
Abstract
Rationale
COPD has attracted widespread attention worldwide. The prevalence of COPD in Taiwan has been reported, but little is known about trends in health care resource utilization and pharmacologic management in COPD treatment.
Objective
The objective of this article was to study trends in health care resource utilization, pharmacologic management, and medical costs of COPD treatment in Taiwan.
Materials and methods
Reimbursement claims in the Taiwan National Health Insurance System from 2004 to 2010 were collected. The disease burden of COPD, including health care resource utilization and medical costs, was evaluated.
Results
The pharmacy cost of COPD increased from 2004 to 2010 due to the increased utilization of long-acting muscarinic antagonist (LAMA) and fixed-dose combination of long-acting β2-agonist and inhaled corticosteroid (LABA/ICS), whereas the cost of all other COPD-related medications decreased. The average outpatient department (OPD) cost per patient increased 29.3% from 1,070 USD in 2004 to 1,383 USD in 2010. The highest average total medical cost per patient was 3,434 USD in 2005, and it decreased 12.4% to 3,008 USD in 2010. There was no significant difference in the average number of OPD visits and emergency department visits per patient. The highest average number of hospital admissions was 0.81 in 2005, and it decreased to 0.65 in 2010. The average number of intensive care unit (ICU) admissions decreased from 0.52 in 2005 to 0.31 in 2010.
Conclusion
From 2004 to 2010, the average total medical cost per patient of COPD was slightly decreased because of the decreased average number of hospital admissions and ICU admissions. The costs of both LAMA and LABA/ICS increased, while the cost for all other COPD-related medications decreased. These findings suggest that the increased utilization of LAMA and LABA/ICS may have contributed to the decreased average number of hospital admissions and ICU admissions in COPD patients from 2004 to 2010.
Introduction
COPD has attracted widespread attention because of its increasing prevalence, mortality rate, and economic burden worldwide.Citation1,Citation2 Patients with COPD have more health care resource utilization than those without COPD because of the existence of comorbidities and repeated acute exacerbation.Citation3,Citation4 Hospitalization due to acute exacerbation of COPD (AECOPD) is the major contributor to the medical cost in COPD patients.Citation5 Recent advances in the pharmacologic and non-pharmacologic management of COPD have been shown to reduce the exacerbation rate in COPD patients.Citation6–Citation9 These findings suggest that health care resource utilization and medical costs of COPD might be affected by the pharmacologic management provided to patients.
A previous study that used a population-based questionnaire survey has reported a COPD prevalence rate of 6.1% among adults who were 40 years or older in Taiwan.Citation10 The frequency of exacerbation and unplanned health care utilization and the delivery format of the prescribed medication have also been reported.Citation11 However, detailed health care resource utilization, pharmacologic management, and medical costs of the COPD patients were not reported. The National Health Insurance System covers >99% of the population in Taiwan. The aim of this study is to use the Taiwan National Health Insurance Research Database (NHIRD) to investigate trends in health care resource utilization, pharmacologic management, and medical costs of COPD treatment in Taiwan from 2004 to 2010.
Materials and methods
Data source
This study was approved by the Chang Gung Medical Foundation Institutional Review Board (IRB approval number: 101-0990B). Reimbursement claims in the NHIRD from 2004 to 2010 were collected for this study. The NHIRD was released by the Bureau of National Health Insurance in the electronic form. This database contains the registration files and the original claims data for reimbursement, including details of claims of hospitalization orders, outpatient department (OPD) visits, and emergency department (ED) visits. The International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) was used as the coding system for the diagnosis of diseases in the NHIRD. Various datasets were extracted from the NHIRD for research purposes. In this study, the Longitudinal Health Insurance Database (LHID) of all the national health insurance (NHI) enrollees was used for analysis. The data in the LHID included information on patient characteristics such as gender, date of birth, date of admission and discharge, and date of outpatient visit. All the LHID data used in this study were anonymous and did not contain any identifiable personal information. In addition, this database also included detailed information on all claims for health insurance reimbursement such as prescribed medications, dosage, duration, orders for health examinations, and all medical costs. The longitudinal design was applied in this study to investigate the health care resource utilization of COPD in Taiwan.
Patient selection and data collection
To identify patients with COPD, all NHI enrollees who were 40 years or older and had a diagnosis of COPD (ICD-9-CM codes 491, 492, and 496) in at least two outpatient (OPD) visits or one hospitalization were screened.Citation12,Citation13 The index date was defined as the date of first medical visit with the ICD-9 CM code for COPD. Those screened patients who had received short-acting muscarinic antagonist (SAMA), long-acting muscarinic antagonist (LAMA), short-acting β2-agonist (SABA), long-acting β2-agonist (LABA), inhaled corticosteroid (ICS), fixed-dose combination of LABA and ICS, or xanthines after the index date were enrolled in this study.
Patient characteristics, diagnosis details, and dose and duration of prescribed medications after the index date in all enrolled patients were collected for analysis. To evaluate the comorbidities and the disease severity, the Charlson Comorbidity Index (CCI) of enrolled COPD patients was calculated as previously described.Citation14 Weights of CCI were referred to the work of Charlson et al,Citation14 and definition based on the ICD-9-CM code system of the comorbid conditions was given by the work of Deyo et al.Citation15 The comorbid conditions were defined as conditions diagnosed using ICD-9-CM codes for at least two outpatient visits or one hospitalization. The pharmacy and non-pharmacy costs of OPD visits, ED visits, and hospitalizations were recorded and defined as total medical costs. The numbers of all-cause OPD visits, ED visits, and hospitalizations after the index date were recorded each year. Intensive care unit (ICU) admission was defined as hospitalization with claims of reimbursement of ICU cost.
Statistical analysis
Descriptive analysis was applied in the study. Continuous variables are presented as values of mean ± standard deviation, and categorical variables are expressed as percentages. Analysis of variance (ANOVA) and the χ2 test were used to analyze continuous and categorical variables, respectively. P-values <0.05 were considered as statistically significant.
Results
Patient characteristics
From 2004 to 2010, there were 385,453 patients who were 40 years or older and had a diagnosis code of COPD in at least two OPD visits or one hospitalization. Among these patients, 351,375 patients received SAMA, LAMA, SABA, LABA, ICS, fixed-dose combination of long-acting β2-agonist and inhaled corticosteroid (LABA/ICS), or xanthines after the index date and were enrolled in this study. The number, average age, and gender of the enrolled patients for each year are shown in . The number of enrolled COPD patients in 2004 was 93,314, which accounted for 1.02% of the total population who were 40 years or older. The number of patients was then gradually increased to 276,499 in 2010 and accounted for 2.6% of the total population who were 40 years or older. However, this number might not represent the prevalence of COPD in Taiwan. Because only the first three diagnosis codes in the OPD visit and the first five diagnosis codes in the hospitalization were recorded in the NHIRD, it is possible that the prevalence of COPD might be underestimated by analysis using NHIRD. The number of newly enrolled patients for each year was also listed. The CCI of the newly enrolled patients for each year increased from 1.9 in 2004 to 2.39 in 2005. There was no significant difference in CCI from 2005 to 2010.
Table 1 Number and characteristics of enrolled COPD patients in each year
Trends in costs of pharmacologic management of COPD
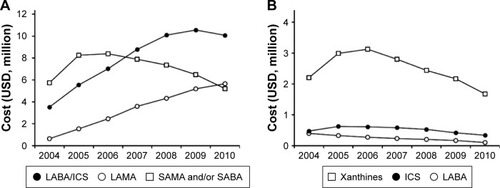
The annual pharmacy cost for SAMA and/or SABA was highest in 2006; it decreased in the following 4 years. The costs for LABA/ICS and LAMA increased from 2004 to 2010 (). The cost for LABA was low in 2004, and this cost decreased further during the study period. There was a slight decrease in the cost for ICS from 2005 to 2010. The cost for xanthines was highest in 2006; it decreased in the following 4 years ().
Figure 1 Descriptive analysis of the utilization of COPD medication.
Abbreviations: LAMA, long-acting muscarinic antagonist; LABA/ICS, fixed-dose combination of long-acting β2-agonist and inhaled corticosteroid; SAMA, short-acting muscarinic antagonist; SABA, short-acting β2-agonist; ICS, inhaled corticosteroid; LABA, long-acting β2-agonist.
Trends in the medical costs for COPD
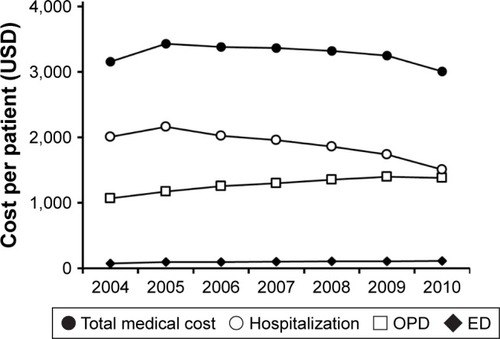
The total medical costs consisted of both the pharmacy and non-pharmacy costs for all-cause OPD visits, ED visits, hospitalizations, and ICU admissions. The average OPD cost per patient increased 29.3% from 1,070 USD in 2004 to 1,383 USD in 2010, while the average hospitalization cost per patient decreased 25% from 2,011 USD in 2004 to 1,508 USD in 2010 (). There was a slight increase in the average ED cost per patient from 79 USD in 2004 to 117 USD in 2010. The highest average total medical cost per patient was 3,434 USD in 2005, and it gradually decreased 12.4% in the following 5 years to 3,008 USD in 2010.
Figure 2 Descriptive analysis of the average cost per COPD patient.
Abbreviations: OPD, outpatient department; ED, emergency department.
Trends in the health care resource utilization in COPD patients
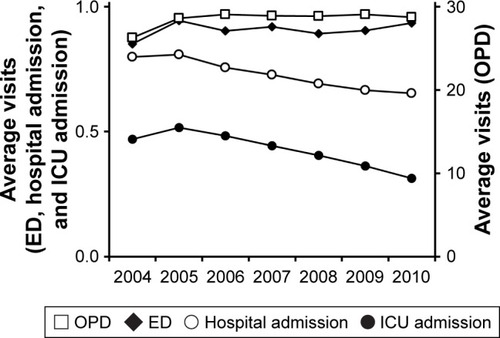
Although the average number of OPD visits per patient increased from 26.3 in 2004 to 28.6 in 2005, there was no significant difference from 2005 to 2010 (). The same trend was also found in the average number of ED visits per patient, which increased from 0.85 in 2004 to 0.95 in 2005; however, there was no significant difference in the average number of ED visits per patient from 2005 to 2010. The highest average number of hospital admissions of these enrolled COPD patients was 0.81 in 2005, and it decreased to 0.65 in 2010. In addition, the average number of ICU admissions also decreased from 0.52 in 2005 to 0.31 in 2010.
Figure 3 Descriptive analysis of the health care resource utilization of COPD in Taiwan.
Abbreviations: OPD, outpatient department; ED, emergency department; ICU, intensive care unit.
Discussion
In this study, we found that the costs for LABA/ICS and LAMA increased from 2004 to 2010 and the costs for all other COPD-related medications decreased. Although the average OPD cost per patient increased, the average total medical cost per patient decreased due to the decreased average hospitalization cost. Both the average number of hospital admissions and ICU admissions were decreased, whereas there were no significant differences in the average OPD visits or ED visits.
The average medical cost per patient decreased from 2004 to 2010 in this study, and this decrease was due to the decreased average hospitalization cost per patient. In addition, the decrease in the average hospitalization cost per patient was mainly due to the decrease in the number of hospital admissions and ICU admissions. AECOPD-related hospitalization has been found to be the major contributor to the total medical cost in COPD patients.Citation5 The reported trends in AECOPD-related hospitalization vary in different countries and study periods. The incidence of AECOPD-related hospitalization in the general population increased in France between 1998 and 2007 and in Australia between 1993 and 2003.Citation16,Citation17 However, the incidence of AECOPD-related hospitalization in the general population decreased in Spain between 2006 and 2010, in the US between 1999 and 2011, and in Puglia between 2005 and 2007.Citation18–Citation20 The incidence of hospitalization for COPD can be significantly affected by the prevalence of COPD and the regional health care policies.Citation21 In the aforementioned study in the US, both the prevalence of COPD and the incidence of COPD-related hospitalization decreased.Citation19 Another study using claims data of Medicare beneficiaries in the US has also shown a substantial decrease in the all-cause and respiratory-related hospitalization rate in COPD patients from 1999 to 2008.Citation22 Using the claims data of the Taiwan NHIRD in this study, we found that both the average number of all-cause hospital admissions and ICU admissions in COPD patients decreased from 2005 to 2010 in Taiwan.
In a previous study, LAMA has been shown to reduce hospitalizations, hospital stay, and average hospitalization cost in COPD patients.Citation23 However, the acquisition cost of LAMA was not considered in that study. Utilization of LABA/ICS had been shown to reduce the exacerbation rate in COPD patients.Citation7,Citation24 However, the impact of the utilization of LABA/ICS on the medical cost remains uncertain. Adding formoterol/budesonide to tiotropium has been shown to increase the short-term total direct cost for COPD patients but reduce the indirect and total costs.Citation25 However, utilization of salmeterol/fluticasone propionate has been shown to reduce the COPD-related total medical cost within 1 year after patients’ discharge from a hospitalization or ED visit.Citation26 Both LABA/ICS and LAMA were approved for the treatment of COPD in Taiwan in 2003. In this study, we found that the costs for LABA/ICS and LAMA increased, whereas the costs for all other COPD-related medications decreased. Although the average OPD cost per patient increased slightly, the average total medical cost per patient decreased due to the decreased average number of hospital admissions and ICU admissions. These findings suggest that the utilization of LABA/ICS and LAMA might contribute to the decreased number of hospital admissions and ICU admissions observed in this study.
There are limitations in this study. First, the indirect cost of COPD was not recorded in the NHIRD. The indirect cost has been found to account for a substantial socioeconomic burden in the working population with COPD.Citation27,Citation28 The lack of this information in the NHIRD has prevented the investigation of the impact of indirect costs on the socioeconomic burden. Second, spirometry results were not recorded in the NHIRD. In addition, the results of the average medical cost and health care resource utilization were raw and unadjusted numbers. Risk adjustment and a control cohort were not considered for evaluating the medical costs, pharmacy costs, and health care resource utilization metrics. The degree of airflow limitation has been shown to correlate with the mortality of COPD patients.Citation29 However, the degree of airflow limitation may not be the only predictor for the prognosis of COPD patients.Citation30 In this study, there was no significant difference in the average CCI of the newly enrolled patients from 2005 to 2010. The existence of comorbidities has been found to be significantly correlated with respiratory impairment, risk of acute exacerbation, and health care resource utilization of COPD.Citation31–Citation33 In addition, the CCI has been shown to be a predictor of mortality and hospital readmissions in AECOPD-related hospitalization.Citation34,Citation35 These findings suggest that the CCI may be used as an indirect indicator of disease severity and predictor of health care resource utilization of COPD. Third, the mortality rate of COPD patients with frequent hospitalizations is higher than that of patients without frequent hospitalizations, and patients with frequent hospitalizations were more likely to die during the study period.Citation36–Citation38 The deaths of COPD patients with frequent hospitalizations during the study period might also have contributed to the decrease in the average hospitalization rate and ICU admission rate from 2004 to 2010. However, previous studies also showed that even under effective treatment, the pulmonary function of COPD patients still decreased over time.Citation6,Citation7 This finding suggested that for patients who did not die during the study period, the disease severity might be increased. In addition, we performed descriptive analysis to investigate the trends in pharmacologic management and health care resource utilization of COPD from 2004 to 2010 in Taiwan. The medical cost inflation during the study period might contribute to the change in the average medical cost of enrolled COPD patients. On the other hand, the medical cost inflation had no effect on the decrease in the average number of hospital admissions and ICU admissions observed in this study.
Conclusion
In this study, we observed a slight decrease in the average total medical cost per patient of COPD in Taiwan from 2004 to 2010. This decrease in the average total medical cost was mainly due to the decrease in the average number of hospital admissions and ICU admissions in COPD patients. At the same time, the pharmacy cost for both LAMA and LABA/ICS increased and the cost for all other COPD-related medications decreased. These findings suggest that the increased utilization of LAMA and LABA/ICS may have contributed to the decreased average number of hospital admissions and ICU admissions in COPD patients from 2004 to 2010.
Author contributions
YH Tsai and TM Yang are co-first authors. All authors contributed toward data analysis, drafting and critically revising the paper, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Acknowledgments
This work was supported by research grants from Chang Gung Memorial Hospital (CORPG6D0161 and COR-PG6D0201) to T-M Yang. This study was based in part on data from the NHIRD provided by the National Health Insurance Administration and the Ministry of Health and Welfare and managed by the National Health Research Institutes (registered number 100342). The interpretation and conclusions contained herein do not represent those of the National Health Insurance Administration, Ministry of Health and Welfare, or National Health Research Institutes.
Disclosure
The authors report no conflicts of interest in this work.
References
- BurneyPSuissaSSorianoJBThe pharmacoepidemiology of COPD: recent advances and methodological discussionEur Respir J Suppl2003431s44s14582902
- MurrayCJLopezADAlternative projections of mortality and disability by cause 1990–2020: Global Burden of Disease StudyLancet19973499064149815049167458
- Lopez VarelaMVMontes de OcaMHalbertRComorbidities and health status in individuals with and without COPD in five Latin American cities: the PLATINO studyArch Bronconeumol2013491146847423856439
- GershonASGuanJVictorJCGoldsteinRToTQuantifying health services use for chronic obstructive pulmonary diseaseAm J Respir Crit Care Med2013187659660123328526
- ChiangCHCost analysis of chronic obstructive pulmonary disease in a tertiary care setting in TaiwanRespirology200813568969418513247
- TashkinDPCelliBSennSA 4-year trial of tiotropium in chronic obstructive pulmonary diseaseN Engl J Med2008359151543155418836213
- CalverleyPMAndersonJACelliBSalmeterol and fluticasone propionate and survival in chronic obstructive pulmonary diseaseN Engl J Med2007356877578917314337
- van RanstDStoopWAMeijerJWOttenHJvan de PortIGReduction of exacerbation frequency in patients with COPD after participation in a comprehensive pulmonary rehabilitation programInt J Chron Obstruct Pulmon Dis201491059106725336938
- KruisALSmidtNAssendelftWJCochrane corner: is integrated disease management for patients with COPD effective?Thorax201469111053105524415716
- ChengSLChanMCWangCCCOPD in Taiwan: a National Epidemiology SurveyInt J Chron Obstruct Pulmon Dis2015102459246726648708
- LimSLamDCMuttalifARImpact of chronic obstructive pulmonary disease (COPD) in the Asia-Pacific region: the EPIC Asia population-based surveyAsia Pac Fam Med2015141425937817
- LindenauerPKStefanMSShiehMSPekowPSRothbergMBHillNSOutcomes associated with invasive and noninvasive ventilation among patients hospitalized with exacerbations of chronic obstructive pulmonary diseaseJAMA Intern Med2014174121982199325347545
- YangHHLaiCCWangYHSevere exacerbation and pneumonia in COPD patients treated with fixed combinations of inhaled corticosteroid and long-acting beta2 agonistInt J Chron Obstruct Pulmon Dis2017122477248528860742
- CharlsonMEPompeiPAlesKLMacKenzieCRA new method of classifying prognostic comorbidity in longitudinal studies: development and validationJ Chronic Dis19874053733833558716
- DeyoRACherkinDCCiolMAAdapting a clinical comorbidity index for use with ICD-9-CM administrative databasesJ Clin Epidemiol19924566136191607900
- WilsonDHTuckerGFrithPAppletonSRuffinREAdamsRJTrends in hospital admissions and mortality from asthma and chronic obstructive pulmonary disease in Australia, 1993–2003Med J Aust2007186840841117437395
- FuhrmanCRocheNVergnenegreAZureikMChouaidCDelmasMCHospital admissions related to acute exacerbations of chronic obstructive pulmonary disease in France, 1998–2007Respir Med2011105459560121130636
- de Miguel-DiezJJimenez-GarciaRHernandez-BarreraVTrends in hospital admissions for acute exacerbation of COPD in Spain from 2006 to 2010Respir Med2013107571772323421969
- FordESCroftJBManninoDMWheatonAGZhangXGilesWHCOPD surveillance – United States, 1999–2011Chest2013144128430523619732
- MorettiAMTafuriSParisiDGerminarioCEpidemiology and costs of hospital care for COPD in PugliaMultidiscip Respir Med20116529930422958809
- EsquinasAMZamarro GarciaCRey TerronLTrends of hospital admissions for acute exacerbation of COPD in Spain: are we needing a new of hospital and health system organization reappraisal?Respir Med201410871066106724820244
- BaillargeonJWangYKuoYFHolmesHMSharmaGTemporal trends in hospitalization rates for older adults with chronic obstructive pulmonary diseaseAm J Med2013126760761423688662
- FriedmanMMenjogeSSAntonSFKestenSHealthcare costs with tiotropium plus usual care versus usual care alone following 1 year of treatment in patients with chronic obstructive pulmonary disorder (COPD)Pharmacoeconomics2004221174174915250751
- SzafranskiWCukierARamirezAEfficacy and safety of budesonide/formoterol in the management of chronic obstructive pulmonary diseaseEur Respir J2003211748112570112
- NielsenRKankaanrantaHBjermerLCost effectiveness of adding budesonide/formoterol to tiotropium in COPD in four Nordic countriesRespir Med2013107111709172123856511
- DalalAAShahMD’SouzaAOMapelDWCOPD-related healthcare utilization and costs after discharge from a hospitalization or emergency department visit on a regimen of fluticasone propionate-salmeterol combination versus other maintenance therapiesAm J Manag Care2011173e55e6521504260
- FletcherMJUptonJTaylor-FishwickJCOPD uncovered: an international survey on the impact of chronic obstructive pulmonary disease [COPD] on a working age populationBMC Public Health20111161221806798
- van BovenJFVegterSvan der MolenTPostmaMJCOPD in the working age population: the economic impact on both patients and governmentCOPD201310662963923845002
- EstebanCQuintanaJMAburtoMPredictors of mortality in patients with stable COPDJ Gen Intern Med200823111829183418795373
- LangePMarottJLVestboJPrediction of the clinical course of chronic obstructive pulmonary disease, using the new GOLD classification: a study of the general populationAm J Respir Crit Care Med20121861097598122997207
- FumagalliGFabianiFForteSINDACO project: COPD and link between comorbidities, lung function and inhalation therapyMultidiscip Respir Med2015101425973198
- ManninoDMThornDSwensenAHolguinFPrevalence and outcomes of diabetes, hypertension and cardiovascular disease in COPDEur Respir J200832496296918579551
- ManninoDMHiguchiKYuTCEconomic burden of COPD in the presence of comorbiditiesChest2015148113815025675282
- HoTWTsaiYJRuanSYHINT Study GroupIn-hospital and one-year mortality and their predictors in patients hospitalized for first-ever chronic obstructive pulmonary disease exacerbations: a nationwide population-based studyPLoS One2014912e11486625490399
- AlmagroPCabreraFJDiezJComorbidities and short-term prognosis in patients hospitalized for acute exacerbation of COPD: the EPOC en Servicios de medicina interna (ESMI) studyChest201214251126113323303399
- WedzichaJABrillSEAllinsonJPDonaldsonGCMechanisms and impact of the frequent exacerbator phenotype in chronic obstructive pulmonary diseaseBMC Med20131118123945277
- Garcia-AymerichJSerra PonsIManninoDMMaasAKMillerDPDavisKJLung function impairment, COPD hospitalisations and subsequent mortalityThorax201166758559021515553
- SuissaSDell’AnielloSErnstPLong-term natural history of chronic obstructive pulmonary disease: severe exacerbations and mortalityThorax2012671195796322684094