
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Background
For patients with COPD, physical activity (PA) is recommended as the core component of pulmonary rehabilitation, but there is lack of a validated questionnaire for assessing the PA effectively.
Aim
To evaluate the reliability and validity of the Chinese version of Physical Activity Scale for the Elderly (PASE-C) in patients with COPD.
Methods
A cross-sectional study was conducted with 167 outpatients aged 60 years or older with COPD. Test−retest reliability and internal consistency were calculated by intraclass correlation coefficient (ICC) and Cronbach’s coefficient α, respectively. Validity was evaluated by correlation with the International Physical Activity Questionnaire-Short (IPAQ-S), data of pedometer, Self-Efficacy for Managing Chronic Disease 6-Item Scale (SES6), Hospital Anxiety and Depression Scale (HADS), Medical Outcomes Study 36-Item Short Form Health Survey (SF-36), grip strength, and disease characteristics.
Results
The PASE-C had an excellent seven-day test−retest reliability (ICC=0.98) and an acceptable internal consistency (Cronbach’s α=0.71). The content validity was supported by an item-content validity index, a scale-content validity index/universal agreement, and a scale-content validity index/average value of 0.70–1, 0.70, and 0.93, respectively. Concurrent validity was tested by correlation with IPAQ-S (r=0.651). Criterion validity was confirmed by correlation with the walking steps (r=0.611) and energy expenditure (r=0.493). For construct validity, PASE-C had correlations with SES6 (r=0.396), HADS for depression (r=−0.234), seven subscales of SF-36 (r=0.182–0.525), grip strength (r=0.341), and disease characteristics including the duration of COPD (r=−0.215), modified British Medical Research Council scale (r=−0.354), forced expiratory volume in one second as percentage of predicted (r=0.307), and Global Initiative for Chronic Obstructive Lung Disease grade (r=−0.264), with a good construct validity (all P<0.05).
Conclusion
The PASE-C has acceptable reliability and validity for patients aged 60 years or older with COPD, and it can be used as a valid tool to measure the PA of patients with COPD in the People’s Republic of China.
Video abstract
Point your SmartPhone at the code above. If you have a QR code reader the video abstract will appear. Or use:
Introduction
Physical activity (PA) is essential to maintain health in healthy and elderly people, especially in patients with chronic conditions.Citation1 PA makes its effect on patients through physiological and psychological mechanisms, such as fall of blood pressure and improvement of depression and anxiety.Citation2 Patients with COPD are commonly found to be physically inactive, compared with healthy subjects.Citation3
Long-term difficulty in breathing reduces exercise ability in patients with COPD leading them to perform only their regular activity,Citation4 and the prevalence of physical inactivity increases with the severity of COPD.Citation5,Citation6 COPD was recently characterized as a preventable and treatable disease, with significant systemic consequences.Citation7,Citation8
However, physical inactivity is considered to be causing the systemic consequences of COPD,Citation9 such as osteoporosis, weakness of skeletal muscle, and cardiovascular diseases.Citation10 In addition, physical inactivity would increase the rate of hospital admission,Citation11 and lead to decline in lung function.Citation12 A previous epidemiologic study showed that physical inactivity is positively associated with the mortality of patients with COPD.Citation11 PA and self-efficacy are the core components of pulmonary rehabilitation.Citation13,Citation14 PA is associated with self-efficacy, and increasing PA is related to improvements in psychological functioning and quality of life.Citation11,Citation15,Citation16
Recently, an increasing number of studies have focused on the effects of PA, screening of physical inactivity, and interventions for increasing PA, aimed to promote the development of recommendations that insist PA requirements to be taken into account for patients with COPD.Citation17,Citation18 However, there is lack of specific tools for an effective and quick assessment of PA in patients with COPD.Citation19 Obviously, finding a reliable and valid tool to assess PA in patients with COPD is the first and crucial step for further study.
There are two different approaches for assessing PA: objective approach including accelerometers and pedometers, and subjective approach mainly including questionnaires. Although objective approach can provide more precise measurements and is widely used for quantifying PA, compared with questionnaires, it is less practical to be used in clinical settings and is unable to distinguish different domain-specific activities.Citation20 Otherwise, questionnaires are inexpensive and not reactive to respondent’s behavior,Citation21 and are being widely applied in large-scale studies.Citation22
Recently, a systematic review showed that there were 13 PA questionnaires for the elderly until 2009, among which only three showed good reliability, including Physical Activity Scale for the Elderly (PASE). Compared with the two other questionnaires, PASE also showed good validity.Citation23 PASE is especially designed for older adults, and is the commonly used self-report measurement of PA, mainly dealing with frequency, duration, and intensity of different activities.Citation24 It has been validated and found to be reliable in several studies in older population,Citation25,Citation26 and in patients with end-stage renal disease and knee pain.Citation27,Citation28
Recently, PASE has been translated into Chinese, and been confirmed to have acceptable reliability and validity in older Chinese population in Hong Kong.Citation29,Citation30 PASE mainly comprises three components – leisure time (six questions), household (three questions), and work-related activities (one question) – which are relevant to patients with COPD.
To our knowledge, PASE has not been validated among Chinese patients aged 60 years or older with COPD. The aim of the this study was to assess the validity and reliability of the Chinese version of PASE (PASE-C) in patients with COPD, including test−retest reliability and measurement error, content validity, concurrent validity, criterion validity, and construct validity.
Methods
Patients
A double-center study was conducted in two tertiary hospitals in Tianjin, People’s Republic of China. A total of 167 outpatients with COPD were recruited in this study from May 2015 to February 2016. The diagnosis of COPD was based on 2016 GOLD (Global Initiative for Chronic Obstructive Lung Disease) guidelines.Citation31 Patients were eligible if they met the following criteria: 1) aged 60 years or older, 2) stable and having COPD with respiratory symptoms (dyspnea, cough, and sputum production) within normal day-to-day variation, and with no change in medication within the last four weeks, 3) able to understand and write Chinese, and 4) volunteering to participate and sign written informed consent. Exclusion criterion was having some disorders or progressive diseases (rheumatoid arthritis, cancer within the last five years, severe heart disease, severe osteoporosis, stroke, or multiple sclerosis), influencing daily life seriously.
Procedure
This study was approved by the Research Ethics Committee of the Tianjin Medical University. All outpatients were informed about the purpose and process of this study, and signed written informed consent was obtained from them. Participants completed a series of six instruments: demographic information, PASE-C and International Physical Activity Questionnaire-Short (IPAQ-S) to measure PA, Self-Efficacy for Managing Chronic Disease 6-Item Scale (SES6) to measure self-efficacy, Hospital Anxiety and Depression Scale (HADS) to measure mood status, and Medical Outcomes Study 36-Item Short Form Health Survey (SF-36) to measure health status. All participants completed these questionnaires at test session 1, and 35 participants were randomly selected to carry pedometer for seven consecutive days, and they completed the PASE-C again after they returned the pedometer at test session 2. All participants received the same instructions from the same researcher, and participants who were selected to carry pedometer were asked to maintain their usual PA during the time period.
Measures
The demographic variables included age, gender, marital status, education level, career, employment status, salary, place of residence, smoking status, and drinking status. The clinical variable included body mass index, heart rate, grip strength (kg), duration of COPD (months), comorbidities, grade of dyspnea (measured by the modified British Medical Research Council [mMRC] scale), frequency of exacerbation in the last year, forced expiratory volume in one second (FEV1) as percentage of predicted (FEV1% pred), and GOLD grade (according to GOLD 1 [mild]: FEV1≥80% predicted, GOLD 2 [moderate]: 50%≤FEV1<80% predicted, GOLD 3 [severe]: 30%≤FEV1<50% predicted, GOLD 4 [very severe]: FEV1<30% predicted).Citation32
PASE, used to assess PA for the elderly was designed by Washburn et al.Citation24 Vaughan and Miller translated the original English PASE into Chinese according to a forward−backward procedure.Citation30
The PASE-C comprises three components: leisure time, household, and work-related activities. Leisure time activities include sitting (L1), walking outside the home (L2), light activities (L3), moderate activities (L4), strenuous activities (L5), and muscle strength/endurance exercise (L6). Household activities include light housework (H7), heavy housework (H8) and home repairs, lawn work/yard care, outdoor gardening, and taking care of another person (H9). Work-related activities include paid or volunteer work (W10). The PASE-C scores were computed according to the weights of each activity and an equation, multiplying the amount of time spent (hours/day during the previous seven days) and participation (yes or no), which ranged from 0 to 500 or more. The PASE-C had acceptable reliability and validity in older Chinese population.Citation30
Steps were tested by a pedometer (SP600; Shenzhenshi Sibowei Technology Co., Ltd, Shenzhen, People’s Republic of China), which introduced the recent three-dimensional accelerometer transducer. The pedometer has a seven-day memory and records the total data, including the number of walking steps and energy expenditure per day. Patients carried the pedometers throughout the day, except while sleeping and bathing. The data for number of walking steps and energy expenditure for seven days were collected.
Grip strength was tested by a grip meter (WCS-100; Nantong Beisite Industry Co., Ltd, Jiangsu, People’s Republic of China). When patients were in the standing position with their feet a foot apart and two arms in the natural prolapsed position, a grip meter was used to measure the grip strength of the dominant hand twice. The higher reading was chosen for analysis.
PA was evaluated by IPAQ-S which was designed to measure PA including walking, moderate activity, and vigorous activity during the previous seven days.Citation33 Scores of the three levels of PA were calculated as frequencies and durations multiplied by known metabolic equivalent of task (MET): walking (3.3 METs), moderate activity (4.0 METs), and vigorous activity (8.0 METs). The scores of the three levels of PA were summed to obtain the total scores of IPAQ-S. IPAQ-S has been used among patients with COPD,Citation34 and has acceptable convergent validity.Citation35
Self-efficacy was evaluated by SES6 which was designed to assess perceived self-efficacy in patients with chronic diseases.Citation36 It is a six-item scale with score of each item ranging from 1 to 10, where 1 stands for no confidence and 10 stands for complete confidence. The total score is the average of the scores of the six items, which ranges from 1 to 10, with higher scores representing greater perceived self-efficacy.Citation36 SES6 has been used among patients with COPD, and the Cronbach’s α was 0.97.Citation37
Anxiety and depression were evaluated by HADS which was designed to measure mood disorders and identify the cases of anxiety and depression in patients with chronic diseases.Citation38 This scale includes 14-item groups divided into two subscales, and odd numbers and even numbers are separately used to measure anxiety (HADS-A) and depression (HADS-D). For each subscale, the total score ranges from 0 to 21. According to previous studies, anxiety or depression symptoms are classified in those patients who score 11 or more, borderline anxiety and depression symptoms are classified in those patients who score from 8 to 10, and score lower than 7 indicates no clinically relevant symptoms.Citation39,Citation40 The HADS which has satisfactory reliability and validityCitation41,Citation42 has been widely used to assess anxiety and depression in patients with COPD.Citation43,Citation44
Quality of life was evaluated by SF-36 which includes eight subscales: physical functioning, role-physical, bodily pain, general health, vitality, social functioning, role-emotional, and mental health.Citation45 The total scores of each subscale range from 0 to 100, and higher scores indicate good health status.Citation46 In addition, SF-36 has been validated in patients with COPD; for subscales of SF-36, the test−retest reliability was acceptable with the Cronbach’s α ranging from 0.75 to 0.99,Citation47 and the construct validity against physician’s evaluation of the patients’ overall health status showed low-to-moderate correlations (r=0.29–0.55).Citation48
Statistical analysis
Cross-cultural adaptations
PASE-C has been obtained from Vaughan and Miller.Citation30 A self-administered questionnaire is used in a new country or culture, and cross-cultural adaptations are essential to reach equivalence between original and target versions of the questionnaire.Citation49 In different countries or cultures, a given PA may not be experienced, even if the PA is translatable, so the item would have to be replaced by a similar item that is experienced in the target culture, which is called experiential equivalence.Citation50 Based on that, PASE-C was not tested in the People’s Republic of China, and PASE-C was required to achieve experiential equivalence to be adapted by the subjects of the People’s Republic of China. Three experts whose major was PA with at least five years of experience in independently conducting experiential equivalence, cited that some PAs are popularized in the People’s Republic of China according to the Compendium of Physical Activities, a coding scheme that classifies PA by energy expenditure.Citation51 The expert committee made critical decisions about the target version of PASE-C. For activities of walking, walking to buy breakfast was added into the examples. For light activities of sport and recreation, tai chi and yangko dance forms were added into the examples. For moderate activities of sport and recreation, brisk walking and flying kites were added into the examples. For strenuous activities of sport and recreation, playing badminton, skiing, and square dance were added into the examples.
All statistical analyses were conducted using IBM SPSS version 19.0 (SPSS, Chicago, IL, USA). For descriptive data, continuous variables were expressed as mean ± standard deviation (SD) or median (first to third quartiles, Q1−Q3) according to the Kolmogorov−Smirnov test, and categorical variables were expressed as relative frequencies and proportions. Significance level was set at a P-value of less than 0.05.
Reliability
Reliability was tested by test−retest reliability and internal consistency. Test−retest reliability of the PASE-C was calculated using intraclass correlation coefficient (ICC) for absolute agreement between the PASE-C scores at test sessions 1 and 2. ICC scores greater than 0.75 indicated good reliability.Citation52 Internal consistency of the scale was analyzed using Cronbach’s coefficient α.
Measurement error
In this research, measurement error was evaluated by the standard error of measurement (SEM), minimal detectable change (MDC), and limits of agreement (LoAs). SEM was calculated from the sample SD and the ICC of the scale according to the following formula:
MDC was calculated by the formula:
LoAs were evaluated through the visual judgment of the relationship between the PASE-C scores of each test and retest using the Bland–Altman plot, which was performed using MedCalc Software bvba (version 16.4.3).Citation55
Validity
The validity of PASE-C was based on content validity, concurrent validity, criterion validity, and construct validity. The content validity index (CVI) was separately evaluated by six experts (including three nurses and three doctors) and four patients. The experts were experienced in COPD and were familiar with the PA for COPD, and they had at least 10 years of working experience. The patients with at least five years’ history of COPD met the inclusion and exclusion criteria of this study. The Likert 4-point scale was used, where “4” indicated “very much relevance”, “3” indicated “strong relevance”, “2” indicated “weak relevance”, and “1” indicated “no relevance”. The CVI was reflexed by item-content validity index (I-CVI), scale-content validity index/universal agreement (S-CVI/UA), and scale-content validity index/average (S-CVI/Ave). The S-CVI/UA is the number of items scaled 3 or 4 divided by the total number of items, and the S-CVI/Ave is the average of I-CVI of each item.Citation56 The scale of I-CVI≥0.78 was considered acceptable,Citation57 the S-CVI/UA>0.8 showed good content validity,Citation58 and the S-CVI/Ave was considered to overpass 0.9.Citation59 Otherwise, experts were needed to provide explanation if they rated any item less than 3. The following are the formulas used for calculations of CVI.Citation56
Results
Characteristics of participants
A total of 167 outpatients with COPD were recruited in this study, with a mean age of 69.1±6.9 (range: 60–89) years. The demographic variables of patients with COPD are shown in , and the clinical variables are shown in . Among all, 35 outpatients completed the PASE-C twice and brought the pedometer with them for seven days.
Table 1 Demographic variables of patients with COPD (N=167)
Table 2 Clinical variables of patients with COPD (N=167)
Reliability
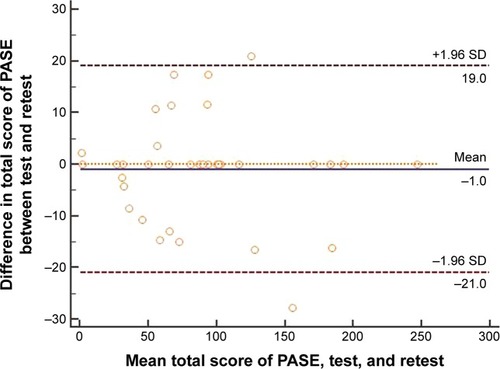
The PASE-C had an excellent seven-day test−retest reliability (ICC=0.98, 95% confidence interval: 0.96–0.99) and an acceptable internal consistency (Cronbach’s α=0.71). For measurement error, the SEM and MDC values were 6.93 and 19.21, respectively. The Bland–Altman plot for the PASE-C score of test and retest is shown in . The Bland–Altman plot nearly showed equal distribution on both sides of the zero line, and the upper LoA was 19.0 and the lower LoA was −21.0, of which two (6%) were not inside the LoA.
Figure 1 Bland–Altman plot for total score of PASE.
Abbreviations: SD, standard deviation; PASE, Physical Activity Scale for the Elderly.
Validity
The I-CVI values of the PASE-C items range from 0.70 to 1. Except for the I-CVI values of L6, H9, and W10 items, the I-CVI values of other items of this scale were 1. The S-CVI/Ave and S-CVI/UA values were 0.93 and 0.70, respectively. shows each expert’s ratings and calculation of CVI. For the lower I-CVI values of items, experts made some explanations. For L6 item, limited by the senility and disease, few patients had ability to do muscle strength/endurance exercise. For H9 item, home repair was a careful and time-consuming activity, which required some experts, and most patients lived in flat without garden, so they had little chance to do these activities. For W10 item, based on the Chinese work system, most people would retire when they are 60 years old, and volunteering is not popular in the People’s Republic of China, so work- or volunteer-related activities had little association with PA of patients aged 60 years or older with COPD. However, in order to ensure the popularity of PASE-C among those aged less than 60 years, we did not delete these items.
Table 3 Each expert’s rating and calculation of CVI
For concurrent validity, PASE-C scores had correlation with IPAQ-S scores (r=0.651, P<0.01). Criterion validity was confirmed by correlation with the walking steps (r=0.611, P<0.01) and energy expenditure (r=0.493, P<0.01). For construct validity, PASE-C scores had correlations with SES6 scores (r=0.396, P<0.01), HADS-D scores (r=−0.234, P<0.01), and seven subscales of SF-36 (r=0.182–0.525, P<0.01). In addition, the PASE-C scores had associations with grip strength (r=0.341, P<0.01), duration of COPD (r=−0.215, P<0.01), mMRC scale (r=−0.354, P<0.01), FEV1% pred (r=0.307, P<0.01), and GOLD grade (r=−0.264, P<0.01). shows the correlations between the PASE-C scores and clinical variables.
Table 4 Correlations between the PASE-C scores and clinical variables
Discussion
For patients with COPD, physical inactivity is common compared to age-matched controls, and physical inactivity would worsen disease progression.Citation66 Physical inactivity can predict the worse outcome of COPD, and has association with mortality and rate of hospital admission.Citation17 Therefore, assessing and increasing PA are becoming increasingly important. The aim of this study was to evaluate PA in patients with COPD using the well-validated PASE-C. To our knowledge, this is the first study in which the psychometric properties of the PASE-C were tested in Chinese patients with COPD. The reliability and validity results showed that the PASE-C was a simple and useful tool to measure the PA of patients aged 60 years or older with COPD in the People’s Republic of China.
In this study, the PASE-C scores were 73.25±49.47, which showed that the PA of patients aged 60 years or older with COPD was worse than that of general older people in the People’s Republic of China (t=5.069, P<0.001).Citation29
The ICC of PASE-C was 0.98, indicating that it had an excellent retest reliability.Citation52
The ICC was superior to the previous studies on elderly, which involved mail (r=0.84) and telephone samples (r=0.68) in the original study,Citation24 and ICC was 0.65 in the Japanese translation study by Hagiwara et alCitation26 and 0.79 in the Chinese translation study by Vaughan and Miller.Citation30 A Cronbach’s coefficient α greater than 0.7 is usually considered indicative of a reliable scale.Citation67 So, our results confirmed that the PASE-C has an acceptable internal consistency.
Two patients were not inside the LoA on the Bland–Altman plot which showed that there was a reporting bias. One of the outliers reported his PA decreased due to the weather, while the other explained that he should take care of his wife who was admitted to hospital recently, which led to increase in his PA. These conditions could explain the difference between test and retest. Thus, in this study, the bias between test and retest was minimal. With high ICC value, there were little measurement error and narrow LoA, and so we consider that the reliability of PASE-C is excellent.
In this study, the PASE-C showed good content validity. As a criterion, the I-CVI≥0.78 indicated that the item has an acceptable content validity.Citation57 However, the I-CVI of H9 was 0.70; hence, it is essential to make further modification. As in our previous hypothesis, concurrent validity was satisfactory due to PASE scores having high correlation with IPAQ-S scores, and criterion validity was acceptable due to PASE-C scores having high correlation with walking steps and moderate correlation with energy expenditure. For the construct validity, there were correlations between the PASE-C scores and SES6 scores, HADS-D scores, most of the subscales scores of SF-36, and disease characteristics, which mainly confirmed our previous hypotheses. So, the PASE-C showed satisfactory construct validity.
Limitations
Although the results indicated that the PASE-C is suitable to assess the population in this study, there are several limitations that need to be addressed. First of all, the original PASE was designed for elderly aged 65 years or older in developed countries, but in the People’s Republic of China, the elderly are defined as people aged 60 years or older. In this study, the participants were aged 60 years or older, which would influence the generalization in the world. Second, PASE-C scores had low correlations with HADS-D scores and some subscales scores of SF-36, which may be because HADS and SF-36 are not specific to patients with COPD, and it is essential to select more specific questionnaires in future study. Third, pedometer may underestimate or overestimate PA, so in order to test the validity of PASE more accurately, future study could use GOLD standard measures of PA as the criterion validity.
Conclusion
The PASE-C has shown acceptable psychometric properties for assessing the PA in patients aged 60 years or older with COPD. Therefore, it is a good method to evaluate PA in patients with COPD, and it can be popularized in the future based on its convenience and effectiveness.
Author contributions
All authors contributed to the conception, design, collection and analysis of data, as well as in the creation and critical review of the manuscript. All authors provided approval of the final manuscript.
Acknowledgments
The authors are grateful for the financial support from the Humanities and Social Science Research of China (Grant No 15YJA2H109), and thank William C. Miller, PhD, for providing the Chinese version of PASE for free. The authors express their appreciation to the staff and outpatients of the respiratory care unit of Tianjin First Center Hospital and Tianjin Chest Hospital for their support in data collection.
Disclosure
The authors report no conflicts of interest in this work.
References
- NelsonMERejeskiWJBlairSNAmerican College of Sports MedicineAmerican Heart AssociationPhysical activity and public health in older adults: recommendation from the American College of Sports Medicine and the American Heart AssociationCirculation200711691094110517671236
- WarburtonDENicolCWBredinSSHealth benefits of physical activity: the evidenceCMAJ2006174680180916534088
- TroostersTSciurbaFBattagliaSPhysical inactivity in patients with COPD, a controlled multi-center pilot-studyRespir Med201010471005101120167463
- ByromBRoweDAMeasuring free-living physical activity in COPD patients: deriving methodology standards for clinical trials through a review of research studiesContemp Clin Trials20164717218426806669
- WatzHWaschkiBBoehmeCClaussenMMeyerTMagnussenHExtrapulmonary effects of chronic obstructive pulmonary disease on physical activity: a cross-sectional studyAm J Respir Crit Care Med2008177774375118048807
- WatzHWaschkiBMeyerTMagnussenHPhysical activity in patients with COPDEur Respir J200933226227219010994
- CelliBRMacNeeWATS/ERS Task ForceStandards for the diagnosis and treatment of patients with COPD: a summary of the ATS/ERS position paperEur Respir J200423693294615219010
- RabeKFHurdSAnzuetoAGlobal Initiative for Chronic Obstructive Lung DiseaseGlobal strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summaryAm J Respir Crit Care Med2007176653255517507545
- NiciLDonnerCWoutersEATS/ERS Pulmonary Rehabilitation Writing CommitteeAmerican Thoracic Society/European Respiratory Society statement on pulmonary rehabilitationAm J Respir Crit Care Med2006173121390141316760357
- BoothFWGordonSECarlsonCJHamiltonMTWaging war on modern chronic diseases: primary prevention through exercise biologyJ Appl Physiol (1985)200088277478710658050
- Garcia-AymerichJLangePBenetMSchnohrPAntóJMRegular physical activity reduces hospital admission and mortality in chronic obstructive pulmonary disease: a population based cohort studyThorax200661977277816738033
- Garcia-AymerichJLangePBenetMSchnohrPAntóJMRegular physical activity modifies smoking-related lung function decline and reduces risk of chronic obstructive pulmonary disease: a population-based cohort studyAm J Respir Crit Care Med2007175545846317158282
- NiciLLareauSZuWallackRPulmonary rehabilitation in the treatment of chronic obstructive pulmonary diseaseAm Fam Physician201082665566020842995
- RochesterCLVogiatzisIHollandAEATS/ERS Task Force on Policy in Pulmonary RehabilitationAmerican Thoracic Society/European Respiratory Society statement on pulmonary rehabilitationAm J Respir Crit Care Med2015192111373138626623686
- BentsenSBWentzel-LarsenTHenriksenAHRokneBWahlAKSelf-efficacy as a predictor of improvement in health status and overall quality of life in pulmonary rehabilitation – an exploratory studyPatient Educ Couns201081151320356700
- GillDLHammondCCReifsteckEJPhysical activity and quality of lifeJ Prev Med Public Health201346Suppl 1S28S3423412703
- Gimeno-SantosFreiASteurer-SteyCPROactive consortiumDeterminants and outcomes of physical activity in patients with COPD: a systematic reviewThorax201469873173924558112
- HartmanJEBoezenHMZuidemaMJde GreefMHTen HackenNHPhysical activity recommendations in patients with chronic obstructive pulmonary diseaseRespiration20148829210024851826
- AraújoACOPD and physical activityRev Port Pneumol (2006)201622529930127094119
- HelmerhorstHJBrageSWarrenJBessonHEkelundUA systematic review of reliability and objective criterion-related validity of physical activity questionnairesInt J Behav Nutr Phys Act2012910322938557
- Munguía-IzquierdoDLegaz-ArreseAMannerkorpiKTranscultural adaptation and psychometric properties of a Spanish-language version of physical activity instruments for patients with fibromyalgiaArch Phys Med Rehabil201192228429421272726
- AinsworthBEHow do I measure physical activity in my patients? Questionnaires and objective methodsBr J Sports Med2009436918718977
- TerweeCBMokkinkLBvan PoppelMNChinapawMJvan MechelenWde VetHCQualitative attributes and measurement properties of physical activity questionnaires: a checklistSports Med201040752553720545379
- WashburnRASmithKWJetteAMJanneyCAThe physical activity scale for the elderly (PASE): development and evaluationJ Clin Epidemiol19934621531628437031
- DingerMKOmanRFTaylorELVeselySKAbleJStability and convergent validity of the Physical Activity Scale for the Elderly (PASE)J Sports Med Phys Fitness200444218619215470317
- HagiwaraAItoNSawaiKKazumaKValidity and reliability of the Physical Activity Scale for the Elderly (PASE) in Japanese elderly peopleGeriatr Gerontol Int20088314315118821997
- JohansenKLPainterPKent-BraunJAValidation of questionnaires to estimate physical activity and functioning in end-stage renal diseaseKidney Int20015931121112711231369
- DunlopDDSongJSemanikPASharmaLChangRWPhysical activity levels and functional performance in the osteoarthritis initiative: a graded relationshipArthritis Rheum201163112716320862681
- NgaiSPCheungRTLamPLChiuJKFungEYValidation and reliability of the Physical Activity Scale for the Elderly in Chinese populationJ Rehabil Med201244546246522549657
- VaughanKMillerWCValidity and reliability of the Chinese translation of the physical activity scale for the elderly (PASE)Disabil Rehabil201335319119722671717
- Global Initiative for Chronic Obstructive Lung DiseaseGlobal strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease – updated 2016 Available from: http://goldcopd.org/global-strategy-diagnosis-management-prevention-copd-2016Accessed July 20, 2016
- VestboJHurdSSAgustíAGGlobal strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summaryAm J Respir Crit Care Med2013187434736522878278
- CraigCLMarshallALSjöströmMInternational physical activity questionnaire: 12-country reliability and validityMed Sci Sports Exerc20033581381139512900694
- HirayamaFLeeAHBinnsCWLeongCCHiramatsuTPhysical activity of patients with chronic obstructive pulmonary disease: implications for pulmonary rehabilitationJ Cardiopulm Rehabil Prev200828533033418784544
- TödtKSkargrenEJakobssonPTheanderKUnossonMFactors associated with low physical activity in patients with chronic obstructive pulmonary disease: a cross-sectional studyScand J Caring Sci201529469770725653122
- LorigKStewartARitterPGonzálezVLaurentDLynchJOutcome Measures for Health Education and Other Health Care InterventionsThousand Oaks, CASage Publications1996
- StellefsonMChaneyBHChaneyJDExamining the efficacy of DVD technology compared to print-based material in COPD self-management education of rural patientsCalif J Health Promot200972264224163639
- ZigmondASSnaithRPThe Hospital Anxiety and Depression ScaleActa Psychiatr Scand19836763613706880820
- KrebberAMBuffartLMKleijnGPrevalence of depression in cancer patients: a meta-analysis of diagnostic interviews and self-report instrumentsPsychooncology201423212113024105788
- OlssønIMykletunADahlAAThe Hospital Anxiety and Depression Rating Scale: a cross-sectional study of psychometrics and case finding abilities in general practiceBMC Psychiatry200554616351733
- JohnstonMPollardBHennesseyPConstruct validation of Hospital Anxiety and Depression Scale with clinical populationsJ Psychosom Res200048657958411033377
- MykletunAStordalEDahlAAHospital Anxiety and Depression (HAD) scale: factor structure, item analyses and internal consistency in a large populationBr J Psychiatry200117954054411731359
- TrappenburgJCTroostersTSpruitMAVandebrouckNDecramerMGosselinkRPsychosocial conditions do not affect short-term outcome of multidisciplinary rehabilitation in chronic obstructive pulmonary diseaseArch Phys Med Rehabil2005861788179216181944
- BentsenSBRokneBWentzel-LarsenTHentiksenAHWahlAKThe Norwegian version of the chronic obstructive pulmonary disease self-efficacy scale (CSES): a validation and reliability studyScand J Caring Sci201024360060920534027
- StewartALWareJEMeasuring Functioning and Well-Being: The Medical Outcome Study ApproachDurham, NCDuke University Press1992
- WareJESnowKKSF-36 Health Survey Manual and Interpretation GuideBoston, MAThe Health Institute, New England Medical Center1993
- HarperRBrazierJEWaterhouseJCWaltersSJJonesNMHowardPComparison of outcome measures for patients with chronic obstructive pulmonary disease (COPD) in an outpatient settingThorax199752108798879404375
- BendtsenPLeijonMSommerASKristensonMMeasuring health-related quality of life in patients with chronic obstructive pulmonary disease in a routine hospital setting: feasibility and perceived valueHealth Qual Life Outcomes20031512740035
- BeatonDEBombardierCGuilleminFFerrazMBGuidelines for the process of cross-cultural adaptation of self-report measuresSpine (Phila Pa 1976)200025243186319111124735
- GuilleminFBombardierCBeatonDCross-cultural adaptation of health-related quality of life measures: literature review and proposed guidelinesJ Clin Epidemiol19934612141714328263569
- AinsworthBEHaskellWLWhittMCCompendium of physical activities: an update of activity codes and MET intensitiesMed Sci Sports Exerc2000329 SupplS498S50410993420
- MarxRGMenezesAHorovitzLJonesECWarrenRFA comparison of two time intervals for test-retest reliability of health status instrumentsJ Clin Epidemiol200356873073512954464
- AtkinsonGNevillAMStatistical methods for assessing measurement error (reliability) in variables relevant to sports medicineSports Med19982642172389820922
- TerweeCBBotSDde BoerMRQuality criteria were proposed for measurement properties of health status questionnairesJ Clin Epidemiol2007601344217161752
- BlandJMAltmanDGMeasuring agreement in method comparison studiesStat Methods Med Res19998213516010501650
- PolitDFBeckCTOwenSVIs the CVI an acceptable indicator of content validity? Appraisal and recommendationsRes Nurs Health200730445946717654487
- LynnMRDetermination and quantification of content validityNurs Res19863563823853640358
- DavisLLInstrument review: getting the most from your panel of expertsAppl Nurs Res199254194197
- WaltzCFStricklandOLLenzERMeasurement in Nursing and Health Research3rd edNew York, NYSpringer2005
- StreinerDLNormanGRHealth Measurement Scales: A Practical Guide to Their Development and UseOxfordOxford University Press2003
- SvegeIKolleERisbergMAReliability and validity of the Physical Activity Scale for the Elderly (PASE) in patients with hip osteoarthritisBMC Musculoskelet Disord2012132622353558
- ThompsonPDBuchnerDPinaILAmerican Heart Association Council on Clinical Cardiology Subcommittee on Exercise, Rehabilitation, and PreventionAmerican Heart Association Council on Nutrition, Physical Activity, and Metabolism Subcommittee on Physical ActivityExercise and physical activity in the prevention and treatment of atherosclerotic cardiovascular disease: a statement from the Council on Clinical Cardiology (Subcommittee on Exercise, Rehabilitation, and Prevention) and the Council on Nutrition, Physical Activity, and Metabolism (Subcommittee on Physical Activity)Circulation2003107243109311612821592
- SchüzNWaltersJACameron-TuckerHScottJWood-BakerRWaltersEHPatient anxiety and depression moderate the effects of increased self-management knowledge on physical activity: a secondary analysis of a randomised controlled trial on health-mentoring in COPDCOPD201512550250925774660
- Garcia-AymerichJFélezMAEscarrabillJPhysical activity and its determinants in severe chronic obstructive pulmonary diseaseMed Sci Sports Exerc200436101667167315595285
- DePewZSGarofoliACNovotnyPJBenzoRPScreening for severe physical inactivity in chronic obstructive pulmonary disease: the value of simple measures and the validation of two physical activity questionnairesChron Respir Dis2013101192723149382
- WatzHPittaFRochesterCLAn official European Respiratory Society statement on physical activity in COPDEur Respir J20144461521153725359358
- StreinerDLStarting at the beginning: an introduction to coefficient alpha and internal consistencyJ Pers Assess20038019910312584072