Abstract
Background
The choice between lower limit of normal or fixed value of forced expiratory volume in one second/forced vital capacity ratio (FEV1/FVC) < 0.70 as the criterion for confirming airway obstruction is an open issue. In this study, we compared the criteria of lower limit of normal and fixed FEV1/FVC for diagnosis of airway obstruction, with a focus on healthy elderly people.
Methods
We selected 367 healthy nonsmoking subjects aged 65–93 years from 1971 participants in the population-based SARA (Salute Respiratoria nell’Anziano, Italian for “Respiratory Health in the Elderly”) study, analyzed their spirometric data, and tested the relationship between spirometric indices and anthropometric variables. The lower limit of normal for FEV1/FVC was calculated as the fifth percentile of the normal distribution for selected subjects.
Results
While FEV1 and FVC decreased significantly with aging, the relationship between FEV1/FVC and age was not statistically significant in men or women. The lower limit of normal for FEV1/FVC was 0.65 in men and 0.67 in women. Fifty-five participants (15%) had FEV1/FVC < 0.70 and would have been inappropriately classified as obstructed according to the Global Initiative for Obstructive Lung Disease, American Thoracic Society/European Respiratory Society, and Canadian guidelines on chronic obstructive pulmonary disease. By applying different FEV1/FVC thresholds for the different age groups, as previously proposed in the literature, (0.70 for <70 years, 0.65 for 70–80 years, and 0.60 for >80 years) the percentage of patients classified as obstructed decreased to 6%. No subjects older than 80 years had an FEV1/FVC < 0.60.
Conclusion
The present results confirm the inadequacy of FEV1/FVC < 0.70 as a diagnostic criterion for airway obstruction after the age of 65 years. FEV1/FVC < 0.65 and <0.67 (for men and women, respectively) could identify subjects with airway obstruction in such a population. Further reduction of the threshold after 80 years is not justified.
Introduction
The most appropriate way to diagnose airway obstruction is currently the subject of heated debate.Citation1–Citation10 Most national and international chronic obstructive pulmonary disease (COPD) guidelines recommend to use a forced expiratory volume in one second/forced vital capacity ratio (FEV1/FVC) of 0.70 as a suitable threshold value to define the presence of an obstructive ventilatory defect. Commonly used guidelines include those of the Global Initiative for Obstructive Lung Disease (GOLD),Citation11 the American Thoracic Society/European Respiratory Society,Citation12 the British Thoracic Society,Citation13 the Canadian Thoracic Society,Citation14 and the National Institute for Health and Clinical Excellence.Citation15
However, there is evidence that the fixed cut-off value of 0.70 for FEV1/FVC becomes less specific in males aged > 40 years and females > 50 years, implying a risk of overestimation of airway obstruction. This is due to an age-related decline in pulmonary volumes, particularly in FEV1, which is observed even in healthy people with no history of exposure to noxious particles or gases.Citation16–Citation19 Proposed strategies for reducing the misclassification of airway obstruction include use of the lower limit of normal for FEV1/FVC, calculated as the fifth percentile of the normal distribution in a healthy population,Citation20–Citation22 or the use of different FEV1/FVC thresholds for different age groups (eg, 0.70 for subjects aged < 70 years, 0.65 for those aged 70–80 years, and 0.60 for those aged > 80 years).Citation19
On this basis, a group of colleagues involved in respiratory research and/or the diagnosis and treatment of lung diseases recently wrote an open letter to members of the GOLD committee inviting them to change the method by which airway obstruction is defined and asking for retraction of the fixed ratio in favor of the lower limit of normal.Citation1
The aim of the present study was to provide additional information for determination of the most appropriate spirometric criteria for confirming airway obstruction in the elderly, by describing lung function and calculating the lower limit of normal for FEV1/FVC in healthy nonsmoking elderly subjects (age > 65 years) who participated in the Italian multicenter SARA (acronym of Salute Respiratoria nell’Anziano, Italian for “Respiratory Health in the Elderly”) study. The degree of potential misclassification relative to use of 0.70 or other proposed fixed thresholds for FEV1/FVC was also evaluated.
Materials and methods
We performed a cross-sectional analysis of data from the SARA study, the design of which, along with technical characteristics of instruments as well as training of operators and results of quality control of spirometry, have been described in detail elsewhere.Citation23 Briefly, the study involved 24 pulmonary or geriatric institutions distributed throughout Italy. A total of 1971 subjects aged 65–100 years were recruited as consecutive outpatients referred between January 1996 and December 1997 to the participating centers (see Appendix). The study design was approved by the ethics committee of the University of Palermo. Patients gave their written consent to participate in the study.
Lung function was measured using an identical fully computerized water-sealed Stead-Wells spirometer (Baires System, Biomedin, Padua, Italy) by specifically trained and certified personnel supervised by a rigorous real-time control of acceptability and repeatabilityCitation23 according to American Thoracic Society recommendations.Citation24 FVC maneuvers were performed with the patient sitting. The largest FVC and FEV1 were selected from a minimum of two acceptable tests. The FEV1/FVC ratio was calculated on the basis of the highest values of individual parameters obtained in the acceptable curves for each subject. Analyses were conducted only on patients with good repeatability of the above-mentioned indices (difference between two best values < 150 mL).Citation25
Of the 1870 subjects who performed spirometry, we selected only those without any previous or present diagnosis or any sign or symptom suggestive of respiratory diseases according to the modified International Union against Tuberculosis and Lung Disease bronchial symptoms questionnaire.Citation25,Citation26 Current smokers and previous smokers with a smoking exposure > 5 pack/year were excluded, since the <5 pack/year smoking exposure was not significantly associated with decreased lung function.Citation27 Additional exclusion criteria were: severe hepatic failure; severe renal failure; severe cardiac failure; cognitive and/or sensory impairment severe enough to affect a multidimensional assessment; severe kyphoscoliosis with occiput wall distance (distance between the occiput and the wall when the patient stands with heels and shoulder against the wall with the back straight) >10; occurrence of a major psychosocial event (eg, bereavement) within the past 6 months; and hospitalization for any reason within the past 6 months. We further excluded individuals who had hypertension (diastolic pressure ≥90 mmHg and/or systolic pressure ≥160 mmHg), diabetes, and/or major electrocardiographic abnormalities.
Statistical analyses were performed using SPSS (SPSS Inc, Chicago, IL) and Stata (Stata Corporation, College Station, TX) software packages. Regression models were used for testing the relationship between spirometric indices and anthropometric variables. Based on the recommendations from the American Thoracic Society/European Respiratory Society task force,Citation22 the lower limit of normal for FEV1/FVC was estimated as the fifth percentile of its frequency distribution. To evaluate the effect of aging on spirometric measures independently of body height, FEV1 and FVC were normalized for height at the third power.Citation28,Citation29
Results
After applying the above-mentioned selection criteria, our final data set consisted of 367 healthy, nonsmoking subjects. One hundred and one subjects were excluded for lack of availability of lung function testing, a further 709 subjects because of a history of respiratory disease, 445 for significant smoking exposure (>5 pack/year), 262 for inadequate quality of spirometry, and 87 for the above-mentioned additional exclusion criteria.
and show anthropometric and functional data for the sample and distribution of the participants according to age and gender. Although the most advanced ages were less represented, a total of 73 subjects aged 80 years and over were included. The sample consisted of 314 never-smokers (85.6%) and 53 former-smokers with a smoking exposure from 0.15 to 5 pack-years (mean ± standard deviation, 2.75 ± 1.5).
Table 1 Anthropometric and functional characteristics of the study sample, with data expressed as the mean ± standard deviation
Table 2 Distribution of subjects according to gender and age group, with data presented as n (%)
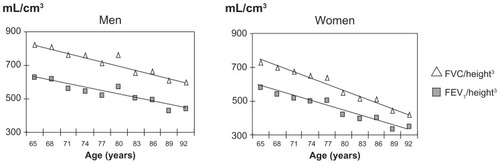
As shown in , the values of FEV1/FVC showed a normal frequency distribution. The mean FEV1/FVC was 0.75 ± 0.6 in males and 0.78 ± 0.6 in females, whereas the corresponding fifth percentiles were 0.65 and 0.67, respectively, in males and females. FEV1 and FVC significantly decreased with age (r = −0.38 and −0.35; P < 0.001), while FEV1/FVC, was not significantly correlated with age or height in either gender group over the considered range of age (lowest P = 0.103). As a consequence, there was no rationale to develop reference equations for FEV1/FVC, with age or height as independent variables in this restricted range of age. shows the decline in FEV1 and FVC with increasing age observed in the study sample in men and women, after normalization for height.
Figure 1 Distribution and fifth percentile of FEV1/FVC by gender (Caucasian Southern Europeans > 65 years).
Note: Asterisks indicate the 5th percentile.
Abbreviations: FEV1, forced expiratory volume in one second; FVC, forced vital capacity.
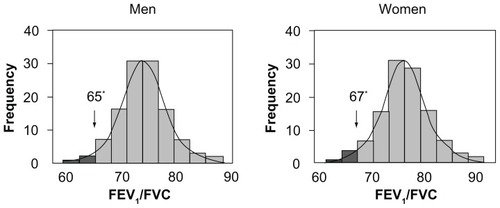
Figure 2 Decline of FEV1 and FVC with aging, normalized for height.Citation3
In the sample of healthy subjects, 15% had a FEV1/FVC < 0.70, and would have been inappropriately classified as obstructed according to GOLD criteria. describes the proportion of participants with the ratio < 70 in the different age groups. By applying the FEV1/FVC thresholds proposed by Hardie et alCitation19 for different age groups (ie, 0.70 for <70 years, 0.65 for 70–80 years, and 0.60 for >80 years), the percentage of obstructed subjects decreased to 6% (men 11%, women 4%). In particular, the proportion of subjects aged 65–70 years with a ratio below 0.70 was 11% (men 16%, women 8%); the proportion of subjects between 70 and 80 years of age with the ratio below 0.65 was 5% (men 12%, women 2%), whereas none of the subjects aged 80 years or more had FEV1/FVC < 0.60.
Table 3 Proportion of healthy elderly subjects with FEV1/FVC ratio < 0.70 in different age groups, with data presented as n (%)
Discussion
This study provides additional evidence helpful for determining the most appropriate spirometric criteria to define airway obstruction in elderly subjects. The fifth percentile of FEV1/FVC observed in the considered sample of healthy subjects aged > 65 years was lower than 0.70 in both men and women, thus confirming the inadequacy of this threshold for FEV1/FVC after the age of 65 years. Moreover, the findings of the present study suggest that, in such a population, FEV1/FVC < 0.65 and <0.67 (for males and females, respectively) could represent valid criteria that are simple to use and incorporate the known physiological decline in lung function with aging.
The present findings are in agreement with observations made by other authors,Citation16–Citation18 who have emphasized that the use of the FEV1/FVC threshold proposed by GOLD leads to a risk of overdiagnosis of COPD in geriatric subjects. Furthermore, the current results suggest that the inaccuracy of using a threshold of 0.70 for FEV1/FVC already exists in subjects aged 65 years and older. This differs to some extent from what has been suggested by the most recent GOLD guidelinesCitation11 (that recognize some imprecision of the threshold of 0.70 for FEV1/FVC in people over 70 years of age) and by Medbo et al,Citation10 who suggested the use of a threshold of FEV1/FVC < 0.65 in subjects over the age of 70 years on the basis of prebronchodilator spirometry data from a population-based study in Norway.
Interestingly, in our study, the rate of decline in the FEV1/FVC ratio with aging was not statistically significant in men or women older than 65 years, because of a concomitant decline in both FEV1 and FVC. Thus, in contrast with the findings of Hardie et al,Citation19 our results do not support the need to decrease the lower limit of normal for FEV1/FVC to 0.60 in elderly subjects (>80 years). For the same reason, no predictive equation for FEV1/FVC could be derived; accordingly, the mean value and the fifth percentile of FEV1/FVC from this healthy population can be used as the predicted value and lower limit of normal, respectively, for people aged 65 years and over.
All reference equations derived from samples with a wide age range describe a progressive decline in the FEV1/FVC ratio with aging; the age-related decrease involves both FEV1 and FVC, seems to be nonlinear, and accelerates with aging.Citation30–Citation32 In 1982, Crapo et alCitation33 found that between 20 and 70 years of age, vital capacity decreases to approximately 75% of the best values achieved previously. According to the present observations, presumably in the oldest people the decline of vital capacity accelerates more than in the younger age groups and such a decline is similar to the reduction of FEV1, so that the FEV1/FVC ratio could undergo minimal variations in the last decades. Recently, Langhammer et alCitation34 and Falaschetti et alCitation35 observed that FEV1/FVC reaches a near plateau phase in elderly subjects. The authors emphasized that, although the sample consisted of subjects with a wide range of height and age, the extremes did not influence the equations.
In a reference study specifically designed for elderly residents in Madrid (age range 65–85 years), Garcia et alCitation36 found a significant relationship between FEV1/FVC and age in men and between FEV1/FVC, age and height in women. Even in this study, the predicted equation for FEV1/FVC had a very low R2 (0.048 and 0.083 for men and women, respectively) and the authors highlighted the strong negative relationship of FVC with age. By applying predictive equations recently derived from Kuster et alCitation37 in a Swiss population, the lower limit of normal for FEV1/FVC does not show important decreases with aging; for example, in men with a height of 170 cm, the lower limit of normal for FEV1/FVC ranges from 0.66 at the age of 65 years to 0.64 for people aged 95 years. All these results support a position in favor of almost stable predicted values and lower limits of normal for FEV1/FVC in elderly people aged 65 years and over.
A clear position in favor of the fixed threshold of FEV1/FVC < 0.70 has been recently reported by other authors, with the claim that it is easy to use, thus helping to remove barriers to widespread use of spirometry.Citation3,Citation6–Citation8 Probably the use of the two lower fixed values for the elderly, suggested by data from the SARA study, does not add elements of particular complexity for physicians involved in interpretation of pulmonary function tests. However, this approach would diminish the number of false diagnoses of COPD, with significant cost savings due to reduction of inappropriately prescribed drugs. Thus, more resources could be redirected to primary prevention of COPD (smoking cessation) and treatment of more severe COPD.
Authors advocating retaining FEV1/FVC < 0.70 often quote the results of Mannino et al, who found that such a threshold is very good for identifying patients at risk of death and COPD-related hospitalizations.Citation38 However, although this indicates that FEV1/FVC < 0.70 may recognize a proportion of individuals at risk, it does not mean that this is the best way to diagnose the disease. On the other hand, Vas Fragoso et alCitation39 found elevated risk of death and respiratory symptoms in adults with FEV1/FVC less than the lower limit of normal. Sorino et alCitation40 recently confirmed that FEV1/FVC less than the lower limit of normal, FEV1/FEV6 less than the lower limit of normal, and FEV1 less than the lower limit of normal are all significant predictors of all-cause and cardiopulmonary mortality in older individuals. The strongest spirometric predictor of all-cause mortality remains the appropriately named vital capacity, because the majority of deaths in adult smokers, with or without COPD, are caused by cardiovascular disease.
Two recent studies investigated subjects in between the two definitions of airway obstruction (ie, FEV1/FVC < 0.70 but ≥ lower limit of normal), showing that their clinical profile is characterized by relevant comorbid disease and poor health-related quality of life, but similar exercise, frequency of exacerbations, and indices of systemic effects.Citation41,Citation42 The investigators emphasized that these subjects might be at risk and should be followed carefully; we should be aware that fewer than one in five smokers with mild airway obstruction ever develop clinically important COPD, and that today we are not yet able to identify which smokers will be rapid fallers.Citation2,Citation4
The present study has some limitations. First, the cohort was recruited for a cross-sectional investigation, whereas the effect of aging on respiratory function would be better assessed in a longitudinal study. It is plausible that FEV1/FVC decreases significantly even after the age of 65 years, but this can be less reliable when derived by a cross-sectional observation of older people. In fact, they could represent individuals who had higher spirometric values at a younger age, and FEV1/FVC similar to those of younger subjects at the time of recruitment. Second, subjects participating in the SARA project were not randomly selected from the population, but consisted mainly of subjects with nonrespiratory illnesses attending outpatient clinics; this might have resulted in some selection bias, although it would not explain the higher pulmonary volumes than in other studies. The authors wish to emphasize that FEV1/FVC less than the lower limit of normal should not be the only criterion used for diagnosis of airway obstruction, but should always be combined with evaluation of FEV1 as percent of predicted. Indeed, patients with severe airflow limitation could have an important reduction both in FEV1 and FVC, with a sustained FEV1/FVC ratio. Thus, in doubtful cases, measurement of residual volume and total lung capacity is recommended.
In conclusion, the present findings confirm the inadequacy of FEV1/FVC < 0.70 for diagnosis of airway obstruction in elderly people, and we propose other easy to remember thresholds for FEV1/FVC after 65 years of age, ie, 0.65 in men and 0.67 women. Further studies are needed to assess both the classificatory and prognostic properties of such a threshold as well as epidemiological surveys to confirm it.
Disclosure
The authors report no conflicts of interest in this work.
References
- QuanjerPHEnrightPLMillerMRThe need to change the method for defining mild airway obstructionEur Respir J20113772072221357929
- EnrightPBrusascoVCounterpoint: Should we abandon FEV1/FVC < 0.70 to detect airway obstruction? YesChest20101381040104221051394
- CelliBRHalbertRJPoint: should we abandon FEV1/FVC < 0.70. NoChest20101381037104021051393
- PellegrinoRBrusascoVViegiGDefinition of COPD: based on evidence or opinion?Eur Respir J20083168169018310402
- EnrightPLAre GOLDen slumbers drug induced?Am J Respir Crit Care Med2008177129118487621
- FabbriLMBoschettoPMappCETime to wake up!Am J Respir Crit Care Med20081771291129218487621
- FabbriLMFEV1/FVC fixed ratio again!Chest20111391252125321540227
- ManninoDMDefining chronic obstructive pulmonary disease … and the elephant in the roomEur Respir J20073018919017666553
- BhattNYWoodKLWhat defines abnormal lung function in older adults with chronic obstructive pulmonary disease?Drugs Aging20082571772818729545
- MedboAMelbyeHLung function testing in the elderly – can we still use FEV1/FVC < 70% as a criterion of COPD?Respir Med20071011097110517239575
- Global Initiative for Chronic Obstructive Lung DiseaseGlobal Strategy for the Diagnosis, Management and Prevention of COPD2011 Available from: http://www.goldcopd.org/Accessed May 20, 2012
- QaseemAWiltTJWeinbergerSEAmerican College of Physicians; American College of Chest Physicians; American Thoracic Society; European Respiratory SocietyDiagnosis and management of stable chronic obstructive pulmonary disease: a clinical practice guideline update from the American College of Physicians, American College of Chest Physicians, American Thoracic Society, and European Respiratory SocietyAnn Intern Med201115517919121810710
- British Thoracic SocietyBTS guidelines for the management of chronic obstructive pulmonary diseaseThorax200459Suppl1232
- O’DonnellDAaronSBourbeauJCanadian Thoracic Society recommendations for management of chronic obstructive pulmonary disease: 2007 updateCan Respir J2007145B32B
- National Institute for Health and Clinical ExcellenceChronic obstructive pulmonary disease: management of chronic obstructive pulmonary disease in adults in primary and secondary careNational Clinical Guideline Centre2010 Available from: http://guidance.nice.org.uk/CG101/Guidance/pdf/EnglishAccessed June 27, 2011
- HankinsonJLOdencrantzJRFedanKBSpirometric reference values from a sample of the general US populationAm J Respir Crit Care Med19991591791879872837
- EnrightPLKronmalRAHigginsMSpirometry reference values for women and men 65 to 85 years of age. Cardiovascular Health studyAm Rev Respir Dis19931471251338420405
- RobertsSDFarberMOKnoxKSFEV1/FVC ratio of 70% misclassifies patients with obstruction at the extremes of ageChest200613020020616840402
- HardieJABuistASVollmerWMRisk of over-diagnosis of COPD in asymptomatic elderly never-smokersEur Respir J2002201117112212449163
- SwanneyMPRuppelGEnrightPLUsing the lower limit of normal for the FEV1/FVC ratio reduces the misclassification of airway obstructionThorax2008631046105118786983
- MillerMRHankinsonJBrusascoVStandardisation of spirometryEur Respir J20052631933816055882
- PellegrinoRViegiGBrusascoVInterpretative strategies for lung function testsEur Respir J20052694896816264058
- BelliaVPistelliRCatalanoFQuality control of spirometry in the elderly. The SARA study. SAlute Respiration nell’Anziano, Respiratory Health in the ElderlyAm J Respir Crit Care Med20001611094110010764296
- American Thoracic SocietyStandardization of spirometry, 1994 updateAm J Respir Crit Care Med1995152110711367663792
- AbramsonMJHensleyMJSaundersNAEvaluation of a new asthma questionnaireJ Asthma1991281291392013560
- BurneyPGLaitinenLAPerdrizetSValidity and repeatability of the IUATLD (1984) Bronchial Symptoms Questionnaire: an international comparisonEur Respir J198929409452606194
- PistelliRBelliaVCatalanoFSpirometry reference values for women and men aged 65–85 living in southern Europe: the effect of health outcomesRespiration20037048448914665773
- PeatJKWoolcockAJCullenKRate of decline of lung function in subjects with asthmaEur J Respir Dis1987701711793569449
- CibellaFCuttittaGBelliaVLung function decline in bronchial asthmaChest20021221944194812475831
- DockeryDWWareJHFerrisBGDistribution of forced expiratory volume in one second and forced vital capacity in healthy, white, adult never-smokers in six US citiesAm Rev Respir Dis19851315115203873193
- GlindmeyerHWLefanteJJMcCollosterCBlue-collar normative spirometric values for Caucasian and African-American men and women aged 18 to 65Am J Respir Crit Care Med19951514124227842200
- BrandliOSchindlerCKunzliNLung function in healthy never smoking adults: reference values and lower limits of normal of a Swiss populationThorax1996512772838779131
- CrapoROMorrisAHClaytonPDLung volumes in healthy nonsmoking adultsBull Eur Physiopathol Respir1982184194257074238
- LanghammerAJohnsenRGulsvikAForced spirometry reference values for Norwegian adults: the Bronchial Obstruction in Nord-Trondelag StudyEur Respir J20011877077911757626
- FalaschettiELaihoJPrimatestaPPrediction equations for normal and low lung function from the Health Survey for EnglandEur Respir J20042345646315065839
- Garcia-RioFPinoJMDorghamASpirometric reference equations for European females and males aged 65–85 yearsEur Respir J20042439740515358698
- KusterSPKusterDSchindlerCReference equations for lung function screening of healthy never-smoking adults aged 18–80 yearsEur Respir J20083186086818057057
- ManninoDMBuistASPettyTLLung function and mortality in the United States: data from the First National Health and Nutrition Examination Survey follow up studyThorax20035838839312728157
- Vas FragosoCAConcatoJMcAvayGThe ratio of FEV1/FVC as a basis for establishing chronic obstructive pulmonary diseaseAm J Respir Crit Care Med201018144645120019341
- SorinoCSherrillDGuerraSPrognostic value of FEV1/FEV6 in elderly peopleClin Physiol Funct Imaging20113110110720969726
- LamprechtBSchirnhoferLKaiserBSubjects with discordant airways obstruction: lost between spirometric definitions of COPDPulm Med2011201178021521637369
- García-RioFSorianoJBMiravitllesMOverdiagnosing subjects with COPD using the 0.7 fixed ratio: correlation with a poor health-related quality of lifeChest20111391072108021183609
Appendix
Respiratory Health in the Elderly study group
Coordinators: V Bellia (Palermo) and F Rengo (Napoli). Scientific committee members: R Antonelli Incalzi (Taranto), V Grassi (Brescia), S Maggi (Padua), G Masotti (Florence), G Melillo (Naples), D Olivieri (Parma), M Palleschi (Rome), R Pistelli (Rome), M Trabucchi (Rome), S Zuccaro (Rome).
Participating centers, principal investigator, and associated investigators (the latter in brackets): Divisione di Medicina I, Ospedale Geriatrici INRCA, Ancona, DL Consales (D Lo Nardo, P Paggi); Divisione di Geriatria, Ospedale Civile, Asti, F Goria (P Fea, G Iraldi, R Corradi); Cattedra di Gerontologia e Geriatria, Policlinico Universitario, Bari, A Capurso (R Flora, S Torres, G Venezia, M Mesto); Divisione di Geriatria, Ospedale Malpighi, Bologna, S Semeraro (L Bellotti, A Tansella); Divisione di Medicina Generale, Ospedale Civile, Brescia, V Grassi (S Cossi, G Guerini, C Fantoni, M De Martinis, L Pini); Clinica Pneumologica, Fondazione “E Maugeri”, Telese, G Melillo (R Battiloro, C Gaudiosi, S De Angelis); Istituto di Medicina Interna e Geriatria, Ospedale Cannizzaro, Catania, L Motta (I Alessandria, S Savia); Istituto di Gerontologia e Geriatrici, Ospedale Ponte Nuovo, Università Florence, Florence, G Masotti (M Chiarlone, S Zacchei); Divisione di Geriatria, Ospedale Morgagni, Forli, V Pedone (D Angelini, D Cilla); Divisione di Geriatria, Ospedale Galliera, Genova, E Palummeri (M Agretti, P Costelli, D Torriglia); Grouppo Ricerca Geriatrica Ricerca Geriatrica, Ospedale Richiedei, Gussago, M Trabucchi (P Barbisoni, F Guerini, P Ranieri); Divisione di Geriatria, Ospedale Generale, L’Aquila, F Caione (D Caione, M La Chiara); Divisione di Geriatria, Ospedale San Gerardo, Monza, G Galetti (A Cantatore, D Casarotti, G Anni); Cattedra di Gerontologia e Geriatria, Università Federico II, Napoli, F Rengo (F Cacciatore, AI Pisacreta, C Calabrese); Istituto di Medicina Interna, Ospedale Geriatrico, Padova, G Enzi (P Dalla Montà, S Peruzza, P Albanese, F Tiozzo); Istituto di Clinica delle Malattie dell’Apparato Respiratorio, Ospedale Rasori, Parma, D Olivieri (V Bocchino, A Comel, N Barbarito); Istituto di Gerontologia e Geriatria, Policlinico Monteluce, Perugia, U Senin (F Arnone, L Camilli, S Peretti); Divisione di Geriatria, Ospedale Israelitico, Roma, SM Zuccaro (M Marchetti, L Palleschi); Divisione di Geriatria, Ospedale Generale Addolorata, Roma, M Palleschi (C Cieri, F Vetta); Istituto di Medicina Interna e Geriatria, Policlinico Gemelli, Roma, PU Carbonin (F Pagano, P Ranieri); Istituto di Semeiotica Medicina e Geriatria, Policlinico Le Scotte, Siena, S Forconi (G Abate, G Marotta, E Pagni); Fondazione San Raffaele, Cittadella della Carità, Taranto, R Antonelli-Incalzi (C Imperiale, C Spada); Cattedra di Gerontologia e Geriatria, Ospedale Maggiore, Milano, C Vergani (G Giardini, MC Sandrini, I Dallera); Cattedra di Malattie dell’Apparato Respiratorio, Ospedale V Cervello, Palermo, V Bellia (F Catalano, N Scichilone, S Battaglia).
Coordinating center: Dipartimento di Medicina, Pneumologia, Fisiologia e Nutrizione Umana, Università degli Studi di Palermo.