
Abstract
Introduction
A low body mass index (BMI) is associated with increased mortality and low health-related quality of life in patients with COPD. The Asia-Pacific classification of BMI has a lower cutoff for overweight and obese categories compared to the World Health Organization (WHO) classification. The present study assessed patients with COPD among different BMI categories according to two BMI classification systems: WHO and Asia-Pacific.
Patients and methods
Patients with COPD aged 40 years or older from the Korean COPD Subtype Study cohort were selected for evaluation. We enrolled 1,462 patients. Medical history including age, sex, St George’s Respiratory Questionnaire (SGRQ-C), the modified Medical Research Council (mMRC) dyspnea scale, and post-bronchodilator forced expiratory volume in 1 second (FEV1) were evaluated. Patients were categorized into different BMI groups according to the two BMI classification systems.
Result
FEV1 and the diffusing capacity of the lung for carbon monoxide (DLCO) percentage revealed an inverse “U”-shaped pattern as the BMI groups changed from underweight to obese when WHO cutoffs were applied. When Asia-Pacific cutoffs were applied, FEV1 and DLCO (%) exhibited a linearly ascending relationship as the BMI increased, and the percentage of patients in the overweight and obese groups linearly decreased with increasing severity of the Global Initiative for Chronic Obstructive Lung Disease criteria. From the underweight to the overweight groups, SGRQ-C and mMRC had a decreasing relationship in both the WHO and Asia-Pacific classifications. The prevalence of comorbidities in the different BMI groups showed similar trends in both BMI classifications systems.
Conclusion
The present study demonstrated that patients with COPD who have a high BMI have better pulmonary function and health-related quality of life and reduced dyspnea symptoms. Furthermore, the Asia-Pacific BMI classification more appropriately reflects the correlation of obesity and disease manifestation in Asian COPD patients than the WHO classification.
Keywords:
Introduction
COPD is a slowly progressive disorder characterized by partially reversible chronic airway obstruction.Citation1,Citation2 Besides its lung manifestation, COPD has been considered to be a systemic disease in recent years due to its significant extrapulmonary findings.Citation3 The body mass index (BMI), which can indirectly represent the degree of obesity, is one of the variables that affects the phenotypic expression of the disease, its course, and prognosis.Citation3–Citation9 Use of the BMI is recommended by the National Heart Lung and Blood Institute (NHLBI)Citation10 and it has been shown to contribute toward the expression of COPD phenotypes.Citation11,Citation12 BMI is included in the Body-Mass Index, Airflow Obstruction, Dyspnea, and Exercise (BODE) index, which predicts the prognosis of patients with COPD.Citation3 A low BMI is associated with increased mortality in patients with COPDCitation3,Citation10,Citation13 through its influences on pulmonary mechanics,Citation14 diaphragmatic muscle weakness,Citation15 decreased lung function,Citation16 as well as systemic inflammation and its biomarkers.Citation17,Citation18 Furthermore, a low body weight is associated with low health-related quality of life.Citation19–Citation21
With the increasing prevalence of obesity in Asia, BMI as a disease predictor has increased in importance. However, there has been controversy when applying international criteria for obesity to an Asian population, and there have been attempts to reinterpret the BMI cutoffs for Asian and Pacific populations.Citation22,Citation23 The World Health Organization (WHO) expert consultation identified further potential public health action points (23.0, 27.5, 32.5, and 37.5 kg/m2).Citation24 In Asia-Pacific countries including Korea, the agreed cutoff for inclusion in the overweight category is 23.0 kg/m2.Citation25 Asian populations have a higher risk of developing comorbidities such as cardiovascular disease and type 2 diabetes at BMIs lower than 25 kg/m2, which is the WHO cutoff point for overweight and, in addition, association between BMI and body fat percentage is different from that for Europeans.Citation24 The prevalence of metabolically obese but normal-weight patients in Korea is almost twice that found in the United States (US) populationCitation26 and, compared to the non-Asian population, their muscle mass is smaller.
Very few studies have evaluated the correlation between BMI and the disease severity of patients with COPD according to the degree of obesity in Asians. We hypothesized that patients with COPD in different BMI groups would exhibit different manifestations of COPD and proportions of comorbidities. In addition, applying two BMI classifications and comparing the related clinical variables can be clinically significant and, to our knowledge, no study comparing two BMI classification systems has been reported.
Our study compared the clinical characteristics, disease severity, and COPD-related comorbidities of Korean patients with COPD in different BMI categories based on both the WHO and Asia-Pacific BMI classifications.
Patients and methods
Study participants
Patients registered in the Korean COPD Subtype Study (KOCOSS) were recruited from 48 tertiary referral hospitals in Korea and were required to visit the hospital to update their COPD status by self-administered questionnaires at least every 6 months.Citation27 The inclusion criteria were as follows: age ≥40 years and post-bronchodilator forced expiratory volume in 1 second (FEV1)/forced vital capacity (FVC) <0.7. The medical history taken from patient questionnaires as well as measurements from their initial visit were used as baseline data. Age, sex, St George’s Respiratory Questionnaire (SGRQ-C) response, and the modified Medical Research Council (mMRC) dyspnea scale score of patients were recorded. Post-bronchodilator FEV1, FVC, and FEV1/FVC were checked by pulmonary function tests. Six-minute walk tests (6MWT) were also performed at the time of enrollment.
BMI and categorization
According to the NHLBI,Citation10 BMI is calculated as weight in kilograms divided by the square of the height in meters (kg/m2) and is categorized into four groups according to the Asian-Pacific cutoff points ():Citation25 underweight (<18.5 kg/m2), normal weight (18.5–22.9 kg/m2), overweight (23–24.9 kg/m2), and obese (≥25 kg/m2). For comparison, BMI was also categorized into four groups according to the conventional WHO classification:Citation10 underweight (<18.5 kg/m2), normal weight (18.5–24.9 kg/m2), overweight (25–29.9 kg/m2), and obese (≥30 kg/m2).
Table 1 Obesity classification according to WHO and Asia-Pacific guidelines
Ethnic backgrounds
Among Korean nationals, 96% are of Korean origin and most immigrants have an Asian background (People’s Republic of China, Vietnam, Japan, etc).Citation28 All patients in this cohort were citizens of the Republic of Korea.
Comorbidities
At the time of enrollment to the cohort, patient comorbidities were checked. History of myocardial infarction, heart failure, peripheral vessel disease, diabetes mellitus, hypertension, osteoporosis, gastroesophageal reflux disease, dyslipidemia, thyroid disorder, inflammatory bowel disease, bronchiectasis, previously diagnosed COPD, measles, pertussis, pneumonia, asthma, allergic rhinitis, and atopic dermatitis were carefully evaluated.
Ethics statement
For KOCOSS patients, written informed consent was obtained from all study participants. Ethics approval for the KOCOSS cohort was obtained from the ethics committee at each center. We also received approval from each center to use clinical records of their subjects for the study while maintaining patient confidentiality with regard to the data. The official name of each approving ethics committee is listed in the Supplementary materials.
Statistical analysis
Continuous variables are reported as mean ± standard deviation. When comparing clinical parameters between BMI groups, an analysis of variance (ANOVA) test was performed for continuous variables, while the chi-squared test was performed for categorical variables. Pearson’s coefficient comparison was used to determine linear associations between numerical variables. Statistical significance was established at a P-value <0.05. The Mantel–Haenszel chi-squared test was performed to determine the association between categorical variables.
Results
Clinical characteristics
lists the baseline characteristics of the study participants. The study included 1,462 subjects, and the number of male patients was 1,396 (90.8%). The mean patient age was 70.5±7.8 years. The predicted mean post-bronchodilator FEV1 percentage was 55.6%±18.3%. The mean FVC was 80.5±17.5 and FEV1/FVC was 48.8±12.3. The mean BMI was 22.8±3.4 kg/m2. The Global Initiative for Chronic Obstructive Lung Disease (GOLD) stage II was seen in the greatest proportion of this COPD cohort, with 758 (52.0%) patients falling into this category. The mean SGRQ-C was 34.6±19.0 and the mean COPD assessment test score was 15.8±7.8. The mean mMRC score was 1.5±0.9.
Table 2 Baseline characteristics of COPD patients (n=1,462)
Distribution of BMI
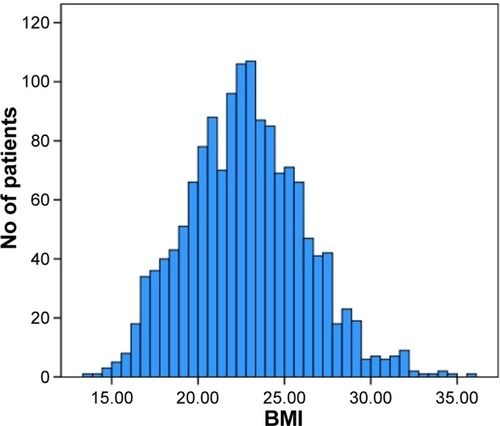
and present the distribution of BMI values among study subjects. The mean BMI value was 22.8 [95% confidence interval (CI) 22.6–23.0] and the median value was 22.7. The lowest BMI value was 13.50, whereas the highest was 35.99 (). shows the distribution of BMI values among the entire study population.
Figure 1 Distribution of the body mass index of the study patients.
Abbreviation: BMI, body mass index.
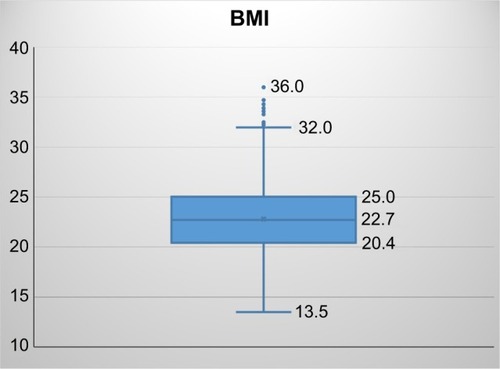
Figure 2 Bar graphs showing the distribution of the body mass index of the study patients.
Correlation of major variables with different BMI categories
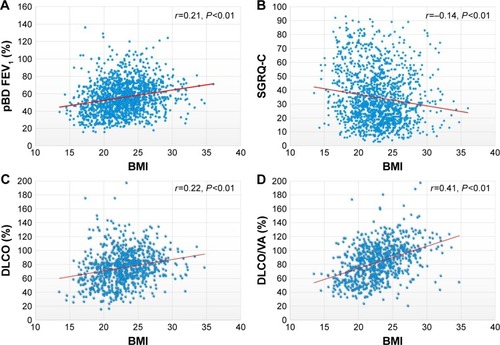
The SGRQ-C was found to be in a linearly decreasing relationship with BMI (Pearson coefficient of correlation r=−0.14, P<0.01). However, the post-bronchodilator FEV1 was in a linearly increasing relationship with BMI (r=0.21, P<0.01). The diffusing capacity of the lung for carbon monoxide (DLCO) percentage and DLCO/alveolar volume (VA) were also in a linearly increasing relationship with BMI (r=0.22, P<0.01 and r=0.41, P<0.01, respectively; ).
Figure 3 Correlation of the body mass index to (A) pBD FEV1 (%), (B) SGRQ-C, (C) DLCO (%), and (D) DLCO/VA (%).
Abbreviations: pBD, post-bronchodilator; FEV1, forced expiratory volume in 1 second; SGRQ-C, St George’s Respiratory Questionnaire; DLCO, diffusing capacity of the lung for carbon monoxide; VA, alveolar volume; BMI, body mass index.
Furthermore, we evaluated differences in the values of major variables when the BMI groups changed (). Changes in variables were also evaluated according to each classification system (WHO and Asia-Pacific). No significant change in the mean age was observed in either classification. A comparison of the normal weight group to the overweight group revealed that the proportion of male patients decreased gradually. Between the underweight and normal weight groups, SGRQ-C and mMRC scores were in a decreasing relationship in both the WHO and Asia-Pacific classifications. However, the two variables increased from the overweight to the obese group.
Table 3 Comparison of clinical variables of by BMI categories according to two cutoff systems
When the WHO cutoffs were applied, an inverse “U”-shaped pattern was observed for FEV1. When the Asia-Pacific cutoffs were applied, FEV1 was in a linearly ascending relationship, whereas DLCO (%) was in a linearly increasing relationship with BMI when the Asia-Pacific cutoffs were applied. However, DLCO (%) had an inverse “U”-shaped pattern when the WHO cutoffs were applied ().
FEV1 (%) and BMI categories
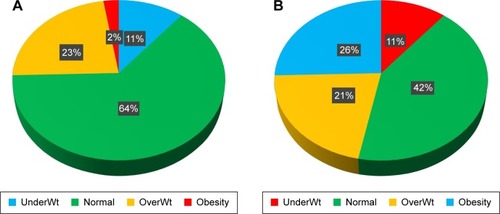
We compared the mean BMI of the groups of patients classified according to the GOLD criteria () and found that mean BMI decreases as the severity of airway obstruction increases. Mean BMI was 23.6 kg/m2 in the GOLD 1 group and 21.2 kg/m2 in the GOLD 4 group. shows the proportion of each BMI group. shows the proportion of each BMI group according to the WHO cutoffs, and shows proportions according to the Asia-Pacific cutoffs. When WHO cutoffs were applied, 2.4% of the patients fell into the obese category, while 25.5% of the patients were found to be obese according to the Asia-Pacific cutoffs.
Figure 4 Body mass index according to GOLD stage.
Abbreviations: BMI, body mass index; GOLD, Global Initiative for Chronic Obstructive Lung Disease.
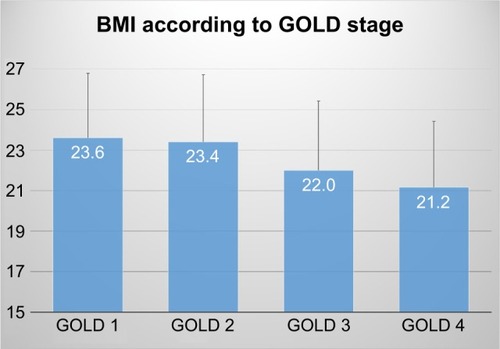
Figure 5 Pie charts showing the proportion of patients in each body mass index group according to (A) the World Health Organization (WHO) classification and (B) the Asia-Pacific classification.
Abbreviation: Wt, weight.
shows the proportion of each BMI group according to the GOLD criteria. As the severity of the GOLD criteria increases, proportions of the different BMI categories by both WHO and Asia-Pacific cutoffs change with statistical significance (P-value <0.001). However, when WHO cutoffs were applied, the percentage of the obese group decreased after an initial increase. Conversely, when the Asia-Pacific cutoffs were applied, the percentage in the obese group linearly decreased as the GOLD criteria increased in severity. The percentage in the underweight patient group increased from 5.5% to 21.4% as the GOLD criteria changed from 1 to 4 for both BMI classifications.
Table 4 Comparison of proportions of airway disease severity in two different body mass classifications
Comorbidities
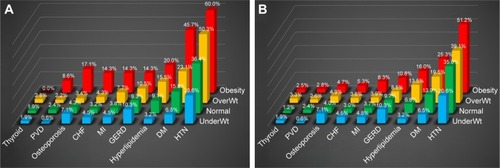
Comorbidities were observed in different percentages in different BMI categories. presents the comorbidities of patients in different BMI groups classified according to the WHO cutoffs, while presents those in BMI groups according to the Asia-Pacific cutoffs. Both graphs show that the percentage of patients with hypertension, diabetes, and hyperlipidemia increased as the groups became more obese. The percentage of patients with congestive heart failure, myocardial infarction, and peripheral vascular disease was also highest in the obese groups. Osteoporosis had the highest proportion of patients in the obese group when the WHO classification was applied and also had the highest proportion of patients in the underweight group when the Asia-Pacific classification was applied ().
Figure 6 Prevalence of comorbidities in different body mass index groups according to (A) the World Health Organization (WHO) classification and (B) the Asia-Pacific classification.
Discussion
The present COPD cohort study evaluated COPD manifestation and comorbidity in different BMI categories. First, FEV1 worsened as the BMI groups changed from obese to underweight. Second, the quality of life and dyspnea score improved as the BMI groups changed from underweight to overweight. Third, comorbidities were observed in different proportions according to the BMI group. Two BMI classifications were used to assess the clinical correlation between clinical parameters and BMI, and several differences were observed.
These results reveal that a low BMI is associated with worse health-related quality of life in patients with COPD, and this result is consistent with those of previous studies.Citation19–Citation21,Citation29 The study by Divo et al shows that the dyspnea score and SGRQ-C showed a “U” shape as the BMI category changed from underweight to obese.Citation30 In the present study, SGRQ-C and mMRC scores were lowest for the overweight group and increased in the obese group, similar to the result from a previous study.Citation30 We speculate that SGRQ-C and mMRC were worse for obese patients compared to overweight patients, due to the influence of obesity on the activities of patients with COPD. An increase in fat mass is likely to be associated with functional limitation.Citation31 Metabolic comorbidity associated with obesity may also be a contributing factor to the relative worsening of quality of life of these patients.
Post-bronchodilator FEV1 decreased as the patients’ BMI decreased. Previous studies have reported that BMI is correlated with the severity of emphysema, with low-BMI COPD patients more likely to have this condition;Citation30,Citation32,Citation33 such findings can provide an explanation for the linear decrease of FEV1 in the low-BMI group. In addition to previously reported results, the DLCO percentage gradually increased as patients were classified into groups of increasing obesity. Such a correlation between DLCO and obesity is controversial. Some studies have reported increased DLCO in more obese patients,Citation30,Citation34–Citation36 while other studies have observed unchanged or reduced DLCO in obese patients.Citation37–Citation39 Nevertheless, a linear decrease of DLCO in lower BMI groups should be interpreted as a correlation between emphysema and low body mass, as previous studies showing a correlation between DLCO and emphysema suggest.Citation40,Citation41 Clinical relationships of FEV1 and DLCO to BMI also support the previously mentioned “obesity paradox” in which patients with COPD with higher BMI have better prognosis compared to low BMI groups.Citation42,Citation43
In this study, the WHO and Asia-Pacific BMI classifications were simultaneously applied to assess patients with COPD, and major clinical variables were evaluated for each classification system. To our knowledge, no study comparing two BMI classifications in Asian patients with COPD has previously been reported. Both BMI classification systems revealed similar changes in major variables as the patients became more obese (). However, when the Asia-Pacific cutoffs were applied, changes in the SGRQ-C and mMRC scores were more constant as the patients fell into the more obese groups. The change in FEV1% was more gradual compared to when the WHO cutoffs were applied.
Furthermore, when the WHO classification was applied, the proportion of obese patients was too low (2.5%) to allow a comparison with less obese patients. The proportions of obese patients were 29.6% according to the studies on the distribution of BMI among patients with COPD in both SpainCitation44 as well as the Middle East and North Africa.Citation45 The study by Rodríguez et al showed that the proportion of the obese was 43% among the selected patients with COPD.Citation46 In addition, when evaluating the clinical parameters associated with BMI, such as health-related quality of life, dyspnea score, and respiratory functions, Asia-Pacific classifications can be more appropriate than WHO classifications in Asian patients with COPD.
We assume that the Asia-Pacific BMI classification is more appropriate for Asian patients for the following reasons. A previous study suggested that weight loss in patients with COPD is due to a loss of skeletal muscle volume; on the other hand, a change in fat mass is not a significant contributor.Citation47 Furthermore, the fat-free mass index (FFMI) is reported to be more significant than fat mass in the assessment of quality of life and respiratory function of patients with COPD.Citation48,Citation49 According to the evaluation of Korea National Health and Nutrition Examination Survey (KNHANES), mean BMI and appendicular skeletal muscle (ASM) of Koreans were 24.0±0.0 kg/m2 and 22.6±0.1 kg in men and 23.2±0.1 kg/m2 and 14.5±0.0 kg in women, respectively.Citation50,Citation51 In contrast, average BMI and ASM from the US population sample from the National Health and Nutrition Examination Survey (NHANES) were 27.9±0.10 kg/m2 and 26.5±0.1 kg in men and 28.2±0.14 in women and 17.8±0.1 kg, respectively.Citation52,Citation53 Because the Asia-Pacific grading of obesity is based on a consensus that the skeletal and muscle mass of patients in the Asia-Pacific region is lower than that in the West,Citation25 we might, therefore, expect a better correlation between BMI according to the Asia-Pacific guidelines than with the WHO grading in Asian patients with COPD.
Metabolic and cardiac problems were more frequent in the obese groups, and such a finding is consistent with the previous study on patients with COPDCitation30 and distribution of comorbidities among the general population.Citation54,Citation55 The prevalence of metabolic disease and cardiovascular disease were much higher when the WHO classification was applied as compared to when the Asia-Pacific classification was applied. The proportion of patients with major comorbidities may differ according to the two different BMI classifications, but the patterns of increase or decrease according to the BMI of the patients with COPD were similar. Moreover, due to the extremely small number of patients falling into the obese category when the WHO cutoffs were applied, some comorbidities such as osteoporosis had an inappropriately high prevalence.
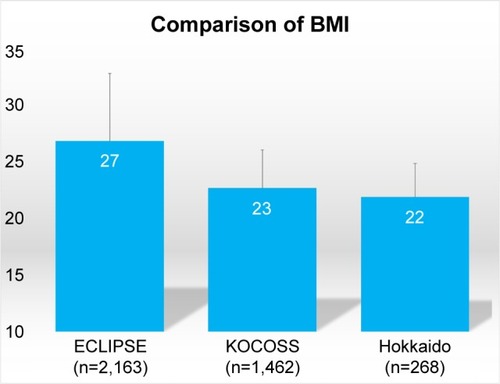
It is widely known that Asian and Western populations differ in mean body mass. However, few studies have compared BMI between Western and Asian patients with COPD. No statistical analysis was conducted for comparison with the other cohorts due to lack of raw data; however, the present study indirectly compared mean BMI of Korean patients with COPD to both Japanese and Western patients with COPD. Interestingly, compared with other major COPD cohorts, the mean BMI of the KOCOSS cohort was much lower than that in the Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints (ECLIPSE; 27±6 kg/m2);Citation56 such a finding can be explained by the difference in body mass between Western and Asian populations. As expected, the Hokkaido cohort’s mean BMI (22±3 kg/m2)Citation57,Citation58 was similar to that for the KOCOSS patients (23±3 kg/m2; ).
Figure 7 Comparison of the mean body mass index of the study patients with the ECLIPSE and Hokkaido cohorts.
Abbreviations: BMI, body mass index; ECLIPSE, Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints; KOCOSS, Korean COPD Subtype Study.
Our study has a few limitations. First, due to the relatively short duration of the observation period of our recently constructed cohort, the mortality of the study patients could not be evaluated. Second, the body composition data, comprising fat and skeletal muscle mass and quadriceps muscle strength, of patients were not measured. Due to lack of body composition data, evaluation of the association of clinical parameters such as lung function and symptom score to FFMM was limited. We planned to include body composition data for the future study. However, we performed the 6 MWT to evaluate the functional capacity of these patients.
Conclusion
The present study revealed that patients with COPD with a high BMI had better pulmonary function and health-related quality of life and fewer dyspnea symptoms. Furthermore, the results suggest that the Asia-Pacific BMI classification is more appropriate in reflecting the correlation between obesity and the manifestation of COPD in Asian patients compared to that with the WHO classification system. Further studies regarding the clinical significance of BMI classification in Asian patients with COPD are needed.
Acknowledgments
The English in this document has been checked by at least two professional editors, both native speakers of English.
Supplementary materials
The names of ethics committees are as follows: Gacheon University Gil Medical Center, Hallym University Kangnam Sacred Heart Hospital, Gangnam Severance Hospital, Kyung Hee University Hospital at Gangdong, Hallym University Kangdong Sacred Heart Hospital, Kangbuk Samsung Hospital, Kangwon National University Hospital, Konkuk University Hospital, Konkuk University Chungju Hospital, Kyungpook National University Hospital, Gyeongsang National University Hospital, Korea University Guro Hospital, Korea University Anam Hospital, Seoul Eulji Hospital, Dongguk University Gyeongju Hospital, Dongguk University Ilsan Hospital, Keimyung University Dongsan Medical Center, Dong-A University Hospital, Hallym University Dongtan Sacred Heart Hospital, Pusan National University Hospital, Inje University Busan Paik Hospital, The Catholic University of Korea Bucheon St Mary’s Hospital, Soonchunhyang University Hospital Bucheon, Seoul National University Bundang Hospital, Bundang CHA Hospital, Seoul Metropolitan Government Seoul National University Bora-mae Medical Center, Samsung Medical Center, Soonchunhyang University Hospital Seoul, The Catholic University of Korea Seoul St Mary’s Hospital, The Catholic University of Korea St Paul’s Hospital, The Catholic University of Korea St Vincent’s Hospital, Severance Hospital, Asan Medical Center, Ajou University Hospital, The Catholic University of Korea Yeouido St Mary’s Hospital, The Catholic University of Korea Uijeongbu St Mary’s Hospital, Yeungnam University Medical Center, Ulsan University Hospital, Wonkwang University Sanbon Hospital, Wonju Severance Christian Hospital, Ewha Womans University Mokding Hospital, Incheon St Mary’s Hospital, Inha University Hospital, Chonnam National University Hospital, Chonbuk National University Hospital, Jeju National University Hospital, Soonchunhyang University Hospital Cheonan, Hallym University Chuncheon Sacred Heart Hospital, Hallym University Sacred Heart Hospital, and Hanyang University Guri Hospital.
We also received approval from each center to use their subjects’ clinical records for the study while maintaining the confidentiality of the data.
Disclosure
The authors report no conflicts of interest in this work.
References
- PauwelsRABuistASCalverleyPMJenkinsCRHurdSSGOLD Scientific CommitteeGlobal strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. NHLBI/WHO Global Initiative for Chronic Obstructive Lung Disease (GOLD) Workshop summaryAm J Respir Crit Care Med200116351256127611316667
- CelliBRMacNeeWATS/ERS Task ForceStandards for the diagnosis and treatment of patients with COPD: a summary of the ATS/ERS position paperEur Respir J200423693294615219010
- CelliBRCoteCGMarinJMThe body-mass index, airflow obstruction, dyspnea, and exercise capacity index in chronic obstructive pulmonary diseaseN Engl J Med2004350101005101214999112
- CasanovaCAguirre-JaímeAde TorresJPLongitudinal assessment in COPD patients: multidimensional variability and outcomesEur Respir J201443374575324072210
- MarinJMAlfagemeIAlmagroPMulticomponent indices to predict survival in COPD: the COCOMICS studyEur Respir J201342232333223222874
- VestboJHurdSSAgustíAGGlobal strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summaryAm J Respir Crit Care Med2013187434736522878278
- PischonTBoeingHHoffmannKGeneral and abdominal adiposity and risk of death in EuropeN Engl J Med2008359202105212019005195
- CastaldiPJDyJRossJCluster analysis in the COPD Gene study identifies subtypes of smokers with distinct patterns of airway disease and emphysemaThorax201469541542224563194
- RennardSILocantoreNDelafontBIdentification of five chronic obstructive pulmonary disease subgroups with different prognoses in the ECLIPSE cohort using cluster analysisAnn Am Thorac Soc201512330331225642832
- Executive summary of the clinical guidelines on the identification, evaluation, and treatment of overweight and obesity in adultsArch Intern Med199815817185518679759681
- Garcia-AymerichJGómezFPBenetMPAC-COPD Study GroupIdentification and prospective validation of clinically relevant chronic obstructive pulmonary disease (COPD) subtypesThorax201166543043721177668
- BurgelPRPaillasseurJLCaillaudDInitiatives BPCO Scientific CommitteeClinical COPD phenotypes: a novel approach using principal component and cluster analysesEur Respir J201036353153920075045
- CaoCWangRWangJBunjhooHXuYXiongWBody mass index and mortality in chronic obstructive pulmonary disease: a meta-analysisPLoS One201278e4389222937118
- FranssenFMO’DonnellDEGoossensGHBlaakEEScholsAMObesity and the lung: 5. Obesity and COPDThorax200863121110111719020276
- VestboJPrescottEAlmdalTBody mass, fat-free body mass, and prognosis in patients with chronic obstructive pulmonary disease from a random population sample: findings from the Copenhagen City Heart StudyAm J Respir Crit Care Med20061731798316368793
- CoxsonHOChanIHMayoJRHlynskyJNakanoYBirminghamCLEarly emphysema in patients with anorexia nervosaAm J Respir Crit Care Med2004170774875215256394
- AgustiAEdwardsLDRennardSIEvaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints (ECLIPSE) InvestigatorsPersistent systemic inflammation is associated with poor clinical outcomes in COPD: a novel phenotypePLoS One201275e3748322624038
- TomodaKYoshikawaMItohTElevated circulating plasma adiponectin in underweight patients with COPDChest2007132113514017625082
- HesselinkAEvan der WindtDAPenninxBWWhat predicts change in pulmonary function and quality of life in asthma or COPD?J Asthma200643751351916939991
- ShoupRDalskyGWarnerSBody composition and health-related quality of life in patients with obstructive airways diseaseEur Respir J1997107157615809230250
- KatsuraHYamadaKKidaKBoth generic and disease specific health-related quality of life are deteriorated in patients with underweight COPDRespir Med200599562463015823461
- WHO/IASO/IOTFThe Asia-Pacific perspective: redefining obesity and its treatmentHealth Communications AustraliaMelbourne2000
- JamesWPChunmingCInoueSAppropriate Asian body mass indices?Obes Rev20023313912164464
- WHO Expert ConsultationAppropriate body-mass index for Asian populations and its implications for policy and intervention strategiesLancet2004363940315716314726171
- PanWHYehWTHow to define obesity? Evidence-based multiple action points for public awareness, screening, and treatment: an extension of Asian-Pacific recommendationsAsia Pac J Clin Nutr200817337037418818155
- LeeKMetabolically obese but normal weight (MONW) and metabolically healthy but obese (MHO) phenotypes in Koreans: characteristics and health behaviorsAsia Pac J Clin Nutr200918228028419713189
- LeeJYChonGRRheeCKCharacteristics of patients with chronic obstructive pulmonary disease at the first visit to a pulmonary medical center in Korea: The KOrea COpd Subgroup Study Team CohortJ Korean Med Sci201631455356027051239
- Kostat.go.krDaejeon: Statistics Korea [updated 2016 Aug 04; cited 2017 Jun 12]. Available from: http://kostat.go.kr/portal/korea/index.action/Accessed Jun 12, 2017
- TsiligianniIKocksJTzanakisNSiafakasNvan der MolenTFactors that influence disease-specific quality of life or health status in patients with COPD: a review and meta-analysis of Pearson correlationsPrim Care Respir J201120325726821472192
- DivoMJCabreraCCasanovaCComorbidity distribution, clinical expression and survival in COPD patients with different body mass indexJ COPD F201412229238
- EisnerMDBlancPDSidneySBody composition and functional limitation in COPDRespir Res20078717261190
- RenvallMJFriedmanPRamsdellJWPredictors of body mass index in patients with moderate to severe emphysemaCOPD20096643243619938965
- OgawaENakanoYOharaTBody mass index in male patients with COPD: correlation with low attenuation areas on CTThorax2009641202518852156
- CollardPWilputteJYAubertGRodensteinDOFransAThe single-breath diffusing capacity for carbon monoxide in obstructive sleep apnea and obesityChest19961105118911938915219
- SaydainGBeckKCDeckerPACowlCTScanlonPDClinical significance of elevated diffusing capacityChest2004125244645214769723
- RayCSSueDYBrayGHansenJEWassermanKEffects of obesity on respiratory functionAm Rev Respir Dis198312835015066614644
- BiringMSLewisMILiuJTMohsenifarZPulmonary physiologic changes of morbid obesityAm J Med Sci1999318529329710555090
- HakalaKStenius-AarnialaBSovijärviAEffects of weight loss on peak flow variability, airways obstruction, and lung volumes in obese patients with asthmaChest200011851315132111083680
- RavipatiGAronowWSSidanaJAssociation of reduced carbon monoxide diffusing capacity with moderate or severe left ventricular diastolic dysfunction in obese personsChest200512831620162216162766
- HolmeJStockleyRARadiologic and clinical features of COPD patients with discordant pulmonary physiology: lessons from alpha1-antitrypsin deficiencyChest2007132390991517573491
- van der LeeIGietemaHAZanenPNitric oxide diffusing capacity versus spirometry in the early diagnosis of emphysema in smokersRespir Med2009103121892189719586765
- JeeSHSullJWParkJBody-mass index and mortality in Korean men and womenN Engl J Med2006355877978716926276
- LandboCPrescottELangePVestboJAlmdalTPPrognostic value of nutritional status in chronic obstructive pulmonary diseaseAm J Respir Crit Care Med199916061856186110588597
- García-RioFSorianoJBMiravitllesMImpact of obesity on the clinical profile of a population-based sample with chronic obstructive pulmonary diseasePLoS One201498e10522025153331
- KoniskiMLSalhiHLahlouARashidNEl HasnaouiADistribution of body mass index among subjects with COPD in the Middle East and North Africa region: data from the BREATHE studyInt J Chron Obstruct Pulmon Dis2015101685169426346564
- RodríguezDAGarcia-AymerichJValeraJLDeterminants of exercise capacity in obese and non-obese COPD patientsRespir Med2014108574575124565602
- IschakiEPapatheodorouGGakiEPapaIKoulourisNLoukidesSBody mass and fat-free mass indices in COPD: relation with variables expressing disease severityChest2007132116416917505043
- PlanasMAlvarezJGarcia-PerisPANutritional support and quality of life in stable chronic obstructive pulmonary disease (COPD) patientsClin Nutr200524343344115896431
- McDonaldVMGibsonPGScottHAShould we treat obesity in COPD? The effects of diet and resistance exercise trainingRespirology201621587588226916174
- KimSGKoKHwangICRelationship between indices of obesity obtained by anthropometry and dual-energy X-ray absorptiometry: The Fourth and Fifth Korea National Health and Nutrition Examination Survey (KNHANES IV and V, 2008–2011)Obes Res Clin Pract20159548749825484303
- KimYHanBDHanKOptimal cutoffs for low skeletal muscle mass related to cardiovascular risk in adults: The Korea National Health and Nutrition Examination Survey 2009–2010Endocrine201550242443325862070
- FlegalKMShepherdJALookerACComparisons of percentage body fat, body mass index, waist circumference, and waist-stature ratio in adultsAm J Clin Nutr200989250050819116329
- PradoCMSiervoMMireEA population-based approach to define body-composition phenotypesAm J Clin Nutr20149961369137724760978
- AronsonDBarthaPZinderOObesity is the major determinant of elevated C-reactive protein in subjects with the metabolic syndromeInt J Obes Relat Metab Disord200428567467914993913
- FlorezHCastillo-FlorezSMendezAC-reactive protein is elevated in obese patients with the metabolic syndromeDiabetes Res Clin Pract20067119210016002176
- VestboJEdwardsLDScanlonPDECLIPSE InvestigatorsChanges in forced expiratory volume in 1 second over time in COPDN Engl J Med2011365131184119221991892
- SuzukiMMakitaHKonnoSHokkaido COPD Cohort Study InvestigatorsAsthma-like features and clinical course of chronic obstructive pulmonary disease. An analysis from the Hokkaido COPD cohort studyAm J Respir Crit Care Med2016194111358136527224255
- HizawaNMakitaHNasuharaYHokkaido COPD Cohort Study GroupFunctional single nucleotide polymorphisms of the CCL5 gene and nonemphysematous phenotype in COPD patientsEur Respir J200832237237818385174