
Abstract
The absence or late initiation of palliative care (PC) in chronic obstructive pulmonary disease (COPD) is multidimensional. To provide palliative care from the moment of COPD diagnosis remains utopic. Even the advanced forms or the end-of-life stages benefit late or never from these services. In this context, the research questions for the present systematic review were focused on the prognosis variables or multicomponent indices in COPD patients alongside the symptoms and unmet needs, which may be useful for the palliative care initiation. The aim was to help clinicians to identify not only the tools reliable to predict poor survival in COPD patients but also to identify the criteria for appropriateness for early palliative care onset. The search included systematic reviews and reviews published in English in the PUBMED database from Jan 1, 2015 to Jan 6, 2020. From a total of 202 findings, after applying filters, using additional sources, and eliminating duplicates, the search strategy screened 16 articles, out of which 10 were selected and included. A Preferred Reporting Items for Systematic Review and Meta-analysis Protocols (PRISMA-P) flow diagram was constructed. The main domains identified as barriers in providing palliative care in COPD patients were complex: from the prognosis difficulties to the prognostic variables and scores proposed for initiating PC; from the troublesome symptoms or the unidimensional symptom tools to the unmet needs of COPD patients. The review concluded that none of the existing prognostic variables and multicomponent indices are reliable enough to exclusively predict poor survival in COPD patients and the decision to initiate PC should be rather based on the presence of refractory symptoms and patients’ unmet needs and preferences. Despite the current advances, the ideal model to initiate palliative care from the moment COPD is diagnosed is a goal for clinicians trained in, and capable of providing palliative care in any COPD patient.
Introduction
Chronic respiratory diseases (CRDs) are a group of chronic diseases that affect the airways and other structures of the lung, according to the definition of the World Health Organization (WHO).Citation1 Both the prevalence and the global burden of CRDs are increasing worldwide, with an important impact on the quality of life.Citation2 Even though CRDs are not curable, the WHO Global Alliance against CRDs (GARD) focuses on the prevention of these diseases and care of these patients worldwide, in order to globally reduce morbidity, disability, and premature mortality related to the diseases.
Under the umbrella term of CRD, one of the most common diseases included is represented by chronic obstructive pulmonary disease (COPD).Citation1 It is considered a public health challenge as a major contributor to global morbidity and mortality.Citation3 Currently, COPD is the fourth-leading global cause of death, and in 2030 it is expected to become the third cause of mortalityCitation4 and the seventh leading cause of disability-adjusted life years (DALYs) lost worldwide.Citation5
Alongside interstitial lung disease (ILD) and bronchiectasis, COPD is a Non-Malignant Respiratory Disease (NMRD), another umbrella term proposed by the National End of Life Care Intelligence Network in 2011.Citation6 Even though, worldwide, over 210 million people have a diagnosis of COPD, and millions of others have another form of NMRD,Citation7 a holistic approach to the diseases is still an idealistic concept globally. Palliative care is a patient-centered holistic approach, focused on the management of symptoms, good communication between patients and health-care providers, and maintaining quality of lifeCitation8 of patients and their family, through the prevention and relief of suffering. According to the World Health Organization (WHO), PC improves the quality of life by early identification and impeccable assessment and treatment not only of pain and other overwhelming symptoms but also addressed to the psychological, social, and spiritual dimensions.Citation9,Citation10
From this point of view, the role of PC for patients with NMRD was emphasized by the key international respiratory guidelines.Citation11 The American Thoracic Society (ATS) highlighted the importance of integrating palliative care from the moment of diagnosis.Citation12 Regardless of the unpredictable course of the disease, PC should be encouraged to occur early in the disease trajectory.Citation11 Still, the estimated need for palliative care in patients with chronic respiratory diseases is high (10.3%), coming second to that in cardiovascular diseases (38.5%) and cancer (34%).Citation13 Unfortunately, palliative care is not available worldwide for these patients, independently of what settings are considered. The possible explanations and barriers for this fact are complex and found even in countries where the role and development of palliative care services are worked out for many years. The aim of the current review was to offer an overview of the latest data about the initiation of palliative care in patients living with COPD, from the existing prognosis and multivariable scores to the burden of refractory symptoms and the unmet needs of patients and those close to them. The purpose was to help clinicians to identify not only the tools reliable to predict poor survival in COPD patients but also to identify the criteria for appropriateness for early palliative care onset.
Research Questions
How should palliative care be initiated in COPD patients: prognostic-based, symptoms-based, and/or needs-based?
Materials and Methods
Inclusion/Exclusion Criteria of the Studies
The inclusion criteria were articles related to palliative care and the prognosis in COPD. Other inclusion criteria were: studies focused on the troublesome symptoms of COPD patients, studies about the unmet needs of patients living with COPD and palliative care. The main included article types were reviews and systematic reviews.
The exclusion criteria were: studies not related to the topic/methodology; articles related to other diseases not to COPD; articles addressed only to lung cancer patients; articles not related at all to the palliative care perspective; studies with only abstracts available; case-studies; randomized control studies; duplicates.
Literature Search
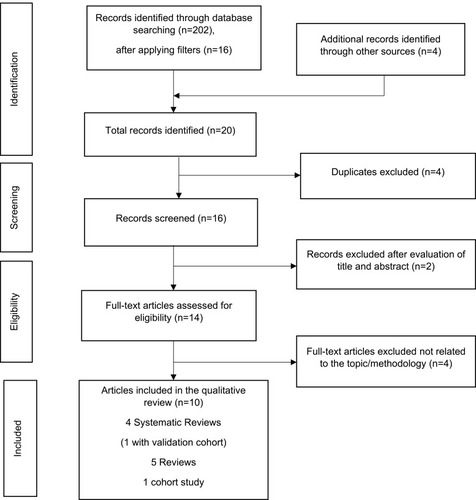
This systematic review was based on the search from electronic data sources using the PubMed (MEDLINE) database. There was no need for Ethics Committee approval since this study was a synthesis of published studies. The initial search strategy on the keywords Palliative Care and Prognosis in COPD identified 202 results. After applying the filters: Systematic Reviews, Review, Full text, published in the last 5 years, Humans, English, 16 records were identified. The publication date of the search was between Jan 1, 2015 and Jan 6, 2020. The search included full-text systematic reviews and reviews published in the English language. We supplemented our electronic database search from other sources, including reference lists of included studies, index-related articles on PubMed, and existing relevant reviews. Four additional records were identified from other sources. From the 20 studies identified, after excluding the 4 duplicates, 16 records were screened. After further evaluations of the title and abstracts, 2 studies were excluded. From the 14 full-text articles assessed for eligibility, 4 articles were excluded because they were not related to the topic. Finally, 10 articles were included in our review: 4 systematic reviews (1 with validation cohort), 5 reviews, and 1 cohort study. A manual search was performed afterward. We were initially focused on the studies involving palliative care onset in COPD mainly from the prognostic perspective, but we further extended our analysis on the importance of refractory symptoms and the unmet needs of COPD patients. A Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA)Citation14 flow diagram was constructed, as shown in . The screening of the English titles and abstracts of the articles with potential eligibility was also simultaneously conducted by one independent researcher (AGR). The two reviewers read and analyzed all full-text articles, considering the inclusion and exclusion criteria. Any differences in opinion were discussed and resolved by consensus. A narrative synthesis of the identified evidence was performed.
Figure 1 Literature identification process (PRISMA flowchart).
Results
After reading and analyzing the included studies, some issues emerged. A brief synthesis of the reviewed articles with their main findings, identified gaps and limitations are summarized in the Supplementary materials Table S1.
Difficulties of Prognosis – an Important Barrier to Provide PC
The unpredictable and prolonged trajectory of the disease makes prognostication difficult for physicians, patients, and their families.Citation15 The inexact prognosis of this chronic life-limiting illness, with a progressive decline punctuated with acute, potentially life-threatening exacerbations, is not only a clinical challenge but also a barrier to timely referral and receipt of palliative care.Citation3,Citation16 The questions about the moment to start PC and which COPD patients should receive it remain controversial.Citation17 In their systematic literature review of 17 European guidelines and 2 pathways, Siouta et al offered an overview of the level of integration of PC in COPD.Citation18 The determination of the referral criteria to start PC, the moment to initiate PC, and the modest predictive value of different prognostic tools were debatable topics analyzed in the systematic review. Though 12 out of the 19 guidelines/pathways explicitly discussed the point of which PC should be initiated, large variations of the exact timing to start PC were noted: from the moment of COPD diagnosis or only for the terminally ill stages or depending on the frequency of exacerbations or hospitalizations, to the last 12 months of life or to the last 6 months of life (3 guidelines from the Netherlands, but none of them invoked the surprise question).Citation18 Besides the above-mentioned aspects, the study highlighted the overall growing awareness for the importance of integrated PC in advanced forms of COPD patients, although a standardized and universally accepted definition of integrated PC is missing.Citation18 A possible solution to overcome these barriers is to include individualized palliative interventions in the management of COPD patients from the moment of diagnosis. Still, the ideal model proposed for early integrated PC in daily practice needs further validation, as Harrington et al outlined.Citation16
Prognostic Variables and Scores Proposed for Initiating PC
Significant factors in prognosticating are available.Citation19 there is a lack of a “gold standard” method to predict prognosisCitation5 and consequently to integrate palliative care as early as possible. Starting from the observation that current recommendations to consider initiation of PC in COPD are often based on an expected poor prognosis (≤1 year survival),Citation17 in their systematic review Almagro et al analyzed the reliability of 17 prognostic variables and 3 multicomponent indices recommended for start PC based on an expected 1-year mortality. The utility of the proposed variables was further validated in a cohort study of 697 patients hospitalized for COPD exacerbation. Ten predictive mortality variables with statistical significance (p-value ≤0.05) were identified. Among them, only 4 had a concomitant sensibility and specificity ≥50%: age ≥70 years, severe dyspnea (3–4 in the modified dyspnea Medical Research Council (mMRC)), depression (Yesavage scale ≥5 points), and poor health-related quality of life (Saint George’s Respiratory Questionnaire ≥60 points). The other predictive mortality variables that reached statistical significance were: severe physical dependence with loss ≥3 activities of daily living (Katz index), low body mass index (BMI ≤21 kg/m2), the presence of comorbidities (Charlson index ≥3) and 3 multicomponent indices ≥7, like the BODE index (Body mass index, Obstruction, Dyspnea and 6 min walking test), the BODEx index (Body mass index, airflow Obstruction, Dyspnea, severe exacerbations) and the CODEX index (Comorbidity, Obstruction, Dyspnea, severe exacerbations). Almagro also tested in the cohort study an adaptation of the Curtis criteria,Citation20 which represent another combination of variables proposed as a main criterion to start PC based on a poor prognosis (forced expiratory volume in 1 s (FEV1) <30% predicted; oxygen dependence; ≥1 hospital admissions in the previous year for an acute exacerbation of COPD; left heart failure or other comorbidities; weight loss or cachexia; decreased functional status; increasing dependence on others; age >70 years). The only statistically significant cut-off for this criterion was ≥3 (61% patients),Citation17 not ≥2 as recommended by Curtis.Citation20
Summarizing the results, the identified variables and multicomponent indices may be considered useful predictors of survival, but they should not be used as exclusive criteria for initiating PC, because none of them is sufficiently reliable. The timing to start PC in COPD patients should be based on the presence of symptoms refractory to conventional treatment, together with patients’ preferences.Citation17 Prognostic variables play rather a secondary role. Smith et alCitation5 highlighted the same conclusion in their systematic review. They did not find a single variable or a multivariate score that can be recommended for use in practice to predict mortality at or less than 1 year. Among the 6 multivariable and the 3 comorbidity indices analyzed, only one score was derived identified - the B-AE-D score:Citation21
B – body mass index [BMI]
AE – severe acute exacerbation of COPD [AECOPD] frequency
D – modified Medical Research Council [mMRC] dyspnea severity.
The results completed the findings of the Almagro study,Citation17 because they were obtained from stable COPD patients (not hospitalized).Citation5 Smith et al also noted, but did not include in their review, four tools for the identification of COPD patients in the last year of life: the Gold Standards Framework Prognostic Indicator Guidance (GSF-PIG), the RADboud Indicators of Palliative Care Needs (RAD-PAC), the Supportive and Palliative Care Indicators Tool (SPICT), and the Necesidades Paliativas (NECPAL) program. The mentioned tools were developed using expert knowledge, based on the existing studies, combined with the clinical experience. However, the major limitation of these tools is that they were not tested for accuracy and no evidence of reliable prognostication prediction or about other outcomes is available. They also may not be compared to other multivariable tools derived using statistical methods. Those were the main motifs for not being included in their review.Citation5 Recently, in 2019, Bloom et al derived a prognostic risk model to predict mortality at 1 year based on 18 different variables - the BARC index, acronym derived from:Citation22
B – body mass index and blood tests,
A – age,
R – respiratory variables (airflow obstruction, exacerbations, smoking),
C – comorbidities.
The Clinical Practice Research Datalink (CPRD) was used as a data source for the COPD populations. Though the model was aimed to increase predictive performance and to offer clinical and practical advantages, the usefulness in primary care or in hospitalized patients seems equivocal. The excessive number (18) of incorporated variables, the lack of specification for the cut-off points and scores of each variable limit the applicability for clinicians.
Initiating Palliative Care in COPD Patients – More Symptom-Based, Than Prognostic-Based
People with advanced COPD experience distressing physical and psychological symptoms together with a lot of concerns,Citation3 expressed more or less. The importance of troublesome symptoms like dyspnea, fatigue, cough, cachexia, depression, or anxiety, that can occur during the course of the disease, was emphasized by literature in recent years.Citation3,Citation15,Citation23 Besides their high prevalence and prognostic implications, their impact on the quality of life is significantly experienced by COPD patients.Citation17 Moreover, they also have an important psychosocial effect. For example, severe breathlessness causing functional disability may contribute to the patient’s isolation and loneliness.Citation3 Refractory symptoms that persist despite optimal management of the underlying diseases must be recognized by clinicians. The detailed medical history, together with comprehensive symptom assessment, including the evaluation of the level of dyspnea or other existing symptoms, their evolution during the course of the disease, and the diagnosis of their underlying factors, have to be carefully evaluated. It is not limited to the severity of symptoms but also includes the multifaceted effect of symptoms on patients and their caregivers’ life.Citation3
The focus on the assessment and the management of patients’ bothersome symptoms and concernsCitation3 should be a priority in clinical practice in order to establish the need for initiating PC according to the patient’s own goals. In this context, integrated palliative care should be considered alongside the usual therapy, the non-pharmacological and the psychological measures,Citation17 in order to reduce suffering,Citation18 by improving the symptoms and the quality of life,Citation3,Citation15 to reduce the health-care utilization and to increase the patient and caregiver satisfaction.Citation3
Refractory breathlessness related to deconditioning, increased depression and anxiety, and impaired quality of life is also associated with a higher risk of hospitalization and premature mortality.Citation23 In order to better assess the dimensions of breathlessness in different settings of COPD population, uni- and multidimensional tools were developed and validated. Ekstrom et al reviewed recent advances in the outcome measurement of refractory breathlessness in COPD patients.Citation23 Two validated unidimensional tools were outlined. The Exacerbations of Chronic Pulmonary Disease Tool (EXACT) – Respiratory Symptoms (RS) (E-RS)Citation24 can be used to measure the intensity of daily respiratory symptoms (breathlessness, cough, sputum, chest symptoms) as a summary score in daily life in patients with stable COPD. The other unidimensional tool that is reliable and responsive measures dyspnea during daily activities in COPD outpatients; this is the weekly mean SOBDA score (Shortness of Breath with Daily Activities).Citation19,Citation25 As the impact of breathlessness is complex, the use of multidimensional tools such as the Dyspnea-12Citation26 score or the Multidimensional Dyspnea Profile,Citation27 aimed to measure the intensity, the unpleasantness, the quality, and the patients’ emotional responseCitation23 to it, can be a useful aid for the clinicians that treat these patients. As Maddocks et alCitation3 highlighted in their review, most pharmacological approaches for breathlessness do not cover all the complex aspects related to this symptom. Though there is a limited evidence base, the use of pharmacological treatments together with non-pharmacological therapies, like pulmonary rehabilitation, component interventions (breathing techniques, hand-held fan), cognitive behavioral therapy, or multi-professional integrated breathlessness services, showed benefits in patients experiencing dyspnea.Citation3 If breathlessness is refractory, unremitting despite the optimal management, other drugs can be used. In these patients, a low dose of oral or parenteral opioids could palliate breathlessness, although the evidence base is of low quality, with few small trials and participants. Potential related side-effects such as constipation, nausea, or vomiting should be constantly identified, managed, and explained,Citation3 as they can be a reason for opioid’s withdrawal and an additional source of concerns for patients and their families. In clinical practice, benzodiazepines may be considered as a second or third-line treatment for breathlessness which is not responding to opioids, though studies failed to support their use. Antidepressants may relieve dyspnea for two reasons: the implication of the serotonergic pathways and the fact that depression commonly occurs together with breathlessness.Citation3 Though severe depressive symptoms or the clinical depression are present in almost 40% of COPD patients,Citation19 they are difficult to diagnose in daily practice due to the symptoms overlapping between the two diseases. In this context, the use of the six-item Hamilton Depression Rating Subscale (HAM-D6),Citation19 a sensitive tool comparable to the original version, can be helpful for the screening of depression. This comorbidity (Yesavage scale ≥5 points) was identified as a statistically significant predictive 1-year mortality variable in COPD patientsCitation17 with an important impairment on the quality of life.Citation17,Citation19 Complex interventions, including cognitive behavioral therapy, psychological and lifestyle interventions, multicomponent exercise training, and antidepressant drugs (selective serotonin-reuptake inhibitors best tolerated) have supporting therapeutic evidence.Citation3 COPD patients may experience different pains, of several aetiologies, possibly caused by the systemic effects or therapies (corticosteroids use) of the disease or by the pre-existing comorbidities.Citation3 Non-opioids, opioids, or new analgesics are the pharmacological options that may be used inpain management.Citation3 The assessment and treatment of the potentially adverse effects are mandatory. Daytime sleepiness and insomnia may be another bothersome symptom in the life of COPD patients. Good sleep hygiene, cognitive behavioral therapy, benzodiazepines, or non-invasive positive pressure ventilation for hypercapnic patients with stable disease may be used for the treatment, as Maddocks et al noted.Citation3
The Complex Unmet Needs of COPD Patients
Due to the complexity of the disease and the multiple areas of needs, the preferences of COPD patients have to be actively assessed. The process should be ongoing, as the preferences of patients and their caregivers might change over time.Citation3 In their systematic review of qualitative findings, Clari et al identified three main domains regarding the perception of the unmet needs:
1) unmet needs regarding information about the disease,
2) unmet physical, emotional, spiritual, financial, and social support needs, and
3) unmet care needs.Citation4
Besides the sustained symptom burden, patients living with COPD often have a limited understanding of their disease.Citation3 A reason for that may be the frequent communication barrier from both the patient and their doctor's perspective.Citation15 The unmet needs around knowledge of COPD include: information regarding different potential risk factors such as cigarette smoking, the lack of understanding of the most-used terminology related to COPD, or the lack of data about the disease management, including self-management decisions and measures.Citation4 Patients' concerns about not receiving information are also related to the prognosis and the progression of the disease, including the end-of-life stages.Citation3,Citation4 On the other hand, health-care professionals should take into account that not all patients and their caregivers are opened to end-of-life discussions; therefore, the assessment of individual communication preferences is extremely important.Citation3
The troublesome symptoms of advanced COPD, like breathlessness, chest pain, fatigue, or the unwanted effects of treatments may compromise not only the physical needs, disrupting the daily living activities, but also the social needs of these patients.Citation4 They may feel frustrated, anxious, depressed, angry,Citation4 self-blaming, or even demeaned by the limitations of the disease.Citation3 The fear and concerns about the future, the fear of dependence (on family, home oxygen), the feeling of being a burden for their families, and the reduced self-esteem, are other sources of their unmet emotional needs.Citation3,Citation4 It is important to identify and treat them, by offering psychological, dignity-conserving therapies and spiritual support.Citation3 Due to the severe symptom burden, patients may become obliged to quit their jobs or pay for household help.Citation3 Living with these constraints, together with the costs for home oxygen and medications, represent important unmet needs regarding financial support.Citation3,Citation4 Not only do COPD patients experience unmet needs, but also do their caregivers, family members, or those who are close to the patient. They may have their own needs and concerns. Therefore, to provide information about COPD and its management and to offer psychological care and support for the caregivers should not be neglected.Citation3
People with COPD often experience difficulties in accessing health-care professionals and health-care services, including community services.Citation4 The reasons are variable, from the scarce knowledge about the modalities and facilities to access the healthcare system in different situations, to the lack of communication between their family doctors and hospitals or the lack of dedicated services for transportation.Citation4
Another important unmet need in the care of COPD patients is the late referral in providing integrated palliative care. There is an increasing awareness about the need to have a greater access to PC services.Citation15,Citation18 Still, patients living with advanced forms of COPD are quite unlikely to get engaged in discussions with their doctors about end-of-life issues and the opportunity to receive palliative care services, including advance care planning (ACP) discussions.Citation16 Though studies on the effectiveness of ACP on subsequent care in COPD are limited, and future research is required, it showed improvement in the quality of communication.Citation3 Despite the communication barriers between doctors and patients, highlighted by the most guidelines/pathways, the referral criteria and timings are not only widely different, but also equivocal because some of them were mainly based on prognostication.Citation18 The wide variability and obstacles in accessing palliative care in different countries, including reimbursement issues,Citation15 the insufficient time claimed by clinicians or their reduced communication skills,Citation3 the focus especially on the terminal phases of the disease,Citation15 the lack of PC trained health-care staff or doctors who are not prepared to provide trained palliative care services, are other potential motifs for the late initiation of PC. In order to overcome these various barriers, proactive palliative care approaches may be early incorporated in the management of COPD.Citation15 The use of the “surprise question” can be a supplementary screening tool for the primary care physicians, to identify patients appropriate for proactive palliative care.Citation15 PC should not be limited to specialists in palliative care. Any physician involved in the care of patients living with COPD should be familiarized with PC. Primary care providers as well as pulmonologists should be trained and competent to identify the appropriateness of a patient who would benefit from proactive outpatient supportive care, as part of comprehensive COPD care.Citation15 Regardless of the care models included in the proactive PC approaches, such as the proactive primary care approach proposed by Vermylen et alCitation15 or the models of integrated PC outlined by Maddocks et al, all of them are focused more on the unmet needs of patients living with COPD, than on the prognosis.Citation3,Citation15 As potential models for integrative working with palliative care for COPD people, Maddocks et al proposed: refractory symptom triggered services (for example, for refractory breathlessness), short-term integrated PC (such as the Breathlessness Support Service), advanced COPD clinics, or Integrated Respiratory Care services (pulmonary rehabilitation, hospital at home).Citation3
The involvement of multidisciplinary PC teams, including physicians, disease specialists, nutritionists, physiotherapists, nurses, psychologists, psychiatrists, occupational therapists, social workers, chaplains, etc., and personnel additionally trained in PC,Citation3,Citation15,Citation18 was promoted in most of the guidelines/pathways, as noted by Siouta and colleagues.Citation18 The global approach of the multidimensional unmet needs of COPD patients, with early, longitudinal palliative care provided by an interdisciplinary team,Citation15 offers an improvement in the care of people living with COPD, including for those that do not correctly identify their needs.Citation4
Discussion
The present review, like other reviews involving the topic of palliative care,Citation18 included studies predominantly from the UK, probably because PC originated from the UK.Citation28
Despite the small number of studies included in our search, some important issues emerged. The barriers to the initiation of palliative care in people living with COPD are multidimensional. The referral criteria and timing for PC,Citation18 the appropriate identification of patients for referral to PC, prognostic variables and scores,Citation5,Citation17 the settings, the staffing, and the models to provide PC,Citation3,Citation15 alongside the complex unmet needs of patients with COPD,Citation3,Citation4 are topics much debated in the literature, including in recent years.Citation15,Citation16,Citation29
The unpredictability of the prognosis in an individual patientCitation15 is one of the main obstacles claimed for timely initiation of PC. Given that prognostication is difficult and inexact, the determination of the referral criteria should be independent of it.Citation18 Though there are more than 400 prognostic models, using a combination of different predictors for COPD related outcomes, a limited number were externally validated.Citation30 On the other hand, to decide which prognostic model is better to choose in different settings, geographical area, and individuals with COPD, even if it was externally validated, may be a challenge for physicians in daily practice.Citation30 Except for the updated 15-point ADO indexCitation31 and the model developed by Bertens et al,Citation32 which were not explored in the studies included in our search, the other prognostic variables like ADO, B-AE-D, and the updated BODE were also analyzed in the systematic review of Bellou et al which showed a low risk of bias for these prognostic models.Citation30 However, according to the data of AlmagroCitation17 and SmithCitation5 none of the prognostic variables and multicomponent indices that were identified offer sufficient reliability to predict 12 months of survival in COPD patients.Citation5,Citation17 A possible explanation is related to the fact that these prognostic factors are usually related to long-term survival; also, their applicability is hard to generalize in any COPD patient.Citation17 The need to move from prognostic paralysis to active total care should be taken into consideration.Citation33
The initiation of PC should not be based on life expectancy,Citation17 but rather on refractory, uncontrolled symptoms like breathlessness, fatigue, cough, called sometimes the respiratory cluster,Citation34 alongside the emotional, social, and spiritual needs and preferences of patients.Citation3,Citation4 The assessment of symptoms such as breathlessness is usually based on unidimensional validated tools or scales.Citation23 Measurement focused only on intensity may overlook the multidimensional nature of symptoms and miss valuable benefits of therapy, such as morphine therapy.Citation35 In order to perceive the clinically relevant improvement in more patients, the prompt assessment and the management of the side effects, which may outweigh the net benefits, are extremely important.Citation3,Citation35 Addressing breathlessness through a proactive palliative method had a positive impact not only on alleviating symptoms but also a potential benefit on the survival of COPD patients.Citation36 In the case that self-reported breathlessness cannot be assessed, proxy measurements from caregivers specialized in palliative care can be used for symptom management.Citation37
Palliative care is a holistic care focused on the whole person.Citation3 Alongside the distressing symptom burden, the multidimensional authentic needs of patients living with COPDCitation4 are other important barriers in offering PC integrated into the management of the disease, as early as the guidelines ideally advise.Citation38 Early recognition of the timing for PC is necessary, but not sufficient, for effective care.Citation33 The relationship between these unsatisfied needs, and prevention and management of the disease has been broadly addressed in the literature.Citation39,Citation40 Knowing the real dimensions in which COPD patients express their unsatisfied needs could lead to a better approach and care, even in individuals who overlook their needs.Citation4 Simple open questions addressed by primary care clinicians or specialists are aimed not only to improve communication barriers, but also to explore these issues with their patients.Citation15
On the other hand, the “surprise-question” (SQ) that physicians may ask themselves is: “Would I be surprised if my patients were to die in the next 12 months?” If the answer is “no,” this may be seen as an additional screening tool for the identification of the patients who would benefit from early proactive palliative care.Citation15,Citation16,Citation33 It is incorporated into clinical guidelines such as the National Institute for Health and Care Excellence (NICE) for End of Life CareCitation41 and included as part of the Gold Standard Framework (GSF) proactive identification guidance tool in the UK.Citation42 Though the predictive power of the SQ varies among clinicians, settings, and seniority,Citation43 its application in COPD was shown to be highly unreliable.Citation17 Moreover, recent data outlined important limitations in the use of the surprise question and clinician-related approaches.Citation44 Therefore, the role of the SQ should be carefully weighed by each physician. They should never forget that palliative care is appropriate for COPD patients at any point in their disease trajectory.Citation16
Study Limitations
Understandably the present review has some limitations. The use of a single selected database and the limitation on the language search could have led to the exclusion of studies on the topic of palliative care and prognosis in COPD patients. Another limitation of the review was the fact that all the results were from papers published in industrialized countries, meaning that different socio-cultures and health-care systems from the developing world were not represented and therefore the results may not be generalized. There is a need for larger prognostic studies, from different settings and forms of COPD, in order to limit the bias of the present review.
Conclusion
The barriers in offering timely integrated PC services to COPD patients are complex. Despite the identification of validated prognostic variables and multidimensional indices, none of them are sufficiently reliable to predict survival and implicit the moment to start PC in COPD patients. The decision to initiate PC should be rather based on the presence of refractory chronic symptoms and patients’ unmet needs and preferences. Despite the current advances, the ideal model to initiate longitudinal palliative care from the moment COPD is diagnosed, alongside the usual management of the disease and intensified care in the end-of-life stages, is a goal for clinicians trained in and capable of providing palliative care in any COPD patient.
Disclosure
The authors report no conflicts of interest in this work.
References
- Chronic respiratory diseases [homepage on the Internet]. Geneva: World Health Organization; 2020 Available from: https://www.who.int/health-topics/chronic-respiratory-diseases#tab=tab_1. Accessed 315, 2020.
- ChuchalinAG, KhaltaevN, AntonovNS, et al. Chronic respiratory diseases and risk factors in 12 regions of the Russian Federation. Int J Chron Obstruct Pulmon Dis. 2014;9:963. doi:10.2147/COPD.S6728325246783
- MaddocksM, LovellN, BoothS, ManWD, HigginsonIJ. Palliative care and management of troublesome symptoms for people with chronic obstructive pulmonary disease. Lancet. 2017;390(10098):988–1002. doi:10.1016/S0140-6736(17)32127-X28872031
- ClariM, IvzikuD, CasciaroR, MatareseM. The unmet needs of people with chronic obstructive pulmonary disease: a systematic review of qualitative findings. COPD. 2018;15(1):79–88. doi:10.1080/15412555.2017.141737329308932
- SmithLJ, MooreE, AliI, SmeethL, StoneP, QuintJK. Prognostic variables and scores identifying the end of life in COPD: a systematic review. Int J Chron Obstruct Pulmon Dis. 2017;12:2239. doi:10.2147/COPD.S13786828814852
- Public Health England. Palliative and end of life care: hospital deaths 2006 to 2017 [homepage on the Internet]; 2019 Available from: https://www.gov.uk/government/publications/palliative-and-end-of-life-care-hospital-deaths-2006-to-2017/palliative-and-end-of-life-care-hospital-deaths-2006-to-2017. Accessed 315, 2020.
- World Health Organization. Action plan of the Global alliance against chronic respiratory diseases, 2008–2013; 2008 Available from: https://apps.who.int/iris/bitstream/handle/10665/43984/9789241597203_eng.pdf?sequence=1&isAllowed=y. Accessed 315, 2020.
- HalpinDMG. Palliative care for chronic obstructive pulmonary disease. Signs of progress, but still a long way to go. Am J Respir Crit Care Med. 2018;198(11):1356‐1358. doi:10.1164/rccm.201805-0955ED
- World Health Organization. WHO definition of palliative care. Available from: http://www.who.int/cancer/palliative/definition/en/. Accessed 519, 2020.
- Al-MahreziA, Al-MandhariZ. Palliative care: time for action. Oman Med J. 2016;31(3):161–163. doi:10.5001/omj.2016.3227162584
- McVeighC, ReidJ, CarvalhoP. Healthcare professionals’ views of palliative care for American war veterans with non-malignant respiratory disease living in a rural area: a qualitative study. BMC Palliat Care. 2019;18(1):22. doi:10.1186/s12904-019-0408-730813937
- LankenPN, TerryPB, DeLisserHM, et al. An official American Thoracic Society clinical policy statement: palliative care for patients with respiratory diseases and critical illnesses. Am J Respir Crit Care Med. 2008;177(8):912–927. doi:10.1164/rccm.200605-587ST18390964
- ConnorSR, BermedoMC, editors. Global Atlas of Palliative Care at the End of Life. Worldwide Palliative Care Alliance; 2014.
- ShamseerL, MoherD, ClarkeM, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation. BMJ. 2015;349:g7647. doi:10.1136/bmj.g7647
- VermylenJH, SzmuilowiczE, KalhanR. Palliative care in COPD: an unmet area for quality improvement. Int J Chron Obstruct Pulmon Dis. 2015;10:1543. doi:10.2147/COPD.S7464126345486
- HarringtonSE, RogersE, DavisM. Palliative care and chronic obstructive pulmonary disease: where the lines meet. Curr Opin Pulm Med. 2017;23(2):154–160. doi:10.1097/MCP.000000000000035828009643
- AlmagroP, YunS, SangilA, et al. Palliative care and prognosis in COPD: a systematic review with a validation cohort. Int J Chron Obstruct Pulmon Dis. 2017;12:1721. doi:10.2147/COPD.S13565728652724
- SioutaN, van BeekK, PrestonN, et al. Towards integration of palliative care in patients with chronic heart failure and chronic obstructive pulmonary disease: a systematic literature review of European guidelines and pathways. BMC Palliat Care. 2016;15(1):18. doi:10.1186/s12904-016-0089-426872741
- ParryA, HigginsonR, GleesonA. End-of-life prognostic indicators in patients with COPD: part 2. Int J Palliat Nurs. 2016;22(11):560–567. doi:10.12968/ijpn.2016.22.11.56027885911
- CurtisJR. Palliative and end-of-life care for patients with severe COPD. Eur Respir J. 2008;32(3):796‐803. doi:10.1183/09031936.00126107
- BoeckL, SorianoJB, Brusse-KeizerM, et al. Prognostic assessment in COPD without lung function: the B-AE-D indices. Eur Respir J. 2016;47(6):1635‐1644. doi:10.1183/13993003.01485-2015
- BloomCI, RicciardiF, SmeethL, StoneP, QuintJK. Predicting COPD 1-year mortality using prognostic predictors routinely measured in primary care. BMC Med. 2019;17(1):73. doi:10.1186/s12916-019-1310-030947728
- EkströmM, CurrowDC, JohnsonMJ. Outcome measurement of refractory breathlessness: endpoints and important differences. Curr Opin Support Palliat Care. 2015;9(3):238–243. doi:10.1097/SPC.000000000000014726203849
- LeidyNK, SextonCC, JonesPW, et al. Measuring respiratory symptoms in clinical trials of COPD: reliability and validity of a daily diary. Thorax. 2014;69(5):443‐449. doi:10.1136/thoraxjnl-2013-204428
- WilcoxTK, ChenWH, HowardKA, et al. Item selection, reliability and validity of the Shortness of Breath with Daily Activities (SOBDA) questionnaire: a new outcome measure for evaluating dyspnea in chronic obstructive pulmonary disease. Health Qual Life Outcomes. 2013;11(1):196. doi:10.1186/1477-7525-11-19624229361
- YorkeJ, Lloyd-WilliamsM, SmithJ, et al. Management of the respiratory distress symptom cluster in lung cancer: a randomised controlled feasibility trial. Support Care Cancer. 2015;23(11):3373–3384. doi:10.1007/s00520-015-2810-x26111954
- BanzettRB, O’DonnellCR, GuilfoyleTE, et al. Multidimensional Dyspnea profile: an instrument for clinical and laboratory research. Eur Respir J. 2015;45(6):1681‐1691. doi:10.1183/09031936.00038914
- ClarkD. From margins to centre: a review of the history of palliative care in cancer. Lancet Oncol. 2007;8(5):430‐438. doi:10.1016/S1470-2045(07)70138-9
- LillyEJ, SenderovichH. Palliative care in chronic obstructive pulmonary disease. J Crit Care. 2016;35:150–154. doi:10.1016/j.jcrc.2016.05.01927481751
- BellouV, BelbasisL, KonstantinidisAK, TzoulakiI, EvangelouE. Prognostic models for outcome prediction in patients with chronic obstructive pulmonary disease: systematic review and critical appraisal. BMJ. 2019;367:l5358. doi:10.1136/bmj.l535831585960
- PuhanMA, HanselNN, SobradilloP, et al. Large-scale international validation of the ADO index in subjects with COPD: an individual subject data analysis of 10 cohorts. BMJ Open. 2012;2(6):e002152. doi:10.1136/bmjopen-2012-002152
- BertensLC, ReitsmaJB, MoonsKG, et al. Development and validation of a model to predict the risk of exacerbations in chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2013;8:493–499.24143086
- MurraySA, BoydK, SheikhA. Palliative care in chronic illness. BMJ. 2005;330(7492):611‐612.
- YorkeJ, SwigrisJ, RussellAM, et al. Dyspnea-12 is a valid and reliable measure of bre Ferreira DH, Silva JP, Quinn S, et al. Blinded patient preference for morphine compared to placebo in the setting of chronic refractory breathlessness–an exploratory study. J Pain Symptom Manage. 2016;51(2):247–254.26598037
- FerreiraDH, SilvaJP, QuinnS, et al. Blinded patient preference for morphine compared to placebo in the setting of chronic refractory breathlessness–an exploratory study. J Pain Symptom Manage. 2016;51(2):247–254. doi:10.1016/j.jpainsymman.2015.10.00526598037
- HigginsonIJ, BauseweinC, ReillyCC, et al. An integrated palliative and respiratory care service for patients with advanced disease and refractory breathlessness: a randomised controlled trial. Lancet Respir Med. 2014;2(12):979–987. doi:10.1016/S2213-2600(14)70226-725465642
- QuinnC, DunbarSB, HigginsM. Heart failure symptom assessment and management: can caregivers serve as proxy? J Cardiovasc Nurs. 2010;25(2):142. doi:10.1097/JCN.0b013e3181bf93a020168194
- NiciL, DonnerC, WoutersE, et al. American thoracic society/European respiratory society statement on pulmonary rehabilitation. Am J Respir Crit Care Med. 2006;173(12):1390–1413. doi:10.1164/rccm.200508-1211ST16760357
- Gruffydd-JonesK, Langley-JohnsonC, DyerC, BadlanK, WardS. What are the needs of patients following discharge from hospital after an acute exacerbation of chronic obstructive pulmonary disease (COPD)? Prim Care Respir J. 2007;16(6):363–368. doi:10.3132/pcrj.2007.0007518038104
- WongSS, AbdullahN, AbdullahA, et al. Unmet needs of patients with chronic obstructive pulmonary disease (COPD): a qualitative study on patients and doctors. BMC Fam Pract. 2014;15(1):6. doi:10.1186/1471-2296-15-6724405525
- National Institute for Health and Care Excellence. End of life care for adults; 2011 Available from: https://www.nice.org.uk/guidance/qs13. Accessed 520, 2020.
- ThomasK, Armstrong WilsonJ; GSF Team. Proactive identification guidance (PIG) national gold standards framework centre in end of life care; 2016 Available from: https://www.nice.org.uk/guidance/qs13. Accessed 519, 2020.
- Da Silva GaneM, BraunA, StottD, WellstedD, FarringtonK. How robust is the ‘surprise question’ in predicting short-term mortality risk in haemodialysis patients? Nephron Clin Pract. 2013;123(3–4):185‐193. doi:10.1159/000353735
- DownarJ, WegierP, TanuseputroP. Early identification of people who would benefit from a palliative approach-moving from surprise to routine. JAMA Netw Open. 2019;2(9):e1911146. doi:10.1001/jamanetworkopen.2019.1114631517959