Abstract
Objectives
Brain metastases (BMs) often advance the course of non-small cell lung cancer (NSCLC). We performed an observational study in order to investigate the possible correlation of selected clinical and epidemiological factors with BM appearance in patients suffering from different histological subtypes of NSCLC stage I–IV.
Methods
The study included 161 consecutive patients with NSCLC. Analyzed data included patient- and tumor-related characteristics.
Results
Thirty-nine patients (24.2%) presented BMs within 12 (0–36) weeks of diagnosis. BMs decreased the mean overall survival significantly (15.6 versus 50.7 weeks, P < 0.001), with hazard ratio (95% confidence interval) 3.60 (2.42–5.35). The age of the patients with BM was significantly lower than that of the patients without BM (60.8 ± 8.9 versus 66.5 ± 8.5, P < 0.001). Patients with BM had significantly higher pack-years consumption (75.9 ± 23.9 versus 58.9 ± 31.9, P = 0.003) and larger tumor size compared with patients without BM (size in mm: 55.1 ± 20.1 versus 45.9 ± 19.3, P = 0.012). The presence of BM was also correlated with the absence of lung (P < 0.001), bone (P = 0.005), and adrenal (P = 0.046) metastases.
Conclusion
Younger NSCLC patients with high tobacco consumption, large tumor size, and absence of metastases in other organs (lung, bones, adrenal metastases) are at high risk of BM appearance during the course of NSCLC and are candidates for prophylactic cranial irradiation early in the course of the disease.
Introduction
Lung cancer was the leading cause of death from cancer in Europe in 2006, with 334,800 deaths (19.7% of total).Citation1 Non-small cell lung cancer (NSCLC) is the most common type of lung cancer, representing more than 80% of lung cancer cases.Citation2
Brain metastases (BMs) are a frequent complication of NSCLC, especially in patients with locally advanced disease.Citation3,Citation4 The addition of chemotherapy to radiation therapy (RT) reduces distant metastases and significantly improves survival.Citation5,Citation6 However, chemoradiotherapy is shown not to reduce the rate of BM,Citation5 but to be associated with increased rates of overall brain failure (21%–54%) and an increased incidence of the brain as the first site of relapse (15%–30%).Citation5–Citation8 These findings emphasize the need for treatment specifically directed at brain micrometastases.
Prophylactic cranial irradiation (PCI) has been demonstrated to reduce the incidence or delay the onset of BM in patients with locally advanced NSCLC, after initial treatment in numerous selected nonrandomized and randomized studies.Citation3,Citation7,Citation9–Citation16 Nevertheless, during the last decade only few studies assessed the clinical and epidemiological factors associated with high risk of BM appearance in NSCLC patients with locally advanced disease at diagnosis.Citation14,Citation17–Citation20 In these studies, several factors such as duration of survival after diagnosis, performance status, chemotherapy regimens, age at diagnosis, sex, and lung cancer histotype and stage have been associated with the risk of BM development.
The authors of this paper hypothesized that among NSCLC patients of stage I–IV may exist a group of patients at high risk of presenting BM that may be protected using PCI. This group should be identified in order to serve as target for future studies of PCI application in NSCLC.
We performed an observational study in order to investigate the possible correlation of selected clinical and epidemiological factors with BM appearance in patients suffering from different histological subtypes of NSCLC stage I–IV.
Methods
The study’s cohort
We recruited 161 consecutive patients with a new diagnosis of NSCLC, between January 2003 and March 2009. Patients’ selection criteria were as follows: confirmed diagnosis of NSCLC and appropriate staging. The sixth edition of the tumor–node–metastasis (TNM) classification was used.Citation21
All patients were treated with surgery and/or chemotherapy and/or radiotherapy according to the current guidelines.Citation22,Citation23 They were evaluated every 3–6 months, depending on the curative or palliative nature of the initial treatment.
For each patient, the following variables were recorded at the time of diagnosis: age, sex, tobacco consumption, comorbidities, TNM status at diagnosis, tumor histotype, computed tomography (CT) scan features (central/peripheral location, side, lung lobe, size, cavitation, pleural effusion), and bronchoscopic findings. During the study period, the variables of patients with BM were registered and compared with those of patients without BM. All patients gave their informed consent, and the study was approved by the Ethics Committee of the “Sotiria” Chest Diseases Hospital, Athens.
Statistical analysis
Mean values (and standard deviation [SD]) or median values (and interquartile range [IR]) were used to describe quantitative variables. For the comparison of quantitative variables without normal distribution between two groups, and between three or more different groups, the Mann– Whitney test and Kruskal–Wallis test were used, respectively. To compare normal distributed quantitative variables between two groups and between three or more different groups, Student’s t-test and analysis of variance test were used, respectively.
To control for type I errors, due to multiple comparisons, Bonferroni correction was used, by which the significance level is defined as 0.05/k (k = number of comparisons). Logistic regression analysis (stepwise method) was used in order to find independent factors associated with BM presentation. Odds ratios (ORs) and 95% confidence intervals (CIs) were computed from the results of logistic analysis. Kaplan–Meyer method was used to estimate survival curves. To compare survival curves, log rank tests were used. Statistical significance was set at 0.05, and all P-values are two tailed. For the statistical analysis, SPSS Statistics 17.0 (IBM Corporation, Somers, NY) and STATA 9.0 (Stata Corp, College Station, TX) programs were used.
Results
Description of the cohort
Patient’s characteristics are summarized in . Most of the patients were males (88.8%), with mean age (±SD) 65.1 ± 8.9 years and mean tobacco consumption (±SD) of 63.0 ± 31.0 pack-years.
Table 1 Patient- and disease-related characteristics
Most of the tumors were located centrally (85.7%). Therefore, they were located within the range of fiber bronchoscopy, which revealed mainly mucosal or submucosal infiltration (67.7%). Most of the tumors were on the right lung (52.2%) and on the upper lobes (70.2%). The mean size (±SD) of the tumors, measured on CT scanners, was 48.1 ± 19.8 mm. Almost one-third (36.6%) were accompanied by pleural effusion at presentation. During the disease course, 37.3% of the patients presented lung, 36.6% bone, 23% liver, and 21.7% adrenal metastases.
BMs
BMs were presented in 24.2% of the patients. The median time (IR) of BM appearance was 12 (0–36) weeks from diagnosis. At the time of BM presentation, most of the patients were classified as T4 (42.9%) and N2 (43.5%) by the TNM classification. A total of 59% of the BMs were ≥2, mostly unilateral (53.8%).
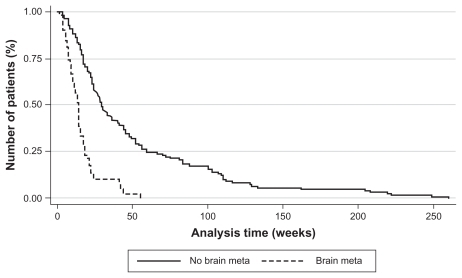
The overall survival of the cohort was influenced by the presence of BM (). Survival time of the patients with BM was shorter compared with those without BM: 15.6 weeks (standard error [SE] = 1.9) versus 50.7 weeks (SE = 4.8, P < 0.001). The hazard ratio, upon Cox model, for the presence of BM was 3.60 (95% CI 2.42–5.35, P < 0.001).
Figure 1 Kaplan–Meier estimation of overall survival (patients with or without brain metastases).
Abbreviation: meta, metastasis.
The age of patients with BM was significantly lower compared with that of the patients without BM (60.8 ± 8.9 versus 66.5 ± 8.5, P < 0.001) (). Furthermore, patients with BM had significantly higher pack-years consumption (75.9 ± 23.9 versus 58.9 ± 31.9, P = 0.003) and larger tumor size compared with patients without BM (size in mm: 55.1 ± 20.1 versus 45.9 ± 19.3, P = 0.012). The presence of BM was also correlated with the absence of lung (P < 0.001), bone (P = 0.005), and adrenal (P = 0.046) metastases.
Table 2 Correlation of brain metastases with patient- and disease-related features (univariate analysis)
Patients with right-sided BM presented a significantly lower rate of arterial hypertension (16.7% versus 83.8%, P = 0.050) (). None of the patients with unilobar BM suffered from diabetes, compared with patients with multilobar (≥2 lobes) metastases (P = 0.015) ().
Table 3 Univariate analysis of brain metastases side
Table 4 Univariate analysis of brain metastases lobes
According to regression analysis, age, tobacco consumption in pack-years, and absence of lung or bone metastases represented independent prognostic factors for the appearance of BM (). In particular, an increase of age reduced the possibility of BM appearance (OR 0.91; 95% CI 0.87–0.96, P < 0.001). Conversely, increasing cigarette consumption increased the possibility of BM appearance (OR 1.02; 95% CI 1.001–1.030, P = 0.006). Patients without lung and bone metastases had 76% and 70% higher possibility of presenting BM, respectively.
Table 5 Correlation of brain metastases with patient- and disease-related features (multivariate analysis)
Discussion
The main finding of this observational study was that younger NSCLC patients with high tobacco consumption, large tumor size, and absence of other metastases are at high risk of developing BMs during the course of their disease.
BM appearance and survival
Robnett et al reported that the timing of chest irradiation can influence the risk of brain recurrences: the rate of BM is 27% in patients receiving induction chemotherapy before thoracic RT compared with 15% in patients who are treated with concurrent chemoradiation.Citation17 The 2-year actuarial rate of BM is 39% versus 20%. The authors hypothesize that early aggressive locoregional and systemic treatment could better control regional disease, which in turn affects the development of brain relapses. In accordance with these findings, BMs presented in 39 out of 161 patients (24.2%) in this present study. The rate of BM is quite similar to the rate which has been previously reported by Robnett et al for patients who were not treated with concurrent chemoradiotherapy. The lack of a radiotherapy department in the “Sotiria” Chest Diseases Hospital renders impossible the application of concurrent chemoradiotherapy and therefore leads to the application of the sequential module.
Once diagnosed, BMs are mostly treated with wholeb-rain radiotherapy, having a response rate of 45%–81% in NSCLC.Citation24,Citation25 The overall survival of NSCLC patients with BM is poor, reported to be 3–6 months, despite medical treatment.Citation26 The overall survival of the patients in this present study with BM was also poor, approximately 4 months.
Patients who are at high risk of developing BM
The delay of BM appearance is expected to improve prognosis of NSCLC patients. To achieve this, we need objective means to indicate patients at high risk for developing BM. Some studies have already been oriented towards this direction. Biologic agents like neuron specific enolase, carcinoembryonic antigen, serum sodium levels, or numerous molecular markers have been correlated with the development of BM and a shorter survival.Citation26–Citation28
Nevertheless, specific phenotypic characteristics may also serve as surrogate prognostic factors. Earlier studies correlated the presence of BM with advanced stage, NSCLC histotypes, delay of lung radiotherapy, younger age, and large tumor size.Citation28–Citation32 However, few studies assessed in this regard tobacco consumption, comorbidities, CT scanner tumor characteristics, or the presence of metastases other than BMs.
Age at diagnosis
Age < 60 years was shown to be associated with an increased risk of BM.Citation30,Citation33,Citation34 In this present study, younger age (60.8 ± 8.9 years) was correlated with a higher possibility of BM appearance (). However, younger patients with BM present a better performance status and longer survival, while they may tolerate aggressive treatment better and are willing to accept a higher risk of toxicity than older patients.Citation26,Citation35
T and N status
T4 initial status was associated with increased risk of BM in a multivariate analysis of 305 patients with localized NSCLC.Citation30 The N2 status was found to be predictive of BM by Jacobs et al and by Tang et al.Citation36,Citation37
In this study, lung tumor size was correlated with the appearance of BM (55.1 ± 20.1 cm) (). This finding is in agreement with the study of Mujoomdar et al.Citation31 However, no correlation was found with the T status itself. T status, as well as N status, has been correlated with BM outbreak in recent studies.Citation30,Citation31
As is the case in the study of Shi et al, the authors of this present study found most of the primary tumors to be located in the right lung and in the upper lobes.Citation32 These frequent locations of lung tumor did not seem to correlate with the appearance of BM.Citation32 Central or peripheral location of primary lung tumor was not found to be correlated to BM, which is in agreement with the study of Mujoomdar et al.Citation31
M status
Previous studies speculate that the spread of lung cancer to the thoracic lymphatic system and to the brain could also relate to the presence of distant metastatic disease in other organs.Citation31 So far, no study has confirmed this hypothesis. On the contrary, in this present study, appearance of BM was correlated with the absence of metastases in other organs, like lung, bone, and adrenal glands. Except adrenal metastases,Citation27 synchronous metastases in other organs have not been correlated with median survival, probably as a result of already poor prognosis of the BM.Citation26
Tobacco consumption
Smoking status has already been correlated with poor prognosis and shorter overall survival in lung cancer patients,Citation18 but no correlation was found with BM. In this study’s cohort, high tobacco consumption (75.9 ± 23.9 pack-years) was correlated with the outbreak of BM.
NSCLC histological subtype
In previous studies, non-squamous lung cancer, mainly lung adenocarcinoma, showed higher prevalence of BM development.Citation30–Citation32 In this study, no correlation was found between NSCLC histotype and BM appearance. This discordance is probably a result of the small number of allocated groups and the relatively large number of unspecified NSCLC tumors in the present study.
PCI
Prophylactic cranial irradiation (PCI) has been demonstrated to reduce the incidence or delay the onset of BM in patients with locally advanced NSCLC after initial treatment.Citation3,Citation7,Citation9–Citation16 Thus, identification of risk population for BM development is pertinent. Specific phenotypes of patients at higher risk for BM development could serve as candidates of PCI and could allow early intervention, which seems more promising than the palliative approach.
Limitations
The patients in this current study were treated with sequential rather than concurrent chemoradiotherapy despite the current treatment guidelines. This limitation of the study is due to the lack of a radiotherapy department in the “Sotiria” Chest Diseases Hospital.
The pathologic data lack molecular markers, which could be related to the overall survival as is the case in many recent studies. In fact, during the study period, molecular data were not available.
Implications
This study records the deleterious effect of BMs on NSCLC patient survival, enriches the high risk profile with more features, and contributes to the discussion of pathophysiologic mechanisms underlying the brain involvement in NSCLC. More studies are needed in order to elucidate these issues.
Conclusion
Younger NSCLC patients with high tobacco consumption, large tumor size, and absence of other metastases (lung, bones, adrenal metastases) are at high risk of BM appearance during the course of NSCLC and may be candidates for PCI early in the course of their disease. Apart from genome-based studies, phenotype-based studies may contribute to future lung cancer therapy.
Disclosure
The authors report no conflicts of interest in this work.
References
- FerlayJAutierPBoniolMHeanueMColombetMBoylePEstimates of the cancer incidence and mortality in Europe in 2006Ann Oncol.20071858159217287242
- WalkerSUpdates in non-small cell lung cancerClin J Oncol Nurs.2008258759618676326
- AlbainKSRuschVWCrowleyJJConcurrent cisplatin/etoposide plus chest radiotherapy followed by surgery for stages IIIA (N2) and IIIB non-small-cell lung cancer: Mature results of Southwest Oncology Group Phase II study 8805J Clin Oncol.199513188018927636530
- AndreFGrunenwaldDPujolJLPatterns of relapse of N2 nonsmall-cell lung carcinoma patients treated with preoperative chemotherapy: Should prophylactic cranial irradiation be reconsidered?Cancer.2001912394240011413530
- CoxJDScottCBByhardtRWAddition of chemotherapy to radiation therapy alters failure patterns by cell type within non-small cell carcinoma of lung (NSCCL): Analysis of Radiation Therapy Oncology Group (RTOG) trialsInt J Radiat Oncol Biol Phys.19994350550910078629
- CooperJDSilvermanSClementJAProphylactic cranial irradiation for lung cancer patients at high risk for development of cerebral metastasis: Results of a prospective randomized trial conducted by the Radiation Therapy Oncology GroupInt J Radiat Oncol Biol Phys.1991216376431651304
- StuschkeMEberhardtWPottgenCProphylactic cranial irradiation in locally advanced nonsmall-cell lung cancer after multimodality treatment: Long-term follow-up and investigations of late neuropsychologic effectsJ Clin Oncol.1999172700270910561344
- AndreFGrunenwaldDPujolJLPatterns of relapse of N2 nonsmall-cell lung carcinoma patients treated with preoperative chemotherapy: Should prophylactic cranial irradiation be reconsidered?Cancer.2001912394240011413530
- StraussGMHerndonJEShermanDDNeoadjuvant chemotherapy and radiotherapy followed by surgery in stage IIIA non-small cell carcinoma of the lung: Report of a Cancer and Leukemia Group B phase II studyJ Clin Oncol.19921023712441732424
- RuschVWGriffinBRLivingstonRBThe role of prophylactic cranial irradiation in regionally advanced non-small cell lung cancer. A Southwest Oncology Group StudyJ Thorac Cardiovasc Surg.1989985355392552227
- SkarinAJochelsonMSheldonTNeoadjuvant chemotherapy in marginally resectable stage III M0 non-small cell lung cancer: Longterm follow-up in 41 patientsJ Surg Oncol.1989402662742538680
- RussellAHPajakTESelimHMProphylactic cranial irradiation for lung cancer patients at high risk for development of cerebral metastasis: Results of a prospective randomized trial conducted by the Radiation Therapy Oncology GroupInt J Radiat Oncol Biol Phys.1991216376431651304
- UmsawasdiTValdiviesoMChenTTRole of elective brain irradiation during combined chemoradiotherapy for limited disease non-small cell lung cancerJ Neuro Oncol.19842253259
- CoxJDStanleyKPetrovichZPaigCYesnerRCranial irradiation in cancer of the lung of all cell typesJAMA.19812454694727452872
- PöttgenCEberhardtWGrannassAProphylactic cranial irradiation in operable stage IIIA non-small-cell lung cancer treated with neoadjuvant chemoradiotherapy: Results from a German multicenter trialJ Clin Oncol.2007254987499217971598
- YavuzAATopkanEOnalCYavuzMNProphylactic cranial irradiation in locally advanced non-small cell lung cancer: Outcome of recursive partitioning analysis group I patientsJ Exp Clin Cancer Res.2008278019055787
- RobnettTJMachtayMStevensonJPAlgazyKMHahnSMFactors affecting the risk of brain metastases after definitive chemoradiation for locally advanced non-small-cell lung carcinomaJ Clin Oncol.2001191344134911230477
- LawAKarpDDDipetrilloTDalyBTEmergence of increased cerebral metastasis after high-dose preoperative radiotherapy with chemotherapy in patients with locally advanced non-small cell lung carcinomaCancer.20019216016411443622
- CeresoliGLReniMChiesaGBrain metastases in locally advanced nonsmall cell lung carcinoma after multimodality treatment: Risk factors analysisCancer.20029560561212209754
- CarolanHSunAYBezjakADoes the incidence and outcome of brain metastases in locally advanced non-small cell lung cancer justify prophylactic cranial irradiation or early detection?Lung Cancer.20054910911515949596
- SobinLHWittekindCthe International Union Against Cancer (UICC), editorsTNM Classification of Malignant Tumors6th edNew York, NYWiley-Liss200299103
- AlbertsMLung Cancer GuidelinesChest.20031231212527589
- AlbertsMDiagnosis and management of lung cancer. Executive summaryChest.200713211917625075
- AddeoRCaragliaMFaiolaVConcomitant treatment of brain metastasis with whole brain radiotherapy [WBRT] and temozolomide [TMZ] is active and improves quality of lifeBMC.2007718
- MaSXuYDengQYuXTreatment of brain metastasis from nonsmall cell lung cancer with whole brain radiotherapy and Gefitinib in a Chinese populationLung Cancer.20096519820319091441
- JacotWQuantinXBoherJMBrain metastases at the time of presentation of non-small cell lung cancer: A multi-centric AERIO* analysis of prognostic factorsBr J Cancer.20018490390911286469
- PenelNBrichetAPrevostBPrognostic factors for synchronous brain metastases from lung cancerLung Cancer.20013314315411551409
- ArrietaOSaavedra-PerezDKuriRBrain metastasis development and poor survival associated with carcinoembryonic antigen (CEA) level in advanced non-small cell cancer: A prospective analysisBMC Cancer.2009911919386089
- RobnettTMachtayMStevensonJFactors affecting the risk of brain metastases after definitive chemoradiation for locally advanced non-small-cell lung carcinomaJ Clin Oncol.2001191344134911230477
- BajardAWesteelVDubiezAMultivariate analysis of factors predictive of brain metastases in localized non-small cell lung carcinomaLung Cancer.20044531732315301872
- MujoomdarAAustinJMalhotaRClinical predictors of metastatic disease to the brain from non-small cell lung carcinoma: Primary tumor size, cell type, and lymph node metastasesRadiology.200724288288817229875
- ShiADigumarthySTemelJHalpernEFKuesterLBAquinoSLDoes initial staging or tumor histology better identify asymptomatic brain metastases in patients with non-small cell lung caner?J Thorac Oncol.2006120521017409858
- CeresoliGLReniMChiesaGBrain metastases in locally advanced non-small cell lung carcinoma after multimodality treatment: Risk factors analysisCancer.20029560561212209754
- SchoutenLJRuttenJHuveneersHATwinjstraAIncidence of brain metastases in a cohort of patients with carcinoma of the breast, colon, kidney, and lung and melanomaCancer.2002942698270512173339
- GoreEBrain metastases in very young patients with lung cancer are still brain metastasesOnkologie.20083129726818547968
- JacobsRHAwanABitranJDProphylactic cranial irradiation in adenocarcinoma of the lung: A possible roleCancer.198759201620193567864
- TangSGLinFJLeungVMImpact of cranial irradiation in adenocarcinoma of the lungJ Formos Med Assoc.1993924134198104594