
Abstract
Doxofylline, which differs from theophylline in containing the dioxalane group at position 7, has comparable efficacy to theophylline in the treatment of respiratory diseases, but with an improved tolerability profile and a favorable risk-to-benefit ratio. Furthermore, it does not have significant drug–drug interactions as exhibited with theophylline, which make using theophylline more challenging, especially in elderly patients with co-morbidities receiving multiple classes of drug. It is now clear that doxofylline also possesses a distinct pharmacological profile from theophylline (no significant effect on any of the known phosphodiesterase isoforms, no significant adenosine receptor antagonism, no direct effect on histone deacetylases, interaction with β2-adrenoceptors) and therefore, should not be considered as just a modified theophylline. Randomized clinical trials of doxofylline to investigate the use of this drug to reduce exacerbations and hospitalizations due to asthma or COPD as an alternative to expensive biologics, and certainly as an alternative to theophylline are to be encouraged.
Theophylline in the treatment of asthma and COPD
Theophylline has been widely used to treat asthma and COPD since the 1930s, but while effective, it is a drug having a narrow therapeutic window and also many drug–drug interactions.Citation1 Although the use of theophylline preparations is still defined in the Global Initiative for Asthma (GINA) 2015 report as add-on therapy for the treatment of adult patients with asthma, the increased availability of inhaled medicines with improved therapeutic windows means in reality less theophylline is being used.Citation2 The Global Strategy for the Diagnosis, Management, and Prevention of COPD (GOLD) 2017 report also still includes theophylline in recognition of its bronchodilator effect in stable COPD, and because it has been demonstrated to elicit a further improvement in forced expiratory volume in 1 s and breathlessness when added to salmeterol.Citation3 However, the evidence regarding the effect of low-dose theophylline on exacerbation rates is not clear and a recent meta-analysis of 7 observational studies suggests that theophylline slightly increases all-cause death in COPD patients.Citation4 Again, with the increased availability of inhaled medicines with an improved safety profile, the current use of theophylline is declining for the treatment of COPD.
The molecular mechanism(s) of action of theophylline
The molecular mechanism(s) of action of theophylline is (are) not well understood, but several potential targets have been suggested, including non-selective inhibition of phosphodiesterases (PDE), inhibition of phosphoinositide 3-kinase-δ (PI3K-δ), adenosine receptor antagonism and increased activity of certain histone deacetylases (HDACs) that deacetylate lysine residues in chromatin, thereby silencing gene transcription.Citation5
Theophylline relaxes airway smooth muscle (ASM) by inhibition mainly of PDE3 activity, and it has been suggested to prevent mediator release from a range of inflammatory cells by inhibition of PDE4 activity.Citation6 However, the degree of inhibition is small at therapeutic concentrations and relatively high concentrations are needed to elicit effective PDE inhibitory activities.Citation6 It is unlikely, therefore, that theophylline works as bronchodilator and anti-inflammatory drug solely through this mechanism. It has been suggested that the anti-inflammatory effects of theophylline may be mediated via activation of HDAC.Citation7 HDAC counteracts the enzymatic activity of histone acetyltransferase that promotes histone acetylation and the exposure of gene promoter regions for transcription.Citation8 These effects of theophylline are independent of PDE inhibition.Citation7 Theophylline is also an antagonist of adenosine receptors with affinities against the human cloned adenosine receptors in the mM range, (A1 receptor, 10–30 µM; A2A receptor, 2–10 µM; A2B receptor, 10–30 µM; A3 receptor, 20–100 µM), levels that can be achieved clinically.Citation5 It has been proposed that antagonism of A2B receptors for adenosine may account for the efficacy of this drug.Citation9 However, antagonism of adenosine receptors has been reported to account for many of the side effects of theophylline, such as central nervous system (CNS) stimulation, cardiac arrhythmias (both via blockade of A1receptors), gastric hypersecretion, gastroesophageal reflux, and diuresisCitation10 and paradoxically, inhibition of adenosine A2A receptor signaling could potentially worsen inflammation.Citation11
The documentation that low plasma levels of theophylline (~5 mg/L) are able to enhance HDAC activity and restore the anti-inflammatory effects of corticosteroids in COPD by selectively inhibiting PI3K-δCitation12 is extremely interesting. This enzyme is a cell membrane localizing protein that leads to the subsequent phosphorylation of downstream signalling molecules (eg, Akt/PKB), which is activated by oxidative stress in lungs with COPD and involved in the inhibition of HDAC2 activity via phosphorylation.Citation5 It has been suggested that the activation of HDAC2 could contribute to the clinical effectiveness of theophylline as an anti-inflammatory drug and for its complementary activity to corticosteroids. In effect, in patients with COPD, a low dose of oral theophylline combined with an inhaled corticosteroid is more effective in reducing inflammation in sputum than either drug alone.Citation13
The development of other xanthines
The numerous side effects associated with theophylline, drug–drug interactions and requirement for plasma monitoring limit the use of this drug.Citation5 The propensity for these side effects are exacerbated in the elderly with comorbidities, impaired renal and liver function, in patients with cardiac failure and in patients on other medications that could give rise to drug–drug interactions, particularly if chronic overdosing occurs.
Nonetheless, the positive clinical effects of theophylline in airway disease, combined with its advantageous oral bioavailability, has spurred the development of other xanthines for the treatment of respiratory disease such as enprofylline, a A2B selective receptor antagonist that showed some efficacy in the clinic, but was ultimately not developed due to several unwanted side effects, including headache and nausea/vomiting and, mainly, abnormalities of liver function and variable blood levels despite constant oral dosage.Citation14 Others have attempted to develop selective A1 receptor antagonists since this receptor type for adenosine is upregulated in subjects with asthma.Citation15 Bamifylline, a known selective A1 receptor antagonist is approved for the treatment of asthma in a number of countries.Citation16 Also acebrofylline and doxofylline, and more selective PDE inhibitors such as roflumilastCitation17 and RPL 554Citation18, have been developed with the anticipation that such drugs would have greater efficacy than theophylline, but with an improved side effect profile.Citation19 This review will discuss the state-of-the-art of one of these xanthines, doxofylline, and consider this in comparison with our current knowledge of theophylline.
Doxofylline
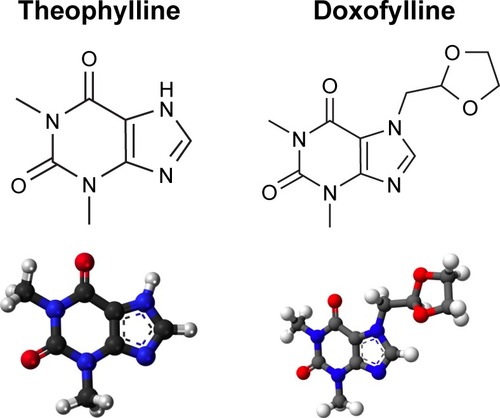
Doxofylline, chemically known as 7-(1,3-dioxolan-2-ylmethyl)-3,7-dihydro-l,3 dimethyl-lH-purine-2,6-dione, is a xanthine derivative having both anti-inflammatory and bronchodilating activities. It differs from theophylline in containing the dioxalane group at position 7 (). It has comparable efficacy with theophylline in the treatment of respiratory diseases, but with an improved tolerability profile.
Figure 1 Bidimensional and tridimensional chemical structure images of theophylline and doxofylline.
The molecular mechanism(s) of action of doxofylline
Doxofylline lacks significant adenosine receptor antagonism. Its affinities against the human, cloned adenosine A1, A2A and A2B receptors are all higher than 100 µM.Citation5 At concentrations that are likely to be achieved in patients following oral dosing, it only has a modest effect on adenosine A2A receptors, but not on any of the other known adenosine receptor subtypes.Citation20 The decreased affinities toward adenosine A1 and A2 receptors, may contribute to its better safety profile.
Animal studies have shown that this poor adenosine antagonism is associated with a negligible stimulation of gastric secretion by doxofyllineCitation23 and importantly, the absence of significant cardiac effects.Citation21 The cardiac activity of doxofylline in comparison with that of theophylline was investigated in guinea pig right and left atrial preparations, and in the anesthetized cat. In spontaneously beating right atria, doxofylline slightly increased the atrial rate, but only at 0.3 mM, while theophylline induced a concentration-dependent positive chronotropic effect that starts at 0.03 mM. In the anesthetized cat, heart rate increased by 13 beats/min with 30 mg/kg doxofylline, but by 20 and 43 beats/min with 10 and 30 mg/kg of theophylline, respectively.Citation24
Doxofylline also has no significant effect on any of the known PDE isoforms, except for PDE2A1, nor is its mechanism of action related to an effect on any of the known HDAC enzymes.Citation20
Recently, using nonlinear chromatography, frontal analysis and molecular docking, Zhang et alCitation25 have documented that the interaction between doxofylline and β2-adrenoceptors elicits relaxation of blood vessel and ASM. Ser169 and Ser173 seem to be the binding sites for the receptor-drug interaction and hydrogen bonding at these sites is likely to be the main driving force for this interaction. Apparently, the nitrogen-atom of the imidazole ring and the oxygen atom of 1,3-dioxolane contributed to the development of this hydrogen bonding. However, it has also been shown that doxofylline, similarly to theophylline, has no effect on formoterol-induced cAMP production (consistent with these drugs not really being significant PDE inhibitors at sensible concentrations) and does not augment formoterol-induced upregulation of the anti-inflammatory protein, mitogen-activated protein kinase phosphatase 1 (MKP-1), in ASM cells.Citation26 Using human peripheral blood eosinophils isolated from asthma patients, Zhou et alCitation27 documented that doxofylline could effectively decrease the open probability of the calcium-activated potassium channels as a result of both the shortening of the open period and the prolongation of the close time. Intriguingly, doxofylline differs from other methylxanthines in its inability to antagonize calcium-activated potassium channels known to be the sites for calcium channel blockers and thus does not interfere with the influx of calcium into cells, or mobilize intracellular calcium stores.Citation28
There is evidence that doxofylline exerts anti-inflammatory activity as it is able to reduce the pleurisy induced by the inflammatory mediator platelet activating factor (PAF) in the rat.Citation29 Additional preclinical studies have shown that doxofylline inhibits bacterial lipopolysaccharide (LPS)-induced neutrophil infiltration into the mouse lung. This effect was secondary to inhibiting leukocyte migration across vascular endothelial cells in vivo and in vitro, suggesting an important effect of this drug on leukocyte diapedesis.Citation30 Furthermore, doxofylline administered for 3 months significantly reduced inflammatory changes and altered cell proliferation of the respiratory tract mucosa, such as infiltration of inflammatory cells, oedema and interstitial fibrosis, in a small group of patients suffering from chronic obstructive bronchitis.Citation31 Interestingly, there is evidence that unlike theophylline, doxofylline does not inhibit tumor necrosis factor-induced interleukin (IL)-8 secretion in ASM cells.Citation26
A very recent study has documented that doxofylline is able to exhibit corticosteroid sparing activity in two murine models of lung inflammation.Citation32 The combination of doxofylline with dexamethasone at doses that themselves did not cause any significant reduction in the inflammation induced by LPS or allergen produced highly significant reductions in leukocyte infiltration into the lung in both models. Indeed the anti-inflammatory effect of the low dose dexamethasone in the presence of a low dose of doxofylline was equivalent to around a 10 times higher dose of dexamethasone administered alone. The precise mechanism of action of doxofylline to explain this corticosteroid sparing effect remains unknown but it is unlikely to be via an HDAC mediated mechanism. Doxofylline is also able to exert prophylactic effects against bronchoconstriction induced by PAFCitation29 and methacholine in experimental animals.Citation33 The results of a study that explored the effects of theophylline and doxofylline on airway responsiveness in beagles showed that doxofylline decreased airway responsiveness at a dose that did not affect heart rate and respiratory rate,Citation33 which was not the case with theophylline under the same experimental conditions.Citation33
Pharmacokinetics of doxofylline
In rats, orally administered doxofylline is rapidly absorbed, metabolized in the liver and partially excreted in the urine.Citation34 It is equally distributed throughout the body, including the brain, although in much lower amounts than those absorbed. Three metabolites have been identified: hydroxyethyltheophylline (β-HET), the chief metabolite of doxofylline, and 2 isomers (cis and trans) of the sulfoxide, of which the trans-isomer predominates. The metabolites are also distributed in tissues, but do not accumulate. β-HET is a weak inhibitor of PDE activity and its affinity for adenosine A1, A2A and A2B receptors is even lower than that of doxofylline. The oral toxicity of β-HET is about 3 times lower than that of doxofylline.Citation35 Elimination is virtually complete at 24 h.
At least in healthy humans, intravenous injection of doxofylline shows a biexponential serum concentration curve with a rapid elimination α-phase of <20 min and total clearance.Citation36 This behavior suggests the involvement of an extra-renal component in its elimination. In Caucasian adults, after oral administration of 400 mg twice daily for 5 days, the peak serum doxofylline concentration was found to be 15.21+1.73 µg/mL with a mean elimination half-life of 7.01+0.80 h.Citation37 A longer half-life results in effective plasma levels, also with twice daily dosing. Even after 12 h from the last oral dose, doxofylline was present in serum in appreciable concentrations. However, there was a large inter-subject variability in peak serum concentrations.
Ethnic differences in the pharmacokinetic profile of doxofylline have been reported. In healthy Chinese volunteers, the concentration time curve obtained from plasma drug concentration data fitted well to a first-order, 1-compartment open model.Citation38 The drug was found to be rapidly absorbed with a marked individual variability, rapidly distributed in the body without an obvious distribution phase, and eliminated with variability among the individuals tested. However, in healthy Indian subjects, pharmacokinetic data were significantly different compared with the Chinese subjects.Citation39 The issue of variability in the pharmacokinetics of doxofylline was also evident in 9 Korean volunteers, although there was no significant correlation between the doxofylline serum level and the body weight, creatinine clearance or age of the subjects.Citation40
From a pharmacokinetic point of view, doxofylline importantly differs from theophylline also because it lacks the ability to interfere with the cytochrome enzymes CYP1A2, CYP2E1 and CYP3A4, thus preventing significant interaction with other drugs metabolized via these pathways in the liver.Citation41 This is a major advantage of doxofylline over theophylline. Furthermore, doxofylline produces more stable serum concentrations than theophylline. Additionally, there is no evidence of an association between doxofylline levels and occurrence of adverse events.Citation22 Therefore, there is no need for continued or repeated blood level monitoring with either low-dose or high-dose doxofylline, which is another big advantage of doxofylline over theophylline.Citation19
Therapeutic differences between doxofylline and theophylline
A number of studies investigating the efficacy and safety of doxofylline have already been discussed in some previous reviews.Citation19,Citation42 Both articles concluded that doxofylline is an effective bronchodilator for relieving airway obstruction and displays a better safety profile with respect to theophylline, having a favorable risk-to-benefit ratio. Indeed, the number of patients needed to treat with doxofylline to spare 1 dropout due to theophylline was found to be 5.Citation22
It is also noteworthy that in patients with endoscopically-proven healed duodenal ulcers, doxofylline, unlike aminophylline, has a low secretagogue activity.Citation43 It also has a superior gastric tolerability than theophylline.Citation19 Furthermore, Sacco et alCitation44 documented that the number of arousals per night when patients were treated with theophylline was almost double compared with when the subjects did not receive any medication, whereas doxofylline did not result in more arousals than no treatment. Sleep architecture and quality remained minimally affected by doxofylline, whereas it was substantially and significantly disrupted by theophylline.
Doxofylline does not increase myocardial oxygen demand,Citation21 which is important when treating patients with ischemic heart disease, particularly relevant for patients with COPD since many such patients suffer from cardiovascular co-morbidities. Doxofylline is also unable to affect atrial frequency or the diastolic pressure in a significant way, unlike theophylline, which often causes hypotension.
In patients with chronic asthma, there is evidence that doxofylline 400 mg t.i.d. is an effective treatment for relieving airway obstruction and displays a better safety profile with respect to theophylline 250 mg t.i.d. with a favorable risk-to-benefit ratio.Citation22 More recently, this finding has also been documented in patients with mild bronchial asthma, whereby both theophylline 300 mg twice a day and doxofylline 400 mg twice a day improved lung function and symptoms, but where doxofylline had a better safety profile.Citation45
Another study that enrolled patients suffering from asthma or COPD showed that doxofylline was more effective than theophylline as demonstrated by improvement in pulmonary function tests, as well as clinical symptoms, a reduced incidence of adverse effects and the need for “rescue” bronchodilator use.Citation46 The maximum beneficial effects of doxofylline were observed earlier in patients with asthma than those with COPD.
A trial conducted in patients with COPD presenting to the chest department of a medical college hospital in India showed that doxofylline 400 mg twice a day was as effective as theophylline 400 mg sustained release once a day.Citation47 There was no statistically significant difference with respect to spirometric variables and symptom score in the 2 groups, and there was no significant difference in the 2 groups with respect to side effects.
However, another Indian study conducted in patients of COPD, that compared theophylline and doxofylline at doses recommended and commonly used in clinical practice, showed that both drugs significantly improved spirometric values and symptoms, cough, shortness of breath and nocturnal severity of symptoms.Citation48 The main factor limiting the use of theophylline in this study was the high incidence of side effects, especially gastric distress (33% in theophylline group and 15% in doxofylline group) and CNS stimulation.
A recent study that aimed to estimate the global cost related to the use of doxofylline and theophylline (associated drugs, specialist visits, hospital admissions, plasma drug monitoring), used data extracted from the Information System of the Pharmaceutical Prescriptions of the Marche Region in Italy for each ATC code (R03DA04 and R03DA11,) in the years 2008–2012.Citation41 A total of 13,574 patients were treated with theophylline and 19,426 patients with doxofylline. The number of patients treated was ~5,000 per year. Co-prescription with other drugs, use of corticosteroids, mean number of visits and hospital admissions (per 100 patients) were all lower for doxofylline vs theophylline (1.55 vs 5.50, 0.3 vs 0.7, 2.05 vs 3.73 and 1.57 vs 3.3). The annual mean cost per patient was € 187.4 for those treated with doxofylline and € 513.5 for theophylline. This “real world” finding is really intriguing because the direct cost of doxofylline is higher than that of theophylline and demonstrates the pharmacoeconomic impact doxofylline can have at a population level when used regularly.
Discussion
The analysis of recent literature confirms that doxofylline produces clinical improvements comparable with those induced by theophylline but has a much better safety profile. However, it is now clear that doxofylline also possesses a distinct pharmacological profile from theophylline and therefore, should not be considered as just a modified theophylline (). Indeed, the improvement in the safety profile of doxofylline must be attributed to substantial differences in the pharmacological profile between this drug and theophylline.
Table 1 Comparison between doxofylline and theophylline
Of particular importance is the observation that doxofylline does not have significant drug–drug interactions as exhibited with theophylline and which makes using theophylline more challenging, especially in elderly patients with co-morbidities receiving multiple classes of drug.
There are now a bewildering array of inhaled devices and formulations of drugs available for the treatment of asthma and COPD, which are often associated with poor adherence.Citation49,Citation50 Thus, the use of an orally active drug that is safe, effective and relatively inexpensive is to be encouraged, particularly for patients who find inhalers difficult to use or who do not get adequate control from other pharmacological classes. We would encourage further randomized clinical trials of doxofylline to investigate the use of this drug to reduce exacerbations and hospitalizations due to asthma or COPD as an alternative to expensive biologics, and certainly as an alternative to theophylline.
Disclosure
The authors are consultants at the ABC Farmaceutici (MGM and MC) and Eurodrug (CP) that manufacture and sell medicinal products containing doxofylline. The authors report no other conflicts of interest in this work.
References
- WeinbergerMHendelesLTheophylline in asthmaN Engl J Med199633421138013888614425
- HorakFDobererDEberEDiagnosis and management of asthma – Statement on the 2015 GINA GuidelinesWien Klin Wochenschr201612815–1654155427370268
- VogelmeierCFCrinerGJMartínezFJGlobal strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 report: GOLD executive summaryAm J Respir Crit Care Med2017195555758228128970
- HoritaNMiyazawaNKojimaRInoueMIshigatsuboYKanekoTChronic use of theophylline and mortality in chronic obstructive pulmonary disease: a Meta-analysisArch Bronconeumol201652523323826612542
- SpinaDPageCPXanthines and phosphodiesterase inhibitorsHandb Exp Pharmacol2017237639127844172
- BarnesPJTheophyllineAm J Respir Crit Care Med201318890190623672674
- ItoKLimSCaramoriGA molecular mechanism of action of theophylline: Induction of histone deacetylase activity to decrease inflammatory gene expressionProc Natl Acad Sci U S A2002998921892612070353
- UrnovFDWolffeAPChromatin remodeling and transcriptional activation: the cast (in order of appearance)Oncogene2001202991300611420714
- ChapmanKRLjungholmKKallenALong-term xanthine therapy of asthma. Enprofylline and theophylline comparedChest1994106140714137956392
- BarnesPJTheophylline: new perspectives for an old drugAm J Respir Crit Care Med200316781381812623857
- HaskóGPacherPA2A receptors in inflammation and injury: lessons learned from transgenic animalsJ Leukoc Biol200883344745518160539
- ToYItoKKizawaYTargeting phosphoinositide-3-kinase-delta with theophylline reverses corticosteroid insensitivity in chronic obstructive pulmonary diseaseAm J Respir Crit Care Med201018289790420224070
- FordPADurhamALRussellREGordonFAdcockIMBarnesPJTreatment effects of low dose theophylline combined with an inhaled corticosteroid in COPDChest20101371338134420299628
- PerssonCGDevelopment of safer xanthine drugs for the treatment of obstructive airways diseaseJ Allergy Clin Immunol1986784 Pt 28178243534062
- FozardJRHannonJPAdenosine receptor ligands: potential as therapeutic agents in asthma and COPDPulm Pharmacol Ther199912211111410373392
- AbbracchioMPCattabeniFSelective activity of bamifylline on adenosine A1-receptors in rat brainPharmacol Res Commun19871985375453432321
- Boswell-SmithVPageCPRoflumilast: a phosphodiesterase-4 inhibitor for the treatment of respiratory diseaseExpert Opin Investig Drugs200615911051113
- CalzettaLPageCPSpinaDEffect of the mixed phosphodiesterase 3/4 inhibitor RPL554 on human isolated bronchial smooth muscle toneJ Pharmacol Exp Ther2013346341442323766543
- PageCPDoxofylline: a “novofylline”Pulm Pharmacol Ther201023423123420380886
- van MastbergenJJolasTAllegraLPageCPThe mechanism of action of doxofylline is unrelated to HDAC inhibition, PDE inhibition or adenosine receptor antagonismPulm Pharmacol Ther2012251556122138191
- DiniFLCogoRDoxofylline: a new generation xanthine bronchodilator devoid of major cardiovascular adverse effectsCurr Med Res Opin200116425826811268710
- GoldsteinMFChervinskyPEfficacy and safety of doxofylline compared to theophylline in chronic reversible asthma – a double-blind randomized placebo-controlled multicentre clinical trialMed Sci Monit200284CR297CR30411951074
- FranzoneJSCirilloRBaroneDDoxofylline and theophylline are xanthines with partly different mechanisms of action in animalsDrugs Exp Clin Res19881474794893240706
- CirilloRGrossiEFranzoneJSDoxofylline, an adenosine-nonblocking xanthine, does not induce cardiostimulant effectsRes Commun Chem Pathol Pharmacol198965121342781149
- ZhangYZengKWangJGaoHNanYZhengXIdentifying the antiasthmatic target of doxofylline using immobilized β2-adrenoceptor based high-performance affinity chromatography and site-directed molecular dockingJ Mol Recognit2016291049249827173639
- PatelBSKugelMJBaehringGAmmitAJDoxofylline does not increase formoterol-induced cAMP nor MKP-1 expression in ASM cells resulting in lack of anti-inflammatory effectPulm Pharmacol Ther201745343928414142
- ZhouBCaiSXZouFCaiCQZhaoHJEffect of doxofylline on calcium-activated potassium channels in human peripheral blood eosinophils in asthmaZhonghua Jie He He Hu Xi Za Zhi20052812817819 Chinese16409781
- FranzoneJSCirilloRReboaniMCDoxofylline differs from methylxanthines in its movement of cytosolic calciumInt J Tissue React19911331311381960014
- FranzoneJSCirilloRBiffignandiPDoxofylline exerts a prophylactic effect against bronchoconstriction and pleurisy induced by PAFEur J Pharmacol19891652–32692772776832
- Riffo-VasquezYManFPageCPDoxofylline, a novofylline inhibits lung inflammation induced by lipopolysacharide in the mousePulm Pharmacol Ther201427217017824456641
- CogoRCastronuovoAEffects of oral doxofylline on inflammatory changes and altered cell proliferation in chronic obstructive bronchitisEur Rev Med Pharmacol Sci20004152011409184
- Riffo-VasquezYVenkatasamyRPageCPSteroid sparing effect of doxofyllinePulm Pharmacol Ther20184814
- SugetaAImaiTIdairaSHirokoshiMOkamotoMAdachiMEffects of theophylline and doxofylline on airway responsiveness in dogsArerugi1997461715 Japanese9078607
- CravanzolaCGrosaGFranzoneJSKinetic and metabolic studies of 7-(1,3-dithiolan-2-ylmethyl)−1,3-dimethylxanthine in the ratDrugs Exp Clin Res19901662852912086163
- FranzoneJSCirilloRReboaniMCPharmacological studies in animals of beta-hydroxyethyltheophylline, the major metabolite of doxofylline in humansMethods Find Exp Clin Pharmacol19911342892991652045
- GrossiEFranzoneISFarmacocinetica clinica della doxofillina. [Doxofillin Clinical Pharmacokinetics]Farmaci198812119133 Italian
- BolognaELaganàATerracinoDBolignariPBiffignandiPOral and intravenous pharmacokinetic profiles of doxofylline in patients with chronic bronchitisJ Int Med Res19901842822882227075
- JianGChunyanZZhaolongCYuzhenLErzhangCThe pharmacokinetics of doxofylline in ChineseChin J New Drugs20006396398
- GannuRBandariSSudkeSGRaoYMShankaBPDevelopment and validation of a stability-indicating RP-HPLC method for analysis of doxofylline in human serum. Application of the method to a pharmacokinetic studyActa Chromatographica200719149160
- LeeJHNamgungHWKwonSYYoonHILeeCTThe pharmacokinetic profiles of oral doxofylline and factors influencing the serum level [abstract]Eur Respir J201138Suppl 55350s
- MenniniFSSciattellaPMarcellusiAMarcobelliARussoACaputiAPTreatment plan comparison in acute and chronic respiratory tract diseases: an observational study of doxophylline vs theophyllineExpert Rev Pharmacoecon Outcomes Res201717550351028277853
- ShuklaDChakrabortySSinghSMishraBDoxofylline: a promising methylxanthine derivative for the treatment of asthma and chronic obstructive pulmonary diseaseExpert Opin Pharmacother200910142343235619678793
- LazzaroniMGrossiEBianchi PorroGThe effect of intravenous doxofylline or aminophylline on gastric secretion in duodenal ulcer patientsAliment Pharmacol Therap1990466436492129651
- SaccoCBarthiroliAGrossEDonnerCFThe effects of doxofylline vs theophylline on sleep architecture in COPD patientsMonaldi Arch Chest Dis1995502981037613555
- MargaySMFarhatSKaurSTeliHATo study the efficacy and safety of doxophylline and theophylline in bronchial asthmaJ Clin Diagn Res201594FC05FC08
- LalDManochaSRayAVijayanVKKumarRComparative study of the efficacy and safety of theophylline and doxofylline in patients with bronchial asthma and chronic obstructive pulmonary diseaseJ Basic Clin Physiol Pharmacol201526544345125894641
- AkramMFNasiruddinMAhmadZAli KhanRDoxofylline and theophylline: a comparative clinical studyJ Clin Diagn Res20126101681168423373027
- NagawaramPRKanchanpallyVComparative study of theophylline and doxofylline in the treatment of stable chronic obstructive pulmonary diseaseInt J Basic Clin Pharmacol201652251256
- RoglianiPCalzettaLCoppolaAOptimizing drug delivery in COPD: the role of inhaler devicesRespir Med201712461428284323
- RoglianiPOraJPuxedduEMateraMGCazzolaMAdherence to COPD treatment: Myth and realityRespir Med201712911712328732818