
Abstract
Background
COPD is a debilitating disease that affects patients’ daily lives. One’s daily physical activity (DPA) decreases due to multifactorial causes, and this decrease is correlated with a poor prognosis in COPD patients. Muscle wasting may at least be partly due to increased activity of the ubiquitin proteasome pathway and apoptosis.
Methods
This study investigated the relationships among DPA, circulating proteasome activity, and protein carbonyl in COPD patients and healthy subjects (HSs). This study included 57 participants (42 patients and 15 healthy subjects). Ambulatory DPA was measured using actigraphy, and oxygen saturation was measured with a pulse oximeter.
Results
COPD patients had lower DPA, lower 6 min walking distance (6MWD), lower delta saturation pulse oxygenation (SpO2) during the 6MWT, and lower delta SpO2 during DPA than HSs. COPD patients had higher proteasome activity and protein carbonyl than HSs. Circulating proteasome activity was significantly negatively correlated with DPA (r=−0.568, P<0.05) in COPD patients, whereas delta SpO2 during the 6MWT was significantly positively correlated with proteasome activity (r=0.685, P<0.05) in HSs. Protein carbonyl was significantly negatively correlated with the body mass index (r=−0.318, P<0.05), mid-arm circumference (r=0.350, P<0.05), calf circumference (r=0.322, P<0.05), forced expiratory volume in the first second (r=-0.441, P<0.01), and 6MWD (r=−0.313, P<0.05) in COPD patients. Our results showed no significant difference in inflammatory markers (interleukin-6 and tumor necrosis factor-α) or ubiquitin between the two groups.
Conclusion
COPD patients had lower DPA levels and higher circulating proteasome activity than HSs, and a negative correlation of DPA with circulating proteasome activity.
Background
COPD patients have pathology involving both the lungs and extrapulmonary abnormalities such as skeletal muscle wasting, cachexia, diabetes, and anemia.Citation1 The mechanistic basis underlying COPD is complex and can involve recurrent inflammation, oxidative stress, a protease/antiprotease imbalance, environmental results, and host genetics.Citation2
Muscle weakness, from atrophy and intrinsic metabolic abnormalities,Citation3 and a reduced exercise capacity are associated with increased mortality in COPD patients, independent of the severity of airflow obstruction.Citation4 Atrophy is mostly attributed to increased protein degradation, and the ubiquitin–proteasome pathway is involved in limb atrophy. Proteasomes regulate important intracellular functionsCitation5 by degrading intracellular proteins. Lower limb muscle atrophy is relatively common in persons with COPD. Calf circumference (CC) is highly associated with exercise tolerance, and it might be of value in predicting exercise intolerance in COPD patients.Citation6 Patients with severe COPD and hypoxemia exhibit greater levels of oxidative stress in their limb muscles, both at rest and after exercise, while showing a poorer quadriceps performance compared to healthy controls.Citation7
Physical activity is defined as any bodily movement produced by skeletal muscles that substantially increases energy expenditure.Citation8,Citation9 Low levels of physical activity are associated with systemic inflammation, left cardiac dysfunction,Citation10 low bone mineral density,Citation11 lung function decline, hospitalization, and mortality.Citation12 COPD is a debilitating disease affecting patients’ daily lives.Citation11 The etiology of reduced daily physical activity (DPA) in COPD patients is multifactorial.Citation13 A sedentary lifestyle, severe COPD, severity of dyspnea, dynamic hyperinflation,Citation14 worse leg muscle function, long-term oxygen therapy, and extrapulmonary effects of COPDCitation10 were independently associated with lower physical activity.Citation15 It is not known if any relationship of proteasomes exists with oxidative stress that develops during DPAs and the functional exercise capacity of patients with COPD. The objectives of this study were to analyze the contributions of DPA, exercise capacity (assessed by the 6 min walking distance [6MWD]), oxidative stress, and systemic inflammation to the circulating proteasome concentration of patients with COPD.
Methods
Study design and patients
We conducted a cross-sectional study in persons who were recruited from the pulmonary outpatient unit of a medical center and healthy volunteers. A diagnosis of COPD was based on the Global Initiative for Chronic Obstructive Lung Disease guidelines.Citation16 Those with an acute infection or acute exacerbation were excluded. In total, 42 patients and 15 healthy subjects (HSs) were qualified and agreed to participate. All participants had similar physical activity patterns during weekdays or weekends and were in a stable condition, and COPD patients were undergoing standard pharmacologic treatment. The study protocol was approved by the Ethics Committee of the Taipei Medical University-Joint Institutional Review Board, and all subjects provided written informed consent before taking part in the study.
Procedures and measurements
Participants were interviewed by well-trained researchers to collect demographic, lifestyle, and disease-related data. Participants’ weight, height, body fat (%), mid-arm circumference (MAC), and CC were measured, and the physical function capacity was evaluated by a well-trained therapist with the 6MWT and pulmonary function tests. Weight, height, MAC, and CC were measured according to standard methods. The body mass index (BMI) was calculated as the weight divided by the height squared (kg/m2). A bioelectrical impedance analysis (TANITA, BF-800 Body Fat Monitor; Tanita, Tokyo, Japan) was performed to determine the percentage body fat. The fat-free mass was calculated from the body weight minus the fat mass. The fat-free mass index was calculated as the fat-free mass (kg)/height (m).Citation17
Enzyme-linked immunosorbent assays were used to determine the plasma levels of interleukin (IL)-6 (eBioscience, San Diego, CA, USA), tumor necrosis factor (TNF)-α (eBioscience), protein carbonyl (Cell Biolabs, San Diego, CA, USA), ubiquitin (Mybiosource, San Diego, CA, USA), and proteasome activity (Biovision, Milpitas, CA, USA), according to the manufacturers’ instructions.
Pulmonary function parameters were assessed using the Vitalograph Spirotac V™ after a 10 min rest; the post-bronchodilator forced expiratory volume in the first second (FEV1) and forced vital capacity (FVC) were measured, and the FEV1/FVC ratio was calculated. All included COPD patients had an FEV1/FVC ratio of <70%.
The exercise capacity was assessed with the 6MWT, according to American Thoracic Society (ATS) guidelines. All subjects were instructed to walk as far as possible, but were allowed to stop and rest during the test.Citation18 Oxygen saturation was recorded using a continuous finger-adapted pulse oximeter.
Oxygen saturation was measured during DPA; we monitored oxygenation with an oximeter (WristOx; Nonin Medical, Plymouth, MN, USA) and daily activity using a Micro-Mini Motionlogger® Actigraph (MM; Ambulatory Monitoring Inc., Ardsley, New York, USA). Each patient underwent an ambulatory recording that produced 24 h of continuous data and a daily-card record. DPA refers to the amount of activities excluding sleep time. We used a desaturation index or percent time for oxygen saturation, which was <90% during the recording.Citation19
Statistical analysis
Results were statistically analyzed with SPSS for Windows 19.0 (IBM Corporation, Armonk, NY, USA) and the pro-gram GraphPad Prism 5 (GraphPad Software, La Jolla, CA, USA). Descriptive data are expressed as the mean ± standard deviation (SD). Continuous variables were compared using Student’s t-test, and categorical variables were compared between the two groups using a chi-squared test. Pearson’s correlation was used to evaluate the strength of the relationship between the ubiquitin–proteasome system and DPA indicators measured with the actigraph. Statistical significance for all evaluations was set at P<0.05.
Results
Baseline characteristics
Descriptive statistics for the variables studied are shown in . Mean ages were similar in HSs and COPD subjects (64.1±11.7 vs 67.1±6.5 years, P>0.05). Anthropometric data for HSs and patients with COPD did not differ significantly. Most COPD patients had a smoking history (92.8%), and they averaged 36.5±23.6 pack-years. As expected, pulmonary function values were significantly lower in COPD patients than in HSs, and COPD patients were in a severe stage (FEV1 =40.5%±16.5%; FEV1/FVC =48.7%±11.0%).
Table 1 Characteristics of the 57 participants
Decreased DPA in COPD patients
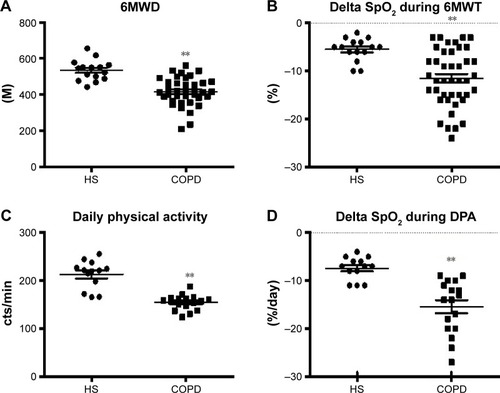
As shown in and , the 6MWD (416.3±11.7 vs 535.1±14.2 m, P<0.01) and delta saturation pulse oxygenation (SpO2; −11.5%±0.9% vs −5.5%±0.6%, P<0.01) were lower in COPD patients than in HSs; the actigraphic record also showed lower DPA (154.4±3.8 vs 213.1±8.1 counts/min, P<0.01) and delta SpO2 (−15.4%±1.4% vs −7.4%±0.7%, P<0.01) in COPD patients.
Figure 1 (A) 6MWD during the 6MWT in healthy subjects and COPD patients. (B) Delta SpO2 during the 6MWT in healthy subjects and COPD patients. (C) DPA in healthy subjects and COPD patients. (D) Delta SpO2 during DPA in healthy subjects and COPD patients. **P<0.01 between groups.
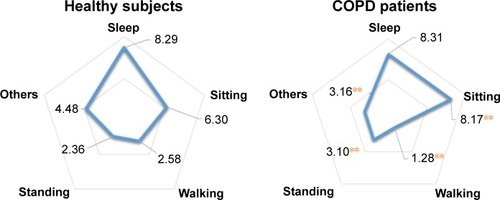
shows the all-day activity distribution. Time spent walking by the COPD patients was lower than that of HSs (1.28±5.36 vs 2.58±0.31 h, P<0.01), while their standing time (3.10±0.12 vs 2.36±0.20 h, P<0.01) and sitting time (8.17±0.22 vs 6.30±0.29 h, P<0.01) were higher than those of HSs and no significant difference was found for lying down time (8.31±0.25 vs 8.29±0.30 h, P>0.05). Our results showed that COPD patients had changed their lifestyle, with over 34% exhibiting a sedentary lifestyle and had reduced their daily activities.
Figure 2 Time spent in each of the activities or body positions in healthy subjects and COPD patients during the entire day.
Increased serum oxidative stress and proteasome activity in COPD patients
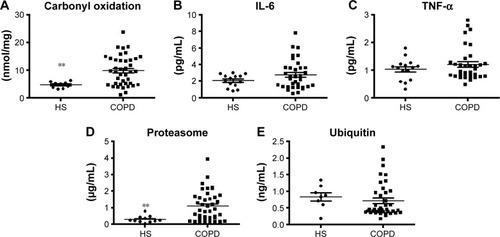
Levels of protein carbonyl, IL-6, TNF-α, proteasome activity, and ubiquitin in HSs and COPD patients are presented in and . In COPD patients, serum levels of protein carbonyl (9.88±5.36 vs 4.72±1.16 nmol/mg, P<0.01) and proteasome activity (1.14±0.88 vs 0.29±0.21 µg/mL, P<0.01) were higher than those in HSs; no significant difference was seen in the levels of IL-6 (2.78±1.76 vs 2.07±0.76 pg/mL, P>0.05), TNF-α (1.21±0.10 vs 1.903±0.39 pg/mL, P>0.05), or ubiquitin (0.72±0.51 vs 0.83±0.35 ng/mL, P>0.05).
Figure 3 (A) Serum protein carbonyl levels in healthy subjects and subjects with COPD. (B) IL-6 levels in healthy subjects and COPD patients. (C) Serum TNF-α levels in healthy subjects and COPD patients. (D) Serum proteasome activity in healthy subjects and COPD patients. (E) Serum ubiquitin levels in healthy subjects and COPD patients. **P<0.01 between groups.
Serum proteasomes, not oxidative stress, are associated with decreased DPA
shows the Pearson’s correlation coefficients of proteasome activity, protein carbonyl, anthropometric indicators, actigraphic data, the 6MWD, and delta SpO2 during the 6MWT. In all subjects, the MAC, CC, FEV1, and 6MWD were significantly correlated with carbonyl oxidation (r=−0.323, P<0.05; r=−0.340, P<0.05; r=−0.526, P<0.01; and r=−0.439, P<0.05, respectively), but there was no significant correlation with proteasome activity (P>0.05). Neither the BMI, fat-free mass index, delta SpO2 during DPA, nor the delta SpO2 during 6MWT was significantly correlated with proteasome activity or protein carbonyl (all P<0.05). DPA was significantly correlated with proteasome activity (r=−0.529, P<0.05), but not with protein carbonyl (r=0.089, P>0.05). In HSs, no parameters, except delta SpO2 during the 6MWT which was significantly positively correlated with proteasome activity (r=0.685, P<0.05), were significantly correlated with proteasome activity or protein carbonyl (all P>0.05). In COPD patients, except DPA which was significantly negatively correlated with proteasome activity (r=−0.568, P<0.05), no other parameters were significantly correlated with proteasome activity; the BMI, MAC, CC, FEV1, and 6MWD were significantly correlated with protein carbonyl (r=−0.318, P<0.05; r=−0.350, P<0.05; r=−0.322, P<0.05; r=−0.441, P<0.01; and r=−0.313, P<0.05, respectively).
Table 2 Pearson’s correlation coefficients (r) of proteasome activity, protein carbonyl, and functional physical activity in subjects
Discussion
The primary findings of this study are that serum proteasome activities were correlated with DPA in patients with COPD and with delta SpO2 during the 6MWT in HSs, but there was no significant correlation with airflow obstruction severity. In addition, patients with COPD had higher protein carbonyl and proteasome activity than HSs. Finally, this study showed that a reduced 6MWD and lower SpO2 during the 6MWT were the best surrogate markers of inactivity during the daily physical life of COPD patients.
The origin and function of blood proteasomes in patients with COPD are unclear. However, our data showed that COPD patients had higher proteasome activity and lower exercise activity than HSs, and the serum proteasome activity appeared to be correlated with low DPA and delta SpO2.
DPA was observed to be lower in COPD patients than in healthy controls and lower than the proposed international guidelines for physical health maintenance.Citation20 COPD patients spent less than one-third of their time walking and standing, and therefore spent much more time sitting or lying around, while HSs spent more than half of their time walking or standing.Citation21 In our study, COPD patients spent 1.28 h of their time walking and more than one-third of their time sitting or lying down, while HSs spent 2.95 h of their time walking and 5.28 h, or less than one-third of their time, sitting. The World Health Organization guidelines for physical activity recommend that all adults should undertake at least 2.5 h of moderate-intensity aerobic activity per week, such as walking, to maintain a healthy lifestyle. In COPD patients, sedentary behaviors are believed to be crucial to the development of skeletal muscle weakness, and resting and exercise muscle metabolism is impaired.Citation22
Inflammation in COPD also leads to a protein catabolic state. COPD patients appear to be under a state of continuous systemic inflammation, as suggested by high levels of C-reactive protein, oxidative stress, and other proinflammatory mediators.Citation23 Our results showed no significant differences in any inflammatory marker between the two groups. Oxidative stress may act as a potential mechanism in the pathogenesis of COPD patients.Citation24 Compared to HSs, COPD patients were characterized by increased systemic and pulmonary oxidative stress markers both at rest and those induced by exercise, and this result suggests that healthy control subjects are able to tolerate exercise more effectively than COPD patients.Citation25 This study observed higher carbonyl oxidation levels in COPD patients, which were higher than those of HSs. We observed that the levels of protein carbonyl were correlated with the airflow obstruction severity in FEV1; this result is similar to that of a past study,Citation26 but there was no correlation with functional physical activity.
Limitations
This study has some limitations. First, this study has a relatively small sample size, and the study sample was drawn from a single hospital. Therefore, larger sample sizes from different centers are needed to confirm our results. Second, the function and mechanism of circulating proteasomes were not evaluated in this study. Further studies are needed to clarify their function and mechanism. Third, this study involved only 24 h ambulatory actigraphy and oximetry, and not all HSs and COPD patients had DPA and SpO2 measured. The applicability of these results to longer periods of actigraphy and oximetry requires further investigation. Fourth, inactivity may not only lead to more proteasome activity, but also cachexia, and the associated high proteasome activity may lead to less daily activity. This study design could not establish causal relationships. Finally, most patients referred to this center were male; hence, we could not assess the effect of gender. Further samples are needed to increase female participation.
Conclusion
Circulating proteasome activities were significantly and negatively correlated with DPA in COPD patients. Our findings suggest that circulating proteasome activity and daily functional activities are related. Further longitudinal observations and exercise interventional studies are required to establish whether this link is causal in nature.
Author contributions
Kang-Yun Lee and Tzu-Tao Chen conceived the idea, designed, carried out the study, and performed the statistical analysis. Ling-Ling Chiang, Hsiao-Chi Chuang, Po-Hao Feng, Wen-Te Liu, and Kuan-Yuan Chen assisted in subject recruiting and helped to carry out the study. Shu-Chuan Ho directed the statistical analysis, data interpretation, and was the main writer of the manuscript. All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work. All authors have read and approved the final version of the manuscript for publication.
Acknowledgments
The authors wish to thank the patients and personnel of the hospital unit for their cooperation during the course of this study. The authors wish to thank Ms Yi-Syuan Lin and Mr Lu-Wei Kuo for their technical assistance with this research.
The study was supported by grants from the Taipei Medical University (TMU102-AE1-B45, TMU103-AE1-B31) and Taipei Medical University-Shuang Ho Hospital (103TMU-SHH-01–4, 103TMU-SHH-01–2, and 104TMU-SHH-24).
Disclosure
The authors report no conflicts of interest in this work.
References
- KiyokawaHMuroSOgumaTImpact of COPD exacerbations on osteoporosis assessed by chest CT scanCOPD20129323524222360380
- FischerBMPavliskoEVoynowJAPathogenic triad in COPD: oxidative stress, protease-antiprotease imbalance, and inflammationInt J Chron Obstruct Pulmon Dis2011641342121857781
- MadorMJDenizOAggarwalAKufelTJQuadriceps fatigability after single muscle exercise in patients with chronic obstructive pulmonary diseaseAm J Respir Crit Care Med200316810210812689846
- GosselinkRTroostersTDecramerMPeripheral muscle weakness contributes to exercise limitation in COPDAm J Respir Crit Care Med19961539769808630582
- BaumeisterWWalzJZuhlFSeemullerEThe proteasome: paradigm of a self-compartmentalizing proteaseCell19989233673809476896
- HoSCHsuMFKuoHPThe relationship between anthropometric indicators and walking distance in patients with chronic obstructive pulmonary diseaseInt J Chron Obstruct Pulmon Dis2015101857186226392760
- KoechlinCMaltaisFSaeyDHypoxaemia enhances peripheral muscle oxidative stress in chronic obstructive pulmonary diseaseThorax2005601083484115964914
- CaspersenCJPowellKEChristensonGMPhysical activity, exercise, and physical fitness: definitions and distinctions for health-related researchPublic Health Rep198510021261313920711
- ThompsonPDBuchnerDPinaILExercise and physical activity in the prevention and treatment of atherosclerotic cardiovascular disease: a statement from the Council on Clinical Cardiology (Subcommittee on Exercise, Rehabilitation, and Prevention) and the Council on Nutrition, Physical Activity, and Metabolism (Subcommittee on Physical Activity)Circulation2003107243109311612821592
- WatzHWaschkiBBoehmeCClaussenMMeyarTMagnussenHExtrapulmonary effects of chronic obstructive pulmonary disease on physical activity: a cross-sectional studyAm J Respir Crit Care Med2008177774375118048807
- LiuWTKuoHPLiaoTHLow bone mineral density in COPD patients with osteoporosis is related to low daily physical activity and high COPD assessment test scoresInt J Chron Obstruct Pulmon Dis2015101737174426366066
- Garcia-AymerichJLangePBenetMSchnohrPAntoJMRegular physical activity reduces hospital admission and mortality in chronic obstructive pulmonary disease: a population based cohort studyThorax200661977277816738033
- PittaFTroostersTProbstVSPossíveis conseqüências de não se atingir a mínima atividade física diária recomendada em pacientes com doença pulmonar obstrutiva cronica estável [Potential consequences for stable chronic obstructive pulmonary disease patients who do not get the recommended minimum daily amount of physical activity]J Bras Pneumol2006324301308 Portuguese17268729
- Garcia-RioFLoresVMedianoODaily physical activity in patients with chronic obstructive pulmonary disease is mainly associated with dynamic hyperinflationAm J Respir Crit Care Med2009180650651219542481
- de KamDSmuldersEWeerdesteynVSmits-EngelsmanBCExercise interventions to reduce fall-related fractures and their risk factors in individuals with low bone density: a systematic review of randomized controlled trialsOsteoporos Int200920122111212519421702
- RabeKFHurdSAnzuetoAGlobal strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summaryAm J Respir Crit Care Med2007176653255517507545
- HsuMFHoSCKuoHPWangJYTsaiACMini-nutritional assessment (MNA) is useful for assessing the nutritional status of patients with chronic obstructive pulmonary disease: a cross-sectional studyCOPD201411332533224475999
- ATS Committee on Proficiency Standards for Clinical Pulmonary Function LaboratoriesATS statement: guidelines for the six-minute walk testAm J Respir Crit Care Med2002166111111712091180
- CasanovaCHernandezMCSanchezATwenty-four-hour ambulatory oximetry monitoring in COPD patients with moderate hypoxemiaRespir Care200651121416142317134522
- BossenbroekLde GreefMHWempeJBKrijnenWPTen HackenNHDaily physical activity in patients with chronic obstructive pulmonary disease: a systematic reviewCOPD2011830631921728804
- PittaFTroostersTSpruitMAProbstVSDecramerMGosselinkRCharacteristics of physical activities in daily life in chronic obstructive pulmonary diseaseAm J Respir Crit Care Med2005171997297715665324
- EngelenMPScholsAMDoesJDGoskerHRDeutzNEWountersEFExercise-induced lactate increase in relation to muscle substrates in patients with chronic obstructive pulmonary diseaseAm J Respir Crit Care Med200016251697170411069799
- BoltonCEEvansMIonescuAAInsulin resistance and inflammation – A further systemic complication of COPDCOPD20074212112617530505
- KirkhamPABarnesPJOxidative stress in COPDChest201314426627323880677
- PinhoRAChiesaDMezzomoKMOxidative stress in chronic obstructive pulmonary disease patients submitted to a rehabilitation programRespir Med200710181830183517376663
- RahmanIvan SchadewijkAACrowtherAJ4-Hydroxy-2-nonenal, a specific lipid peroxidation product, is elevated in lungs of patients with chronic obstructive pulmonary diseaseAm J Respir Crit Care Med2002166449049512186826