
Abstract
Background
Chronic obstructive pulmonary disease (COPD) is a chronic inflammatory disease with exacerbations causing hospitalizations, morbidity, and mortality. COPD exacerbation causes a substantial health impact, and its subtypes might differ in prognosis and treatment response.
Methods
This study evaluated the factors of COPD exacerbations and explored the probabilities of frequent severe COPD exacerbations. Categorical and continuous variables between groups were compared. The hazard ratio (HR) and the probability of no hospital readmission were also estimated.
Results
A total of 617 COPD patients were enrolled and comprised the frequent exacerbator (N = 226) and the non-frequent exacerbator (N = 391) groups. The frequent exacerbator group significantly displayed a higher eosinophil count (EC; p=0.004), a higher percentage of the frequent severe acute exacerbation history before the index hospitalization (IH; p < 0.001), a lower FEV1 value (p=0.001), and a higher triple combination inhaler prior and following the IH (p < 0.001 and p=0.002) than the non-frequent exacerbator one. Increasing age (aOR of 1.02), higher EC (aOR of 1.09), and lower FEV1 value (aOR of 0.72) were significantly associated with an increased hospital readmission risk. The readmission rate and risk were higher in patients with a history of frequent severe acute exacerbation (aHR of 3.38) than those without severe acute exacerbation. Cases treated with the triple combination inhaler before the IH had a higher readmission rate and risk than non-users.
Conclusion
Patients with EC ≥2%, FEV1 <50%, or frequent severe acute exacerbation history before the IH have a higher risk of being diagnosed with a frequent exacerbator phenotype. Besides, higher age, triple combination inhaler before the IH, and smoking might be independently correlated with the frequent readmission risk within 1-year post-exacerbation. A better comprehension of the COPD exacerbation mechanism may further identify the best course of preventative strategy and lead to novel interventions.
Introduction
Chronic obstructive pulmonary disease (COPD) is a chronic inflammation disease of the airways characterized by an incompletely reversible airflow limitation.Citation1 The COPD disease progression is punctuated by periodic deterioration in respiratory symptoms called exacerbations that cause most hospitalizations followed by significant morbidity and mortality.Citation2 COPD exacerbations could lead to hospital admissions contributing to a significant clinical and economic load worldwide.Citation3 Exacerbations might get more frequent and more severe as COPD progresses,Citation4 and their recurrence is correlated with a lung function decline and health status of patients.Citation5 The hospitalization cost of severe COPD exacerbation can be 60 times more expensive than mild or moderate exacerbations managed by primary care services.Citation6
For patients surviving after a COPD exacerbation-related hospitalization, readmission is a significant problem. Identifying and reducing risk factors for frequent readmission is therefore essential.Citation7 The official American Thoracic Society workshop report on reducing COPD readmission emphasized the requirement to identify risk factors for COPD readmissions.Citation8
Acute exacerbations are an essential feature in COPD’s natural history, and identifying the frequent exacerbator phenotype may benefit from avoiding these complications. Furthermore, identifying COPD patients with risk factors associated with severe exacerbations may alert physicians, induce closer follow-up, and adopt preventive measures. Identification of biomarkers enables phenotype-driven approaches to manage and prevent exacerbations.
COPD exacerbations are heterogeneous, and various phenotypes that differ in biological basis, prognosis, and response to therapy have been proposed.Citation9 The specific phenotype of frequent exacerbations in COPD patients has been identified using different thresholds primarily derived from the median exacerbation frequency in various cohorts, containing two or more moderate-to-severe exacerbations during 1 year.Citation9 Consequently, most researchers use this cutoff to describe the frequent exacerbator phenotype,Citation4,Citation10 and this definition is now recorded in the Global Initiative for Chronic Obstructive Lung Disease guidelines (GOLD).Citation1
This study’s primary aim was to develop and validate possible predictors of frequent severe exacerbations in COPD patients requiring hospitalization (two or more exacerbations per year) in reliance on data collection of the clinical records obtained during hospital admission. The secondary aim was to investigate the independent clinical parameters involved in frequent readmission risk during 1 year after an exacerbation.
Materials and Methods
Study Design
An observational and retrospective cohort study was conducted in a tertiary education hospital, which screened the medical records for COPD-related hospitalizations from January 2016 to December 2019. The inclusion criteria: 1) Patients admitted to the hospital from outpatient or emergency department with a severe acute exacerbation. 2) Patients who were previously diagnosed with COPD by a specialist pulmonologist and assigned one of the ICD 10 (International Classification of Diseases) codes, J44, J44.0, J44.1, J44.8, and J44.9. 3) Patients with no exacerbation in one month before preceding enrollment. 4) Patients with more than one diagnosis code of J44 and sub-segment. 5) Patients having COPD-related hospital admission for at least one time during this period. The definition of index hospitalization (IH) was the first admission related to COPD during the study period, and patients were survived at the IH. This study’s protocol was approved by Institutional Review Board, Taipei Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation in August 2020 (Protocol number 09-X-059). The informed consent was signed and provided by each included participant.
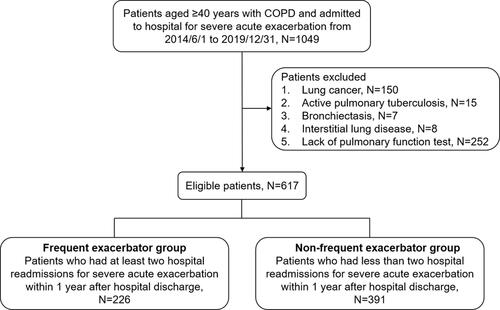
The COPD diagnosis was based on a spirometry and compatible history. COPD was defined as the volume of post-bronchodilator forced expiratory in one second (FEV1)/forced vital capacity (FVC) ratio <0.7 according to 2020 GOLD guidelines.Citation1 Severe exacerbation of COPD was identified as more than 2 consecutive days with sustained worsening of patient’s symptoms beyond day-to-day variations causing hospitalization. Only COPD severe exacerbations were accounted for and merged for in the analysis.Citation2 Frequent severe exacerbation was defined as hospital readmission within 1 year over 2 times from chest diseases outpatient or emergency department.Citation3 Non-frequent exacerbator was defined as patients with less than two hospital readmissions for severe acute exacerbation within 1 year after hospital discharge. The number of hospitalizations within 1 year after hospital discharge had already included the IH during the study period. During the candidate reassessment, the exclusion criteria were as follows: absence of obstructive pattern on pulmonary function test (PFT) results, absence of a valid PFT result before IH, mislabeled as asthmatic (Non-smokers with or without obstructive spirometry results and no COPD record in medical records), tuberculosis, diagnosis result of lung cancer in the prior 3 years, those unable to complete the follow-up, and those who received systemic steroids within 48 h before the blood test at the IH. COPD patients with severe exacerbations were classified into two groups conforming to their frequency count 1 year after the IH: The frequent exacerbator group (Severe acute exacerbation with hospitalization ≥2) and the non-frequent exacerbator group (≤1). The subject distribution is summarized in .
Figure 1 Flowchart of selected population in this study.
Measurement
The following data collected according to the medical records before the IH: demographics, body mass index, smoking history, comorbidities (the neuromuscular disease included stroke, Parkinsonism), severe exacerbations' frequency in previous 12 months, the use of home noninvasive ventilation, pulmonary function test, and the respiratory medicines including inhaled corticosteroids (ICS), long-acting beta-agonists (LABA), and long-acting antimuscarinic agents (LAMA). The following data were collected during the IH: arterial blood gas, C-reactive protein (CRP) levels, chest X-ray (CXR), and hemogram measured during a corticosteroid-free time frame, defining as no use of systemic corticosteroid from 1 h to 48 h prior venipuncture.
Primary in-hospital treatments were recorded, including antibiotics, systemic steroids at IH, rate of intensive care unit (ICU) or respiratory care center (RCC) utilization, and mechanical ventilation. Hospital stays and inhaler prescriptions after discharge were also recorded.
Outcomes
The primary outcome was to compare clinical characteristics, laboratory findings, and treatment between frequent exacerbator and non-frequent exacerbator and the independent factors related to frequent severe exacerbation phenotype. The secondary outcomes have assessed the relationship between independent factors and the time of the first COPD-related readmission within 12 months.
Ethical Statement
The study was approved by the Institutional Review Board, Taipei Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation in August 2020 (protocol number 09-X-059).
Statistical Analyses
Baseline characteristics were compared between groups using Chi-squared tests and independent t-tests to detect any differences in the categorical and continuous demographic variables. Data were displayed as a number (percentage) of categorical variables and mean±SD for continuous variables. Cox regression models were used to estimate the adjusted hazard ratio (aHR) and its 95% confidence intervals (CIs) of the risk of hospital readmission. The assumption of proportional hazards was checked, and the probability of no hospital readmission was estimated by Kaplan–Meier method. A Log rank test was used to test the differences between groups. All P values were two-sided with a significance level of 0.05. Data management and subsequent statistical analyses were conducted using SAS version 9.4 software (SAS Institute, Inc.).
Result
A total of 617 COPD patients were enrolled following the inclusion and exclusion criteria (). Of them, 226 patients who underwent at least two hospital readmissions for severe acute exacerbation less than 1 year after hospital discharge were grouped into the frequent exacerbator group, and 391 patients who underwent less than two hospital readmissions were grouped into the non-frequent exacerbator group (). The baseline characteristics and laboratory data of both groups are shown in . The frequent exacerbator group displayed a significantly higher percentage of eosinophil (2.37±3.65 vs 1.60±2.20, p=0.004) on hospital admission and more than 1 severe acute exacerbation in the past year prior to the IH (12.83% vs 2.81%, p < 0.001) than the non-frequent exacerbator group. In addition, the GOLD 2019 classification showed a significant difference between the frequent exacerbator and non-frequent exacerbator group (p < 0.001). Differences in the pulmonary function and arterial blood gas tests were found between these two groups (). FEV1 value was higher in non-frequent exacerbator group (1.20±0.47 vs 1.07±0.46, p=0.001) with a higher FEV1/FVC ratio (56.45±11.24 vs 52.63±12.00, p < 0.001) and PH value (7.38±0.06 vs 7.35±0.10, p=0.046). Treatments on hospital admission and concurrent medications were also studied to delineate their association with hospital readmission frequency (). The percentage of antibiotic-steroid combination treatment was significantly higher in the frequent exacerbator group than in the non-frequent exacerbator (72.32% vs 60.10%, p=0.005). Similar trends are also shown in patients who received a triple combination inhaler before the IH (p < 0.001) and following the IH (p=0.002). There was no significant difference in both the infection status and the length of stay between the two groups.
Table 1 Baseline Characteristics and Laboratory Findings on Admission Frequent Exacerbator Group vs Non-Frequent Exacerbator Group
Table 2 Pulmonary Function Test Results and Arterial Blood Gases on Admission (Frequent Exacerbator Group vs Non-Frequent Exacerbator Group)
Table 3 Treatments on Admission and Concurrent Medications (Frequent Exacerbator Group vs Non-Frequent Exacerbator Group)
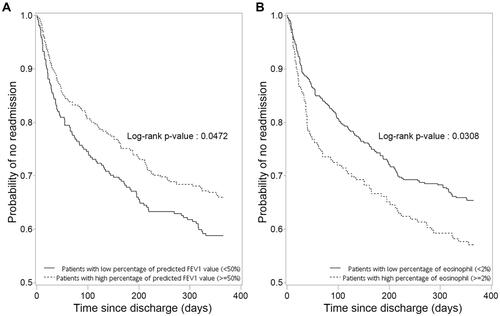
Increasing age (aHR of 1.02), higher eosinophil count (EC; aHR of 1.09), and lower FEV1 value (aHR of 0.72) were significantly associated with an increased hospital readmission risk. Cases with a low percentage of predicted FEV1 value (<50%) showed a significantly lower probability of no readmission during the 1-year follow-up time than cases with a high percentage of predicted FEV1 value (≥50%) (Log rank test, p= 0.047, ). The probability of no readmission was significantly lower in patients with a high percentage of eosinophil (≥2%) when compared to patients with a low percentage of eosinophil (<2%) (p=0.031) ().
Figure 2 Kaplan–Meier curves for time to hospital readmissions within 1 year after hospital discharge. (A) Comparison between patients with FEV1 <50% (% of predicted) and FEV1 ≥50% (% of predicted). (B) Comparison between patients with eosinophil count <2% and eosinophil count ≥2%.
The readmission rate was higher in patients with more than one severe acute exacerbation in the past year (63.90 vs 16.29 per 100 person-years) and at risk (aHR of 3.38; 95% CI, 2.23–5.11; p < 0.001) than those with no history of severe acute exacerbation by more than three times. Cases treated with the triple combination inhaler before the IH also had a higher readmission rate (30.18 vs 13.31 per 100 person-years) and readmission risk (aHR of 1.83; 95% CI, 1.33–2.54; p < 0.001) in comparison with the non-users. Besides, current smokers had a higher readmission rate (23.40 vs 15.62 per 100 person-years) and risk (aHR 1.43; 95% CI, 1.01–2.03; p=0.044) than non-smokers ().
Table 4 Hazard Ratios and Event Rates for COPD-Related Readmission in Different Clinical Characteristic Comparisons
Discussion
In this study, a COPD subgroup with frequent exacerbator phenotype has been proposed with distinct outcomes compared to the non-frequent exacerbator one. Phenotypes of frequent exacerbators had been postulated and surveyed in previous studies.Citation3 This COPD-related phenotype has recently been described using data from the Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints (ECLIPSE) study.Citation4 The COPD exacerbations are clustered together in time rather than random events, and there is a high-risk period for recurrent exacerbations after the initial exacerbation.Citation4 Le Rouzic et al confirmed the existence and clinical relevance of a subgroup of frequent exacerbator in COPD patients identified using a threshold of two exacerbations per year, allowing easy identification of routine care for at-risk patients before the prolonged follow-up.Citation3
In the present study, the frequent exacerbator group significantly showed a higher peripheral blood eosinophil percentage (PBEC, 2.37%) and a shorter time of first hospital readmission due to COPD, similar to previous studies.Citation11–Citation13 Couillard et al reported that a patient with higher eosinophilia had a higher readmission risk due to COPD (OR of 3.59) and a shorter time to first readmission due to COPD (aHR of 2.74).Citation12 Bélanger et al reported that the eosinophilic inflammation confers an increased risk of readmission due to COPD.Citation11 One of our previous studies demonstrated a significant linear correlation between the blood eosinophil percentage and readmission numbers.Citation13 A recent study on acute exacerbation of chronic obstructive pulmonary disease (AECOPD) also showed an increased exacerbation risk in patients with elevated blood eosinophils.Citation14 With respiratory-related readmissions in the study being dominated by exacerbations, the results showed consistency with the COPD gene and ECLIPSE studies. In these studies, increased blood EC was reported to correlate with increased risk of recurrent exacerbations in stable COPD.Citation15,Citation16 These shreds of evidence could reveal that eosinophilic COPD exacerbation is a well-known risk factor for readmissionsdue to COPD.
A recent study reported a lower risk in patients with all-cause readmission having blood ECs above 300 cells/μL.Citation17 However, there is conflicting evidence with analyses of two previous cohort studies showing no association between blood eosinophils and increased exacerbation risk.Citation18,Citation19 These differences may come for several reasons: 1) The different cutoffs for the definition of human blood eosinophil cell showing inconsistent results associated with the influence of eosinophil cell counts on readmissions throughout sensitivity analyses; 2) The range of respiratory diagnoses included in the intervention study was physician defined. For example, a study recruited the first three ICD coding with COPD diagnosis, and some excluded the diagnosis of pneumonia.Citation17,Citation20 In this study, the patients without evidence of previous corroborative spirometry or imaging were excluded. 3) Methodological differences reveal that positive studies were exempt from the confounding effect of systemic corticosteroid use. The primary consideration was the effect of the relative timing of systemic corticosteroid administration on eosinophil level.Citation14 4) Difference of following times after discharge for COPD-related readmission.Citation20 One study excluded the patients with >4 hospitalizations in the previous 12 months for any cause.Citation21
In this study, the FEV1 value and FEV1/FVC ratio were lower in the frequent exacerbator group. Lower FEV1 values were significantly associated with an increased hospital readmission risk. Besides, cases with the FEV1 values of <50% showed a substantially lower probability of no readmission during the 1-year follow-up period than cases with ≥50%. A previous study indicated that FEV1<50% was one of the independent predictors of frequent severe exacerbations.Citation22 Another study revealed that the requirement for ventilatory support increased the likelihood of readmission by logistic regression analysis of patient-related factors. COPD stage IV patients were reported to have a higher need for ventilatory support.Citation23 Poor lung function was related to frequent severe exacerbations as expected, and spirometry data admitting to clinicians would confirm the diagnosis and risk-stratification of patients.
Decreased FEV1 is mainly associated with increased symptoms and heightened inflammatory response, thus may alter an exacerbation risk.Citation24 The frequent exacerbations are positively associated with a rapid decline of FEV1.Citation25 Donaldson et alCitation26 reported a mean of 2.92 exacerbations yearly in COPD patients with moderate to very severe disease. The mean rate of FEV1 decline was greater in patients with more exacerbations (p < 0.05). Celli et al reported the influence of frequent exacerbations on the FEV1 decline data from the Toward a Revolution in COPD Health (TORCH) study, in which patients experiencing greater frequency of exacerbations had a faster decline in FEV1 during the 3-yr study period.Citation27 Repeated episodes of COPD exacerbations might impair lung tissues and lead to an accelerated rate of pulmonary function decline. This concept is supported by patients suffering recurrent exacerbations who showed increased concentrations of inflammatory markers in sputum.Citation28 Analysis of exacerbations for 2138 patients enrolled in the ECLIPSE study demonstrated that exacerbations were more frequent and more severe with increased severity of the disease defined using spirometry measures.Citation4 Generally, 22% of patients with stage II disease, 33% with stage III, and 47% with stage IV had frequent exacerbations during the first-year follow-up.Citation4 The same study also presented that the single best predictor of exacerbations across all GOLD stages was the history of exacerbations.Citation4
The readmission rate and risk were higher in patients with two or more severe acute exacerbations in the past year than those with no severe acute exacerbation history in this study. Two previous studies reported that following the first severe COPD exacerbation, each subsequent recurrence requiring hospitalization had increased the risk of a subsequent event and death, with increasing severity of subsequent events.Citation9,Citation29 Müllerová et al have studied a large primary care cohort of 18,568 patients aged ≥40 years in the USA to explore the COPD exacerbation frequency and associated factors. They found noticeable differences between patients managed in primary care who had one or more exacerbations (41.46%) than patients with no COPD exacerbations recorded during the 12-month follow-up period.Citation23 Previous hospitalization for AECOPD was also a strong predictor for future readmission as the rehospitalization frequency is closely linked to the admission frequency in the previous year.Citation30 Exacerbation frequency is also increased with raising airflow limitation and similarly with higher dyspnoea score.Citation31 The exacerbation frequency was well correlated with symptom severity based on prospective studies’ findings;Citation24 however, these two factors are semi-independent and recurrent exacerbations could happen in patients with moderate airflow limitation.Citation4
In this study, a triple inhaler presented before discharge is one of the independent factors associated with increased severe acute exacerbations risk of COPD. On the contrary, after discharge, a triple inhaler is one of the independent factors for less frequent severe acute exacerbation. Inhaled corticosteroids (ICS) are commonly prescribed to COPD patients to reduce exacerbations. A recent meta-analysis with thirteen randomized controlled trials containing 15,519 patients with COPD (ICS/LABA/LAMA combination, 53.1%; ICS/LABA combination, 46.9%) indicated that combination therapy with ICS/LABA/LAMA was correlated with the more reduction of moderate or severe AECOPD risk (relative risk of 0.78; 95% CI, 0.71–0.85) and better lung function than either LABA/LAMA combination therapy or single long-acting bronchodilator therapy.Citation32 Besides, compared to LABA/LAMA combination therapy, the ICS/LABA/LAMA combination therapy was correlated with higher blood ECs, and no significant differences were detected concerning the pneumonia risk between triple combination therapy and comparators.Citation32 These findings appear to support the current recommendations of the management strategy for the COPD from Global Initiative for Chronic Obstructive Lung Disease (GOLD), which suggests the use of triple therapy in patients with clinically significant symptoms and are at increased risk for frequent or severe exacerbations (GOLD group D).Citation2 Furthermore, the triple therapy showed the same cardiovascular safety profile compared to the ICS/LABA combination.Citation33–Citation37
There are several limitations to this study. First, this was a single-center study in Taiwan involving only the Asian race with a relatively small sample size, which might potentially limit the geographical scope of the findings and be affected by the biases related to such studies. Secondly, due to the lack of complete records of some patients, the estimation of exacerbation patients with no hospitalization was absent in this study. Therefore, it might underestimate the frequency of moderate-to-severe exacerbations and lead to analysis bias. Thirdly, discharged patients had to be alive to be included in this study. This might influence intra-hospitalized characteristics such as length of stay, ICU utilization rate, and mechanical ventilation. Thus, no conclusions can be obtained from these data for outcomes during the IH. All analyses were based on a single measurement at the time of IH, and any changes due to treatment or simple disease progression during the in-hospital stay were not assessed. Fourthly, this study considers the time effect of systemic corticosteroid administration and ECs. This possible bias must be recognized that excluding such patients might lose patients with the experience of outpatient treatment failure within the last 48 hours. Finally, although a spirometry recording was required for COPD patients’ eligibility in the present study, all COPD patients were not ensured to be enrolled due to lack of PFT.
Conclusion
The distinct COPD exacerbation subtype of severe acute exacerbations was proposed and showed a difference in prognosis and treatment response. EC ≥2%, FEV1 <50%, and patients with severe acute exacerbations history of at least 2 in 1 year of post-exacerbation before the IH might be the predictors of the frequent exacerbator COPD phenotype. Besides, higher age, triple combination inhaler before the IH, and smoking might be independently correlated with the frequent readmission risk within 1-year post-exacerbation. These findings underline the importance of identifying COPD patients with a risk of frequent exacerbation, and the management of COPD should involve phenotype-directed strategies. In addition, these results provide information for physicians to a better understanding of the mechanisms of COPD exacerbations with more prospective studies.
Ethics Approval and Informed Consent
The study was approved by the Institutional Review Board, Taipei Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation in August 2020 (protocol number 09-X-059). Written informed consent was signed and provided by each included participant.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval for the version to be published; and agreed to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
Additional information
Funding
References
- Singh D, Agusti A, Anzueto A, et al. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease: the GOLD science committee report 2019. Eur Respir J. 2019;53(5):1900164. Published 2019 May 18. doi:10.1183/13993003.00164-2019
- Vogelmeier CF, Criner GJ, Martinez FJ, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 report: GOLD executive summary. Eur Respir J. 2017;49:557–582. doi:10.1183/13993003.00214-2017
- Le Rouzic O, Roche N, Cortot AB, et al. Defining the “frequent exacerbator” phenotype in COPD: a hypothesis-free approach. Chest. 2018;153:1106–1115. doi:10.1016/j.chest.2017.10.009
- Hurst JR, Vestbo J, Anzueto A, et al. Susceptibility to exacerbation in chronic obstructive pulmonary disease. N Engl J Med. 2010;363:1128–1138. doi:10.1056/NEJMoa0909883
- Vestbo J, Edwards LD, Scanlon PD, et al. Changes in forced expiratory volume in 1 second over time in COPD. N Engl J Med. 2011;365:1184–1192. doi:10.1056/NEJMoa1105482
- Andersson F, Borg S, Jansson SA, et al. The costs of exacerbations in chronic obstructive pulmonary disease (COPD). Respir Med. 2002;96:700–708. doi:10.1053/rmed.2002.1334
- Iacobucci G. Hospital readmissions for COPD in England are rising, audit shows. BMJ. 2017;356:j557. doi:10.1136/bmj.j557
- Press VG, Au DH, Bourbeau J, et al. Reducing chronic obstructive pulmonary disease hospital readmissions. An official American Thoracic Society workshop report. Ann Am Thorac Soc. 2019;16:161–170. doi:10.1513/AnnalsATS.201811-755WS
- Pavord ID, Jones PW, Burgel PR, Rabe KF. Exacerbations of COPD. Int J Chron Obstruct Pulmon Dis. 2016;11(Spec Iss):21–30.
- McGarvey L, Lee AJ, Roberts J, et al. Characterisation of the frequent exacerbator phenotype in COPD patients in a large UK primary care population. Respir Med. 2015;109:228–237. doi:10.1016/j.rmed.2014.12.006
- Bélanger M, Couillard S, Courteau J, et al. Eosinophil counts in first COPD hospitalizations: a comparison of health service utilization. Int J Chron Obstruct Pulmon Dis. 2018;13:3045–3054. doi:10.2147/COPD.S170743
- Couillard S, Larivée P, Courteau J, Vanasse A. Eosinophils in COPD exacerbations are associated with increased readmissions. Chest. 2017;151:366–373. doi:10.1016/j.chest.2016.10.003
- Wu CW, Lan CC, Hsieh PC, Tzeng IS, Wu YK. Role of peripheral eosinophilia in acute exacerbation of chronic obstructive pulmonary disease. World J Clin Cases. 2020;8:2727–2737. doi:10.12998/wjcc.v8.i13.2727
- Li Q, Larivée P, Courteau J, et al. Greater eosinophil counts at first COPD hospitalization are associated with more readmissions and fewer deaths. Int J Chron Obstruct Pulmon Dis. 2019;14:331–341. doi:10.2147/COPD.S187375
- Vedel-Krogh S, Nielsen SF, Lange P, Vestbo J, Nordestgaard BG. Blood eosinophils and exacerbations in chronic obstructive pulmonary disease. The Copenhagen General Population Study. Am J Respir Crit Care Med. 2016;193:965–974. doi:10.1164/rccm.201509-1869OC
- Yun JH, Lamb A, Chase R, et al. Blood eosinophil count thresholds and exacerbations in patients with chronic obstructive pulmonary disease. J Allergy Clin Immunol. 2018;141:2037–2047 e2010. doi:10.1016/j.jaci.2018.04.010
- Håkansson KEJ, Ulrik CS, Godtfredsen NS, et al. High suPAR and low blood eosinophil count are risk factors for hospital readmission and mortality in patients with COPD. Int J Chron Obstruct Pulmon Dis. 2020;15:733–743.
- Casanova C, Celli BR, de-Torres JP, et al. Prevalence of persistent blood eosinophilia: relation to outcomes in patients with COPD. Eur Respir J. 2017;50(5):1701162. Published 2017 Nov 22. doi:10.1183/13993003.01162-2017
- Hastie AT, Martinez FJ, Curtis JL, et al. Association of sputum and blood eosinophil concentrations with clinical measures of COPD severity: an analysis of the SPIROMICS cohort. Lancet Respir Med. 2017;5:956–967. doi:10.1016/S2213-2600(17)30432-0
- Duman D, Aksoy E, Agca MC, et al. The utility of inflammatory markers to predict readmissions and mortality in COPD cases with or without eosinophilia. Int J Chron Obstruct Pulmon Dis. 2015;10:2469–2478. doi:10.2147/COPD.S90330
- Bafadhel M, Greening NJ, Harvey-Dunstan TC, et al. Blood eosinophils and outcomes in severe hospitalized exacerbations of COPD. Chest. 2016;150:320–328. doi:10.1016/j.chest.2016.01.026
- Ozyilmaz E, Kokturk N, Teksut G, Tatlicioglu T. Unsuspected risk factors of frequent exacerbations requiring hospital admission in chronic obstructive pulmonary disease. Int J Clin Pract. 2013;67:691–697. doi:10.1111/ijcp.12150
- Hartl S, Lopez-Campos JL, Pozo-Rodriguez F, et al. Risk of death and readmission of hospital-admitted COPD exacerbations: European COPD audit. Eur Respir J. 2016;47:113–121.
- Donaldson GC, Wedzicha JA. COPD exacerbations.1: epidemiology. Thorax. 2006;61:164–168. doi:10.1136/thx.2005.041806
- Anzueto A, Leimer I, Kesten S. Impact of frequency of COPD exacerbations on pulmonary function, health status and clinical outcomes. Int J Chron Obstruct Pulmon Dis. 2009;4:245–251.
- Donaldson GC, Seemungal TA, Bhowmik A, Wedzicha JA. Relationship between exacerbation frequency and lung function decline in chronic obstructive pulmonary disease. Thorax. 2002;57:847–852. doi:10.1136/thorax.57.10.847
- Celli BR, Thomas NE, Anderson JA, et al. Effect of pharmacotherapy on rate of decline of lung function in chronic obstructive pulmonary disease: results from the TORCH study. Am J Respir Crit Care Med. 2008;178:332–338. doi:10.1164/rccm.200712-1869OC
- Crooks SW, Bayley DL, Hill SL, Stockley RA. Bronchial inflammation in acute bacterial exacerbations of chronic bronchitis: the role of leukotriene B4. Eur Respir J. 2000;15:274–280. doi:10.1034/j.1399-3003.2000.15b09.x
- Suissa S, Dell’Aniello S, Ernst P. Long-term natural history of chronic obstructive pulmonary disease: severe exacerbations and mortality. Thorax. 2012;67:957–963. doi:10.1136/thoraxjnl-2011-201518
- Baker CL, Zou KH, Su J. Risk assessment of readmissions following an initial COPD-related hospitalization. Int J Chron Obstruct Pulmon Dis. 2013;8:551–559.
- Müllerová H, Shukla A, Hawkins A, Quint J. Risk factors for acute exacerbations of COPD in a primary care population: a retrospective observational cohort study. BMJ Open. 2014;4:e006171.
- Cazzola M, Rogliani P, Calzetta L, Matera MG. Triple therapy versus single and dual long-acting bronchodilator therapy in COPD: a systematic review and meta-analysis. Eur Respir J. 2018;52(6):1801586. doi:10.1183/13993003.01586-2018
- Calzetta L, Cazzola M, Matera MG, Rogliani P. Adding a LAMA to ICS/LABA therapy: a meta-analysis of triple combination therapy in COPD. Chest. 2019;155(4):758–770. doi:10.1016/j.chest.2018.12.016
- Ferguson GT, Rabe KF, Martinez FJ, et al. Triple therapy with budesonide/glycopyrrolate/formoterol fumarate with co-suspension delivery technology versus dual therapies in chronic obstructive pulmonary disease (KRONOS): a double-blind, parallel-group, multicentre, phase 3 randomised controlled trial. Lancet Respir Med. 2018;6:747–758.
- Lipson DA, Barnacle H, Birk R, et al. FULFIL trial: once-daily triple therapy for patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2017;196:438–446. doi:10.1164/rccm.201703-0449OC
- Lipson DA, Barnhart F, Brealey N, et al. Once-daily single-inhaler triple versus dual therapy in patients with COPD. N Engl J Med. 2018;378:1671–1680. doi:10.1056/NEJMoa1713901
- Singh D, Papi A, Corradi M, et al. Single inhaler triple therapy versus inhaled corticosteroid plus long-acting β2-agonist therapy for chronic obstructive pulmonary disease (TRILOGY): a double-blind, parallel group, randomised controlled trial. Lancet. 2016;388:963–973. doi:10.1016/S0140-6736(16)31354-X