pract. 2017;17:351–364.
- Eaton RJ, Bradley G. The role of gender and negative affectivity in stressor appraisal and coping selection. Int J Stress Manag. 2008;15(1):94–115. doi:10.1037/1072-5245.15.1.94
- González-Morales MG, Peiró JM, Rodríguez I, Greenglass ER. Coping and distress in organizations: the role of gender in work stress. Int J Stress Manag. 2006;13(2):228–248. doi:10.1037/1072-5245.13.2.228
- Folkman S, Lazarus RS. An analysis of coping in a middle-aged community sample. J Health Soc Behav. 1980;21(3):219. doi:10.2307/2136617
- Matud MP, Bethencourt JM, Ibáñez I. Gender differences in psychological distress in Spain. Int J Soc Psychiatry. 2015;61(6):560–568. doi:10.1177/0020764014564801
- Fife BL, Kennedy VN, Robinson L. Gender and Adjustment to Cancer. J Psychosoc Oncol. 1994;12(1–2):1–21. doi:10.1300/J077V12N01_01
- Goldzweig G, Andritsch E, Hubert A, et al. How relevant is marital status and gender variables in coping with colorectal cancer? A sample of middle-aged and older cancer survivors. Psycho-Oncology. 2009;18(8):866–874. doi:10.1002/pon.1499
- Jacobs-Lawson JM, Schumacher MM, Hughes T, Arnold S. Gender differences in psychosocial responses to lung cancer. Gend Med. 2010;7(2):137–148. doi:10.1016/j.genm.2010.03.002
- McCaughan E, Prue G, Parahoo K, McIlfatrick S, McKenna H. Exploring and comparing the experience and coping behaviour of men and women with colorectal cancer after chemotherapy treatment: a qualitative longitudinal study. Psycho-Oncology. 2012;21(1):64–71. doi:10.1002/pon.1871
- Oppegaard K, Dunn L, Kober K, et al. Gender differences in the use of engagement and disengagement coping strategies in patients with cancer receiving chemotherapy. Oncol Nurs Forum. 2020;47(5):586–594. doi:10.1188/20.ONF.586-594
- Carver CS, Scheier MF, Weintraub JK. Assessing coping strategies: a theoretically based approach. J Pers Soc Psychol. 1989;56(2):267–283. doi:10.1037/0022-3514.56.2.267
- Esser P, Hartung TJ, Friedrich M, et al. The Generalized Anxiety Disorder Screener (GAD-7) and the anxiety module of the Hospital and Depression Scale (Hads-A) as screening tools for generalized anxiety disorder among cancer patients. Psycho-Oncology. 2018;27(6):1509–1516. doi:10.1002/pon.4681
- Spitzer RL, Kroenke K, Williams JBW, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166(10):1092–1097. doi:10.1001/archinte.166.10.1092
- Swinson RP. The GAD-7 scale was accurate for diagnosing generalised anxiety disorder. What is the diagnostic accuracy of the GAD-7 scale. Evid Based Med. 2006;11(6):184. doi:10.1136/ebm.11.6.184
- Kroenke K, Spitzer RL, Williams JBW. The PHQ-9. J Gen Intern Med. 2001;16(9):606–613. doi:10.1046/j.1525-1497.2001.016009606.x
- Spitzer RL, Kroenke K, Williams JB. Validation and utility of a self-report version of PRIME-MD the phq primary care study. JAMA. 1999;282(18):1737. doi:10.1001/jama.282.18.1737
- LaunchPad for psychology, fifth edition; 2020.
- Kelly MM, Tyrka AR, Price LH, Carpenter LL. Sex differences in the use of coping strategies: predictors of anxiety and depressive symptoms. Depress Anxiety. 2008;25(10):839–846. doi:10.1002/da.20341
- Gater R, Tansella M, Korten A, Tiemens BG, Mavreas VG, Olatawura MO. Sex differences in the prevalence and detection of depressive and anxiety disorders in general health care settings. Arch Gen Psychiatry. 1998;55(5):405. doi:10.1001/archpsyc.55.5.405
- Leach LS, Christensen H, Mackinnon AJ, Windsor TD, Butterworth P. Gender differences in depression and anxiety across the adult lifespan: the role of psychosocial mediators. Soc Psychiatry Psychiatr Epidemiol. 2008;43(12):983–998. doi:10.1007/s00127-008-0388-z
- Bergerot CD, Clark KL, Nonino A, Waliany S, Buso MM, Loscalzo M. Course of distress, anxiety, and depression in hematological cancer patients: association between gender and grade of neoplasm. Palliat Support Care. 2015;13(2):115–123. doi:10.1017/S1478951513000849
- Tung HH, Hunter A, Wei J, Chang CY. Gender differences in coping and anxiety in patients after coronary artery bypass graft surgery in Taiwan. Heart and Lung. 2009;38(6):469–479. doi:10.1016/j.hrtlng.2009.01.006
- Artinian NT, Duggan CH. Sex differences in patient recovery patterns after coronary artery bypass surgery. Heart & Lung. 1995;24(6):483–494. doi:10.1016/S0147-9563(95
- Modica M, Ferratini M, Spezzaferri R, de Maria R, Previtali E, Castiglioni P. Gender differences in illness behavior after cardiac surgery. J Cardiopulm Rehabil Prev. 2014;34(2):123–129. doi:10.1097/HCR.0000000000000043
- Brezinka V, Dusseldorp E, Maes S. Gender differences in psychosocial profile at entry into cardiac rehabilitation. J Cardiopulm Rehabil. 1998;18(6):445–449. doi:10.1097/00008483-199811000-00007
- Grace SL, Krepostman S, Brooks D, et al. Illness perceptions among cardiac patients: relation to depressive symptomatology and sex. J Psychosom Res. 2005;59(3):153–160. doi:10.1016/j.jpsychores.2005.05.005
- Van’t Spijker A, Trijsburg RW, Duivenvoorden HJ. Psychological sequelae of cancer diagnosis. Psychosom Med. 1997;59(3):280–293. doi:10.1097/00006842-199705000-00011
- Shaffer RB, Corish C. Cardiac surgery and women. J Cardiovasc Nurs. 1998;12(4):14–31. doi:10.1097/00005082-199807000-00003
- Rassoulian A, Gaiger A, Loeffler-Stastka H. Gender differences in psychosocial, religious, and spiritual aspects in coping: a cross-sectional study with cancer patients. Women’s Health Rep. 2021;2(1):464–472. doi:10.1089/whr.2021.0012
- Henrich MKG. Illness-related distress: does it mean the same for men and women?: gender aspects in cancer patients’ distress and adjustment. Acta Oncol. 1999;38(6):747–755. doi:10.1080/028418699432905
- Sharpley CF, Bitsika V, Christie DRH. Diagnosing ‘male’ depression in men diagnosed with prostate cancer: the next step in effective translational psycho-oncology interventions? Psycho-Oncology. 2014;23(9):1042–1048. doi:10.1002/pon.3530
- Matud MP. Gender differences in stress and coping styles. Pers Individ Dif. 2004;37(7):1401–1415. doi:10.1016/j.paid.2004.01.010
- Ptacek JT, Smith RE, Dodge KL. Gender differences in coping with stress: when stressor and appraisals do not differ. Pers Soc Psychol Bull. 1994;20(4):421–430. doi:10.1177/0146167294204009
- Delgado-Guay MO, Hui D, Parsons HA, et al. Spirituality, religiosity, and spiritual pain in advanced cancer patients. J Pain Symptom Manage. 2011;41(6):986–994. doi:10.1016/j.jpainsymman.2010.09.017
- Kaliampos A, Roussi P. Religious beliefs, coping, and psychological well-being among Greek cancer patients. J Health Psychol. 2017;22(6):754–764. doi:10.1177/1359105315614995
- Asgeirsdottir GH, Sigurbjörnsson E, Traustadottir R, Sigurdardottir V, Gunnarsdottir S, Kelly E. To cherish each day as it comes”: a qualitative study of spirituality among persons receiving palliative care. Support Care Cancer. 2013;21(5):1445–1451. doi:10.1007/s00520-012-1690-6
- Alcorn SR, Balboni MJ, Prigerson HG, et al. If god wanted me yesterday, i wouldn’t be here today”: religious and spiritual themes in patients’ experiences of advanced cancer. J Palliat Med. 2010;13(5):581–588. doi:10.1089/jpm.2009.0343
- McCoubrie RC, Davies AN. Is there a correlation between spirituality and anxiety and depression in patients with advanced cancer? Support Care Cancer. 2006;14(4):379–385. doi:10.1007/s00520-005-0892-6
- Kristeller JL, Sheets V, Johnson T, Frank B. Understanding religious and spiritual influences on adjustment to cancer: individual patterns and differences. J Behav Med. 2011;34(6):550–561. doi:10.1007/s10865-011-9335-7
- Renz M, Mao MS, Omlin A, Bueche D, Cerny T, Strasser F. Spiritual experiences of transcendence in patients with advanced cancer. Am J Hosp Palliat Med. 2015;32(2):178–188. doi:10.1177/1049909113512201
- Anxiety and its disorder.
- Nolen-Hoeksema S, Larson J, Grayson C. Explaining the gender difference in depressive symptoms.. J Pers Soc Psychol. 1999;77(5):1061–1072. doi:10.1037/0022-3514.77.5.1061
- Holahan CJ, Moos RH, Holahan CK, Brennan PL, Schutte KK. Stress generation, avoidance coping, and depressive symptoms: a 10-year model. J Consult Clin Psychol. 2005;73(4):658–666. doi:10.1037/0022-006X.73.4.658
- Garnefski N, Kraaij V. Relationships between cognitive emotion regulation strategies and depressive symptoms: a comparative study of five specific samples. Pers Individ Dif. 2006;40(8):1659–1669. doi:10.1016/j.paid.2005.12.009
- Kohn PM, Hay BD, Legere JJ. Hassles, coping styles, and negative well-being. Pers Individ Dif. 1994;17(2):169–179. doi:10.1016/0191-8869(94)90023-X
- Chan I, Au A, Li P, Chung R, Lee MP, Yu P. Illness-related factors, stress and coping strategies in relation to psychological distress in HIV-infected persons in Hong Kong. AIDS Care. 2006;18(8):977–982. doi:10.1080/09540120500490093
- Ravindran AV, Griffiths J, Merali Z, Anisman H. Primary dysthymia: a study of several psychosocial, endocrine and immune correlates. J Affect Disord. 1996;40(1–2):73–84. doi:10.1016/0165-0327(96
- Horney DJ, Smith HE, McGurk M, et al. Associations between quality of life, coping styles, optimism, and anxiety and depression in pretreatment patients with head and neck cancer. Head Neck. 2011;33(1):65–71. doi:10.1002/hed.21407
- Aarstad AKH, Beisland E, Aarstad HJ. Personality, choice of coping and T stage predict level of distress in head and neck cancer patients during follow-up. Eur Arch Oto-Rhino-L. 2012;269(9):2121–2128. doi:10.1007/s00405-011-1884-4
- Hassanein KAAM, Musgrove BT, Bradbury E. Psychological outcome of patients following treatment of oral cancer and its relation with functional status and coping mechanisms. J Craniomaxillofac Surg. 2005;33(6):404–409. doi:10.1016/j.jcms.2005.05.005
- Oancea C, Papava I, Enatescu V, et al. The impact of coping on the somatic and mental status of patients with COPD: a cross-sectional study. Int J Chron Obstruct Pulmon Dis. 2016:1343. doi:10.2147/COPD.S106765
- Holmgren GL. Physical and psychological correlates of speaker recognition. J Speech Hear Res. 1967;10(1):57–66. doi:10.1044/jshr.1001.57