
Abstract
The use of inhaled corticosteroids (ICSs) in long-term treatment of COPD has been a debated topic for a long time. According to the evidence produced till now, ICSs are presently advocated in combination with long-acting bronchodilators for high-risk symptomatic COPD patients with a history of frequent COPD exacerbations. However, the heterogeneity of COPD patients in terms of prevalent underlying disease, with its associated biological and functional characteristics, and different types of exacerbation makes this recommendation highly questionable. This review aims to discuss the usefulness of ICSs in the pharmacological management of COPD and trys to detect those aspects that may likely anticipate a beneficial response following their therapeutic use related to respiratory function, functional decline, prevention of exacerbation, and quality of life. In this respect, the BERN acronym, meaning Bronchiolitis, Eosinophilia, Responsiveness to bronchodilator, and Non-smoker, may be of practical utility to select among COPD patients those that can take more advantage from ICS adoption when positive and vice versa when negative.
Background
Presently, there are widespread, evidence-based, expert recommendations about inhaled corticosteroid (ICS) use in patients suffering from COPD suggesting their adoption in the chronic treatment of COPD combined with long-acting bronchodilators when in symptomatic patients pulmonary function is halved (ie, postbronchodilator FEV1 <50%–60% predicted) and/or frequency of COPD-related acute exacerbations (AECOPDs) is two or more episodes per year or in the presence of at least one severe AECOPD per year in the previous year/s.Citation1 These recommendations stem from evidence that has been produced from randomized controlled trials (RCTs) where recruitment of large cohorts of patients had simply required an age >40 years, smoking history >10 pack/years, and FEV1/FVC ratio <70% after acute administration of bronchodilators and no self-reported asthma.
Apart from three historical RCTs looking at annual FEV1 decline rates in COPD patients suffering from moderate airflow obstruction treated with ICSs alone,Citation2–Citation4 all COPD patients enrolled in more recent RCTs have had moderate–severe airflow obstruction (usually with mean postbronchodilator FEV1 around 50% of predicted), and for AECOPD reduction as outcome, a history of one or rarely two or more AECOPDs reported in the previous year.Citation5–Citation8
Within this framework (for the last 20 years), ICSs alone or more often in combination with bronchodilators (long-acting β2 agonists [LABAs]) compared to placebo or bronchodilators (LABAs) did not significantly reduce overall mortality or appreciably the mean FEV1-decline rate, but were able to give some improvement in lung function, sometimes associated with lesser symptoms and greater exercise tolerance, better quality of life, and a reduction in AECOPDs of 25%–40% vs placebo and almost invariably of about 20%–30% vs LABAs.Citation9 Considering the well-recognized heterogeneity of COPD patients, going from the underlying prevalent disease (ie, fibrosing chronic bronchiolitis alone versus fibrosing chronic bronchiolitis plus centrilobular emphysema, from mild to advanced, versus panlobular emphysema), to the different nature of AECOPDs (eg, from infective to eosinophilic, pauci-inflammatory, comorbidity-related), the aforementioned evidence appears limited and coarse.Citation10
In the era of targeted or even personalized therapy, it seems really illogical in COPD to deny ICSs (if useful) until 50% of lung function has been lost, or in contrast, to advocate ICSs in the presence of frequent, but noneosinophilic AECOPDs, trying to prevent them. This may lead to the confusion that is only going to increase among general practitioners and specialists, leading to the opposite result, ie, to give the same treatment to everybody.Citation11 The future challenge in order to build helpful evidence is to find useful and practical biomarkers (clinical, functional, biological, radiological, omic) to select COPD patients accurately who deserve ICSs in combination with one or two bronchodilators. Until then, it might be interesting for the reader to take in current knowledge about ICSs in COPD in terms of why, what, who, and when.
Why
The relatively few data we have about the activity of ICSs in COPD patients from bronchial biopsies, induced sputum, or bronchoalveolar lavage (BAL) — biological windows of proximal, large, or small airways, respectively — have demonstrated many anti-inflammatory and immunomodulatory effects. In a meta-analysis published in 2012, four studies using bronchial biopsies (n=102 participants with COPD) showed a significant reduction in CD4+ and CD8+ lymphocyte counts with no effect in neutrophils in bronchial walls, and in five studies using BAL (n=309 participants with COPD) a significant reduction in both lymphocyte and neutrophil counts at the epithelial surface of more peripheral airways with ICSs vs placebo.Citation12
Although these findings may be influenced by the current smoking status of patients and concomitant use of other drugs, such as bronchodilators and theophylline, they firmly suggest that ICSs essentially downregulate lymphocytic inflammation and adaptive immunity that become predominant in the later stages of COPD. In addition, ICS or oral CS use has been associated with lower occurrence of lymphoid follicles in small airways, which tends to increase with progression of airflow obstruction: <5% in GOLD stages 1 and 2, and >30% in GOLD stages 3 and 4.Citation13
Data on eosinophils for both bronchial biopsies and BAL were controversial and overall not significant using ICSs vs placebo.Citation12 Another meta-analysis on six studies looking at the effects of ICSs on inflammatory cells in induced sputum (n=162 participants with COPD) showed a reduction in lymphocyte and neutrophil counts, with on average no change in eosinophils.Citation13 The conflicting and surprising data about the ICS effect on eosinophils, with both positive and negative results in COPD, could be related to the unselected recruitment of the patients. We know that only a third of COPD patients have a persistent and relevant eosinophilic airway inflammation, as documented by induced sputum and BAL, and likely only these COPD patients may respond to ICSs treatment in terms of eosinophil reduction and related benefit.Citation14,Citation15 In fact, in subgroups of stable COPD patients with high eosinophilic counts in sputum, the adoption of ICSs on top of bronchodilators has produced greater functional improvement in terms of FEV1 increase and better quality of life in terms of St George's Respiratory Questionnaire score reduction than other subgroups of COPD patients with lower eosinophilic counts in the sputum.Citation16 The same results were observed in nonsmoking COPD patients with high levels of exhaled FeNO, which are usually associated with eosinophilic airway inflammation.Citation17
It is important to say that such immunomodulatory and anti-inflammatory effects after long-term treatment with ICSs appear significant compared with placebo in sputum, BAL, and bronchial biopsies, mostly in nonsmoking (never-smokers or ex-smokers) than in smoking COPD patients.Citation18 Oxidative and nitrative stress in COPD patients is high, and in those who smoke it is higher than in nonsmoking COPD patients. Although a bit controversial, it is believed that because of the oxidative/nitrative-induced HDAC2 inactivation in smoking COPD patients, ICSs cannot exert their genomic actions.Citation19 This may explain the so-called ICS resistance of COPD-related inflammation, which can be partly reversed by stopping smoking or avoiding the HDAC2 inactivation through antioxidant drugs and low-dose theophylline and experimentally by PI3Kδ inhibitors. In any case, current smoking greatly reduces the aforementioned biological effects of ICSs.
Interestingly, in a small cohort of moderate–severe COPD patients (n=32 participants), long-term treatment with ICSs induced partial changes in extracellular matrix composition of the bronchial wall by increasing both proteoglycans and collagen I and III deposition (versican and collagen III significantly vs placebo). These modifications might reduce the compliance of the bronchial walls by modulating airway remodeling and increase lung function by preventing small-airway collapse.Citation20 All these effects can offer a biological explanation for the favorable response to ICSs observed in some subgroups of COPD patients, where ICSs together with bronchodilators might actually represent a disease-modifying drug, able to control a relevant part of underlying inflammation and its consequences: symptoms, mechanical impairment, functional decline, a number of AECOPDs, quality of life, and perhaps all-cause mortality.Citation21
What
Chronic Bronchiolitis Versus Pulmonary Emphysema
Small-airway inflammation and remodeling with progressive peribronchiolar fibrosis, namely fibrosing chronic bronchiolitis, represents the most common disease underlying COPD, because of the extensive small-airway resistance increase. In contrast, few COPD patients suffer from panlobular emphysema as the initial underlying cause of chronic airflow reduction. With natural progression of small-airway disease involving the respiratory intra-acinar bronchioli, very often the associate development of another form of emphysema starting from the center of secondary lobule, so-called centrilobular emphysema, is observed that can progress from mild to moderate, confluent, and finally advanced form, according to the extent of diseased lung.Citation22
In mild–moderate COPD (GOLD stages 1 and 2), air trapping in the diseased lung is almost entirely due to chronic bronchiolitis, while in more severe COPD (GOLD stages 3 and 4) this is largely caused by associated centrilobular emphysema that progressively increases, as elegantly shown by parametric response–mapping computed tomography (CT)-scan studies.Citation23 That means that abnormal lung inflation in the early phase of COPD is essentially “functional” (disappearing at full inspiration) due to the decreased caliber of small airways, while in the latter COPD is also “anatomical” (remaining at full inspiration), because of irreversible destruction of alveolar septa. Therefore, the main determinants of airflow obstruction change from increased small-airway resistance to expiratory small-airway collapse and loss of elastic recoil with progression of COPD severity.
It is logical that the anti-inflammatory and immunomodulatory effects of ICSs in combination with bronchodilators are most useful when the prevalent underlying disease is still chronic bronchiolitis (mild–moderate COPD) in the attempt to control and avoid the harmful consequences of adaptive immunity on airway remodeling and peribronchiolar alveolar septa damage subsequent to the recruitment and activation of CD4+ and mainly CD8+ lymphocytes. In contrast, when the prevalent disease has become centrilobular emphysema, especially if confluent or advanced (severe–very severe COPD), antiapoptotic activity on neutrophils of ICSsCitation24 should represent a contraindication to their use, due to the risk of further progression of alveolar septa digestion by the uncontrolled protease burden typically associated with this type of inflammation. This has been proved by the GLUCOLD study, an RCT with a 30-month follow-up performed in a cohort of 114 COPD patients (64 current smokers) with no history or diagnosis of asthma, which aimed to assess the pathological and clinical efficacy (and their link) of long-term treatment with ICSs. These patients were characterized by moderate airflow obstruction (mean FEV1=56% predicted), but with almost normal lung diffusion capacity (mean KCO =73% predicted), presence of airway hype-responsiveness, and some degree of bronchial responsiveness (mean ∆FEV1 =7% of predicted postbronchodilator).
In the arms treated with fluticasone alone or in combination with salmeterol, the mean FEV1-decline after 2.5 years was +7 mL/year and -16 mL/year, respectively, vs -79 mL/year for the placebo arm (p<0.001).Citation25 These findings clearly show that in COPD patients affected substantially by chronic bronchiolitis, ICSs can attenuate or even stop their functional decline in association with a decrease in airway inflammation, as documented by the reduction in inflammatory cell counts (CD4+ and CD8+ lymphocytes and mast cells) on bronchial biopsies at 6 and 30 months. A subanalysis of this study aimed to identify predictors of best response to ICSs in terms of FEV1 decline after 30 months compared to placebo, found that COPD patients who initially had higher DLCO (>65% predicted), lower air trapping (residual volume/total lung capacity ratio <42%), lower sputum inflammatory-cell total count (<169×10/mL cell), and fewer pack-years (<42) exhibited attenuated or no functional loss if actively treated.Citation26 In other words, COPD patients benefit much more from long-term treatment with ICSs if they have less severe airway inflammation, no or mild emphysema, lower pulmonary hyperinflation, and lower smoking history.
In addition, an insightful prospective observational study performed in >200 Japanese COPD patients (Hokkaido COPD cohort study) aged 69 years on average who were treated with usual therapy, including ICSs, and followed for 5 years showed unequivocally that in those with chronic bronchiolitis with or without mild associated emphysema (indicated by the normal or nearly normal CT-scan lung densitometry and mean KCO > 70% predicted), no change in FEV1 was observed (no decliners). In contrast, those with a substantial presence of pulmonary emphysema on CT-scan quantitative analysis and lowest KCO (<60% predicted) had a markedly abnormal FEV1-decline rate, irrespective of any treatment (fast decliners). In those patients with an intermediate extent of pulmonary emphysema and KCO values, the rate of FEV1 decline was similar or slightly greater than what is expected in normal controls of the same age range (slow decliners).Citation27
Chronic Eosinophilic Bronchiolitis
Many studies have shown that in COPD patients (about 20%–35%) with no history or diagnosis of asthma, persistent eosinophilic inflammation is found in sputum with eosinophilic values ≥3% of total inflammatory cell numbers.Citation28,Citation29 In the bronchial and bronchiolar epithelial cells of these COPD patients, increased upregulation and expression of proinflammatory gene–driven type 2 inflammation has been found in response to noxious stimuli, associated with significant better respiratory functional response to ICSs vs placebo.Citation30–Citation32 It is highly plausible that these COPD patients may frequently have AECOPDs with raised levels of eosinophils in sputum (>2%) and in bloodCitation33 that respond better to systemic corticosteroids without need of antibioticsCitation34 and can be more effectively prevented by long-term treatment with ICSs combined with bronchodilators.
A post hoc analysis of several trials and recent data of prospective RCTs aimed to assess the ability of treatment with ICSs in combination with ultra-LABAs and ultra-LABAs + ultra-long-acting muscarinic antagonists to prevent AECOPDs in COPD patients with frequent exacerbations showed that the presence of ICSs decreased the annual rate of AECOPDs in terms of initial percentage or absolute number of eosinophils in blood measured in stable conditions, with a clear dose–response curve:Citation35–Citation41 no effect below 2% or 100–150 elements per 100 μL of blood, and much greater effect above 4% or 300–350 elements per 100 μL of blood.Citation42
Presently, high eosinophil counts in the blood of stable COPD patients who frequently exacerbate is considered a biomarker of positive response to ICSs in preventing AECOPDs (likely eosinophilic),Citation43 with a cut off of 300–350 elements per 100 μL of blood that is less sensitive, but markedly more specific, with highest positive predictive power.Citation44 In addition, a recent post hoc analysis of data collected in the ISOLDE trial where COPD patients (mean FEV1 50% predicted) were randomly treated with ICSs alone or placebo to assess ICS effect on lung-function decline during a 3-year follow-up, showing no effect of active treatment in the overall COPD population, has provided very interesting results. After division of the patients according to initial percentage of blood eosinophils, compared to placebo subgroups those with >2% blood eosinophils did not show any postbronchodilator FEV1 decline during follow-up. In contrast, no effect, with a similar rate of FEV1 decline observed with placebo, was found in those with <2% blood eosinophils.Citation45 Within the limits of a post hoc analysis and the choice of a 2% cutoff, these findings strongly suggest that ICS treatment in stable COPD patients with blood eosinophilia may significantly attenuate or even stabilize their functional decline rate, even in those with moderate–severe airflow obstruction.
Bronchial Responsiveness
Although by definition, no COPD patients displays complete reversibility of airflow obstruction after bronchodilator inhalation (acute or chronic), some (about 12%) exhibit consistent and significant bronchodilator responsiveness (partial reversibility) to acute administration of an inhaled short-acting bronchodilator (salbutamol).Citation46 An increment in postbronchodilator FEV1 ≥12% from baseline with at least 200 mL absolute change defines this functional characteristic, which has been shown to be related to higher eosinophil count in induced sputum and elevated FeNO consistent with airway eosinophilic inflammation.Citation47 Therefore, the presence of significant bronchial responsiveness, suggesting a more likely eosinophilic airway inflammationCitation15 and also higher eosinophilic blood count,Citation48 may be considered a favorable predictor of ICS treatment.Citation49
It must be recognized that a positive response to bronchodilators may be a mere consequence of FVC increase, with no change or even decrease in FEV1/FVC ratio. This feature identifies COPD patients, so-called volume responders, who are more frequently observed in GOLD stages 3 and 4.Citation50 In contrast, a similar significant FEV1 increase after acute inhalation of short-acting bronchodilators may occur with an increase in FEV1/FVC ratio. This feature identifies COPD patients, so called flow responders, who are mostly found in GOLD stage 2, a milder stage of airflow obstruction where chronic bronchiolitis is the predominant disease underlying COPD.Citation46
Prevention of Acute Exacerbations of COPD
Several studies in the last few years have focused on reduction of AECOPDs as a primary outcome of pharmacological treatments in COPD patients with a history of frequent COPD exacerbations.Citation7,Citation8,Citation35–Citation41 About 35%–40% of COPD patients suffer from two or more AECOPDs or have a severe AECOPD leading to hospitalization each year.Citation51 Knowing independent risk factors for AECOPDsCitation51 and mainly the relevant negative role of frequent AECOPDs in the natural history of COPD,Citation52 effective prevention of these episodes of rapidly increased airway inflammation with a background of airway chronic inflammation has become a mandatory goal of treatment (pharmacological and nonpharmacological) in these COPD patients.Citation9,Citation53,Citation54
It must be realized, however, that AECOPDs have different etiology, essentially infectious (viral, or bacterial, or both) and uninfectious.Citation9,Citation33,Citation55 Among those uninfectious, a number have sustained increased eosinophilic inflammation in the airways, as confirmed by sputum cytological analysis and reflected by peripheral blood eosinophilia, so-called eosinophilic AECOPDs.Citation33 Other AECOPDs, among those uninfectious and noneosinophilic, have several different causes that need to be identified from time to time.Citation9,Citation55
In each COPD patient who exhibits frequent exacerbations, a prevalent AECOPD phenotype seems involved,Citation56 which should be recognized and prevented accordingly, in order to reduce the overall AECOPD number, eg, by about 70%–80% and not about 20%–30%, as generally obtained in RCTs where every type of AECOPD is counted and the treatment to prevent them is the same. These stereotyped RCTs have also been done with ICSs, usually combined with long-acting or ultralong-acting bronchodilators.
Actually, is becoming clearly evident that ICSs are highly effective in preventing eosinophilic AECOPDs, which are the most prevalent phenotype in COPD patients suffering from chronic eosinophilic bronchiolitis, as already mentioned.Citation35–Citation41 In contrast, ICSs could be useless or even noxious if chronically administered to prevent infectious AECOPDs or uninfectious and noneosinophilic AECOPDs if such phenotypes are mostly involved. In these cases, the risk of pneumonia may become unjustifiably elevated.Citation57 Therefore, in combination with bronchodilators, ICSs should be advised to prevent acute COPD exacerbations, essentially in COPD patients who have frequent eosinophilic AECOPDs, and not extensively in all COPD patients who have frequent AECOPDs.Citation58 Treatments other than ICSs have to be implemented in baseline pharmacological therapy to reduce the risk of noneosinophilic AECOPDs in frequent exacerbators.Citation9,Citation53,Citation59
Asthma–COPD Overlap
Although asthma and fibrosing chronic bronchiolitis and/or pulmonary emphysema (asthma-COPD overlap [ACO]) rarely coexist in the same individual, this may occur and depicts an unfavorable clinical condition in terms of symptoms, acute exacerbations, quality of life, and use of rescue drugs.Citation60 In this context, the main difficulty remains the accurate identification of these patients, which is generally based on the presence of some anamnestic, clinical, functional, and possibly radiological features of both asthma and COPD,Citation61 namely subjects with a history of asthma and respiratory symptoms before age 40 years, presence of atopy and allergies, airflow obstruction not fully reversible, but with high responsiveness to bronchodilators, together with a relevant smoking history, and sometimes radiological aspects of pulmonary emphysema with reduced KCO.Citation60,Citation61 Despite the lack of specific interventional RCTs in patients with ACO, it is widely thought that ACO, especially when the underlying inflammatory endotype is eosinophilic, represents a strong indication for ICS treatment combined with long-acting bronchodilators,Citation62 in view of favorable effects on hospitalization and death as compared to LABAs alone, irrespective of lung-function impairment.Citation63
Who
Based on the aforementioned observations, the profile of COPD patients who deserve ICSs emerges definitively, and has been previously outlined by the presence of predictors of a positive response.Citation49 Briefly, ICSs combined with bronchodilators are indicated as a disease-modifying drug to treat COPD patients: 1) who are suffering from chronic bronchiolitis as isolated or prevalent underlying disease (associated with mild–moderate centrilobular emphysema) (B); 2) who in stable condition have an airway eosinophilic inflammation demonstrated by induced sputum and can be associated with persistent (and otherwise unexplained) blood eosinophilia (>300–350 elements/μL) (E), and (if exacerbators) have prevalent eosinophilic exacerbations 3) who consistently show significant bronchial responsiveness after acute bronchodilators (∆FEV1 >12% from baseline with >200 mL increment), but with an increase in FEV1/FVC ratio (so-called flow responders) (R); and 4) who are nonsmokers (ie, ex-smokers or never-smokers) (N). These COPD patients can be identified as BERN-positive (3 or 4 out of 4 criteria). In addition, the same is indicated for those COPD patients who have ACO.
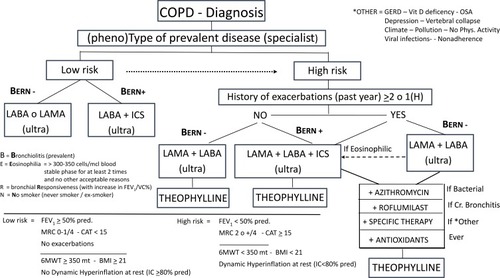
In contrast, ICSs should do not be offered to COPD patients: 1) who suffer from panlobular emphysema or have developed confluent or advanced centrilobular emphysema as prevalent disease, respectively; 2) who do not have consistent eosinophilic inflammation in small airways or (if exacerbators) do not have eosinophilic exacerbations, but other causes of AECOPDs; 3) who do not respond to acute bronchodilators or show significant bronchial responsiveness, but with no change or decrease in FEV1/FVC ratio (so-called volume-responders); and 4) who continue to smoke. These COPD patients can be identified as BERN-negative (3 or 4 out of 4 criteria). They should be treated only with one or two bronchodilators and specific measures to prevent AECOPDs if exacerbators, according to the prevalent cause of their AECOPDs ().
Figure 1 Targeted pharmacological treatment in COPD.
When
In COPD patients who deserve ICSs because of the presence of the aforementioned characteristics (BERN+), ICSs on top of one or two bronchodilators should be offered as soon as possible, independently of severity of symptoms, degree of airflow reduction, and presence of AECOPDs. In COPD patients who do not have these characteristics (BERN–), ICSs should never be recommended.
Safety
The adverse effects of chronic ICS administration have been recognized for a long time and are a function of daily dose, being more common when higher dosage is assumed (ie, ≥1,000 μg fluticasone propionate equivalent per day). Although to a less extent than with systemic CSs, the risk of developing or worsening diabetes, cataracts, osteoporosis, adrenal insufficiency, active tuberculosis, skin bruises, and electrolyte imbalance is significantly increased in COPD patients consuming ICSs, especially at high doses.Citation49
In contrast with asthmatics, however, COPD patients treated with ICSs have shown an increased risk of pneumonia compared with those who do not consume ICSs.Citation64 Although the risk of pneumonia seems mainly related to age, severity of airflow obstruction, history of AECOPDs, and comorbidities of COPD patients treated with ICSsCitation6,Citation65 than ICS treatment per se, after adjusting for these variables some significant residual risk persists that is a function of the duration and daily dose of ICSs consumed.Citation66 The size of the increased risk, the frequency of events, and the related excess mortality make pneumonia the most dangerous side effect in COPD patients treated with ICSs.Citation57
Although the effect on AECOPD reduction has been much greater than the occurrence of pneumonia in previous RCTs, this does not justify the use of high doses of ICSs in treatment of COPD.Citation49 In fact, in studies where moderate doses of ICSs combined with bronchodilators have been used, the percentage of pneumonia was lowerCitation67,Citation68 or not different from the arm treated only with bronchodilators.Citation69,Citation70 Notably, if ICSs are prescribed in COPD patients with high levels of blood eosinophilia to prevent AECOPDs (essentially eosinophilic), the risk of ICS-related pneumonia is reduced or even zero.Citation35 In summary, the risk of adverse effects of ICS treatment requires accurate selection of subgroups of COPD patients who warrant it and suggests the avoidance of high-dose ICSs in chronic therapy of these patients, with the only possible exception being patients with ACO.
Conclusion
Is clearly evident that the heterogeneity of patients affected by COPD should necessitate different treatment strategies. In this respect, the decision to adopt ICSs in combination with bronchodilators for chronic background therapy is crucial and has to be made at the beginning. The use of the simple BERN acronym (positive or negative) might be helpful in settling this choice. The usefulness of ICSs in the prevention of AECOPDs appears substantially limited to those eosinophilics that again belong to COPD patients who are BERN+.
Disclosure
The authors report no conflicts of interest in this work.
References
- Global Initiative for Chronic Obstructive Lung Disease. Progetto Mondiale BPCO Strategia Globale Per La Diagnosi, Il Trattamento E La Prevenzione Della Broncopneumopatia Cronica Ostruttiva; Aggiornamento 2016 [World COPD Project Global Strategy For Diagnosis, Treatment And Prevention Of Chronic Obstructive Pulmonary Disease; Update 2016]. Available from: http://goldcopd.it/wp-content/uploads/materiali/2016/GOLD_workshop_report_2016.pdf. Accessed 53, 2017 Italian.
- VestboJ, SorensenT, LangeP, BrixA, TorreP, ViskumK. Long-term effect of inhaled budesonide in mild and moderate chronic obstructive pulmonary disease: a randomized controlled trial. Lancet. 1999;353:1819–1823. doi:10.1016/S0140-6736(98)10019-310359405
- PauwelsRA, LofdhalGG, LaitinenLA, et al. Long term treatment with inhaled budesonide in persons with mild chronic obstructive pulmonary disease who continue smoking. European Respiratory Society study on chronic obstructive pulmonary disease. N Engl J Med. 1999;340:1948–1953. doi:10.1056/NEJM19990624340250310379018
- The Lung Health Study Research Group. Effect of inhaled triamcinolone on the decline in pulmonary function in chronic obstructive pulmonary disease. N Engl J Med. 2000;343:1902–1909. doi:10.1056/NEJM20001228343260111136260
- CarlverleyPMA, PauwelsRA, VestboJ, et al. Combined salmeterol and fluticasone in the treatment of chronic obstructive pulmonary disease: a randomized controlled trial. Lancet. 2003;361:449–453. doi:10.1016/S0140-6736(03)12459-212583942
- CalverleyPMA, AndersonJA, CelliB, et al. Salmeterol and fluticasone propionate and survival in chronic obstructive pulmonary disease. N Engl J Med. 2007;356:775–789. doi:10.1056/NEJMoa06307017314337
- KardosP, WenkerM, GlaabT, VolgelmeierC. Impact of salmeterol/fluticasone propionate versus salmeterol on exacerbation in severe chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2007;175:144–149. doi:10.1164/rccm.200602-244OC17053207
- WedzichaJA, CalverleyPMA, SeemungalTA, et al. The prevention of chronic obstructive pulmonary disease exacerbations by salmeterol/fluticasone propionate or tiotropium bromide. Am J Respir Crit Care Med. 2008;177:19–26. doi:10.1164/rccm.200707-973OC17916806
- TantucciC, PiniL. COPD it is time to change! Int J Chron Obstruct Pulmon Dis. 2015;10:2451–2457. doi:10.2147/COPD.S8769626648707
- BrusselleG, PriceD, Gruffydd-JonesK, et al. The inevitable drift to triple therapy in COPD: an analysis of prescribing pattern in the UK. Int J Chron Obstruct Pulmon Dis. 2015;10:2207–2217. doi:10.2147/COPD.S9169426527869
- JenR, RennardSI, SinDD. Effects of inhaled corticosteroids on airway inflammation in chronic obstructive pulmonary disease: a systematic review and meta-analysis. Int J Chron Obstruct Pulmon Dis. 2012;7:587–595. doi:10.2147/COPD.S3276523055709
- HoggJC, ChuFS, UtokaparchS, et al. The nature of small airway obstruction in chronic obstructive pulmonary disease. N Engl J Med. 2004;350:2645–2653. doi:10.1056/NEJMoa03215815215480
- GanWQ, ManSF, SinDD. Effects of inhaled corticosteroids on sputum cell counts in stable chronic obstructive pulmonary disease: a systematic review and a meta-analysis. BMC Pulm Med. 2005;5:3. doi:10.1186/1471-2466-5-315707484
- BalzanoG, StefanelliF, IorioC, et al. Eosinophilic inflammation in stable chronic obstructive pulmonary disease. Relationship with neutrophils and airway function. Am J Respir Crit Care Med. 1999;160:1486–1492. doi:10.1164/ajrccm.160.5.981010510556110
- PerngDW, HuangHY, ChenHM, LeeYC, PerngRP. Characteristic of airway inflammation and bronchodilator reversibility in COPD: a potential guide to treatment. Chest. 2004;126:375–381. doi:10.1378/chest.126.2.37515302720
- BrightilngCE, McKennaS, HargadonB, et al. Sputum eosinophilia and the short term response to inhaled mometasone in chronic obstructive pulmonary disease. Thorax. 2005;60:193–198. doi:10.1136/thx.2004.03251615741434
- DummerJF, EptonMJ, CowanJO, et al. Predicting corticosteroids response in chronic obstructive pulmonary disease using exhaled nitic oxide. Am J Respir Crit Care Med. 2009;180:846–852. doi:10.1164/rccm.200905-0685OC19661244
- HoonhorstSJM, Ten HackenNHT, VonkJM, et al. Steroid resistance in COPD? Overlap and differential anti-inflammatory effects in smokers and ex-smokers. PLoS One. 2014;9(2):e87443. doi:10.1371/journal.pone.008744324505290
- BarnesPJ, AdcockIM, ItoK. Histone acetylation and deacetylation: importance in inflammatory lung diseases. Eur Respir J. 2005;25:552–563. doi:10.1183/09031936.05.0011750415738302
- KunzLIZ, StrebusJ, BudulacSE, et al. Inhaled steroids modulate extracellular matrix composition in bronchial biopsies of COPD patients: a randomized, controlled trial. PLoS One. 2013;8(5):e63430. doi:10.1371/journal.pone.006343023667615
- GlaabT, TaubeC. Effects of inhaled corticosteroids in stable chronic obstructive pulmonary disease. Pulm Pharmacol Ther. 2011;24:15–22. doi:10.1016/j.pupt.2010.08.00620816832
- LynchDA, AustinJH, HoggJC, et al. CT-definable subtypes of chronic obstructive pulmonary disease: a statement of Fleischner Society. Radiology. 2015;277:192–205. doi:10.1148/radiol.201514157925961632
- BhattSP, SolerX, WangS, et al. Association between functional small airway disease and FEV1 decline in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2016;194:178–184. doi:10.1164/rccm.201511-2219OC26808615
- ZhangX, MoilanenE, KankaanrantaH. Beclomethasone, budesonide and fluticasone propionate inhibit human neutrophil apoptosis. Eur J Pharmacol. 2001;431:365–371.11730731
- LapperreTS, Snoeck-StrobandJB, GosmanMME, et al. Effect of fluticasone with and without salmeterol on pulmonary outcomes in chronic obstructive pulmonary disease. Ann Intern Med. 2009;151:517–527. doi:10.7326/0003-4819-151-8-200910200-0000419841453
- Snoeck-StrobandJB, LaperreTS, SterkPJ, et al. Prediction of long-term benefits of inhaled steroids by phenotypic markers in moderate-to-severe COPD: a randomized controlled trial. PLoS One. 2015;10(12):e0143793. doi:10.1371/journal.pone.014379326659582
- NishimuraM, MakitaH, NagaiK, et al. Annual change in pulmonary function and clinical phenotype in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2012;185:44–52. doi:10.1164/rccm.201106-0992OC22016444
- PizzichiniE, PizzichiniMMM, GibsonP, et al. Sputum eosinophilia predicts benefit from prednisone in smokers with chronic obstructive bronchitis. Am J Respir Crit Care Med. 1998;158:1511–1517. doi:10.1164/ajrccm.158.5.98040289817701
- LeighR, PizzichiniMMM, MorrisMM, MaltaisF, HargreaveFE, PizzichiniE. Stabel COPD: predicting benefit from high-dose of inhaled corticosteroid treatment. Eur Respir J. 2006;27:964–971. doi:10.1183/09031936.06.0007210516446316
- SteilingK, van den BergeM, HijaziK, et al. A dynamic bronchial airway gene expression signature of chronic obstructive pulmonary disease and lung function impairment. Am J Respir Crit Care Med. 2013;187:933–942. doi:10.1164/rccm.201208-1449OC23471465
- van den BergeM, SteilingK, TimensW, et al. Airway gene expression in COPD is dynamic with inhaled corticosteroid treatment and reflects biological pathways associated with disease activity. Thorax. 2014;69:14–23. doi:10.1136/thoraxjnl-2012-20287823925644
- ChristensonSA, SteilingK, van den BergeM, et al. Asthma-COPD overlap. Clinical relevance of genomic signatures of type-2 inflammation in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2015;191.
- BafadhelM, McKennaS, TerryS, et al. Acute exacerbations of chronic obstructive pulmonary disease. Identification of biologic clusters and their biomarkers. Am J Respir Crit Care Med. 2011;184:662–671. doi:10.1164/rccm.201104-0597OC21680942
- BafadhelM, McKennaS, TerryS, et al. Blood eosinophils to direct corticosteroid treatment of exacerbations of chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2012;186:48–55. doi:10.1164/rccm.201108-1553OC22447964
- PascoeS, LocantoreN, DransfieldMT, BarnesNC, PavordID. Blood eosinophil count, exacerbations and response to the addition of inhaled fluticasone furoate to vilanterol in patients with chronic obstructive pulmonary disease: a secondary analysis of data from two parallel randomized controlled trials. Lancet Resp Med. 2015;435–442. doi:10.1016/S2213-2600(15)00106-X
- SiddiquiSH, GuasconiA, VestboJ, et al. Blood eosinophils: a biomarker of response to extrafine beclomethasone/formoterol in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2015;192:523–526. doi:10.1164/rccm.201502-0235LE26051430
- WedzichaJA, PriceD, Karen MezziK, FogelR, BanerjiD. Indacaterol plus Glypirronium compared with salmeterol/fluticasone on exacerbations and its correlation with baseline blood eosinophils: a pooled analysis of Lantern and Illuminate. Eur Respir J. 2015;46.
- FergusonGT, RabeKF, MartinezFJ, et al. Triple therapy with budesonide/glycopyrrolate/formoterol fumarate with co-suspension delivery technology versus dual therapies in chronic obstructive pulmonary disease (KRONOS): a double-blind, parallel-group, multicentre, Phase 3 randomised controlled trial. Lancet Resp Med. 2018;6:747–758.
- WatzH, TetzlaffK, WoutersEF, et al. Blood eosinophil count and exacerbations in severe chronic obstructive pulmonary disease after withdrawal of inhaled c orticosteroids: a post-hoc analysis of the WISDOM trial. Lancet Resp Med. 2016;4:390–398. doi:10.1016/S2213-2600(16)00100-4
- BafadhelM, PetersonS, De BlasMA, et al. Predictors of exacerbation risk and response to budesonide in patients with chronic obstructive pulmonary disease: a post-hoc analysis of three randomised trials. Lancet Respir Med. 2018;6:117–126. doi:10.1016/S2213-2600(18)30006-729331313
- LipsonDA, BarnhartF, BrealeyN, et al. Once-daily single-inhaler triple versus dual therapy in patients with COPD. New Engl J Med. 2018;378:1671–1680. doi:10.1056/NEJMoa171390129668352
- SuissaS, Dell’AnielloS, ErnstP. Comparative effectiveness of LABA-ICS versus LAMA as initial treatment in COPD targeted by blood eosinophils: a population-based cohort study. Lancet Resp Med. 2018;6:855–862. doi:10.1016/S2213-2600(18)30368-0
- BrusselleGG, BrackeK, LahousseL. Targeted therapy with inhaled corticosteroids in COPD according to blood eosinophil counts. Lancet Resp Med. 2015;3:416–417. doi:10.1016/S2213-2600(15)00145-9
- NegewoNA, McDonaldVM, BainesKJ, et al. Peripheral blood eosinophils: a surrogate marker for airway eosinophilia in stable COPD. Int J Chron Obstruct Pulmon Dis. 2016;11:1495.27445469
- BarnesNC, SharmaR, LettisS, CalverleyPMA. Blood eosinophils as a marker of response to inhaled corticosteroids in COPD. Eur Respir J. 2016;47:1374–1382. doi:10.1183/13993003.01370-201526917606
- AlbertP, AgustiA, EdwardsL, et al. Bronchodilator responsiveness as a phenotypic characteristic of established chronic obstructive pulmonary disease. Thorax. 2012;67:701–708. doi:10.1136/thoraxjnl-2011-20145822696176
- PapiA, RomagnoliM, BaraldoS, et al. Partial reversibility of airflow limitation and increased exhaled NO and sputum eosinophilia in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2000;162:1773–1777. doi:10.1164/ajrccm.162.5.991011211069811
- SitkauskieneB, SakalaukasR, MalakauskasK, LotvallJ. Reversibility to a beta-2-agonist in COPD: relationship to atopy and neutrophil activation. Resp Med. 2003;97:591–598. doi:10.1053/rmed.2003.1485
- ErnstP, SaadN, SuissaS. Inhaled corticosteroids in COPD: the clinical evidence. Eur Respir J. 2015;45:525–537. doi:10.1183/09031936.0012891425537556
- CerveriI, PellegrinoR, DoreR, et al. Mechanisms for isolated volume response to bronchodilator in patients with COPD. J Appl Physiol. 2000;88:1989–1995. doi:10.1152/jappl.2000.88.6.198910846010
- HurstJR, VestboJ, AnzuetoA, et al. Susceptibility to exacerbation in chronic obstructive pulmonary disease. N Engl J Med. 2010;363:1128–1138. doi:10.1056/NEJMoa090988320843247
- Soler-CatalunaJJ, Martìnez-GarcìaMA, Romàn SanchezP, SalcedoE, NavarroM, OchandoR. Severe acute exacerbations and mortality in patients with chronic obstructive pulmonary disease. Thorax. 2005;60:925–931. doi:10.1136/thx.2005.04052716055622
- PavordID, JonesPW, BurgelP-R, RabeKF. Exacerbation of COPD. Int J Chron Obstruct Pulmon Dis. 2016;11:21–30. doi:10.2147/COPD.S8597826937187
- WedzichaJA, MiravittlesM, HurstJR, et al. Management of COPD exacerbation: a European Respiratory Society/american Thoracic Society guideline. Eur Respir J. 2017;49:1600791. doi:10.1183/13993003.00791-201628298398
- ZhouA, ZhouZ, ZhaoY, ChenP. The recent advances of phenotypes in acute exacerbations of COPD. Int J Chron Obstruct Pulmon Dis. 2017;12:1009–1018. doi:10.2147/COPD.S12860428392685
- HurstJR. Exacerbation phenotyping in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2011;184:625–626. doi:10.1164/rccm.201106-1136ED21920921
- SuissaS, PatenaudeV, LapiF, et al. Inhaled corticosteroids in COPD and the risk of serious pneumonia. Thorax. 2013;68:1029–1036. doi:10.1136/thoraxjnl-2012-20287224130228
- SuissaS, ErnstP. Precision medicine urgency: the case of inhaled corticosteroids in COPD. Chest. 2017;152:227–231. doi:10.1016/j.chest.2017.05.02028797382
- SantosS, MarinA, Serra-BatllesJ, et al. Treatment of patients with COPD and recurrent exacerbations: the role of infection and inflammation. Int J Chron Obstruct Pulmon Dis. 2016;11:515–525. doi:10.2147/COPD.S9833327042040
- Global Initiative for asthma (GINA). Global strategy for asthma management and prevention; 2018 Available from: http://www.ginasthma.org/guideline-report-2018.htlm. Accessed 326, 2020.
- GibsonPG, SimpsonJL. The overlap syndrome of asthma and COPD: what are its feature and how important is it? Thorax. 2009;64:728–735. doi:10.1136/thx.2008.10802719638566
- KitaguchiYK, KomatsuY, FujimotoK, HanaokaM, KuboK. Sputum eosinophilia can predict responsiveness to inhaled corticosteroid treatment in patients with overlap syndrome of COPD and asthma. Int J Chron Obstruct Pulmon Dis. 2012;7:283–289. doi:10.2147/COPD.S3065122589579
- GershonAS, CampitelliMA, CroxfordR, et al. Combination of long-acting β-agonists and inhaled corticosteroids compared with long-acting β-agonists alone in older adults with chronic obstructive pulmonary disease. JAMA. 2014;312:1114–1121. doi:10.1001/jama.2014.1143225226477
- AlmirallJ, BolibarI, Serra-PrtaM, et al. New evidence of risk factors for community-acquired pneumonia: a population-based study. Eur Respir J. 2008;31:1274–1284. doi:10.1183/09031936.0009580718216057
- CrimC, CalvereleyPM, AndersonJA, et al. Pneumonia risk in COPD patients receiving inhaled corticosteroids alone or in combination: TORCH study results. Eur Respir J. 2009;34:641–647. doi:10.1183/09031936.0019390819443528
- KewKM, SeniukovichA. Inhaled steroids and risk of pneumonia for chronic obstructive pulmonary disease. Cochrane Database Sys Rev. 2014;CD010115.
- FergusonGT, AnzuetoA, FeiR, EmmetA, KnobilK, KalbergC. Effect of fluticasone propionate/salmeterol (250/50 microg) or salmeterol (50 microg) on COPD exacerbations. Respir Med. 2008;102:1099–1108. doi:10.1016/j.rmed.2008.04.01918614347
- AnzuetoA, FergusonGT, FeldmanG, et al. Effect of fluticasone propionate/salmeterol (250/50 microg) on COPD exacerbations and impact on patient outcomes. COPD. 2009;6:320–329. doi:10.1080/1541255090314088119863361
- VestboJ, PapiA, CorradiM, et al. Single inhaler extrafine triple therapy versus long-acting muscarinic antagonist therapy for chronic obstructive pulmonary disease (TRINITY): a double-blind parallel group, randomized controlled trial. Lancet. 2017;389:1919–1929. doi:10.1016/S0140-6736(17)30188-528385353
- PapiA, VestboJ, FabbriL, et al. Extrafine inhaled triple therapy versus dual bronchodilator therapy in chronic obstructive pulmonary disease (TRIBUTE): a double-blind parallel group, randomized controlled trial. Lancet. 2018;391:1076–1084. doi:10.1016/S0140-6736(18)30206-X29429593