Abstract
Background
We investigated a large population of patients with chronic obstructive pulmonary disease (COPD) to determine their frequency of medication use and patterns of pharmacotherapy.
Methods
Medical and pharmacy claims data were retrospectively analyzed from 19 health plans (>7.79 million members) across the US. Eligible patients were aged ≥40 years, continuously enrolled during July 2004 to June 2005, and had at least one inpatient or at least two outpatient claims coded for COPD. As a surrogate for severity of illness, COPD patients were stratified by complexity of illness using predefined International Classification of Diseases, Ninth Revision, Clinical Modification, Current Procedural Terminology, Fourth Edition, and Healthcare Common Procedure Coding System codes.
Results
A total of 42,565 patients with commercial insurance and 8507 Medicare patients were identified. Their mean age was 54.7 years and 74.8 years, and 48.7% and 46.9% were male, respectively. In total, 66.3% of commercial patients (n = 28,206) were not prescribed any maintenance COPD pharmacotherapy (59.1% no medication; 7.2% inhaled short-acting β2-agonist only). In the Medicare population, 70.9% (n = 6031) were not prescribed any maintenance COPD pharmacotherapy (66.0% no medication; 4.9% short-acting β2-agonist only). A subset of patients classified as high-complexity were similarly undertreated, with 58.7% (5358/9121) of commercial and 68.8% (1616/2350) of Medicare patients not prescribed maintenance COPD pharmacotherapy. Only 18.0% and 9.8% of diagnosed smokers in the commercial and Medicare cohorts had a claim for a smoking cessation intervention and just 16.6% and 23.5%, respectively, had claims for an influenza vaccination.
Conclusion
This study highlights a high degree of undertreatment of COPD in both commercial and Medicare patients, with most patients receiving no maintenance pharmacotherapy or influenza vaccination.
Introduction
The World Health Organization estimates chronic obstructive pulmonary disease (COPD) to be the fourth leading cause of death, accounting for at least 5% of all deaths worldwide (about 3.02 million).Citation1 This is likely an underestimate of COPD mortality, given that COPD patients often have a high number of comorbidities and complications,Citation2,Citation3 and airflow obstruction is an important contributor to other causes of morbidity and mortality.Citation4,Citation5
Advances in pharmacotherapy and improvements in COPD disease management have brought about the realization that COPD is a preventable and treatable disease.Citation2 These advances have also resulted in the development of COPD diagnosis and treatment guidelines,Citation6–Citation9 which are widely available to health care practitioners. Treatment guidelines aim to increase awareness of COPD and improve patient management and outcomes. For example, the Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines recommend that an effective COPD management plan should include assessment and monitoring of the disease, reduction in risk factors, management of stable COPD, and management of exacerbations.Citation9,Citation10
Despite the widespread availability of evidence-based guidelines, survey results suggest that practitioners have major gaps in their knowledge of the core elements of COPD management, with at least 50% reportedly unaware of guidelines for COPD diagnosis and treatment.Citation11 This lack of knowledge of recommended treatment may lead to suboptimal management of COPD patients in the primary care setting. COPD is a progressive illness with worsening symptoms, and therefore patients need to be actively prescribed appropriate therapies and to have ongoing assessments to manage their COPD and improve their health status.
In this retrospective analysis of managed care patients, we sought to document and evaluate patterns of medication utilization and medication-related assessments recorded for COPD patients. Medication utilization, adherence, and indicators of treatment and care were analyzed to assess treatment of COPD patients based on recognized guidelines. A subgroup of COPD patients with the most severe or complex COPD were identified and analyzed to determine if COPD severity changes the patterns of medication use in this cohort of commercial and Medicare patients.
Materials and methods
Study design
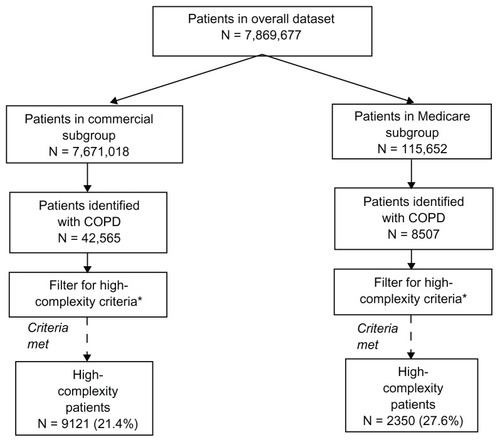
Continuously eligible populations from commercial, Medicare, and Medicaid membership of large, national US health plans including 12.4 million covered lives were identified from the PharMetrics database (Watertown, MA). The database included 19 health plans across the US: 3.2 million from the Northeast, 6.4 million from the Midwest, 1.8 million from the South, and 0.7 million from the West. The plans varied in size: six were <200,000 covered lives, nine were between 200,001 and one million covered lives, and four were over one million covered lives.Citation12 Pharmacy and medical claims from the 7.79 million members who were continuously eligible during the study period (July 2004 and June 2005) were retrospectively analyzed for COPD cohorts. Medicaid (a government-funded program primarily for indigent younger adults and children) claims data were analyzed, but are not reported here because only 485 of 83,007 patients were identified as having COPD. Patient stratification is outlined in . The commercial population represented employees and their eligible dependants from employer-based health insurance product offerings, including health maintenance organization, preferred provider organization, and point of service plans. Medicare is a government-sponsored health care program for patients aged ≥65 years and for others with certain disabilities. The Medicare population in this analysis includes persons who chose to have this benefit managed by a private insurance company. Additional details of the populations studied in this analysis have been reported elsewhere.Citation12
Figure 1 Flow of patients through the study. Complexity is used as a surrogate for COPD disease severity, and methodology for classification is described in full elsewhere.Citation12
Identification of populations
Patients were identified as having COPD if they were aged ≥40 years and had any one of the following:
One inpatient hospitalization or one emergency room encounter with a COPD diagnosis (2004 International Classification of Diseases, Ninth Revision, Clinical Modification [ICD-9-CM] codes 491.x [chronic bronchitis], 492.x [emphysema], or 496 [chronic airway obstruction]) listed in any position as a discharge diagnosis
Two professional claims, with different dates of services, with a COPD diagnosis listed in any position
A COPD-related surgical procedure (eg, lung volume reduction) listed on either a professional or facility claim. COPD-related surgical procedures included open excision plication of bullae of lung, open excision plication of emphysematous lung(s) for lung volume reduction, and thoracoscopy with excision plication of bullae of lung.
Medication utilization
Use of COPD medication(s) was analyzed during the one-year period based on pharmacy claims in the datasets. A patient was considered to be taking a medication if they had at least one filled prescription for that medication product during the one-year study period. The following medications were considered maintenance COPD pharmacotherapy: long-acting β2-agonist bronchodilators (LABA), short-acting or long-acting anticholinergic bronchodilators (SAAC and LAAC, respectively), methylxanthine bronchodilators (theophylline), and inhaled corticosteroids. As per the GOLD guidelines, short-acting β2-agonists (SABAs) were considered symptomatic medications or rescue drugs.Citation10 Medication utilization is reported in two ways:
Medications of interest, which represent the number of COPD patients who filled at least one prescription for a defined medication class (or fixed-dose combination) of a respiratory or nonrespiratory medication (eg, antimicrobials, narcotic analgesics, diuretics, antidepressants, anxiolytics/sedatives, gastrointestinal antisecretory/antiulcer agents, β-blockers, antihistamines [not part of cough/cold preparations], smoking deterrents/nicotine replacements, gastrointestinal promotility agents, antiarrhythmia agents) during the one-year study period. Reporting in this manner is not mutually exclusive and patients could be receiving more than one medication of interest.
Medication patterns, which represent the number of COPD patients who filled at least one prescription for each defined respiratory drug class or drug class combination during the one-year study period. Reporting in this manner is mutually exclusive and patients could only be classified as receiving one medication pattern. Medication patterns are used to evaluate the proportion of patients who received single or multiple maintenance COPD medications and for identifying patients receiving single or multiple therapies during the one-year study period as well as those receiving no therapy or SABA therapy alone.
To illustrate the differences between these two methods of reporting, a patient who received an inhaled anticholinergic and an inhaled corticosteroid during the study period was reported in both classes in medications of interest, but only in the anticholinergic + inhaled corticosteroid category of medication patterns.
In order to characterize further medication use in this population of COPD patients, the following were also assessed: claims for smoking cessation therapy in COPD patients documented to be current smokers (based on current tobacco use using ICD-9-CM codes); use of a maintenance COPD pharmacotherapy within 45 days following a hospitalization for a COPD exacerbation;Citation13 and proportion of patients vaccinated against influenza.
High-complexity criteria for medication pattern reporting
The guidelines are clear that patients with more severe disease should receive maintenance COPD pharmacotherapy.Citation10 We therefore conducted an analysis of a subset with likely more severe disease. Claims data do not contain pulmonary function test values, and it was therefore not possible to assess COPD severity according to the GOLD guidelines.Citation10 Instead, a claims-based classification of COPD complexity was used to serve as a surrogate for COPD disease severity. The methodology for this has been described fully elsewhere.Citation12 For this analysis, comorbid respiratory conditions and medical procedures occurring during the study period were used to assign patients to a high complexity subset, based on selected diagnostic, therapeutic, procedures, and services codes (2004 ICD-9-CM, Current Procedural Terminology, Fourth Edition, and Healthcare Common Procedure Coding System).Citation12 For example, a patient with a claim for tuberculosis, malignant neoplasm, or cor pulmonale was classified as high complexity. A medications patterns analysis is reported for this high-complexity subset.
Adherence
Adherence to prescribed medications was estimated using pharmacy claims by calculating a medication possession ratio (MPR), defined as the total days of medication supplied in all prescription fills/total days between the first and last fill + days supplied in last prescription. MPR is a commonly used metric to assess adherence/compliance.Citation14 Adherence with noninhaled medications (tablets, capsules, liquids) was calculated using the actual reported days of supply from the claims data. However, because the days of supply reported in pharmacy claims for inhaled medication prescriptions is often unreliable, the number of “days supplied” for inhaled medications was assigned a value based on average adult doses (in number of puffs) for each product and the number of puffs per container. Adherence to each respiratory medication is reported as the average MPR for all patients receiving two or more prescriptions of a relevant medication. MPR was only calculated for maintenance COPD medications.
Data collection and outcome measures
DTEC™ software (Version 3.3, Pfizer, New York, NY) was used to integrate administrative data and claims files, identify and stratify patients with COPD, as well as to characterize demographics, comorbidities (respiratory and nonrespiratory), and utilization of medications. All analyses were specified prior to the study and programmed in the software.Citation12 These analyses, including rationale for complexity stratification, were developed by a panel of experts including pulmonologists, outcomes researchers, and claims-based research consultants.Citation12 They were developed based on information from accepted guidelines,Citation9,Citation15 but also incorporate the previous experiences of the panel in claims-based research. While DTEC (a proprietary software program) was used for these analyses, the algorithms for the data reported have been specifically outlined and published previously,Citation12 in order that they may be used in other claims querying systems.
Claims data during the 1-year study period were analyzed and are presented as means with standard deviations. Categorical data are presented as numbers and percentages. The database was compiled in accordance with all aspects of the Health Information Portability and Accountability Act of 1996.
Results
Identification of COPD population
Of the 7,869,677 patients in the overall dataset, 42,565 commercial and 8507 Medicare patients were identified as having COPD (). Among these two groups, 21.4% of commercial (9121/42,565) and 27.6% of Medicare patients (2350/8507) were categorized as high-complexity, based on comorbid respiratory and nonrespiratory conditions and claims for procedures and services.Citation12
Population characteristics
Patients with COPD from the commercial and Medicare data sets had a mean age of 54.7 years and 74.8 years, respectively, and approximately half were male (). The most common comorbidity was hypertension in both data sets (55.2% commercial; 71.6% Medicare) followed by dyslipidemia (48.2% commercial; 47.3% Medicare). The majority of patients recorded at least one office visit/consultation (98.7% commercial; 96.4% Medicare) with a mean of 11.3 visits in the commercial group and 11.5 visits in the Medicare group during the one-year study period. More than half (53.9%) of the Medicare cohort and nearly 40% of the commercial cohort (39.8%) were hospitalized at least once for any reason during the study period. In total, 1651 Medicare patients (19.4%) and 5922 commercial patients (13.9%) were hospitalized at least once due to COPD. Additional details describing these COPD populations have been published in full elsewhere.Citation12
Table 1 Patient characteristics
Medication utilization
Medications of interest
The proportion of COPD patients in the commercial and Medicare populations receiving different classes of respiratory and nonrespiratory drugs are shown in . Oral corticosteroids and SABAs were the most commonly filled respiratory medications in commercial (30.1%; 30.0%) and Medicare (20.9%; 25.5%) populations, respectively. Systemic antibiotics or antimicrobials were the most common non-COPD medications used in both data sets, prescribed to 57.7% and 40.2% of the commercial and Medicare populations, respectively.
Table 2 Medications of interest: COPD patients
Medication patterns
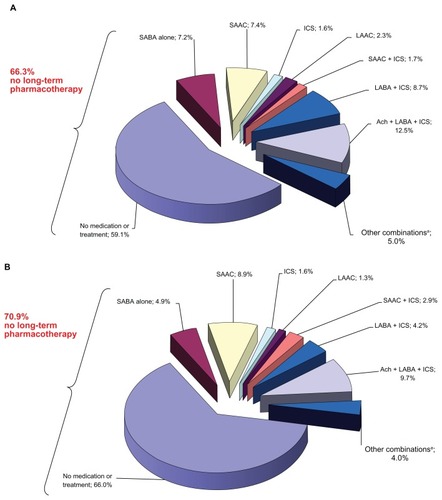
shows patterns of medication use, and indicates that the majority of patients in both cohorts did not receive any maintenance COPD pharmacotherapy. shows that 66.3% of commercial patients (n = 28,206) received no maintenance COPD pharmacotherapy, including 25,157/42,565 (59.1%) prescribed no COPD medications and 3049/42,565 (7.2%) prescribed only inhaled SABAs. shows that 70.9% of Medicare patients (n = 6376) received no maintenance COPD pharmacotherapy, including 5615/8507 (66.0%) prescribed no COPD medications, and 416/8507 (4.9%) prescribed SABA only.
Figure 2 Respiratory medication patterns in COPD patientsa. (A) Commercial (n = 42,565) and (B) Medicare (n = 8507).
Abbreviations: Ach, anticholinergics; ICS, inhaled corticosteroid; LAAC, long-acting anticholinergic; LABA, long-acting β2-agonist inhaled bronchodilator; SAAC, short-acting anticholinergic; SABA, short-acting β2-agonist bronchodilator.
High-complexity criteria for medication pattern reporting
In order to evaluate medication utilization in patients with a high number of comorbidities who were more likely to be severe and compromised, we performed a similar evaluation for COPD patients who met criteria for high complexity (as a surrogate for COPD severity)Citation12 and found similar trends. More than half of all high-complexity patients were not prescribed maintenance COPD pharmacotherapy. For the commercial population, 5358 (58.7%) of high-complexity patients did not receive any maintenance COPD pharmacotherapy, including 4756 (52.1%) receiving no COPD medications and 602 (6.6%) receiving SABAs only. Similarly, 68.8% (1616/2350) high-complexity Medicare patients did not receive any maintenance COPD pharmacotherapy, including 1504/2350 (64.0%) receiving no COPD medication and 112/2350 (4.8%) receiving SABAs only.
Treatment measures
The evaluation of other measures of treatment also highlighted that COPD in both cohorts was often managed suboptimally. For example, smoking deterrents/nicotine replacement products were prescribed to less than 10% of patients in either population (commercial 9.4% [3990/42,565] versus Medicare 2.8% [234/8507]). Indeed, of the commercial and Medicare patients diagnosed as smokers, only 18.0% (n = 1466/8104) and 9.8% (n = 62/636), respectively, had a claim for a smoking cessation intervention (medication or behavioral therapy) during the one-year study period. Among patients hospitalized for COPD, less than half of the commercial cohort (40.2% [1912/4757] were prescribed bronchodilator therapy within 45 days following their hospitalization, and fewer still (29.9% [359/1200]) of the older Medicare cohort. Furthermore, despite guidelines recommending vaccination against influenza as a risk reduction strategy for all patients with COPD, only 7070 patients (16.6%) in the commercial cohort and 1996 patients (23.5%) in the Medicare cohort were documented to have received the vaccine.
Adherence
Medication adherence (reported as mean MPR by drug class) is provided in . While adherence was above 50% for each respiratory medication class for both cohorts, acceptable adherence (MPR ≥ 80%)Citation14 was only achieved for the oral drug classes (leukotriene modifiers and theophylline). Among the inhaled agents, LAAC and LABA had the highest average adherence, while SAAC had the lowest.
Table 3 Adherence (shown as average medication possession ratio) to COPD-related medications in commercial and Medicare datasets
Discussion
This analysis of more than 51,000 patients highlights significant undertreatment of COPD in typical US commercial and Medicare populations. The majority of diagnosed COPD patients remain undertreated with no maintenance COPD pharmacotherapy for their COPD over the one-year study period.
Inhaled bronchodilators are the accepted f irst-line therapies for symptomatic COPD management, because regular use can increase exercise capacity and improve health status.Citation9,Citation16,Citation17 However, in the present analysis, more than two-thirds of COPD patients in the commercial population and >70% of the Medicare population were not prescribed any long-term maintenance COPD medications. Because patients with mild COPD may appropriately not be prescribed long-term therapy according to GOLD guidelines, we also evaluated subsets of patients classified as “high-complexity,” where complexity served as a surrogate for disease severity and represented patients with the highest number of comorbid conditions and complications.Citation12 More than half of high-complexity commercial and 69% of high-complexity Medicare patients failed to receive any maintenance COPD pharmacotherapies. Although clinicians may be less likely to prescribe chronic COPD pharmacotherapy to older patients receiving multiple medications who may have cognitive impairment or difficulty using inhalers, the observation that 70% of older patients, such as those represented by the Medicare cohort, and 60% of high-complexity Medicare patients, did not receive even one long-term COPD pharmacotherapy is a cause for concern.
The effectiveness of recommended treatment regimens is dependent on how well patients adhere with them. Adherence to COPD medications in the present study based on medication refills was only about 50%, which is comparable with other studies,Citation18,Citation19 but still suboptimal for patients to derive benefit from therapies being prescribed.
Our findings are particularly noteworthy given recommended guidelines outlining a clear strategy for COPD and the management of associated exacerbations.Citation7,Citation9,Citation10,Citation20 In addition, recent large, multiyear studies have shown therapies such as LAACs and LABA/inhaled corticosteroid combinations used chronically offer significant benefits to COPD patients, including a reduction in exacerbation frequency and possibly a reduction in mortality.Citation21,Citation22 The undermanagement highlighted here is in agreement with a survey of primary care physicians, which reported that only 35% of physicians chose a long-acting bronchodilator (recommended by GOLD)Citation10 if use of a short-acting agent had failed to manage a patient’s COPD symptoms.Citation23 Furthermore, although 55% of physicians were aware of major COPD guidelines (GOLD or American Thoracic Society/European Respiratory Society guidelines), only 25% used them to guide decision-making.Citation23
In addition to highlighting the suboptimal prescription of COPD medications, we also found suboptimal use of certain non-COPD maintenance pharmacotherapies. Less than 20% of COPD patients in this study were documented to have received an influenza vaccine, despite vaccination being recommended for all COPD patients to reduce exacerbation frequency.Citation9 In addition, 82% of patients reported to be current smokers in the commercial dataset did not receive any smoking cessation intervention. Similarly, 90% of current smokers in the Medicare population did not receive smoking cessation interventions. The majority of COPD cases can be attributed to tobacco smoking,Citation2 and smoking cessation has been shown to be the most effective method of slowing the progression of COPD.Citation9,Citation10,Citation24 The evidence indicates that smoking cessation interventions, including non-nicotine pharmacotherapy,Citation25,Citation26 or nicotine replacement therapy,Citation27 combined with counseling, are both effective and cost-effective.Citation28–Citation30
Our data should be interpreted in light of certain limitations. As with any retrospective database study, the COPD diagnosis for patients in the present study was established by the presence of claims coded for this diagnosis from health care providers, and no spirometry results are available to verify diagnosis or assess disease severity. We compensated for the latter using a surrogate, ie, COPD complexity, for severity using service and procedure codes and comorbid conditions selected by a panel of experts. It is possible that there is under-reporting of medication utilization because the study was limited to a one-year period, and newly diagnosed patients near the end of the inclusion period may not have had time to begin drug therapy. However, our sensitivity analyses using high-complexity patients showed similar underuse of COPD medications in this subgroup as per the whole cohort. Some diagnoses and therapies are consistently under-reported in claims data, including smoking and antismoking medications, since many health care plans do not cover these medications. Therefore, the proportion of patients recorded as smokers or taking smoking cessation therapies in the current study may actually be an under-representation. While this study primarily evaluates treatment with pharmacotherapy, other therapies are important in the treatment of COPD. Other health care utilization in this population including hospitalization and outpatient services such as respiratory-related equipment and supplies (including oxygen) and respiratory therapy services (including assisted ventilation) have been reported elsewhere.Citation12 A detailed analysis of oxygen therapy in a US managed care population has also been reported previously.Citation31
Medication adherence was estimated using reasonable assumptions for patients who filled more than two prescriptions. Patients who filled only one prescription and could be, therefore, nonadherent, were not included in the calculation. Our method of estimating the number of “days supplied” for inhaled drugs based upon recommended doses and number of puffs/inhaler,Citation32 could be inaccurate in patients on unusual doses. While these assumptions are reasonable for the population as a whole, unusual dosing in a specific patient could result in inaccurate MPRs. We cannot account for prescriptions that were filled but not taken by the patient, or for medication samples that may have been dispensed by the health plan physicians, because these are not accounted for in claims data. Because the study was a cross-sectional analysis, no cause and effect analyses could be conducted. Analysis of the management of comorbid conditions was beyond the scope of this analysis.
Our study used data from 2004 to 2005, prior to the publication of landmark studies, such as the Towards a Revolution in COPD Health (TORCH) and the Understanding Potential Long-Term Impacts on Function with Tiotropium (UPLIFT®) studies,Citation21,Citation22 which demonstrated significant benefits of providing maintenance pharmacotherapy for COPD.Citation33 Although we hope that the undertreatment documented in the present study has improved with the publication of these studies, the magnitude of our findings and their consistency with other reportsCitation34,Citation35 make it very likely that a significant problem with the undermanagement of COPD patients still exists.
Conclusion
This study highlights marked undertreatment of COPD in both commercial and Medicare managed care populations. The majority of patients with COPD, even those with a high number of comorbidities, were untreated with respiratory medications. Adherence with COPD therapies was suboptimal, and related therapies, such as smoking cessation and influenza vaccinations, were underprescribed. These findings suggest that there is significant opportunity to improve the lives of patients with COPD with appropriate treatment. A major educational effort is needed to disseminate evidence-based guidelines supported by recent landmark trials to health care providers, and educate providers and patients on the long-term benefits of appropriately treating COPD.
Disclosure
This study was sponsored by Pfizer Inc. Medical writing support was provided by Karen Burrows and Jon Edwards of UBC Scientific Solutions and funded by Pfizer Inc. BM has participated in advisory boards and received honoraria for speaking from Pfizer Inc within the past 5 years. MPD and JPM are employees of and have stock options in Pfizer Inc. RP-R was an employee of Pfizer Inc at the time of the study. DWM was a paid consultant to Pfizer Inc in connection with conduct of the analysis and development of the manuscript. DWM has served as a consultant to and received research funding from Pfizer Inc, GlaxoSmithKline, and AstraZeneca. Parts of these data were presented at the American Thoracic Society meeting, May 22, 2007, San Francisco, CA.
References
- World Health Organization (WHO)World Health Statistics 2008COPD predicted to be third leading cause of death in 2030GenevaWHO2008 Available at: http://www.who.int/respiratory/copd/World_Health_Statistics_2008/en/index.htmlAccessed January 13, 2011
- ManninoDMBuistASGlobal burden of COPD: risk factors, prevalence, and future trendsLancet2007370958976577317765526
- SinDDAnthonisenNRSorianoJBAgustiAGMortality in COPD: role of comorbiditiesEur Respir J20062861245125717138679
- TockmanMSAnthonisenNRWrightECDonithanMGAirways obstruction and the risk for lung cancerAnn Intern Med198710645125183826952
- SinDDManSFWhy are patients with chronic obstructive pulmonary disease at increased risk of cardiovascular diseases? The potential role of systemic inflammation in chronic obstructive pulmonary diseaseCirculation2003107111514151912654609
- National Collaborating Center for Chronic ConditionsChronic obstructive pulmonary disease. National clinical guideline on management of chronic obstructive pulmonary disease in adults in primary and secondary careThorax200459Suppl 11232
- CelliBRMacNeeWStandards for the diagnosis and treatment of patients with COPD: a summary of the ATS/ERS position paperEur Respir J200423693294615219010
- O’DonnellDEHernandezPKaplanACanadian Thoracic Society recommendations for management of chronic obstructive pulmonary disease – 2008 update – highlights for primary careCan Respir J200815Suppl A1A8A
- Global Initiative for Chronic Obstructive Lung Disease (GOLD)Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease (updated 2010 Available at: http://www.goldcopd.org/uploads/users/files/GOLDReport_April112011.pdfAccessed January 13, 2011
- PauwelsRABuistASCalverleyPMJenkinsCRHurdSSGlobal strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. NHLBI/WHO Global Initiative for Chronic Obstructive Lung Disease (GOLD) Workshop summaryAm J Respir Crit Care Med200116351256127611316667
- RutschmannOTJanssensJPVermeulenBSarasinFPKnowledge of guidelines for the management of COPD: a survey of primary care physiciansRespir Med2004981093293715481268
- MapelDWDutroMPMartonJPWoodruffKMakeBIdentifying and characterizing COPD patients in US managed care – a retrospective, cross-sectional analysis of administrative claims dataBMC Health Serv Res20111114321345188
- StollerJKClinical practice. Acute exacerbations of chronic obstructive pulmonary diseaseN Engl J Med20023461398899411919309
- HalpernMTKhanZMSchmierJKRecommendations for evaluating compliance and persistence with hypertension therapy using retrospective dataHypertension20064761039104816651464
- American Thoracic Society/European Respiratory Society Task ForceStandards for the Diagnosis and Management of Patients with COPD. updated September 8, 2005 Available at: http://www.thoracic.org/go/copdAccessed January 13, 2011
- NederJAFuldJPOverendTEffects of formoterol on exercise tolerance in severely disabled patients with COPDRespir Med2007101102056206417658249
- LieskerJJVan De VeldeVMeysmanMEffects of formoterol (Oxis Turbuhaler) and ipratropium on exercise capacity in patients with COPDRespir Med200296855956612195835
- DolceJJCrispCManzellaBRichardsJMHardinJMBaileyWCMedication adherence patterns in chronic obstructive pulmonary diseaseChest19919948378412009784
- KrigsmanKNilssonJLRingLAdherence to multiple drug therapies: refill adherence to concomitant use of diabetes and asthma/COPD medicationPharmacoepidemiol Drug Saf200716101120112817566142
- The COPD Guidelines Group of the Standards of Care Committee of the BTSBTS guidelines for the management of chronic obstructive pulmonary diseaseThorax199752Suppl 51289039230
- TashkinDPCelliBSennSA 4-year trial of tiotropium in chronic obstructive pulmonary diseaseN Engl J Med2008359151543155418836213
- CalverleyPMAndersonJACelliBSalmeterol and fluticasone propionate and survival in chronic obstructive pulmonary diseaseN Engl J Med2007356877578917314337
- FosterJAYawnBPMaziarAJenkinsTRennardSICasebeerLEnhancing COPD management in primary care settingsMed Gen Med20079324
- AnthonisenNRConnettJEKileyJPEffects of smoking intervention and the use of an inhaled anticholinergic bronchodilator on the rate of decline of FEV1. The Lung Health StudyJAMA199427219149715057966841
- WagenaEJKnipschildPGHuibersMJWoutersEFvan SchayckCPEfficacy of bupropion and nortriptyline for smoking cessation among people at risk for or with chronic obstructive pulmonary diseaseArch Intern Med2005165192286229216246996
- TashkinDPRennardSHaysJTMaWLawrenceDLeeTCEffects of varenicline on smoking cessation in patients with mild to moderate COPD: a randomized controlled trialChest2011139359159920864613
- WestRZhouXIs nicotine replacement therapy for smoking cessation effective in the “real world”? Findings from a prospective multinational cohort studyThorax20076211998100217573444
- HoogendoornMFeenstraTLHoogenveenRTRutten-van MolkenMPLong-term effectiveness and cost-effectiveness of smoking cessation interventions in patients with COPDThorax201065871171820685746
- HowardPKnightCBolerABakerCCost-utility analysis of varenicline versus existing smoking cessation strategies using the BENESCO simulation model: Application to a population of US adult smokersPharmacoeconomics200826649751118489200
- WagenaEJvan der MeerRMOsteloRJJacobsJEvan SchayckCPThe efficacy of smoking cessation strategies in people with chronic obstructive pulmonary disease: results from a systematic reviewRespir Med200498980581515338790
- MapelDWRobinsonSBLydickEA comparison of health-care costs in patients with chronic obstructive pulmonary disease using lightweight portable oxygen systems versus traditional compressed-oxygen systemsRespir Care20085391169117518718034
- US Food and Drug AdministrationThe National Drug Code DirectoryDepartment of Health and Human Services Available at: http://www.fda.gov/cder/ndc/Accessed August 3, 2011
- NiewoehnerDETORCH and UPLIFT: what has been learned from the COPD “mega-trials”?COPD2009611319229702
- MillerRMGeorgeDHalbertRJImproving the management of chronic obstructive pulmonary diseaseJ Healthc Qual2005272424716190311
- FromerLBarnesTGarveyCOrtizGSaverDFYawnBInnovations to achieve excellence in COPD diagnosis and treatment in primary carePostgrad Med2010122515016420861599