
Abstract
Purpose
To investigate how the changes of definition in assessment of Global Initiative for Chronic Obstructive Lung Disease (GOLD) stratification 2017 lead to changes of chronic obstructive pulmonary disease (COPD) patient clinical characteristics across categories in China.
Patients and methods
COPD patients from 11 medical centers in China were stratified into old and new groups A–D twice according to the GOLD 2011 and 2017 comprehensive assessment. Demography and clinical characteristics were compared between old and new groups A–D.
Results
In 1,532 COPD patients, the distribution from group A to D was 330 (21.5%), 132 (8.6%), 411 (26.8%), 659 (43.0%) and 557 (36.4%), 405 (26.4%), 184 (12.0%), 386 (25.2%), respectively according to GOLD 2011 and 2017. 46.7% (500/1,070) patients in high-risk groups were regrouped to low-risk groups. Compared to the old groups A and B, the new groups A and B had a higher proportion of males, lower body mass index, higher modified Medical Research Council (mMRC) grade, poor pulmonary function, more patients with chronic bronchitis, and fewer patients with coronary heart disease and hypertension disease. Compared to the old groups C and D, the new groups C and D had older patients, fewer men, better pulmonary functions, frequent acute exacerbations in the previous year, and more patients with chronic bronchitis, coronary heart disease, or diabetes mellitus. The new group D had more patients with stroke than the old group D.
Conclusion
In China, GOLD 2017 shifted the overall COPD comprehensive assessments distribution to more low-risk groups. The new high-risk groups had more characteristics associated with high risk of acute exacerbation and mortality. Some of the changes in demography and clinical characteristics of the new low-risk groups were associated with high risk of acute exacerbation and/or mortality.
Introduction
Chronic obstructive pulmonary disease (COPD) is a common, preventable, and treatable disease characterized by persistent respiratory symptoms and airflow limitation that is due to airway and/or alveolar abnormalities usually caused by significant exposure to noxious particles or gases.Citation1 The clinical management of COPD was mostly guided by the severity of airflow limitation before 2011.Citation2 However, there is heterogeneity in clinical presentation, imaging findings, physiological pulmonary function testing, response to therapy, and patient survival in COPD.Citation3–Citation6 As a result, there is now a consensus that forced expiratory volume in one second (FEV1) alone does not adequately reflect the complexity of the disease, and that measurement of FEV1 should not be used in isolation for the optimal diagnosis, assessment, and management of patients with COPD. At the same time, Hurst et alCitation3 found that the best predictor of having frequent exacerbations (defined as two or more exacerbations per year) is the history of past-year exacerbation instead of pulmonary function. An understanding of the impact of COPD on an individual patient combines the symptomatic assessment with the patient’s spirometric classification and/or risk of exacerbations, and the 2011 revision of the Global Initiative for Chronic Obstructive Lung Disease (GOLD)Citation7 incorporated assessment of symptoms, severity of airflow limitation, and history of exacerbations into the ratings of severity. The classification system was linked to initial disease management, including the use of short- and long-acting bronchodilators and inhaled corticosteroids (ICS). However, there were some important limitations of the GOLD 2011 assessment. This assessment tool performed no better than the spirometric grades for prediction of mortalityCitation8,Citation9 and pulmonary function’s declineCitation9,Citation10 or other important health outcomes in COPD. Because of the limitations of GOLD 2011 assessment, the refinement of the ABCD assessment tool is proposed in the GOLD 2017.Citation1 GOLD 2017 revises the classification system and removes spirometry measure in the categorization, leaving the categorization based on symptoms and frequency of exacerbations.Citation1 Because of the change of criterion of the assessment tool, patients from high-risk groups (groups C and D) without COPD exacerbation history in the previous year will be shifted to the low-risk groups (groups A and B). We sought to investigate how the changes of definition lead to changes of patient demography and clinical characteristics across categories.
Methods
Study design and patients
The study was a retrospective database analysis and involved a national cross-sectional observational survey, which was performed to investigate the attitudes and actions of patients with COPD in 11 medical centers of seven provinces (Beijing, Liaoning, Inner Mongolia, Sichuan, Shanghai, Hubei, and Guangdong) in China. Patients were recruited from COPD outpatient clinics in 2007 and 2008. The study was approved by the Ethics Committee of Peking University Third Hospital. All data in the database were de-identified.
Subjects with post-bronchodilator FEV1/forced vital capacity (FVC) <70% were defined as having COPD according to the criteria recommended by the Chinese Medical Society.Citation11 Persistent airflow limitation was defined as FEV1/FVC <70% after 400 µg of inhaled salbutamol. Briefly, patients were enrolled consecutively during a visit in 11 medical centers for a COPD diagnosis in stable stage. Patients with stable COPD were free from acute exacerbation of symptoms and upper respiratory tract infection in the two months preceding the study. Patients with bronchiectasis, bronchial asthma, lung cancer, and left ventricular dysfunction were excluded. Each patient was interviewed on a single occasion.
Study procedures
Self-administered questionnaires were given to each patient and included the modified Medical Research Council (mMRC) questionnaire to record demographic and medical history data including symptoms, exacerbation history, past history, and the results of pulmonary function tests. The short form-36 mental component summary (SF-36 MCS) and the short form-36 physical component summary (SF-36 PCS) were also used to assess the life quality of patients. The GOLD 2011 comprehensive assessmentCitation7 stratified patients initially on the basis of symptoms (mMRC grade 0–1 vs ≥2) with a score resulting in two low-symptom categories (A and C) and two high-symptom categories (B and D). Exacerbation risk was assessed with either spirometric airflow obstruction measured by FEV1% predicted (<50% or ≥50%), or by COPD exacerbation history in the previous year (0 vs ≥1 hospitalization). This allowed stratification of patients into low-risk categories (A and B) and high-risk (C and D) categories. When the exacerbation risk, as determined by FEV1% predicted value, or the previous exacerbation history were not identical, risk was defined by the method showing the greater risk. Exacerbations were defined as clinical presentations requiring assessment and treatment in hospital admission in the previous year. All of the groups based on the GOLD 2011 were named old groups in the study, such as old A (AO), old B (BO), old C (CO), and old D (DO). The GOLD 2017 comprehensive assessmentCitation1 stratified patients also on the basis of symptoms (mMRC grade 0–1 vs ≥2) with a score resulting in two low-symptom categories (A and C) and two high-symptom categories (B and D). Exacerbation risk was assessed only by COPD exacerbation history in the previous year (0 vs ≥1 hospitalization); this allowed stratification of patients into low-risk categories (A and B) and high-risk (C and D) categories. All of the groups based on the GOLD 2017 were named new groups in the study, such as new A (AN), new B (BN), new C (CN), and new D (DN).
Statistical analysis
All statistical analyses were performed with SPSS version 17.0 (SPSS, Chicago, IL, USA). Descriptive data with normal distribution were expressed as means ± SD. Descriptive data without normal distribution were expressed as medians (interquartile range) and frequencies were expressed as percentages. The McNemar test was used to assess changes in distribution by GOLD 2011 and GOLD 2017 comprehensive assessment. Forest plot using standardized mean difference of continuous variables and or odds ratio of categorical variables was used to show the differences between new groups A–D and old groups A–D.
Results
Patient distribution by GOLD 2011 and 2017 comprehensive assessment methods
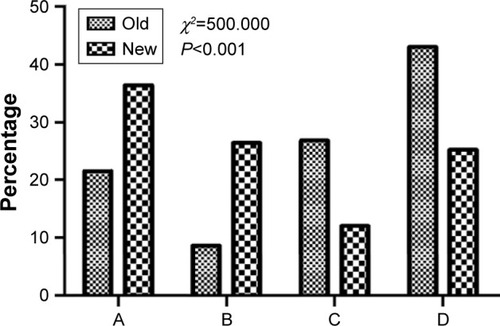
From the initial surveyed number of 2,072 patients, 540 patients were excluded in which 337 patients had no pulmonary function test result, 38 patients did not meet the COPD criteria, and 165 patients had no records of acute exacerbation, and 1,532 patients were finally analyzed (). Of the 1,532 patients with COPD recruited to this study, the distribution of old comprehensive assessment groups according to GOLD 2011: Group AO was 21.5% (330/1,532), BO was 8.6% (132/1,532), CO was 26.8% (411/1,532), and DO was 43.0% (659/1,532). Using the new GOLD 2017 comprehensive assessment, group AN was 36.4% (557/1,532), BN was 26.4% (405/1,532), CN was 12.0% (184/1,532), and DN was 25.2% (386/1,532) (). 46.7% (500/1,070) patients in high-risk groups (groups CO and DO) were regrouped to low-risk groups (groups AN and BN). Group C became the smallest group instead of group B ().
Figure 1 Study flow chart.
Note: Groups A–D: COPD patients were stratified into group A to D twice according to the GOLD 2011 and 2017 comprehensive assessments.
Abbreviations: COPD, chronic obstructive pulmonary disease; GOLD, Global Initiative for Chronic Obstructive Lung Disease; PFT, pulmonary function test.
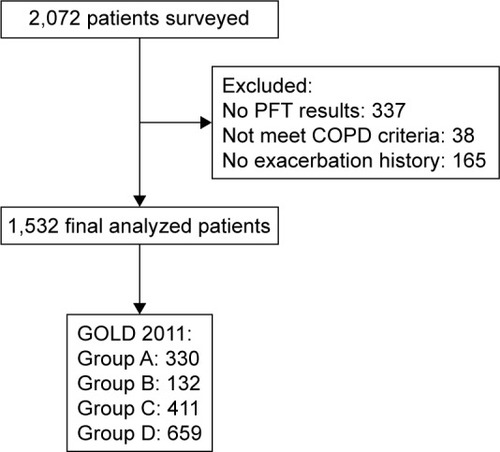
Figure 2 Distribution of groups A–D of the old (GOLD 2011) and new (GOLD 2017) comprehensive assessment.
Abbreviation: GOLD, Global Initiative for Chronic Obstructive Lung Disease.
Changes in demographic and clinical characteristics of low-risk groups according to the changes in distribution by GOLD 2011 and 2017 comprehensive assessment methods
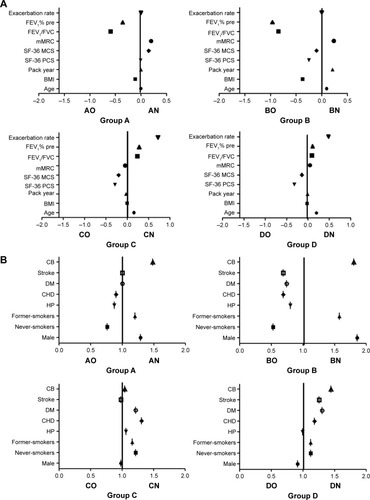
According to the GOLD 2017 comprehensive assessment, low-risk groups (groups AN and BN) had been increased by about 2 times. Demographic and clinical characteristics of old and new groups A and B by GOLD 2011 and GOLD 2017 comprehensive assessment were different (). Compared to the groups AO and BO, the groups AN and BN had more men, smokers, and patients with chronic bronchitis whereas fewer patients with coronary heart disease and hypertension disease. The patients of groups AN and BN had lower body mass index (BMI), higher mMRC grade, and poorer pulmonary function ().
Table 1 The distribution by GOLD 2011 and 2017 comprehensive assessment in demographic and clinical characteristics
Figure 3 Difference in demographic and clinical characteristics for GOLD 2011 and GOLD 2017 categories.
Abbreviations: AO, old A; AN, new A; BMI, body mass index; BO, old B; BN, new B; CB, chronic bronchitis; CHD, coronary heart disease; CO, old C; CN, new B; DM, diabetes mellitus; DO, old D; DN, new D; FEV1, forced expiratory volume in one second; FVC, forced vital capacity; GOLD, Global Initiative for Chronic Obstructive Pulmonary Disease; HP, hypertension; mMRC, modified Medical Research Council; SF-36 MCS, short form-36 mental component summary; SF-36 PCS, short form-36 physical component summary; SMD, standardized mean difference.
Changes in demographic and clinical characteristics of high-risk groups according to the changes in distribution by GOLD 2011 and 2017 comprehensive assessment methods
Following the changes in distribution, there were differences between the high-risk groups and low-risk groups (). When the patients who did not have acute exacerbations in the previous year were shifted to low-risk group, the high-risk groups were reduced and changed in its demographic and clinical characteristics. Compared to the groups CO and DO, the groups CN and DN had older patients, and fewer male patients and smokers. There were more patients with chronic bronchitis, coronary heart disease, or diabetes mellitus in groups CN and DN. Furthermore, the patients of groups CN and DN had lower SF-36 PCS and SF-36 MCS, better pulmonary functions, and more times of acute exacerbations in the previous year. Otherwise, group CN had more patients with hypertension disease than group CO whereas group DN had more patients with stroke than group DO ().
Discussion
This study investigated the distribution and clinical characteristics of COPD in a disease cohort in China using GOLD 2011 and GOLD 2017 comprehensive assessment. GOLD 2017 shifted the overall COPD severity distribution to low-risk categories. The new high-risk groups had more demography and clinical characteristics, which were associated with high risk of acute exacerbation and/or mortality. However, the changes in demography and clinical characteristics of the new low-risk groups were in two opposite ways in terms of risks of acute exacerbation and mortality. Some characteristics of the new low-risk groups were associated with high risk of acute exacerbation and/or mortality. The key difference of pharmacologic therapy between high-risk and low-risk groups was the use of ICS. When we make the decision about the treatment of ICS for COPD patients, should we just care about the history of acute exacerbation?
The core change of refinement of the ABCD assessment tool proposed in the GOLD 2017 was the shift of patients with lower frequency of acute exacerbation and poor pulmonary function from the high-risk groups to the low-risk groups. In the present study, COPD patients were recruited from 11 outpatient clinics at medical centers in China. According to the GOLD 2011, about 70% of patients were in the high-risk groups. The relative number of patients with COPD was greatest in group D. This prevalence was similar to that reported in the previous COPD cohorts that were recruited from hospital clinics but was clearly different from that described in COPD patients identified in the general population, where group A predominates.Citation12–Citation15 The distribution of patient categories in the GOLD classification system may be different in different populations and may also depend on the patient selection criteria. GOLD 2011 shifted the overall COPD severity distribution to more severe categories.Citation8 According to the GOLD 2017, almost half of old high-risk groups were regrouped to the new low-risk groups. More than 60% of patients were in the low-risk groups. Group A became the biggest group. Neven Tudoric et al also showed according to the revised ABCD classification, more than a third of patients formerly classified as “D” and almost half of patients formerly classified as “C” solely on the basis of poor lung function moved from the high-risk groups to the low-risk groups.Citation16 GOLD 2017 shifted the overall COPD severity distribution to milder categories.
What is the clinical implication for the changes of distribution? The new definition changes in distribution lead to changes in distribution of patients’ demography and clinical characteristics across categories. Patients of groups CN and DN had better pulmonary function but higher acute exacerbation rates, as well as the similar degree of dyspnea. Groups CN and DN had older patients and more patients with chronic bronchitis, coronary heart disease, and diabetes mellitus than groups CO and DO. There is a strong relativity between age and exacerbation times in the past 12 months in this study. Several studies had proved that age was statistically significantly associated with a higher odds of hospitalized exacerbationsCitation17 and mortalityCitation17,Citation18 in the following year in the multivariable modes. Several large studies also have shown that chronic bronchitis was significantly and consistently associated with both a higher mortalityCitation19 and an increased risk of COPD hospitalization.Citation20–Citation22 Chronic mucus hypersecretion may be one of the reasons for higher acute exacerbation and mortality of COPD patients with chronic bronchitis. Comorbidities had been proved to occur in patients with mild, moderate, or severe airflow limitation.Citation4 Diabetes has been identified as a predictor of increased risk of COPD readmission in the stepwise multivariate analysisCitation23 and an independent risk factor of death in COPD.Citation18,Citation24 Diabetes mellitus may contribute to the acute exacerbation of group DN patients for the susceptibility to infections. Cardiovascular disease is associated with poor clinical outcomes in COPD.Citation24–Citation26 These characteristics may raise all-cause mortality. Group DN had more patients with stroke, which may decrease the ability of expectoration and recovery. All of the characteristics of group CN and/or DN mentioned above were associated with high risk of acute exacerbation or mortality, some of which increase risks of infection or systemic inflammation.
Patients with poor pulmonary function and without in-hospital–treated acute exacerbation in the previous year were shifted to the low-risk groups. As a result, pulmonary function in the groups AN and BN were worse than the groups AO and BO. Several other changes in demography and clinical characteristics were found in the present study. Compared with the groups AO and BO, the groups AN and BN had a higher proportion of male patients, a higher proportion of smokers, and a greater number of smoking pack years. Landis et alCitation27 showed that the difference of gender is associated with tobacco smoking, because of a higher prevalence of current smokers reported among men. Furthermore, Kohansal et alCitation28 observed that cigarette smokers have a greater annual rate of decline in FEV1. At the same time, Burney et alCitation29 found that airflow limitation increased with mean pack years smoked. Therefore, the changes of sex and smoking status may be associated with the changes of pulmonary functions. The patients in groups AN and BN had a high prevalence of chronic bronchitis than the patients in groups AO and BO. Thomsen et al observed that smoking was associated with more symptoms, more severe disease, and higher burden of systemic inflammation in COPD patients.Citation30 Two studies have shown that COPD patients with chronic bronchitis had greater initial and longitudinal decline in FEV1.Citation20,Citation31 Compared to the groups AO and BO, the groups AN and BN had lower BMI and fewer patients with coronary heart disease and hypertension disease. The lower BMI may increase the risk of acute exacerbation and mortality of the low-risk groups. The decreased numbers of patients with coronary heart disease and hypertension disease may decrease all-cause mortality. Therefore, the changes of demography and clinical characteristics may affect the risk of exacerbation and mortality in different directions.
GOLD 2017 suggests escalation and de-escalation strategies whereas GOLD 2011 only proposes initial therapy. This assessment approach acknowledges the limitations of FEV1 in making treatment decisions for individualized patient care and highlights the importance of patient symptoms and exacerbation risk in guiding the therapies in COPD. This will facilitate more precise treatment recommendations based on parameters that are driving the patient’s symptoms at any given time. The biggest change of treatment for the patients who were shifted from the high-risk groups to the low-risk groups was the reduction of ICS according to the GOLD 2017. According to several data,Citation32,Citation33 COPD patients with frequency of acute exacerbation and poor life quality may benefit from ICS while others will not no matter how poor the pulmonary function was. But besides the chronic inflammation of airway, the COPD patients had systemic features, such as aging, smoking, smoking-associated disease, and diseases associated with systemic inflammation, such as skeletal muscle wasting, ischemic heart disease, osteoporosis, anemia, diabetes, and metabolic syndrome. These systemic features may have impact on health status and survival.Citation34 In general, the presence of comorbidities should not alter COPD treatment and comorbidites should be treated per usual standards regardless of the presence of COPD.Citation1 The main pharmacologic therapy for stable COPD such as ICS and bronchodilators should be according to the severity or characteristics (such as pulmonary function, hyperresponsiveness, and the eosinophils) of lung itself, but not extrapulmonary predictors of acute exacerbation or mortality.
This study had several limitations. First, the patients were recruited from tertiary hospitals, which may not reflect the status of COPD throughout the Chinese population. Second, the study was a retrospective database analysis and involved a national cross-sectional observational survey, and patients were not followed up to evaluate long-term clinical outcomes such as exacerbation frequency, hospitalization, and mortality, and retrospective studies are limited by the quality and completeness of recorded data and the potential for bias and confounding factors. Third, the diagnosis of acute exacerbation of COPD lacked an objective standard, other than hospitalization, which did not include the mild acute exacerbation of patients treated in outpatient clinics or primary care. Fourth, we did not include the COPD assessment test, because it was not available at the start of the study. Therefore, we cannot compare all symptom tools in our study.
Conclusion
In conclusion, we found that under GOLD 2017, about 47% of patients in high-risk groups will be reclassified into low-risk groups in China. The new high-risk groups had more demography and clinical characteristics associated with high risk of acute exacerbation and/or mortality. Some changes in demography and clinical characteristics of the new low-risk groups were associated with high risk of acute exacerbation and/or mortality. Clinicians should revisit patient’s current treatment for those patients who are reclassified into low-risk groups. Further research should examine whether treatment de-escalation is appropriate.
Author contributions
Lina Sun, Yahong Chen, Rui Wu, Ming Lu and Wanzhen Yao were responsible for conception and design, acquisition of data, or analysis and interpretation of data, drafting the article or revising it critically for important intellectual content, final approval of the version to be published, and all agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All authors have read the manuscript and approve its submission.
Acknowledgments
The authors would like to acknowledge the substantial contributions to conception and design, acquisition of data from Jian KANG, MD of The First Hospital Affiliated to The Chinese Medical University, Baiqiang CAI, MD of Peking Union Hospital, Beijing, Xin ZHOU, MD of The First People’s Hospital in Shanghai, Zheng LIU, MD of China Oil and Gas Group Central Hospital, Ping CHEN, MD of Shenyang Military General Hospital, Dejun SUN, MD of Inner Mongolia Autonomous Region People’s Hospital, Jinping ZHENG, MD of Institute of Respiratory Disease, Guoyang WANG of Jingmei Group General Hospital, Yulin FENG of West China Hospital and Yongjian XU of Tongji Hospital, affiliated to Huazhong Science and Technology University. The authors acknowledge grant funding for this study from the Research Special Fund for Public Welfare Industry of Health (Grant Number: 201002008), the Chinese Medical Association Chronic Respiratory Diseases Grants (Grant Number: 07010360044), and the 12th Five-Year National Science and Technology Support Program (Grant Number: 2013BAI06B02). The authors also would like to acknowledge the substantial contributions from David Au, Evan Carey, and Methods in Epidemiology, Clinical and Operations Research (MECOR) course. This manuscript is original and has not been submitted for publication elsewhere. No part of the research presented has been funded by tobacco industry sources.
Disclosure
The authors report no conflicts of interest in this work.
References
- VogelmeierCFCrinerGJMartinezFJGlobal strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 report. GOLD executive summaryAm J Respir Crit Care Med2017195555758228128970
- RabeKFHurdSAnzuetoAGlobal strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summaryAm J Respir Crit Care Med2007176653255517507545
- HurstJRVestboJAnzuetoASusceptibility to exacerbation in chronic obstructive pulmonary diseaseN Engl J Med2010363121128113820843247
- AgustiACalverleyPCelliBCharacterization of COPD heterogeneity in the ECLIPSE cohortRespir Res20101112220831787
- HanMKAgustiACalverleyPMChronic obstructive pulmonary disease phenotypesAm J Respir Crit Care Med2010182559860420522794
- DivoMCoteCde TorresJPComorbidities and risk of mortality in patients with chronic obstructive pulmonary diseaseAm J Respir Crit Care Med2012186215516122561964
- VestboJHurdSSAgustíAGGlobal strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summaryAm J Respir Crit Care Med2013187434736522878278
- SorianoJBLamprechtBRamirezASMortality prediction in chronic obstructive pulmonary disease comparing the GOLD 2007 and 2011 staging systems: a pooled analysis of individual patient dataLancet Respir Med20153644345025995071
- GoossensLMLeimerIMetzdorfNBeckerKRutten-van MolkenMPDoes the 2013 GOLD classification improve the ability to predict lung function decline, exacerbations and mortality: a post-hoc analysis of the 4-year UPLIFT trialBMC Pulm Med20141416325326750
- KimJYoonHIOhYMLung function decline rates according to GOLD group in patients with chronic obstructive pulmonary diseaseInt J Chron Obstruct Pulmon Dis2015101819182726379432
- Chinese Medical Association of Respiratory Disease BranchGuideline of diagnosis and treatment of Chronic obstructive pulmonary disease (2007 Revision)Chin J Tuberc Respir Dis2007301817
- LangePMarottJLVestboJPrediction of the clinical course of chronic obstructive pulmonary disease, using the new GOLD classification: a study of the general populationAm J Respir Crit Care Med20121861097598122997207
- SorianoJBAlfagemeIAlmagroPDistribution and prognostic validity of the new Global Initiative for Chronic Obstructive Lung Disease grading classificationChest2013143369470223187891
- AgustiAEdwardsLDCelliBCharacteristics, stability and outcomes of the 2011 GOLD COPD groups in the ECLIPSE cohortEur Respir J201342363664623766334
- SahadevanACusackRO’KellyBAmoranOLaneSJThe Value of the combined assessment of COPD in accurate characterization of stable COPDIr Med J2016109133834026904790
- TudoricNKoblizekVMiravitllesMGOLD 2017 on the way to a phenotypic approach? Analysis from the phenotypes of COPD in central and eastern Europe (POPE) cohortEur Respir J2017494160251828446560
- SantibáñezMGarrastazuRRuiz-NuñezMPredictors of hospitalized exacerbations and mortality in chronic obstructive pulmonary diseasePLoS One2016116e015872727362765
- GudmundssonGUlrikCSGislasonTLong-term survival in patients hospitalized for chronic obstructive pulmonary disease: a prospective observational study in the Nordic countriesInt J Chron Obstruct Pulmon Dis2012757157623055707
- KimVCrinerGJChronic bronchitis and chronic obstructive pulmonary diseaseAm J Respir Crit Care Med2013187322823723204254
- BurgelPRNesme-MeyerPChanezPInitiatives Bronchopneumopathie Chronique Obstructive Scientific CommitteeCough and sputum production are associated with frequent exacerbations and hospitalizations in COPD subjectsChest2009135497598219017866
- KimVHanMKVanceGBCOPDGene InvestigatorsThe chronic bronchitic phenotype of COPD: an analysis of the COPDGene studyChest2011140362663321474571
- KimVMakeBJReaganEAChronic bronchitis predicts greater frequency and severity of COPD exacerbations in moderate to severe COPD [abstract]Am J Respir Crit Care Med2012185A3735
- CrisafulliETorresAHuertaAC-reactive protein at discharge, diabetes mellitus and ≥1 hospitalization during previous year predict early readmission in patients with acute exacerbation of chronic obstructive pulmonary diseaseCOPD201512330631425279441
- LaforestLRocheNDevouassouxGFrequency of comorbidities in chronic obstructive pulmonary disease, and impact on all-cause mortality: a population-based cohort studyRespir Med2016117333927492511
- AgustiAEdwardsLDRennardSIPersistent systemic inflammation is associated with poor clinical outcomes in COPD: a novel phenotypePLoS One201275e3748322624038
- LangePMogelvangRMarottJLCardiovascular morbidity in COPD: a study of the general populationCOPD20107151020214458
- LandisSHMuellerovaHManninoDMContinuing to confront COPD international patient survey: methods, COPD prevalence, and disease burden in 2012–2013Int J Chron Obstruct Pulmon Dis2014959761124944511
- KohansalRMartinez-CamblorPAgustíAThe natural history of chronic airflow obstruction revisited: an analysis of the Framingham offspring cohortAm J Respir Crit Care Med2009180131019342411
- BurneyPJithooAKatoBBurden of Obstructive Lung Disease (BOLD) StudyChronic obstructive pulmonary disease mortality and prevalence: the associations with smoking and poverty a BOLD analysisThorax201469546547324353008
- ThomsenMNordestgaardBGVestboJLangePCharacteristics and outcomes of chronic obstructive pulmonary disease in never smokers in Denmark: a prospective population studyLancet Respir Med20131754355024461615
- ShermanCBXuXSpeizerFEFerrisBGJrWeissSTDockeryDWLongitudinal lung function decline in subjects with respiratory symptomsAm Rev Respir Dis199214648558591416410
- YangIAClarkeMSSimEHFongKMInhaled corticosteroids for stable chronic obstructive pulmonary diseaseCochrane Database Syst Rev20127CD002991
- NanniniLJLassersonTJPoolePCombined corticosteroid and long-acting beta(2)-agonist in one inhaler versus long-acting beta(2)-agonists for chronic obstructive pulmonary diseaseCochrane Database Syst Rev201299CD006829
- MillerJEdwardsLDAgustíAEvaluation of COPD longitudinally to identify predictive surrogate endpoints (ECLIPSE) investigatorsComorbidity, systemic inflammation and outcomes in the ECLIPSE cohortRespir Med201310791376138423791463