
Abstract
Cigarette smoking results in the accumulation of iron both systemically and locally, in the lung thereby causing imbalance in iron homeostasis. This disruption in iron homeostasis can be associated with oxidative stress and consequent tissue injury. Therefore, in this study, we tested the association between iron homeostasis and airway obstruction by examining a large cohort of smokers and non-smokers for relationships between 1) serum ferritin and iron concentrations and transferrin saturation and 2) forced vital capacity (FVC), forced expiratory volume in 1 s (FEV1), and their ratio (FEV1/FVC). Data from the National Health and Examination Survey III were analyzed. The study population included persons aged 20 years and above with their following data recorded: race, gender, serum ferritin and iron concentrations, and transferrin saturation; the final sample number was 7,251. In the total population, Pearson correlation coefficients between 1) serum ferritin and iron concentrations and transferrin saturation and 2) FVC and FEV1 were significantly positive; whereas those between 1) serum ferritin concentrations and transferrin saturation and 2) FEV1/FVC were significantly negative. With separate analyses, serum ferritin concentrations demonstrated positive associations with FVC and FEV1 but an inverse relationship with FEV1/FVC in smokers and non-smokers. Serum ferritin levels increased with worsening airway obstruction among smokers, and its highest concentrations were found among those with the lowest values of FEV1/FVC ratio (<60%). Comparable to cigarette smokers, serum ferritin concentrations among non-smokers were greatest in those with the lowest FEV1/FVC ratio. Furthermore, elevated levels of serum iron and saturation of transferrin also corresponded with decreased FEV1/FVC ratio among non-smokers. Thus, we conclude that indices of iron homeostasis are associated with airway obstruction in both smokers and non-smokers.
Introduction
Smoking a single cigarette exposes the human respiratory tract to high levels of particulate matter (PM) (between 15,000 and 40,000 µg PM).Citation1 PM is deposited in the human lung at a high rate.Citation2 Furthermore, incomplete oxidation of tobacco leaves produces oxygen-containing functional groups (eg, carboxylates, esters, and phenolic hydroxides) at the surface of the retained cigarette smoke particles.Citation2 Following dissociation of proton at physiological pH level, the aforementioned functional groups introduce a negatively charged solid–liquid interface into the lung tissue. Furthermore, Fe3+ has a high affinity toward oxygen-donor ligands due to its electropositivity, and thus, it forms complexes with the PM deposited from cigarette smoke.Citation3 Subsequently, these complexes accumulate on the surface of the lungs of smokers.Citation4 However, elevated iron concentrations are observed not only in the lower respiratory tract but systemically as well.Citation4,Citation5 Reflecting this disruption in the homeostasis of iron and its accumulation, serum concentrations of ferritin, a metal storage protein, and iron concentrations increase in cigarette smokers.Citation5 Similarly, saturation of transferrin, an iron transport protein, is elevated in the serum of smokers.Citation5 The disruption in iron homeostasis in smokers can be associated with oxidative stress, which triggers a cascade of biochemical events culminating in inflammation, fibrosis, and cancer, both locally in the lungs and systemically.
COPD most frequently refers to the combination of chronic bronchitis and emphysema, a pair of commonly co-existing lung diseases in which the airways become functionally narrowed. The vast majority of COPD in the United States is the result of cigarette smoking. A fundamental characteristic of COPD is the physiological limitation of the expiratory flow of air from the lungs, which is irreversible. One of the best indicators of airflow obstruction is the ratio of forced expiratory volume in 1 s (FEV1) to forced vital capacity (FVC).Citation6 The natural course of COPD is characterized by a gradual worsening of obstruction (ie, FEV1/FVC ratio decreases) over years with exacerbations of airflow obstruction caused by infections and air pollution.
Disruption in iron homeostasis with the subsequent accumulation of this metal has been proposed to contribute to COPD.Citation7,Citation8 If metal-associated biological effects (eg, oxidative stress) contribute to lung injury following smoking, an accumulation of iron following cigarette smoking should correlate with physiological indices of damage. Therefore, in this study, we evaluated the association between iron homeostasis and airway obstruction by examining a large cohort of both smokers and non-smokers for relationships between 1) serum concentrations of ferritin and iron and transferrin saturation and 2) FVC, FEV1, and their ratio (FEV1/FVC).
Materials and methods
Study population
Data from the National Health and Nutrition Examination Survey III (NHANES III, conducted 1988 to 1994) were analyzed. The study population included persons aged 20 years and above with their following data recorded: race, gender, serum ferritin and iron concentrations, serum transferrin saturation, and serum C-reactive protein. Of the 13,941 persons initially selected, 2,944 were excluded as they reported a respiratory infection at either the time of or within 3 weeks prior to the interview. Individuals were categorized as either “smoker” or “non-smoker”. A smoker was defined as a person who reported smoking cigarettes for at least 1 year duration at the time of interview. A nonsmoker was defined as a person who reported smoking less than 100 cigarettes during their lifetime, and whose serum cotinine concentration was less than 1.0 ng/mL. Records of 3,746 persons who did not fit the definitions of “smoker” and “non-smoker” were eliminated from the database for a final sample size of 7,251 individuals.
Blood indices and pulmonary function tests
Measurements of blood endpoints and pulmonary function indices are provided in detail.Citation9
Data analysis
Analyses were performed using SAS and WesVar statistical software (SAS Institute, Inc., Cary, NC, USA and Westat, Rockville, MD, USA, respectively) enabling weighting and adjustment for the survey sampling methodology in estimating variances during the final analysis. Data analysis was performed to explore variable distributions and correlations. Geometric means and standard errors (SE) of FVC, FEV1, FEV1/FVC ratio, serum concentrations of ferritin and iron, transferrin saturation, and serum levels of C-reactive protein are reported. Age categories of 10 year increments were created; results are described by the first year of age in each category. Pearson product-moment correlation coefficients were calculated. Tests were two-sided. Significance was set at P<0.05.
Results
Demographic characteristics of the study population, smoking status, and FEV1/FVC values are provided in . There were 2,549 (35%) smokers and 4,702 (65%) non-smokers. Forty-nine percent of the cohort was between 20 and 39 years of age and only 13% was above the age 70 years.
Table 1 Characterization of the study population
In the study population, serum ferritin and iron concentrations, transferrin saturation, and C-reactive protein levels had means (± SE) of 73.8±1.7 ng/mL (166±4 pmol/L), 80.4±0.6 µg/dL (14.4±0.1 µmol/L), 22.9%±0.2%, and 0.31±0.01 mg/dL (30±1 nmol/L), respectively. The log-transformed values of serum ferritin and iron concentrations and transferrin saturation more closely approximated a normal distribution than the original values. The distribution of serum C-reactive protein levels was highly skewed with greater than 50% of the subjects having values below the limit of detection. For correlation analysis, both absolute and log-transformed values of serum ferritin, iron, transferrin saturation, and C-reactive protein were used. The mean (±SE) for the FVC, FEV1, and FEV1/FVC ratio were 3.582±0.029 L, 2.834±0.025 L, and 0.790%±0.002%, respectively. FEV1, FVC, and FEV1/FVC ratio were normally distributed.
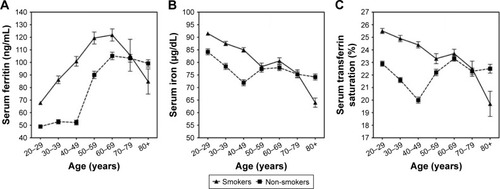
Absolute values of serum ferritin and iron concentrations and transferrin saturation for smokers and non-smokers were plotted against age (). The concentration of serum ferritin increased with age, whereas the concentration of serum iron generally decreased. Relative to non-smokers, serum ferritin concentration was found to be increased among smokers in the age group of 70 years, after which it declined; serum concentrations among non-smokers were significantly higher than that of smokers in the age group of 80 years. Similarly, serum iron concentrations and serum transferrin were elevated among smokers until the age of 50 and 60 years, respectively, at which times, serum concentrations in non-smokers were comparable, although all serum concentrations of iron were higher among non-smokers after the age of 70 years.
Figure 1 Changes in serum ferritin, iron, and transferrin saturation for smokers and non-smokers with age. Serum ferritin increased with age (A), whereas both serum iron (B) and transferrin saturation (C) decreased with age. Serum ferritin was elevated in smokers until 70 years of age, whereas serum iron and serum transferrin were elevated in smokers until 50 and 60 years of age, respectively.
Pearson correlations between age, indices of iron homeostasis, serum C-reactive protein levels, and pulmonary function parameters reveal significant correlations among all in the study population, among smokers and among nonsmokers (–). Age was correlated with all endpoints of iron homeostasis and pulmonary function except ln serum transferrin saturation among non-smokers. Serum ferritin concentrations were positively associated with age, whereas serum iron concentrations and serum transferrin saturation were negatively associated with age. All pulmonary function parameters decreased with age. Serum iron concentrations and transferrin saturation showed stronger positive correlations with both FVC and FEV1 than that of serum ferritin concentrations; the same pattern was evident with FEV1, but the relationship with serum ferritin did not reach significance in non-smokers. In contrast, serum ferritin had the greatest correlation with FEV1/FVC but was negative. Ln serum C reactive protein levels correlated negatively with FVC, FEV1, and FEV1/FVC ratio among smokers and negatively with FVC and FEV1 among non-smokers.
Table 2 Correlations between age, indices of iron homeostasis, and pulmonary function endpoints (n=7,251). Pearson product-moment correlation coefficients and P-values are provided
Table 3 Correlations between age, indices of iron homeostasis, and pulmonary function endpoints for smokers (n=2,549). Pearson product-moment correlation coefficients and P-values are provided
Table 4 Correlations between age, indices of iron homeostasis, and pulmonary function endpoints for non-smokers (n=4,702). Pearson product-moment correlation coefficients and P-values are provided
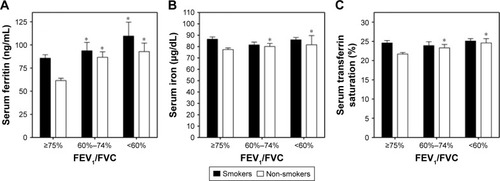
Higher serum ferritin concentrations were observed among smokers with airway obstruction. There were significant differences in serum ferritin concentrations between smokers with airway obstruction with FEV1/FVC ≥75%, FEV1/FVC between 60% and 74%, and those with FEV1/FVC <60% (). The greatest concentrations of this iron-storage protein were among those with the lowest values of FEV1/FVC (<60%). In contrast, there were no significant differences in either serum iron concentration or transferrin saturation among smokers with FEV1/FVC >75%, between 60 and 74%, and <60% (, respectively). However, all three indices of systemic iron homeostasis (ie, serum ferritin, serum iron, and transferrin saturation) showed significant differences among non-smokers with FEV1/FVC ≥75%, between 60 and 74%, and <60% (). Similar to the cigarette smokers, serum ferritin concentrations were greatest among non-smokers with the lowest values of FEV1/FVC (ie, the worst airway obstruction). Elevated concentrations of serum iron in non-smokers were found with decreasing FEV1/FVC. Finally, serum transferrin saturation among non-smokers increased with worsening airway obstruction.
Figure 2 Indices of iron homeostasis change with FEV1/FVC. Serum ferritin (A) significantly increased in both smokers and non-smokers with FEV1/FVC values ranging from 60% to 74% and less than 60%, respectively. However, comparable elevation in serum iron (B) and transferrin saturation (C) among those with FEV1/FVC values from 60% to 74% and less than 60%, respectively, were observed to be significant only in non-smokers. *Significant difference relative to that group (smokers and non-smokers) with FEV1/FVC ≥75%.
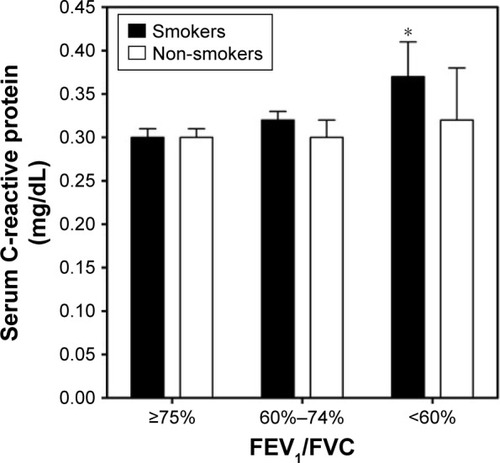
The effect of inflammation on airway obstruction was gauged using serum concentrations of C-reactive protein. Among smokers, those individuals with the greatest airway obstruction (FEV1/FVC <60%) demonstrated a higher level of C-reactive protein than those with FEV1/FVC between 60 and 74% or >75% (). There was no significantly different relationship between C-reactive protein and FEV1/FVC among non-smokers ().
Figure 3 C-reactive protein among smokers and non-smokers with varying FEV1/FVC. C-reactive protein was increased in smokers with the lowest values of FEV1/FVC, but there were no differences among non-smokers with and without obstruction. *Significant difference relative to smokers with FEV1/FVC ≥75%.
Discussion
In an NHANES III cohort, serum indices of iron homeostasis differed by age and were dissimilar between smokers and non-smokers. Serum ferritin concentrations have been repeatedly demonstrated to increase with age comparable to other measures of total body stores of iron;Citation10,Citation11 the exception to this is the first six months of life when iron stores are utilized and depleted by the newborn child.Citation12 Similar to age, race can impact serum ferritin concentrations with individuals of black race consistently have elevated values relative to Caucasians.Citation13 However, the factor which has the greatest impact on serum ferritin concentrations and stores of iron is gender, with males having significantly greater values than females throughout their adult lives.Citation14 This investigation again demonstrated an association between cigarette smoking and serum ferritin with elevated concentrations among current smokers.Citation5 The relationship between serum ferritin and smoking supports the concept that cigarette smoking disrupts iron homeostasis and is associated with metal accumulation. Among smokers, levels of iron increase both systemically and locally in the lung (eg, concentrations in both alveolar macrophages and lavage fluid).Citation15–Citation18 The elevated levels of serum ferritin in smokers reflect increased concentrations of total body iron. In this investigation, serum iron concentrations and transferrin saturation decreased with age but were elevated among smokers until 50 and 60 years of age, respectively.
Results support a negative relationship between FEV1/FVC ratio and serum ferritin among the entire study population, smokers, and non-smokers and between FEV1/FVC and transferrin saturation among the entire population and non-smokers. This is comparable to prior investigation which demonstrated that serum ferritin concentration negatively correlated with the FEV1/FVC ratio reflecting a positive association of the metal storage protein with airway obstruction.Citation19 Studies have also demonstrated that FVC and FEV1 can correlate positively with serum ferritin and iron concentrations and transferrin saturation.Citation20–Citation22 The disruption in iron homeostasis with cigarette smoking can be associated with oxidative stress, and this can initiate pathways resulting in COPD. However, indices of iron homeostasis were also associated with COPD in non-smokers. Etiologies of irreversible airway obstruction in non-smokers can include occupational exposures to particles (eg, miners, tunnel workers, and concrete workers and air pollution).Citation23,Citation24 The basic mechanism of the biological effect of such particles is the same as that of cigarette smoke particles, that is, they also disrupt iron homeostasis resulting in an accumulation of iron with an oxidative stress and injury ensuing.Citation25 Accordingly, it is anticipated that FEV1/FVC ratio will also decrease with particle exposures other than those associated with cigarette smoke and contribute to airway obstruction in non-smokers. FEV1/FVC in non-smokers decreased not only with elevations in serum ferritin but also with increased levels of serum iron and transferrin saturation. This further supports a role of disruption in iron homeostasis among those with obstruction.
Indices of iron homeostasis are thought to be associated with airway obstruction as they reflect total body iron, especially serum ferritin concentrations.Citation26–Citation29 Molecular evolution selected iron to perform a wide range of biological functions, and it is an essential nutrient utilized in almost every aspect of normal cell function. Those same chemical properties which allow iron to serve as a catalyst in reactions of molecular oxygen make it potentially injurious to cells through the generation of oxidative stress. A delicate balance of iron results in every living system with available concentrations being only great enough to meet homeostatic requirements. With elevations in concentrations of available iron following exposures to cigarette smoke and other particles, oxidative stress and injury are possible. The injury can include inflammation. Obstruction is included among the inflammatory responses of the airways to cigarette smoke and other particles.Citation30 Free radical generation catalyzed by increased concentrations of available iron is proposed to be ultimately responsible for tissue injuries such as COPD after exposure to particles.
There are alternative explanations for the relationship between indices of iron homeostasis and FEV1/FVC ratio. Obstructive lung disease can be associated with an acute inflammation and changes in the levels of acute phase reactants, which include serum ferritin and iron concentrations.Citation31–Citation35 Elevation in serum C-reactive protein concentration, reflecting inflammation, is associated with the exacerbation and mortality due to obstructive lung disease.Citation35–Citation37 It can be proposed that the association between serum ferritin concentrations and FEV1/FVC ratio simply reflects the inflammatory response in obstructive lung disease. However, non-smokers with decreased FEV1/FVC ratio demonstrated elevated serum iron concentrations and transferrin saturation which are not consistent with inflammation but can rather reflect increased metal availability.Citation38 This is comparable to previous findings in which there was no relationship between serum C-reactive protein levels and decline in lung function (in a population of individuals 9 years of age and older).Citation39 A second alternative explanation of these results is that both smoking and non-smoking individuals with pre-existing alterations in iron homeostasis may be at increased risk for airway obstruction (ie, the accumulation of metal precedes the obstruction and is independent of it). However, there is no evidence suggesting that such genetic factors could affect obstructive pulmonary disease (eg, airway obstruction is not a prominent feature of hemochromatosis).
The major limitation of this study is the inability to conduct a multivariate regression to determine contributions to FEV1/FVC ratio (including serum iron and ferritin, transferrin saturation, C reactive protein, smoking, race, gender, and age as independent variables). Such a regression is precluded as the variables are not truly independent (eg, serum ferritin increases with smoking, race, gender, and age). In addition, the primacy of the variables and the relationships between the variables determining the order of addition into such a multivariate regression are uncertain (eg, aging is of great significance in determining FEV1/FVC ratio but can possibly reflect the integrated effects of iron accumulation).
Conclusion
We conclude that iron homeostasis is associated with airway obstruction in both smokers and non-smokers with elevation in serum ferritin concentration correlating with lower FEV1/FVC. It is proposed that metal accumulation in cigarette smokers triggers a cascade of biochemical events culminating in inflammatory injury including airway obstruction.Citation40,Citation41 Retention of these particles in lung tissue, with continued iron accumulation, is likely to account for progression of injury and declines in FEV1/FVC despite smoking cessation.Citation42 This same accumulated metal associated with cigarette smoking will increase the risk of other diseases recognized as co-morbidities of obstructive airway disease (eg, coronary artery disease, cerebrovascular disease, peripheral vascular disease, diabetes, neoplasms, and infections).Citation43 Our results are consistent with a documented impact of iron homeostasis on respiratory disease and human mortality.Citation22,Citation44,Citation45 Exposure to particles in non-smokers likely impacts an equivalent metal accumulation to initiate the same pathways of injury. Further investigation into therapies addressing depletion of iron stores may be warranted in the treatment of patients with obstructive lung disease.Citation8,Citation46
Acknowledgments
We thank Edward Hudgens of US Environmental Protection Agency, Office of Research and Development for contract management and Robert Clickner and Rebecca Jeffries of Westat, Rockville Maryland for analytic assistance (contract # 68-D-02-062, WA 3-06).
This report has been reviewed by the National Health and Environmental Effects Research Laboratory, United States Environmental Protection Agency and approved for publication. Approval does not signify that the contents necessarily reflect the views and policies of the Agency nor does mention of trade names or commercial products constitute endorsement or recommendation for use.
Disclosure
The authors report no conflicts of interest in this work.
References
- National Research CouncilEnvironmental Tobacco Smoke: Measuring Exposures and Assessing Health EffectsWashington, DCNational Academy Press1986
- BakerRRSmoke chemistryDavisDLNielsenMTTobacco-Production, Chemistry and Technology, Chapter 12Oxford, UKBlackwell Science2000398439
- FinelliVNPeteringHGEffects of metal-binding fractions of tobacco smoke on in vitro activity of enzymesArch Environ Health1972252971005045069
- GhioAJStonehuernerJQuigleyDRHumic-like substances in cigarette condensate and lung tissue of smokersAm J Physiol19942664 Pt 1L382L3888179015
- GhioAJHilbornEDStonehuernerJGParticulate matter in cigarette smoke alters iron homeostasis to produce a biological effectAm J Respir Crit Care Med2008178111130113818723436
- American Thoracic SocietyLung function testing: selection of reference values and interpretative strategiesAm Rev Respir Dis19911445120212181952453
- KimWJLeeSDCandidate genes for COPD: current evidence and researchInt J Chron Obstruct Pulmon Dis2015102249225526527870
- CloonanSMGlassKLaucho-ContrerasMEMitochondrial iron chelation ameliorates cigarette smoke-induced bronchitis and emphysema in miceNat Med201622216317426752519
- CDCNHANES III (1988–1994) – Reference Manuals and Report Available from: https://www.cdc.gov/nchs/nhanes/nh3rrm.htmAccessed May 5, 2015
- LoríaAHershkoCKonijnAMSerum ferritin in an elderly populationJ Gerontol1979344521524448043
- LeggettBABrownNNBryantSJDuplockLPowellLWHallidayJWFactors affecting the concentrations of ferritin in serum in a healthy Australian populationClin Chem1990367135013552372951
- KeenCLHurleyLSDevelopmental changes in concentrations of iron, copper, and zinc in mouse tissuesMech Ageing Dev19801321611767432004
- PanYJacksonRTInsights into the ethnic differences in serum ferritin between black and white US adult menAm J Hum Biol200820440641618348278
- ValbergLSSorbieJLudwigJPelletierOSerum ferritin and the iron status of CanadiansCan Med Assoc J197611454174211253085
- QuanSGGoldeDWIdentification and localization of toxic elements in normal human lung macrophagesProc Soc Exp Biol Med198116721751817232423
- ThompsonABBohlingTHeiresALinderJRennardSILower respiratory tract iron burden is increased in association with cigarette smokingJ Lab Clin Med199111764934992045717
- McGowanSEMurrayJJParrishMGIron binding, internalization, and fate in human alveolar macrophagesJ Lab Clin Med198610865875953783029
- McGowanSEHenleySAIron and ferritin contents and distribution in human alveolar macrophagesJ Lab Clin Med198811166116173373107
- LeeCHGoagEKLeeSHAssociation of serum ferritin levels with smoking and lung function in the Korean adult population: analysis of the fourth and fifth Korean National Health and Nutrition Examination SurveyInt J Chron Obstruct Pulmon Dis2016113001300627942209
- ShibataYInoueSIgarashiAElevated serum iron is a potent biomarker for spirometric resistance to cigarette smoke among Japanese males: the Takahata studyPLoS One201389e7402024040149
- McKeeverTMLewisSASmitHABurneyPCassanoPABrittonJA multivariate analysis of serum nutrient levels and lung functionRespir Res200896718823528
- BrighamEPMcCormackMCTakemotoCMMatsuiECIron status is associated with asthma and lung function in US womenPLoS One2015102e011754525689633
- BalmesJBecklakeMBlancPEnvironmental and Occupational Health Assembly, American Thoracic SocietyAmerican Thoracic Society Statement: occupational contribution to the burden of airway diseaseAm J Respir Crit Care Med2003167578779712598220
- AssadNABalmesJMehtaSCheemaUSoodAChronic obstructive pulmonary disease secondary to household air pollutionSemin Respir Crit Care Med201536340842126024348
- GhioAJSoukupJMDaileyLAAir pollution particles and iron homeostasisBiochim Biophys Acta20161860122816282527217087
- CookJDClinical evaluation of iron deficiencySemin Hematol19821916186763340
- CookJDSkikneBSIron deficiency: definition and diagnosisJ Intern Med198922653493552681511
- BeutlerEFelittiVHoNJGelbartTRelationship of body iron stores to levels of serum ferritin, serum iron, unsaturated iron binding capacity and transferrin saturation in patients with iron storage diseaseActa Haematol2002107314514911978935
- MeiZCogswellMEParvantaIHemoglobin and ferritin are currently the most efficient indicators of population response to iron interventions: an analysis of nine randomized controlled trialsJ Nutr200513581974198016046725
- BrüskeIThieringEHeinrichJHusterKMNowakDRespirable quartz dust exposure and airway obstruction: a systematic review and meta-analysisOccup Environ Med201471858358924863263
- BaynesRBezwodaWBothwellTKhanQMansoorNThe non-immune inflammatory response: serial changes in plasma iron, iron-binding capacity, lactoferrin, ferritin and C-reactive proteinScand J Clin Lab Invest19864676957043787168
- BeardJLMurray-KolbLERosalesFJSolomonsNWAngelilliMLInterpretation of serum ferritin concentrations as indicators of total-body iron stores in survey populations: the role of biomarkers for the acute phase responseAm J Clin Nutr20068461498150517158435
- SheikhNDudasJRamadoriGChanges of gene expression of iron regulatory proteins during turpentine oil-induced acute-phase response in the ratLab Invest200787771372517417667
- BroekhuizenRWoutersEFCreutzbergECScholsAMRaised CRP levels mark metabolic and functional impairment in advanced COPDThorax2006611172216055618
- TkacovaRKluchovaZJoppaPPetrasovaDMolcanyiovaASystemic inflammation and systemic oxidative stress in patients with acute exacerbations of COPDRespir Med200710181670167617449234
- SinDDManSFSystemic inflammation and mortality in chronic obstructive pulmonary diseaseCan J Physiol Pharmacol200785114114717487253
- KaradagFKirdarSKarulABCeylanEThe value of C-reactive protein as a marker of systemic inflammation in stable chronic obstructive pulmonary diseaseEur J Intern Med200819210410818249305
- ShenkinATrace elements and inflammatory response: implications for nutritional supportNutrition199511Suppl 11001057749254
- FogartyAWJonesSBrittonJRLewisSAMcKeeverTMSystemic inflammation and decline in lung function in a general population: a prospective studyThorax200762651552017251312
- RahmanIMacNeeWRole of oxidants/antioxidants in smoking-induced lung diseasesFree Radic Biol Med19962156696818891669
- PryorWACigarette smoke radicals and the role of free radicals in chemical carcinogenicityEnviron Health Perspect1997105Suppl 48758829255574
- RutgersSRPostmaDSten HackenNHOngoing airway inflammation in patients with COPD who do not currently smokeThorax2000551121810607796
- FordESCogswellMEDiabetes and serum ferritin concentration among U.S. adultsDiabetes Care199922121978198310587829
- KimKSSonHGHongNSLeeDHAssociations of serum ferritin and transferrin % saturation with all-cause, cancer, and cardiovascular disease mortality: Third National Health and Nutrition Examination Survey follow-up studyJ Prev Med Public Health201245319620322712047
- MenkeAMuntnerPFernández-RealJMGuallarEThe association of biomarkers of iron status with mortality in US adultsNutr Metab Cardiovasc Dis201222973474021330119
- MartinezJAGuerraCCNeryLEJardimJRIron stores and coagulation parameters in patients with hypoxemic polycythemia secondary to chronic obstructive pulmonary disease: the effect of phlebotomiesSao Paulo Med J199711512139514029460300