
Abstract
Introduction
Chronic obstructive pulmonary disease (COPD) is associated with increased cardiovascular morbidity and mortality. Elevated arterial stiffness, measured by aortic pulse wave velocity (aPWV), is a cardiovascular risk surrogate and is potentially modifiable by inhaled corticosteroid/long-acting beta2-agonist combinations in patients with COPD.
Materials and methods
The effects of once-daily inhaled fluticasone furoate/vilanterol (FF/VI) 100/25 µg, VI 25 µg, versus placebo on arterial stiffness in patients with COPD and baseline aPWV ≥11.0 m/s were investigated in a 24-week, multicenter, double-blind, randomized, stratified (by COPD exacerbation history), parallel-group, placebo-controlled trial. Eligible patients were ≥40 years old, with ≥10 pack-year smoking history, forced expiratory volume in 1 s (FEV1)/forced vital capacity ≤0.70, and post-bronchodilator FEV1 ≤70% of predicted. Patients with a major cardiovascular event in the previous 6 months/current severe heart failure/uncontrolled hypertension were excluded. Primary endpoint is change from baseline in aPWV after 24 weeks of treatment. Safety analyses included adverse events (AEs).
Results
The intent-to-treat population included 430 patients: FF/VI (n=135), VI (n=154), and placebo (n=141). Patients were predominantly male (79%) and Asian or White (each 48%), with a mean age of 68.5 years (standard deviation [SD] =7.9), percentage predicted post-bronchodilator FEV1 50.1% (SD =13.3), and aPWV 13.26 m/s (SD =2.22) at screening. At 24 weeks, mean (standard error [SE]) changes from baseline in aPWV were −1.75 m/s (SE =0.26, FF/VI), −1.95 m/s (SE =0.24, VI), and −1.97 m/s (SE =0.28, placebo). AEs occurred in 57% (FF/VI), 51% (VI), and 41% (placebo) of patients.
Conclusion
No differences were observed in aPWV-adjusted mean change from baseline for FF/VI 100/25 µg, compared with placebo.
Introduction
Chronic obstructive pulmonary disease (COPD) is associated with accelerated atherosclerosis, and the majority of mild-to-moderate COPD-related mortality is due to cardiovascular disease (CVD).Citation1,Citation2 Airflow obstruction is independently associated with CVD.Citation3–Citation7 Structural and functional elements of COPD (emphysema/airflow obstruction) are associated with increased arterial stiffness,Citation8–Citation11 which is associated with atherosclerosis and CVD.Citation12–Citation14
Although the mechanisms underlying these associations are not well defined, pulmonary and systemic inflammation are potential contributors.Citation1,Citation15,Citation16 Systemic endothelial dysfunction and vascular re-modeling (including proliferation of smooth muscle cells, elastin degradation, and collagen deposition, which may be followed by calcification and ultimately result in arterial stiffening),Citation18 are also evident at all severities of COPD and further contribute to arterial stiffening.Citation19 Additional impacts of COPD, such as reduced ability to exercise, may also contribute to arterial stiffening by altering vascular hemodynamics.Citation16
As a potentially modifiable element, in addition to being a strong risk factor for CVD, arterial stiffness may serve as an intermediate endpoint for interventions aimed at reducing cardiovascular risk. In inflammatory conditions, such as polymyalgia rheumatica and peripheral arterial disease, improvements in aPWV have been detected following treatment with corticosteroidsCitation20 (targeting inflammation)Citation16 or long-acting beta2-agonistsCitation21 (long-acting beta2 agonist [LABA], inducing endothelial nitric oxide synthase-mediated vasodilation).Citation22
In recent years, few studies have attempted modulation of arterial stiffness in COPD, using exercise therapy, LABA, or inhaled corticosteroids (ICS).Citation22–Citation25 Given the associations between lung function, inflammation, and arterial stiffness noted above, medications modulating pulmonary function/inflammation might also be effective in reducing arterial stiffness for patients with COPD. In a 12-week study, fluticasone propionate/salmeterol had no effect on aortic pulse wave velocity (aPWV [carotid femoral PWV]), the gold standard measure of arterial stiffness, relative to placebo.Citation25 However, post hoc analysis suggested that individuals with aPWV >10.9 m/s had significantly reduced arterial stiffness with the treatment.Citation25 Another 12-week study comparing once-daily fluticasone furoate (FF)/vilanterol (VI) with tiotropium in patients with aPWV ≥11 m/s reported aPWV reduction from baseline in both the arms, but no significant difference between the arms.Citation26 No placebo comparator was included, limiting the conclusions.Citation26 The length of treatment may also be important to see significant effects. For example, although LABAs may lower aPWV initially, the additional anti-inflammatory benefit of ICS therapy in a LABA/ICS combination may only be seen after longer-term treatment. This study hypothesized that once-daily FF/VI 100/25 µg would reduce aPWV after 24-weeks of treatment, compared with placebo. This is the first respiratory medication-focused, placebo-controlled, interventional trial examining aPWV modulation as a primary outcome of interest.
Materials and methods
Study design
This multicenter, randomized, placebo-controlled, double-blind, parallel-group study (March 2011 to November 2014; 61 centers; Norway/Germany/the Republic of Korea/the Philippines/Thailand/USA; GSK HZC113108; ClinicalTrials.gov NCT1336608) was approved by applicable institutional review boards/independent ethics committees and conducted in accordance with the International Conference on Harmonisation: Guidance for Good Clinical Practice (GCP)Citation27 and the Declaration of Helsinki.Citation28 Details of the ethical review boards for this study are provided in the Supplementary Materials. Patients provided prior written informed consent.
Patients aged ≥40 years with a history of COPD, current/prior smoking history (≥10 pack-years), a post-albuterol (salbutamol) forced expiratory volume in 1 s (FEV1) ≤70% of the predicted normal value, a FEV1/forced vital capacity ratio ≤0.70, and aPWV ≥11.0 m/s, measured by SphygmoCor CPVH according to the manufacturer’s instructions (AtCor Medical Inc., Itasca, IL, USA)Citation25 were eligible. Patients were excluded if: the underlying cause of their COPD was α1-antitrypsin deficiency; they had other respiratory disorders (including active tuberculosis or lung cancer); they had current severe heart failure; they had had a recent cardiovascular event (such as acute coronary syndrome or stroke, within the previous 6 months); they had clinically significant uncontrolled hypertension; they had an abnormal/clinically significant 12-lead electrocardiogram finding; or they had started, discontinued, and/or were receiving medications (such as anti-hypertensives, lipid-lowering agents, hypoglycemic agents or nitrates) without reaching a stable dose in the last 3 months and/or were not anticipated to remain at a stable dose throughout the study period.
After a 2-week, single-blind, placebo run-in period, during which COPD stability and protocol compliance were evaluated, eligible patients were randomized (by center, 1:1:1; telephone-based Registration and Medication Ordering System; stratified according to COPD exacerbation in the previous 3 years [yes/no]) to receive FF/VI 100/25 µg, VI 25 µg, or placebo, administered once daily for 24 weeks via the ELLIPTA® inhaler (GSK, Brentford, UK). Participants’ usual COPD medications were discontinued from 24 h to 12 weeks prior to the first clinic visit (screening) and thereafter at any time during the study, with the exception of ipratropium bromide (for patients receiving a stable dose throughout the study) and the study-provided albuterol (salbutamol, used as rescue medication), which were withheld for 4 h prior to study visits. Full details are given in Supplementary Table 1.
Further clinic visits were scheduled at treatment weeks 4, 12, 18, and 24 with a follow-up phone call 1 week after the final visit. The treatments in this study were double-blind. Neither the investigator (nor study staff) nor the patient knew which treatment the patient was receiving. Treatment codes could be unblinded by the investigator or treating physician only in the case of a medical emergency or in the event of a serious medical condition, when knowledge of the investigational product was essential for the clinical management or welfare of the patient. The sponsor’s (GSK) Global Clinical Safety and Pharmacovigilance staff could unblind treatment codes in the event of a serious adverse event (SAE).
The following non-COPD medications were allowed if the patient had been on a stable dose for at least 3 months prior to screening and was anticipated to remain on a stable dose throughout the 6-month treatment period: anti-hypertensives (angiotensin-converting enzyme inhibitors, diuretics, angiotensin2-receptor antagonists, beta-blockers, calcium-channel blockers, alpha-blockers, central alpha-agonists), lipid-lowering agents (eg statins, ezetimibes), hypoglycemic agents for the treatment of diabetes (sulfonylurea, glitizone, metformin, etc), and nitrates. In addition, the following non-COPD medications were permitted: cardioselective beta-blockers (stable dose) and ophthalmic beta-blockers; antihistamines and nasal decongestants; over-the-counter cough suppressants; intranasal cromolyns or nedocromil; intranasal corticosteroids (provided the patient was on a stable daily dose for at least 4 weeks prior to clinic visit 1 and remained on this dose throughout the study); topical (≤1% hydrocortisone in strength) or ophthalmic corticosteroids; antibiotics that were not strong inhibitors of cytochrome P450 3A4 for short-term treatment (≤14 days) of acute non-respiratory tract infections (eg erythromycin); influenza and/or pneumonia vaccines; tricyclic antidepressants and monamine oxidase inhibitors; diuretics; smoking cessation medications; all medications for other disorders as long as the dose remains constant wherever possible and their use would not be expected to affect lung function or aPWV.
Two amendments were made to the original protocol (dated December 15, 2010), which applied to all investigational sites. The first revised the inclusion criteria for baseline aortic pulse wave velocity (aPWV) from ≥12 m/s to ≥11 m/s due to low enrollment (effective from August 19, 2011). The second revised the sample size re-estimation for reasons discussed below (effective from February 01, 2013).Citation29
Efficacy and safety assessments
The primary endpoint was change from baseline in aPWV at 24 weeks (day 168) for the comparison of FF/VI 100/25 µg versus placebo. aPWV was measured (as described)Citation26 at screening and on weeks 4, 12, 18, and 24.
Secondary endpoints included morning trough (pre- bronchodilator/pre-dose) FEV1 (measured at every clinic visit) and the mean number of albuterol used during a 24-h period throughout treatment. Other endpoints included inspiratory capacity (IC), biomarkers (high sensitivity C-reactive protein [hsCRP], fibrinogen, interleukin 6 [IL-6], pulmonary and activation-regulated chemokine [PARC]), and quality of life (by the St George’s Respiratory Questionnaire for COPD patients [SGRQ]). Exploratory endpoints were peripheral/central pulse pressures (PP), aortic augmentation index (AIx),Citation26,Citation30 and COPD Assessment Test (CAT).
Safety assessments were performed at each clinic visit, including incidence of adverse events (AEs), pneumonia, and oropharyngeal examination. Vital signs (pulse rate and blood pressure [BP]) were measured at each visit. COPD exacerbations were not recorded as AEs, but were recorded as SAEs if they met the definition of a SAE. A SAE was any AE that resulted in any of the following outcomes: death; immediate risk of death, in the view of the investigator; hospitalization (or prolonged an existing hospitalization); disability or incapacity; congenital anomaly in the patient’s offspring; or jeopardized the patient, according to the medical judgment of the investigator.
Statistical methods
Analyses for study population, efficacy, health outcomes, and biomarker data used the intent-to-treat (ITT) population (all the patients randomized who received at least one dose of medication were randomized, excluding 14 patients from one center with GCP issues not associated with the current trial). The safety population was the ITT population plus the 14 patients noted. Further details are provided in the Supplementary materials.
Sample size calculations were based on an estimate of the standard deviation (SD) of mean change from baseline in aPWV of 2.6 m/s.Citation26 Accordingly, 143 patients per arm were required to provide 80% power for the detection of a 1 m/s treatment difference on day 168, at a significance level of 0.05, based on a two-sample, two-sided t-test, allowing for a 25% withdrawal rate. More information is provided in the Supplementary materials.
Change from baseline aPWV recorded on days 28, 84, 126, and 168 was analyzed using mixed models repeated measures with terms for visit, treatment, age, gender, smoking history, COPD exacerbation history, geographic region, baseline aPWV, and interaction terms of baseline aPWV by clinic visit and treatment by clinic visit. From this model, treatment effects and differences were obtained for each visit. Change from baseline trough FEV1 was analyzed using a similar model, with the covariate of baseline FEV1 instead of baseline aPWV. The mean number of occasions of albuterol use for the entire 24-week treatment period was analyzed using analysis of covariance with covariates of baseline rescue medication use, geographic region, and COPD exacerbation history.
Multiplicity was controlled using a closed testing procedure. For the primary treatment comparison, secondary endpoints were nested under the primary endpoint in the following order: trough FEV1, followed by the mean number of occasions of albuterol use, to make inferences for predefined secondary endpoints while controlling for the overall Type I error. In the absence of significance for the primary endpoint, then the tests for the secondary and other efficacy endpoints must be interpreted as descriptive only. The primary treatment comparison was fluticasone furoate/vilanterol 100/25 µg versus placebo. All other treatment comparisons were considered as supportive.
AEs were coded and grouped by System Organ Class and Preferred Term using the Medical Dictionary for Regulatory Activities (MedDRA; Version 17.1). AEs of special interest were defined a priori based on known pharmacologic effects of LABAs and/or ICSs.
Post hoc analyses
Post hoc logistic regression analyses compared the proportion of responders (patients with an aPWV reduction from baseline of ≥1 m/s on day 168) between arms, where 1) withdrawn patients were classified as nonresponders and 2) withdrawn patients (prior to day 168) were classified as missing. An investigation comparing change from baseline in aPWV with the baseline aPWV was also carried out post hoc.
Results
Patient disposition
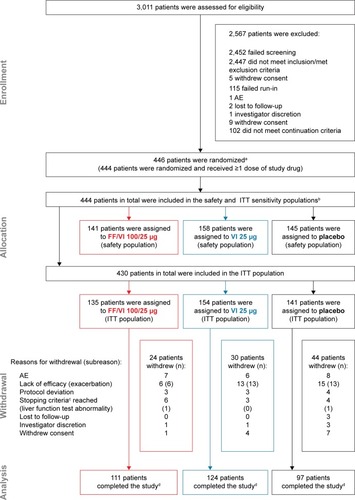
The ITT population comprised 430 patients, of whom 332 (77%) completed the study (). The most frequent reason for early withdrawal was lack of efficacy. Baseline characteristics and demographics were generally comparable between arms (). Most patients were Asian or White and in Global Initiative for Chronic Obstructive Lung Disease (GOLD) group B or D, with moderate or severe airflow limitation.Citation19 Hypertension (65%) and hypercholesterolemia (41%) were the most common comorbid cardiovascular history/risk factors.
Table 1 Screening and baseline characteristics
Figure 1 CONSORT diagram.
Abbreviations: AE, adverse event; FF, fluticasone furoate; ITT, intent-to-treat; VI, vilanterol.
Efficacy
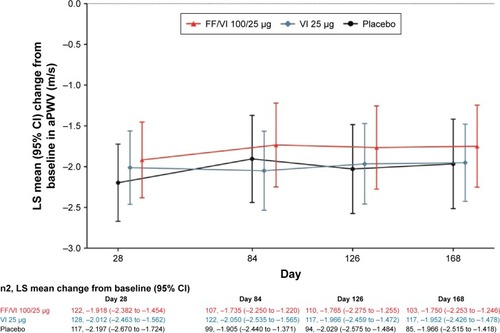
Numerical reductions from baseline in aPWV were seen in all treatment groups at all time points (), but the comparison of FF/VI versus placebo on day 168 () was not statistically significant. All secondary and other endpoints were therefore regarded as descriptive only.
Table 2 aPWV measurements on day 168
Figure 2 Adjusted mean change from baseline in aPWV (m/s).
Abbreviations: aPWV, aortic pulse wave velocity; CI, confidence interval; COPD, chronic obstructive pulmonary disease; FF, fluticasone furoate; LS, least squares; SE, standard error; VI, vilanterol.
Exploratory analyses revealed no significant interactions of treatment with each of geographic region, age, gender, or smoking status on aPWV on day 168. There were no significant correlations between change from baseline in aPWV and central and peripheral systolic and diastolic BP, central and peripheral PP, central and peripheral mean arterial pressure (MAP), or trough FEV1. A significant correlation on day 168 was observed between aPWV and IC in the VI 25 µg arm (P=0.033); however, this was not observed with either the FF/VI 100/25 µg or placebo arm. No relationship was seen between aPWV and inflammatory biomarkers (hsCRP, fibrinogen, IL-6, PARC) (Figure S1).
Changes from baseline in AIx were minimal and similar in magnitude across the treatment groups (). There were no differences between groups in changes in central and peripheral PP. FF/VI 100/25 µg and VI 25 µg improved trough FEV1 from baseline, versus placebo (), and a numerical increase in IC was also observed at all time points with FF/VI 100/25 µg versus placebo ().
Table 3 Aortic AIx and blood pressure measurements on day 168
Figure 3 Adjusted treatment differences compared with placebo for lung function and health outcomes scores.
Abbreviations: CAT, COPD Assessment Test; COPD, chronic obstructive pulmonary disease; CI, confidence interval; FEV1, forced expiratory volume in 1 s; FF, fluticasone furoate; IC, inspiratory capacity; SGRQ, St George’s Respiratory Questionnaire for COPD patients; VI, vilanterol.
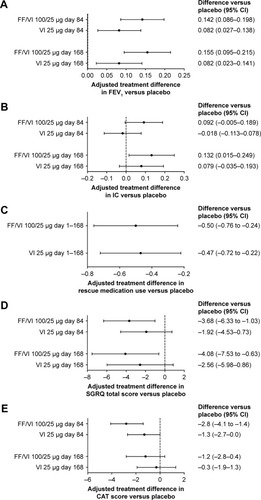
The mean number of albuterol uses in a 24-h period throughout treatment was reduced by FF/VI 100/25 µg and VI 25 µg versus placebo (). On day 168, SGRQ total score was reduced by 4.08 units with FF/VI 100/25 µg, versus placebo (). The adjusted mean change from baseline in CAT score was reduced for FF/VI 100/25 µg and VI 25 µg on day 168 ().
During the treatment period, 41 patients (10%) experienced a total of 42 moderate/severe COPD exacerbations (none were fatal); the incidence was the same in the placebo and VI 25 µg groups (11%) and lower in the FF/VI 100/25 µg group (6%).
Post hoc analyses
When withdrawn patients were classified as nonresponders, there was a higher proportion of responders in the FF/VI 100/25 µg (50%) and VI 25 µg (50%) groups, versus placebo (36%). The odds ratios (95% confidence interval [CI]) were 1.7 (1.0–2.8; nominal P=0.036) with FF/VI 100/25 µg and 1.8 (1.1–2.9; nominal P=0.017) with VI 25 µg, relative to placebo. When withdrawn patients were classified as missing, there remained more responders on FF/VI 100/25 µg (60%) and VI 25 µg (62%) compared with placebo (53%). The odds ratios (95% CI) were 1.3 (0.7–2.4) with FF/VI 100/25 µg and 1.5 (0.8–2.6) with VI 25 µg, relative to placebo.
There was no observed pattern between the effect of baseline aPWV on aPWV at day 168, and no trends by treatment arm (Figure S2).
Safety
The incidence of on-treatment AEs was higher in the FF/VI 100/25 µg (57%) and VI 25 µg (51%) groups compared with placebo (41%). The most frequently reported AE was nasopharyngitis (). Local steroid effects, primarily oral candidiasis, occurred predominantly with FF/VI 100/25 µg and were of mild or moderate intensity. Other AEs of special interest for ICS-/LABA-containing treatment were infrequent (incidences of pneumonia were ≤1% in all groups) (). Two fatal serious AEs were reported during the treatment period (); neither was considered by the investigator to be related to the study treatment.
Table 4 AEs, SAEs, AESI, and AEs leading to withdrawal
There were no differences between groups for changes in central or peripheral MAP, or systolic BP ().
Discussion
In this 24-week study, neither FF/VI 100/25 µg nor VI 25 µg had significant effects on arterial stiffness versus placebo. By contrast, the active treatments improved lung function (FEV1) and quality of life (SGRQ total score reached the minimally clinically important difference of 4 on day 168)Citation31 versus placebo. Although lung function is known to be inversely correlated with the elevated arterial stiffness,Citation32 this study did not find any associations, with the exception of one significant positive correlation between aPWV on day 168 and IC (VI 25 µg); however, this may be a chance finding as no similar correlation was observed with FF/VI 100/25 µg or placebo in this population with moderate airflow obstruction (across all treatment groups, the mean FEV1 was 50.1% [SD =13.34] of predicted normal values).
Arterial stiffness (measured by aPWV) provides incremental risk information to traditionally measured cardiovascular risk factors. Thus, elevated arterial stiffness is an indicator of cardiovascular risk reduction. aPWV increases with age, and for every 1 m/s increase in aPWV, cardiovascular risk increases by 15% in the general population;Citation33 COPD may accelerate this. Various mechanisms are implicated in the pathogenesis of accelerated atherosclerosis in COPD (oxidative stress, renin angiotensin system overactivation, and heightened sympathetic activity), but the strongest evidence points to systemic inflammation, which has been associated with an increased risk of cardiac injury in patients with moderate-to-severe airflow obstruction.Citation1,Citation16
A plausible connection between COPD and CVD lies in the vascular response to cigarette smoke (a risk factor for the development of COPD)Citation19 and hypoxic pulmonary vasoconstriction.Citation34 Evidence of endothelial dysfunction and vascular re-modeling have been detected both in individuals with COPD and in “healthy” individuals who smoke.Citation18 This could be due to shared risk factors such as cigarette smoking, which in addition to being a risk factor for airway obstruction,Citation16 is also known to induce vascular endothelial dysfunction.Citation18 Notably in this study, the smoking history (including years smoked, cigarettes per day, pack-years, and smoking status) was similar across the groups.
Anti-inflammatories and bronchodilators used in COPD can reduce arterial stiffness, which may modulate cardiovascular risk.Citation25,Citation26,Citation35 Short-acting beta2-agonists (and possibly LABAs) cause systemic vasodilation through the nitric oxide pathway.Citation36 A randomized study comparing fluticasone propionate/salmeterol with placebo reported no effect of active treatment on aPWV.Citation25 However, post hoc analysis suggested that participants with baseline aPWV >10.9 m/s had substantial reductions in arterial stiffness with fluticasone propionate/salmeterol.Citation25 Pepin et al showed that both FF/VI and tiotropium reduced aPWV in patients with elevated baseline aPWV.Citation26 However, that study was not placebo controlled and the reduction in stiffness in both the arms could be due to regression to the mean, since patients were included with high baseline aPWV. The present study included a placebo arm; although FEV1 was improved in the active treatment arms versus placebo, this study did not observe any significant change in aPWV between FF/VI 100/25 µg, VI 25 µg, and placebo. The mean reduction in aPWV across all arms attained the minimally clinically important difference of 1 m/sCitation37 and was likely due to regression to the mean as patients were recruited with elevated aPWV.
Systemic inflammation itself can also result in vascular remodeling and increased arterial stiffness;Citation16 however, the evidence for this relationship in COPD is unclear, with one study suggesting a weak association,Citation38 and no association has been demonstrated in other studies.Citation8,Citation9,Citation12,Citation23,Citation39 Approximately one-third of patients in the Evaluation of COPD to Longitudinally Identify Predictive Surrogate Endpoints (ECLIPSE) study had no baseline systemic inflammation, and only 16% showed persistent systemic inflammation.Citation40 This study did not observe reductions in inflammatory biomarkers with FF/VI 100/25 µg or VI 25 µg versus placebo, nor any correlation between systemic inflammation and elevated arterial stiffness.
Increased arterial stiffness is due to multiple factors, including senescence, elastin fiber breaks, collagen deposition, fibrosis, inflammation, and calcification.Citation16 Although the results suggest that ICS/LABA therapies do not reduce arterial stiffness, it is possible that the patients had arteries that were calcified and resistant to modulation. Patients with aPWV ≥11 m/s may have had heterogeneous causes of elevated stiffness that were less amenable to modulation; however, regardless of baseline aPWV, all patients had aPWV reductions during the study.
The uniform reduction of aPWV across all three arms cannot be easily explained. A systemic decrease in “white coat” effects over time may be hypothesized; however, data from a previous studyCitation25 do not agree. The requirement of a stable use of concomitant medications shown to influence aPWV might have led to a good compliance of taking those medications across all arms, which subsequently reduced aPWV for all patients. However, again, it does not seem to be the case for the previous studyCitation25 with the same requirement. This study has also noted a higher proportion of hypertensive patients in the placebo group compared with either active group in the present study, which may or may not have contributed to the reduction of aPWV with placebo; however, there were no significant changes between groups and anti-hypertensives were included in the list of concomitant medications for which a stable dose was required. The observation on aPWV in the present study cannot be directly compared with that in the other previous studyCitation26 that did not include placebo.
Safety findings were in line with established FF/VI 100/25 µg and VI 25 µg profiles. There were fewer COPD exacerbations in the FF/VI 100/25 µg group than in VI 25 µg or placebo. The incidence of pneumonia in the ICS-treated groups was not greater than that in the placebo group, which might be related to study duration,Citation41–Citation44 as the overall incidence of pneumonia was low in this study.
This study had some limitations. As mentioned previously, it was speculated that by selecting patients with a high baseline aPWV (decided a priori based on previous post hoc resultsCitation45), patients with calcified arteries and variable aPWV have been selected. Calcification was not measured directly in this study, but as the patients with higher baseline aPWV values had similar reductions in aPWV compared with patients with lower baseline aPWV, this did not seem to be the case. Additionally, the findings cannot be generalized to patients with COPD and low baseline aPWV. Furthermore, patients may have taken concomitant medications that could have impacted their aPWV during the study, but any such effects were unknown, and this was also the case in previous studies.Citation25,Citation26 Finally, as the sample size requirement was altered during the course of the study, an alpha adjustment may have been required if a significant difference in aPWV change had been detected with FF/VI 100/25 µg or VI 25 µg treatment, versus placebo.
The main strength of this study was that this was a prospective, randomized, blinded study with a placebo arm and active comparator arms. The VI 25 µg arm was included to elucidate the impact of ICS (FF) and LABA (VI). aPWV is the gold standard to measure arterial stiffness and the SphygmoCor CPVH system that has been used can accurately assess this parameter, which is predictive of CV outcomes.Citation46,Citation47 However, the measurement of endothelial function may provide valuable supportive information in future studies. Furthermore, dose regimens of permitted concomitant medications known to affect aPWV were maintained during the study, and to avoid impact on aPWV from patients’ previous medications, such as other ICS and LABAs, all these medications were excluded for an appropriate time period prior to the study.Citation48,Citation49
Conclusion
No differences were observed in aPWV-adjusted mean change from baseline for FF/VI 100/25 µg compared with placebo. More research is needed to identify responders to ICS/LABA therapy, who may derive CVD benefits from the treatment in addition to lung function improvements.
Acknowledgments
The authors would like to acknowledge the work of participating investigators at the study centers; Lori Hall, Lori DeMauro, and Rita Dhuna’s contributions on data management and study operation. Editorial support was provided by Jennifer Lawton, PhD, at Gardiner-Caldwell Communications (Macclesfield, UK) and was funded by GSK.
Disclosure
SPB has received an NIH KL2 Scholarship (1KL2TR001419); MTD has acted as a consultant for GSK, AstraZeneca, and Boston Scientific; JRC has acted as a consultant for GSK, NIVALIS, and Novartis and has received research support from GSK (NCT1656421); JW-J, DAM, DBR, CAS-W, and CC are employees of GSK and hold restricted/unrestricted GSK shares. Study HZC113108 (NCT1336608) was sponsored by GSK. The abstract of this paper was published in the American Thoracic Society International Conference Abstracts, B.23 Cardiovascular and Respiratory Interactions in COPD, Poster Discussion Session, Monday, May 16, 9:00 am to 11:00 am as an abstract with interim findings. The authors report no other conflicts of interest in this work.
References
- BhattSPDransfieldMTChronic obstructive pulmonary disease and cardiovascular diseaseTransl Res2013162423725123727296
- SinDDAnthonisenNRSorianoJBAgustiAGMortality in COPD: role of comorbiditiesEur Respir J20062861245125717138679
- SinDDManSFChronic obstructive pulmonary disease as a risk factor for cardiovascular morbidity and mortalityProc Am Thorac Soc20052181116113462
- HoleDJWattGCDavey-SmithGHartCLGillisCRHawthorneVMImpaired lung function and mortality risk in men and women: findings from the Renfrew and Paisley prospective population studyBmj19963137059711715 discussion 715–7168819439
- CurkendallSMDeLuiseCJonesJKCardiovascular disease in patients with chronic obstructive pulmonary disease, Saskatchewan Canada cardiovascular disease in COPD patientsAnn Epidemiol2006161637016039877
- ChenWThomasJSadatsafaviMFitzGeraldJMRisk of cardiovascular comorbidity in patients with chronic obstructive pulmonary disease: a systematic review and meta-analysisLancet Respir Med20153863163926208998
- TabaraYMuroSTakahashiYAirflow limitation in smokers is associated with arterial stiffness: the Nagahama StudyAtherosclerosis20142321596424401217
- McAllisterDAMaclayJDMillsNLArterial stiffness is independently associated with emphysema severity in patients with chronic obstructive pulmonary diseaseAm J Respir Crit Care Med2007176121208121417885263
- SabitRBoltonCEEdwardsPHArterial stiffness and osteoporosis in chronic obstructive pulmonary diseaseAm J Respir Crit Care Med2007175121259126517363772
- OdaMOmoriHOnoueAAssociation between airflow limitation severity and arterial stiffness as determined by the brachial-ankle pulse wave velocity: a cross-sectional studyIntern Med201554202569257526466690
- ChenRHeWZhangKAirflow obstruction was associated with elevation of brachial-ankle pulse wave velocity but not ankle-brachial index in aged patients with chronic obstructive pulmonary diseaseAtherosclerosis2015242113514026188536
- BhattSPColeAGWellsJMDeterminants of arterial stiffness in COPDBMC Pulm Med201414124387157
- Ben-ShlomoYSpearsMBoustredCAortic pulse wave velocity improves cardiovascular event prediction: an individual participant meta-analysis of prospective observational data from 17,635 subjectsJ Am Coll Cardiol201463763664624239664
- LaurentSAlivonMBeaussierHBoutouyriePAortic stiffness as a tissue biomarker for predicting future cardiovascular events in asymptomatic hypertensive subjects [abstract]Ann Med201244SupplS93S9722713154
- AgustiAFanerRSystemic inflammation and comorbidities in chronic obstructive pulmonary diseaseProc Am Thorac Soc201292434622550240
- SinDDManSFWhy are patients with chronic obstructive pulmonary disease at increased risk of cardiovascular diseases? The potential role of systemic inflammation in chronic obstructive pulmonary diseaseCirculation2003107111514151912654609
- CeceljaMChowienczykPMolecular mechanisms of arterial stiffeningPulse (Basel)201641434827493903
- Weir-McCallJRStruthersADLipworthBJHoustonJGThe role of pulmonary arterial stiffness in COPDRespir Med2015109111381139026095859
- VestboJHurdSSAgustiAGGlobal strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summaryAm J Respir Crit Care Med2013187434736522878278
- PieringerHStubyUHargassnerSBiesenbachGTreatment with corticosteroids reduces arterial stiffness in patients with polymyalgia rheumatica as measured with pulse wave analysisAnn Rheum Dis20086727918192309
- KalsJKampusPKalsMPulgesATeesaluRZilmerMEffects of stimulation of nitric oxide synthesis on large artery stiffness in patients with peripheral arterial diseaseAtherosclerosis2006185236837416051250
- DawesMChowienczykPJRitterJMEffects of inhibition of the L-arginine/nitric oxide pathway on vasodilation caused by beta-adrenergic agonists in human forearmCirculation1997959229322979142007
- GaleNSDuckersJMEnrightSCockcroftJRShaleDJBoltonCEDoes pulmonary rehabilitation address cardiovascular risk factors in patients with COPD?BMC Pulm Med2011112021510856
- VivodtzevIMinetCWuyamBSignificant improvement in arterial stiffness after endurance training in patients with COPDChest2010137358559219880908
- DransfieldMTCockcroftJRTownsendRREffect of fluticasone propionate/salmeterol on arterial stiffness in patients with COPDRespir Med201110591322133021696934
- PepinJLCockcroftJRMidwinterDSharmaSRubinDBAndreasSLong-acting bronchodilators and arterial stiffness in patients with COPD: a comparison of fluticasone furoate/vilanterol with tiotropiumChest201414661521153025058845
- BaberNInternational conference on harmonisation of technical requirements for registration of pharmaceuticals for human use (ICH)Br J Clin Pharmacol19943754014048054244
- RickhamPPHuman experimentation. Code of ethics of the world medical association. Declaration of HelsinkiBr Med J19642540217714150898
- GSK [Clinical Study Register – Study 113108]UKGlaxoSmithKline plc [updated April 2, 2015]. Available at http://www.gsk-clinical-studyregister.com/study/113108?study_ids=hzc113108#psAccessed April 14, 2016
- JonesPWHardingGBerryPWiklundIChenWHKline LeidyNDevelopment and first validation of the COPD assessment TestEur Respir J200934364865419720809
- JonesPWInterpreting thresholds for a clinically significant change in health status in asthma and COPDEur Respir J200219339840411936514
- BrunnerEJShipleyMJWitteDRArterial stiffness, physical function, and functional limitation: the Whitehall II StudyHypertension20115751003100921444833
- QvistLNilssonUJohanssonVCentral arterial stiffness is increased among subjects with severe and very severe COPD: report from a population-based cohort studyEur Clin Respir J2015162
- WuC-FLiuP-YWuT-JHungYYangS-PLinG-MTherapeutic modification of arterial stiffness: An update and comprehensive reviewWorld J Cardiol201571174275326635922
- SabitRBoltonCEAllanbyCCockcroftJRShaleDJArterial stiffness is reduced by combination inhaled corticosteroid/long acting beta-2 agonist therapy in patients with COPD [abstract]Thorax200762SupplA142
- DawesMChowienczykPJRitterJMEffects of inhibition of the L-arginine/nitric oxide pathway on vasodilation caused by beta-adrenergic agonists in human forearmCirculation1997959229322979142007
- LantelmePMestreCLievreMGressardAMilonHHeart rate: an important confounder of pulse wave velocity assessmentHypertension20023951083108712052846
- MillsNLMillerJJAnandAIncreased arterial stiffness in patients with chronic obstructive pulmonary disease: a mechanism for increased cardiovascular riskThorax200863430631118024535
- VanfleterenLESpruitMAGroenenMTArterial stiffness in patients with COPD: the role of systemic inflammation and the effects of pulmonary rehabilitationEur Respir J20144351306131524311762
- AgustiAEdwardsLDRennardSIPersistent systemic inflammation is associated with poor clinical outcomes in COPD: a novel phenotypePLoS One201275e3748322624038
- CrimCCalverleyPMAndersonJAPneumonia risk in COPD patients receiving inhaled corticosteroids alone or in combination: TORCH study resultsEur Respir J200934364164719443528
- KewKMSeniukovichAInhaled steroids and risk of pneumonia for chronic obstructive pulmonary diseaseCochrane Database Syst Rev20143CD010115
- LiapikouAToumbisMTorresAManaging the safety of inhaled corticosteroids in COPD and the risk of pneumoniaExpert Opin Drug Saf20151481237124726113207
- WedzichaJACalverleyPMSeemungalTAHaganGAnsariZStockleyRAINSPIRE InvestigatorsThe prevention of chronic obstructive pulmonary disease exacerbations by salmeterol/fluticasone propionate or tiotropium bromideAm J Respir Crit Care Med20081771192617916806
- VivodtzevIMinetCTamisierRArterial stiffness by pulse wave velocity in COPD: reliability and reproducibilityEur Respir J20134241140114224081763
- LaurentSCockcroftJVan BortelLExpert consensus document on arterial stiffness: methodological issues and clinical applicationsEur Heart J200627212588260517000623
- VlachopoulosCAznaouridisKStefanadisCPrediction of cardiovascular events and all-cause mortality with arterial stiffness: a systematic review and meta-analysisJ Am Coll Cardiol201055131318132720338492
- WeirDCRobertsonASGoveRIBurgePSTime course of response to oral and inhaled corticosteroids in non-asthmatic chronic airflow obstructionThorax19904521181212180106
- TwentymanOPFinnertyJPHarrisAPalmerJHolgateSTProtection against allergen-induced asthma by salmeterolLancet1990336133813421978163