
Abstract
Purpose
Little is known about the incidence, risk factors, and prognostic implications of acute kidney injury (AKI) in patients with acute exacerbation of chronic obstructive pulmonary disease (AECOPD) in China. In this study, we investigated the incidence, risk factors, and short-term outcomes of AKI in these patients.
Patients and Methods
We analyzed the records of 1768 patients admitted to Nanjing First Hospital with a principal diagnosis of AECOPD. Of these, 377 patients had AKI.
Results
AKI occurred in 377 patients (21%). Independent risk factors for AKI in patients with AECOPD were advanced age, coronary artery disease, anemia, cancer, chronic kidney disease, hypercapnic encephalopathy, acute respiratory failure, and mechanical ventilation. Patients with AKI had worse prognostic implications and were more likely to require mechanical ventilation (38.7% vs 19.1%, P<0.001); non-invasive mechanical ventilation (38.2% vs 18.9%, P<0.001); invasive mechanical ventilation (18.3% vs 3.1%, P<0.001); intensive care unit (ICU) admission (33.7% vs 12.9%, P<0.001); had a longer ICU stay (9 days vs 8 days, P=0.033) and longer hospitalization (13 days vs 10 days, P<0.001); and higher in-hospital mortality (18.0% vs 2.7%, P<0.001) than those without AKI. Multivariable analysis indicated that compared to patients without AKI, those with stage 1, 2, or 3 AKI had a 1.9-fold, 2.1-fold, or 6.0-fold increased risk of in-hospital death, respectively.
Conclusion
AKI is common in patients with AECOPD requiring hospitalization. Patients with AKI have worse short-term outcomes. Thus, AKI may be a prognostic predictor of patient survival.
Introduction
Worldwide, chronic obstructive pulmonary disease (COPD) affects 9–10% of people over 40 years of age. Citation1 Exacerbation of COPD is a major cause of morbidity and mortality, resulting in decreased health status;Citation2,Citation3 acute kidney injury (AKI) is recognized as also a severe complication of the acute exacerbation of chronic obstructive pulmonary disease (AECOPD).
Fabbian et al previously reported that AKI was an independent risk factor for in-hospital mortality in patients with AECOPD.Citation4 Barakat et al showed that the incidence of AKI in patients with COPD was 128/100,000 person-years, and the prevalence of AKI in patients with AECOPD was 1.9%.Citation5 Moreover, AECOPD patients with AKI had a 1.80-fold higher risk of death within the first 6 months post COPD exacerbation compared to those without AKI.Citation5 However, the incidence, risk factors, and prognostic implications of AKI in Chinese patients with AECOPD remain unknown.
In the present observational study, we determined the incidence of AKI in patients with AECOPD, investigated the factors that predict AKI, and evaluated whether the presence of AKI can predict the requirement for renal replacement therapy (RRT), mechanical ventilation, intensive care unit (ICU), length of mechanical ventilation, ICU stay, length of hospitalization, and in-hospital mortality in patients with AECOPD.
Methods
Study Design
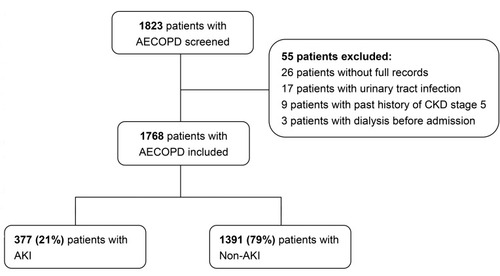
We enrolled patients with AECOPD from Nanjing First Hospital between January 2014 and January 2017. The diagnostic criteria for AECOPD were: (i) history of COPD (forced expiratory volume in one second [FEV1]/forced vital capacity [FVC] <0.70 in the clinically stable state) and (ii) an acute worsening of respiratory symptoms such as dyspnea, cough, or purulent sputum, warranting hospital admission.Citation6 The inclusion criterion was patients with COPD exacerbation required hospitalization. The exclusion criteria were patients without full medical records, patients with urinary tract infection, patients with a history of stage 5 chronic kidney disease (CKD), and those undergoing dialysis prior to hospital admission (). This study was performed in accordance with the Declaration of Helsinki and was approved by the Regional Human Research Ethics Committee of Nanjing First Hospital. Individual patient consent was waived on condition that all patient data were deidentified before analysis, because this study was a retrospective analysis.
Figure 1 Flowchart used to determine patient selection.
Definitions of AKI
AKI was defined as a serum creatinine (SCr) change that met the 2012 Kidney Disease Improving Global Outcomes (KDIGO) criteria, which defined AKI as an increase in SCr levels of ≥0.3 mg/dL within 48 h or ≥1.5-fold from baseline within 7 days.Citation7 We staged AKI according to KDIGO criteria using the difference between baseline and peak serum creatinine levels (in other words, peak injury).Citation7 More specifically, stage 1 AKI was defined as an increase of 50–100% in baseline serum creatinine level or an absolute increase in baseline creatinine of greater than or equal to 0.3mg/dL; stage 2 AKI was defined as an increase of 100–200% in baseline serum creatinine level; stage 3 AKI was defined as a greater than or equal to 200% increase from baseline serum creatinine levels or the initiation of dialysis.
Data Collection
Socio-demographic, comorbidity, and complications were collected from the hospital records. In-hospital outcomes included the requirement for invasive mechanical ventilation, non-invasive mechanical ventilation, mechanical ventilation, the duration of mechanical ventilation, intensive care unit (ICU) admission, the duration of stay in the ICU, renal replacement therapy (RRT), the duration of hospitalization, 30-day mortality and in-hospital mortality.
Data Analysis
The categorical variables are represented as percentages, and carried out using the chi-squared test and the Fisher’s exact test as appropriate. The continuous variables with normal distribution are shown as mean ± standard, and using t-test for univariate comparison; and those with non-normal distribution are shown as median values (25th–75th percentile), and using the Mann–Whitney U-test to compare median values. The variables with P < 0.05 in univariate comparison are included in the multivariate logistic regression analysis to select risk factors associated with AKI. To evaluate the independent factors associated with in-hospital death, we use Cox proportional hazards model. The proportional hazards assumption is assessed using graphical methods, and the proportional hazards assumption is met. The proportional hazards assumption is assessed graphically by plotting the scaled Schoenfeld residuals against follow-up time and by a log-minus-log-survival plot. We set the duration of hospitalization as the time, set the in-hospital death as the status, and set all the variables in as the covariate. Variables that are significant in the univariate analysis are applied to perform multivariate analysis. P values <0.05 are considered as statistically significant. Statistical analysis was using SPSS software, version 22 (IBM, Armonk, NY, USA).
Table 1 Risk Factors for In-Hospital Mortality
Results
AKI Incidence
In total, 1823 patients were admitted with COPD exacerbation, of whom 55 (3.0%) were excluded. Therefore, there were 1768 patients with AECOPD enrolled for analysis, with the mean age of 77.0 ± 9.1 years. Most of the study population consisted of males (76%). AKI occurred in 377 patients (21%), including 13% stage 1 AKI, 5% stage 2 AKI, and 3% stage 3 AKI.
AKI Characteristics
The demographic data, comorbidity, and complications are shown in . Compared with non-AKI group, there was no significant difference in gender for AKI group, but patients with AKI were advanced age (81 years vs 77 years; P < 0.001). Patients with AKI were more commonly complicated with acute respiratory failure (ARF) (44% vs 28%; P < 0.001) and hypercapnic encephalopathy (8.5% vs 2.7%; P < 0.001). Comparison of the incidence of comorbidities in patients with AKI and non-AKI revealed approximately equal proportions of patients with either pulmonary arterial hypertension or chronic liver disease. Nevertheless, patients with AKI had a higher proportion of chronic cor pulmonale (46.9% vs 39.0%; P = 0.006), atrial fibrillation (15.6% vs 8.9%; P < 0.001), hypertension (59.7% vs 50.7%; P = 0.002), diabetes mellitus (19.4% vs 15.0%; P = 0.038), coronary artery disease (42.7% vs 24.4%; P < 0.001), CKD (27.1% vs 7.8%; P < 0.001), anemia (42.7% vs 27.6%; P < 0.001), cerebrovascular disease (26.3% vs 19.3%; P = 0.003), and cancer (8.5% vs 5.2%; P = 0.018).
Table 2 Demographics of Patients with or Without AKI
Risk Factors for AKI
Risk factors for AKI in patients with AECOPD were advanced age (odds ratio [OR], 1.06; 95% CI, 1.04–1.07; P < 0.001), coronary artery disease (OR, 1.68; 95% CI, 1.28–2.20; P < 0.001), CKD (OR, 4.35; 95% CI, 3.14–6.03; P < 0.001), anemia (OR, 1.34; 95% CI, 1.03–1.75; P = 0.029), cancer (OR, 1.81; 95% CI, 1.13–2.91; P = 0.014), ARF (OR, 1.44; 95% CI, 1.06–1.98; P = 0.022), hypercapnic encephalopathy (OR, 1.95; 95% CI, 1.12–3.38; P = 0.018), and mechanical ventilation (OR, 2.23; 95% CI, 1.61–3.08; P < 0.001) (). Our model achieved an apparent area under the receiver operating characteristic curve (AUC-ROC) of 0.76 (95% CI, 0.74–0.79, P < 0.001).
Table 3 Multivariate Analysis of Risk Factors for AKI in Patients with AECOPD
In-Hospital Outcomes
In-hospital outcomes for patients with or without AKI are shown in and .
Table 4 Duration of Hospital Stay in Patients with or Without AKI
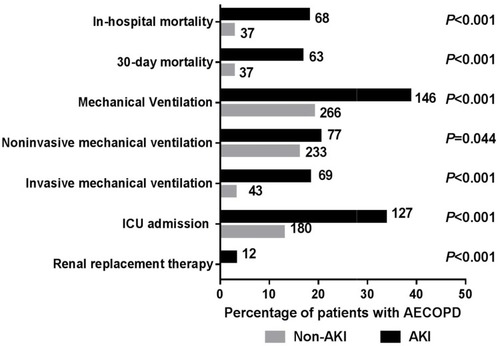
Figure 2 In-hospital outcomes of patients with or without AKI. This graph shows a comparison of the proportion (%) of patients with or without AKI that required renal replacement therapy, ICU admission, invasive mechanical ventilation, non-invasive mechanical ventilation, and mechanical ventilation during hospitalization. The graph also shows a comparison of 30-day mortality and in-hospital mortality between AKI and non-AKI groups. Numbers at the top of bars represent the number of patients in the respective category for with/without AKI. P-values were calculated using the Pearson chi-squared test/Fisher’s exact test where appropriate.
Mechanical Ventilation
Patients with AKI were more likely to require mechanical ventilation (38.7% vs 19.1%; P < 0.001), non-invasive mechanical ventilation (38.2% vs 18.9%; P < 0.001), and invasive mechanical ventilation (18.3% vs 3.1%; P < 0.001) compared with the non-AKI group. However, there was no significant difference in duration of mechanical ventilation between AKI (8 days; interquartile ratio [IQR], 5–16 days) and non-AKI groups (9 days; IQR, 5–14 days; P = 0.803).
Renal Replacement Therapy
Overall, there were12 patients requiring renal replacement therapy (RRT), which accounted for 3.2% of all patients with AKI. Moreover, the in-hospital mortality of this group was as high as 91.7% (11/12).
ICU Admission
ICU admission for patients with AKI had a higher proportion than the non-AKI group (33.7% vs 12.9%; P < 0.001). Moreover, compared with the non-AKI group (8 days; interquartile ratio [IQR], 4–13 days), patients with AKI had a longer median stay in the ICU (9 days; IQR, 6–16 days; P = 0.033).
Duration of Hospitalization
Patients with AKI also had a longer median duration of hospitalization (13 days; IQR, 8–18 days) compared with the non-AKI group (10 days; IQR, 7–13 days; P < 0.001).
In-Hospital Mortality
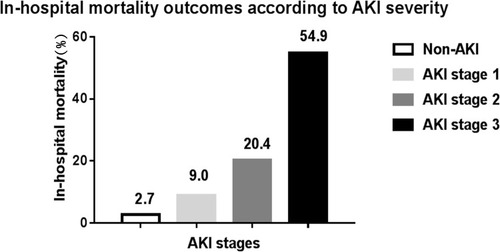
During the hospitalization, the overall in-hospital mortality was 5.9% (105/1768). In-hospital mortality was 2.7% in the non-AKI group, compared with 18.0% in patients with the AKI group. In particular, more than half of the patients (54%) with stage 3 AKI died during hospitalization. shows the in-hospital mortality according to AKI stages.
Figure 3 Inpatient mortality outcomes according to AKI stages. This figure shows the proportion (%) of patients with each stage of AKI who died during hospitalization.
Risk Factors for in-Hospital Death
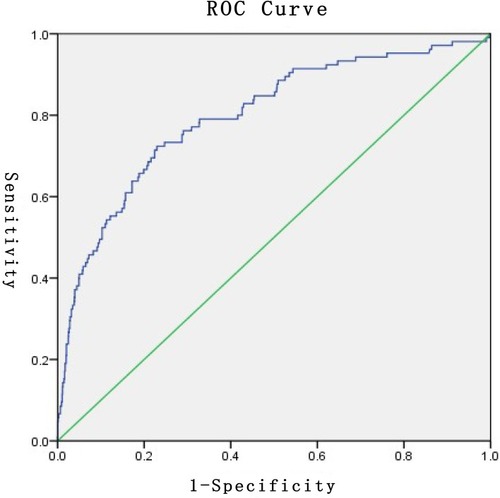
shows the independent factors of in-hospital death. After adjustment for other significant factors of death, comparing to patients without AKI, the in-hospital death of patients with stage 1, stage 2, and stage 3 AKI increased 1.92-fold (95% CI, 1.11–3.33; P = 0.020), 2.14-fold (95% CI, 1.16–3.96; P = 0.015), and 6.06-fold (95% CI, 3.46–10.46; P < 0.001), respectively. In addition, age (hazard ratio [HR] 1.03, 95% CI, 1.01–1.06; P = 0.026), CKD (HR 1.68, 95% CI, 1.02–2.77; P = 0.042), and ARF (HR 4.19, 95% CI, 2.48–7.08; P < 0.001) were also independent risk factors for in-hospital death. This model achieved an apparent AUC-ROC of 0.80 (95% CI, 0.75–0.85, P < 0.001) ().
Figure 4 Receiver operator characteristic (ROC) curve showing discrimination power of this model for in-hospital death.
Discussion
In this study, approximately one-fifth of in-patients with AECOPD had AKI, and patients with AKI had worse prognostic implications. Compared with the non-AKI group, AKI occurring in patients with AECOPD was independently associated with increased in-hospital mortality, an increased risk of requiring mechanical ventilation, non-invasive mechanical ventilation, invasive mechanical ventilation, ICU admission, and a longer duration of ICU stay and hospitalization.
We found that the incidence of AKI was 21.3% in in-patients with AECOPD. Our current results showed a much higher incidence compared to the 1.9% and 5.0% reported in previous studies by Barakat et al and Fabbian et al, respectively.Citation4,Citation5 We tried to explain the difference. Firstly, in recent years, the incidence of AKI was steadily increasing (note that the study by Fabbian et al started in 2000, and the study by Barakat et al started in 2004).Citation8 Therefore, the incidence of AKI was underestimated. Secondly, ARF was an important factor for AKI, and previous studies reported that the incidence of AKI in patients with ARF ranged from 35% to 62%.Citation9–Citation11 In our study, about one-third of patients suffered complications from ARF. Thirdly, in the studies by Fabbian et al and Barakat et al, AKI was diagnosed by the International Classification of Diseases.Citation4,Citation5 However, the performance of International Classification of Diseases in identifying AKI reported that the sensitivity was only 17%, and specificity was >98%, which might underestimate the incidence of AKI.Citation12
Our study showed that the risk factors for AKI are advanced age, coronary artery disease, CKD, anemia, cancer, ARF, hypercapnic encephalopathy and mechanical ventilation. Barakar et al reported that advanced age, hypertension, angina, heart failure, and CKD were independently associated with AKI in patients with AECOPD.Citation5 Mechanical ventilation was an important treatment for patients with AECOPD.Citation13 On the contrary, mechanical ventilation was also an independent risk factor for AKI. Previous study had reported that there were three main mechanisms for explaining AKI caused by mechanical ventilation.Citation14 Firstly, through effects on arterial blood gases. Either severe hypoxemia or hypercapnia could reduce renal blood flow (RBF). Secondly, through an effect on systemic and renal blood flow. Mechanical ventilation decreased preload and increased right ventricular afterload, and ultimately decreased cardiac output. Thirdly, mechanical ventilation may lead to bio-trauma, which was an inflammatory reaction in the lung and inflammatory mediators released into the systemic circulation. In addition, other studies had also verified the release of inflammatory mediators by mechanical ventilation.Citation15–Citation18 This study was the first to report that hypercapnic encephalopathy was a risk factor for AKI, which may be associated with blood gas disturbances and RBF. Hypoxemia could reduce RBF by increasing renal vascular resistance as a result of the activation of vasoactive factors such as endothelin, angiotensin II, as well as decreased level of nitric oxide.Citation19–Citation21 Hypercapnia was also correlated inversely with RBF mainly by releasing noradrenaline and resulting in constricting blood vessels.Citation22
In our study, AKI increased the risk of patients requiring mechanical ventilation, ICU admission, a longer length of ICU stay, a longer length of hospitalization, and higher in-hospital mortality. More specially, advanced age, ARF, AKI, and CKD were independent risk factors for in-hospital death. We found that both CKD and AKI played an important role in increasing in-hospital mortality in patients with AECOPD. In our study, patients with CKD had a 1.68 times increased risk for in-hospital death. This was consistent with a previous meta-analysis that reported CKD was an independent predictor for short-term mortality in COPD exacerbations.Citation23 A study performed by Hasegawa et al showed that patients with COPD who required hospitalization coexisting with CKD had a 1.73 times increased risk of in-hospital death.Citation24 Additionally, previous studies regarding the association between AKI and in-hospital mortality during COPD exacerbation were even scarcer. Fabbian and coworkersCitation4 found that the mortality rate for AKI was 16.6% compared to 4.0% for cases without AKI, and AKI was one of the predictors associated with higher in-hospital mortality, and increasing 3.85-fold risk of in-hospital mortality. Alaithan et alCitation25 evaluated 119 patients with COPD who were admitted to ICU and found that AKI was identified as an independent risk factor associated with in-hospital mortality. In our study, in-hospital mortality was significantly higher in patients who suffered from AKI compared with those without AKI (18.0 vs 2.7%). Patients with stage 1, stage 2, and stage 3 AKI had a 1.9-fold, 2.1-fold, and 6.0-fold increased risk of in-hospital death, respectively. Advanced age and ARF are two common risk factors for in-hospital death in patients with AECOPD.Citation26 Steer et alCitation27 developed a simple prediction tool, termed the DECAF score, which could identify high risk of in-hospital mortality in patients admitted for COPD exacerbation. Unfortunately, AKI was not considered in this scoring system; future studies should attempt to incorporate AKI into the DECAF scoring system.
There were several limitations in this study. Firstly, this was a retrospective single-center study, so its inherent weakness could not be avoided. Secondly, data such as body mass index, COPD severity stage, and smoking were not available, which may be associated with AKI. Thirdly, we did not assess urine output in determining the presence of AKI. Although AKI is partly defined by urine volume,Citation7 most AKI staging studies have used only SCr levels, and not urine output.Citation28 Fourthly, the timeframe to evaluate the presence of AKI is crucial for interpretation of the causal relationships between AKI and other endpoints or complications. As this study is a retrospective observational study, in this study we simply analyze and observe the association between AKI and other endpoints or complications, and cannot prove to be interpretation of the causal relationships between AKI and other endpoints or complications.
Conclusions
AKI was common in in-patients with AECOPD, and patients with AKI had worse prognostic implications.
Ethics Approval
Approval was granted by the Regional Human Research Ethics Committee of Nanjing First Hospital.
Author Contributions
The study was designed by C-CC, WX and D-WC. Data were analysed by YT, M-QM, and FZ. Z-HL, YC, and WS were responsible for collecting the data. All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
Acknowledgment
This study was supported by the Science and Technology Development Fund of Nanjing Medical University (NMUB2018324), Research project of Health and Family Planning Commission of Jiangsu Province (BJ15004), and Natural Science Foundation of Jiangsu Province (BK20171485).
References
- World Health Organization. Chronic Obstructive Pulmonary Disease (COPD); 2014 [cited 723, 2014] Available from: http://www.who.int/respiratory/copd/en/. Accessed 429, 2020.
- CelliBR, BarnesPJ. Exacerbations of chronic obstructive pulmonary disease. Eur Respir J. 2007;29:1224–1238. doi:10.1183/09031936.0010990617540785
- WedzichaJA, SeemungalTA. COPD exacerbations: defining their cause and prevention. Lancet. 2007;370:786–796. doi:10.1016/S0140-6736(07)61382-817765528
- FabbianF, De GiorgiA, ManfrediniF, et al. Impact of renal dysfunction on in-hospital mortality of patients with severe chronic obstructive pulmonary disease: a single-center Italian study. Int Urol Nephrol. 2016;48:1121–1127. doi:10.1007/s11255-016-1272-527020445
- BarakatMF, McDonaldHI, CollierTJ, et al. Acute kidney injury in stable COPD and at exacerbation. Int J Chron Obstruct Pulmon Dis. 2015;10:2067–2077. doi:10.2147/COPD.S8875926451102
- VestboJ, HurdSS, AgustiAG, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2013;187:347–365. doi:10.1164/rccm.201204-0596PP22878278
- KellumJA, LameireN, GroupKAGW. Diagnosis, evaluation, and management of acute kidney injury: a KDIGO summary (Part 1). Crit Care. 2013;17:204. doi:10.1186/cc1145423394211
- KolheN. Epidemiology of Acute Kidney Injury in England – 1998 to 2013; 2014 NLM identifier: NCT2216695 [cited 429, 2015] Available from: https://clinicaltrials.gov/ct2/show/NCT2216695. Accessed 429, 2020.
- LiuKD, GliddenDV, EisnerMD, et al. Predictive and pathogenetic value of plasma biomarkers for acute kidney injury in patients with acute lung injury. Crit Care Med. 2007;35:2755–2761.18074478
- MandelbaumT, ScottDJ, LeeJ, et al. Outcome of critically ill patients with acute kidney injury using the Acute Kidney Injury Network criteria. Crit Care Med. 2011;39:2659–2664. doi:10.1097/CCM.0b013e3182281f1b21765352
- SotoGJ, FrankAJ, ChristianiDC, et al. Body mass index and acute kidney injury in the acute respiratory distress syndrome. Crit Care Med. 2012;40:2601–2608. doi:10.1097/CCM.0b013e3182591ed922732288
- GramsME, WaikarSS, MacMahonB, et al. Performance and limitations of administrative data in the identification of AKI. Clin J Am Soc Nephrol. 2014;9:682–689. doi:10.2215/CJN.0765071324458075
- National Collaborating Centre for Chronic C. Chronic obstructive pulmonary disease. National clinical guideline on management of chronic obstructive pulmonary disease in adults in primary and secondary care. Thorax. 2004;59(Suppl 1):1–232.
- KuiperJW, GroeneveldAB, SlutskyAS, et al. Mechanical ventilation and acute renal failure. Crit Care Med. 2005;33:1408–1415. doi:10.1097/01.CCM.0000165808.30416.EF15942363
- RanieriVM, SuterPM, TortorellaC, et al. Effect of mechanical ventilation on inflammatory mediators in patients with acute respiratory distress syndrome: a randomized controlled trial. JAMA. 1999;282:54–61. doi:10.1001/jama.282.1.5410404912
- GurkanOU, O’DonnellC, BrowerR, et al. Differential effects of mechanical ventilatory strategy on lung injury and systemic organ inflammation in mice. Am J Physiol Lung Cell Mol Physiol. 2003;285:L710–718. doi:10.1152/ajplung.00044.200312754185
- ImaiY, ParodoJ, KajikawaO, et al. Injurious mechanical ventilation and end-organ epithelial cell apoptosis and organ dysfunction in an experimental model of acute respiratory distress syndrome. JAMA. 2003;289:2104–2112. doi:10.1001/jama.289.16.210412709468
- HepokoskiM, EnglertJA, BaronRM, et al. Ventilator-induced lung injury increases expression of endothelial inflammatory mediators in the kidney. Am J Physiol Renal Physiol. 2017;312:F654–660. doi:10.1152/ajprenal.00523.201628365585
- BallevreL, ThonneyM, GuignardJP. Role of nitric oxide in the hypoxemia-induced renal dysfunction of the newborn rabbit. Pediatr Res. 1996;39:725–730. doi:10.1203/00006450-199604000-000268848351
- HuetF, SemamaDS, GouyonJB, et al. Protective effect of perindoprilat in the hypoxemia-induced renal dysfunction in the newborn rabbit. Pediatr Res. 1999;45:138–142. doi:10.1203/00006450-199901000-000239890622
- SemamaDS, ThonneyM, GuignardJP. Does endothelin-1 mediate the hypoxemia-induced renal dysfunction in newborn rabbits? Biol Neonate. 1995;67:216–222. doi:10.1159/0002441677640322
- AnandIS, ChandrashekharY, FerrariR, et al. Pathogenesis of congestive state in chronic obstructive pulmonary disease. Studies of body water and sodium, renal function, hemodynamics, and plasma hormones during edema and after recovery. Circulation. 1992;86:12–21. doi:10.1161/01.CIR.86.1.121617764
- SinganayagamA, SchembriS, ChalmersJD. Predictors of mortality in hospitalized adults with acute exacerbation of chronic obstructive pulmonary disease. Ann Am Thorac Soc. 2013;10:81–89. doi:10.1513/AnnalsATS.201208-043OC23607835
- HasegawaW, YamauchiY, YasunagaH, et al. Factors affecting mortality following emergency admission for chronic obstructive pulmonary disease. BMC Pulm Med. 2014;14:151. doi:10.1186/1471-2466-14-15125253449
- AlaithanAM, MemonJI, RehmaniRS, et al. Chronic obstructive pulmonary disease: hospital and intensive care unit outcomes in the Kingdom of Saudi Arabia. Int J Chron Obstruct Pulmon Dis. 2012;7:819–823. doi:10.2147/COPD.S3761123269866
- HuGP, ZhouYM, WuZL, et al. Red blood cell distribution width is an independent predictor of mortality for an acute exacerbation of COPD. Int J Tuberc Lung Dis. 2019;23(7):817–823. doi:10.5588/ijtld.18.042931439113
- SteerJ, GibsonJ, BourkeSC. The DECAF Score: predicting hospital mortality in exacerbations of chronic obstructive pulmonary disease. Thorax. 2012;67:970–976. doi:10.1136/thoraxjnl-2012-20210322895999
- ThomasME, BlaineC, DawnayA, et al. The definition of acute kidney injury and its use in practice. Kidney Int. 2015;87:62–73. doi:10.1038/ki.2014.32825317932