
Abstract
The well-recognized individual heterogeneity within COPD patients has led to a growing interest in greater personalization in the approach of these patients. Thus, the treatable traits strategy has been proposed as a further step towards precision medicine in the management of chronic airway disease, both in stable phase and acute exacerbations. The aim of this paper is to perform a critical review on the treatable traits strategy and propose a guide to approach COPD patients in the light of this new concept. An innovative stepwise approach is proposed – a multidisciplinary model based on two distinct phases, with the potential to be implemented in both primary care and hospital settings. The first phase is the initial and focused assessment of a selected subset of treatable traits, which should be addressed in all COPD patients in both settings (primary care and hospital). As some patients may present with advanced disease at diagnosis or may progress despite this initial treatment requiring a more specialized assessment, they should progress to a second phase, in which a broader approach is recommended. Beyond stable COPD, we explore how the treatable traits strategy may be applied to reduce the risk of future exacerbations and improve the management of COPD exacerbations. Since many treatable traits have already been related to exacerbation risk, the strategy proposed here represents an opportunity to be proactive. Although it still lacks prospective validation, we believe this is the way forward for the future of the COPD approach.
Introduction
Over the last 20 years, the management of chronic obstructive pulmonary disease (COPD) has undergone significant changes.Citation1,Citation2 In the first Global Initiative for Chronic Obstructive Lung Disease (GOLD) document, published in 2001,Citation3 the classification and management of COPD were based solely on the severity of airflow limitation: this was the so-called FEV1-centric approach.Citation1 As a result of the intensive research in this area, GOLD moved towards a more patient-centric approach, de-emphasising the importance of FEV1 in favour of symptoms and exacerbation history.Citation2 In 2019, the need for individualised follow-up was addressed, along with the introduction of new treatment algorithms.Citation4 This recent trend indicates that we are moving towards a precision medicine approach in COPD. Similarly, other guidelines, such as the Czech guidelines, already advocate a more personalised treatment strategy, with a phenotype-based concept but also incorporates some elements of the treatable traits strategy by recognising that a patient can be characterised by more than in phenotype and by treating all phenotypical labels that apply.Citation5
A careful analysis of the evolution of COPD management reveals that the natural history of the disease could only be modified with personalised treatment strategies. This was evidenced by the results obtained with: i) smoking cessation in smokers;Citation6 ii) long-term oxygen therapy in COPD patients with chronic hypoxia;Citation7 and iii) lung-volume reduction surgery, in a subset of emphysematous COPD patients.Citation8 In recent years, triple therapy has also been shown to modify the natural history of the disease in exacerbators.Citation9 Other strategies have shown promising results, such as alpha-1-antitrypsin (AAT) augmentation therapy and lung transplant.Citation10–Citation12 In all these studies, patients were approached through their individual characteristics and treated accordingly.
There is significant individual heterogeneity within COPD.Citation13 This reflects different biological and physiological mechanisms underlying different clinical presentations: endotypes and phenotypes respectively.Citation13–Citation15 In 2010, a variation of the phenotype concept was proposedCitation16 that encompasses clinically meaningful outcomes. In the last decade, intensive research has been conducted to identify the underlying biological mechanisms that result from the complex interaction between the genetic background and cumulative environmental exposures.Citation13,Citation17 This research has culminated in the emergence of the Treatable Traits (TT) strategy: a “new strategy where patients are individually assessed for a specified set of treatable problems, and an individualised treatment programme is developed and implemented based on this multidimensional assessment”.Citation18 In this context, a TT can be defined as a “therapeutic target identified by phenotype or endotype, through validated biomarker(s)”.Citation18
The TT strategy acknowledges that several phenotypes can co-exist in the same patient and that all must be addressed.
The key message of this strategy is that TTs are not mutually exclusive.Citation18 Indeed, several TTs can be addressed in a COPD patient, and an individualised treatment programme shall be developed in a multidimensional approach.Citation18
Many researchers consider this strategy a first step towards deconstructing existing labels such as asthma and COPD. Within this label-free approach, several candidate traits have already been identified for chronic airway diseases.Citation14,Citation15,Citation18,Citation19 Some authors have also explored this approach to manage asthma and COPD individually.Citation20–Citation23
Considering the potential impact of the TT strategy on COPD patients, healthcare professionals would greatly benefit from harmonised recommendations based on the research conducted so far. The aim of this paper is to perform a critical review on the TT strategy and propose a guide to approach COPD patients in the light of this new concept.
Treatable Traits for COPD
Treatable traits should fulfil three characteristics: be clinically relevant and associated with specific outcomes (symptoms, health status, risk of future events), be easily identifiable and measurable, and be treatable.Citation15,Citation18
The identification of a TT should be carried out objectively through a biomarker. The classic and best established biomarker in COPD is alpha-1-antitrypsin (AAT) levels. In fact, the quantitative determination of AAT levels in blood is crucial to identify deficiency of AAT – a treatable trait.Citation10
However, and because those markers, besides biological, may be functional, imaging or clinical, the term TIM – treat identification markerCitation18 has been proposed. In the setting of the discussion herein proposed, we consider that this term is more appropriate and will therefore be adopted it in the following sections of this article. It should be ensured that the markers are feasible and easy to measure.
GOLD recognizes two major treatable traits in COPD – dyspnea and exacerbations.Citation24 Furthermore it recommends that follow-up regarding pharmacological and non-pharmacological treatment should be based on these two traits. However, should they be regarded as treatable traits or as therapeutic goals? A Spanish group published a critical analysis of the treatable traits approach and introduced the concept of therapeutic goal ().Citation19 According to this group, therapeutic goals ‘are not therapeutic targets, but rather clinical problems that must be eliminated or improved’.Citation19 For each therapeutic goal, there is a set of treatable traits. Thus, the treatable traits to address must consider the selected therapeutic goal. For example, in a patient whose therapeutic goal is symptom control, the TTs to address should only be those that have been proven to be related to the symptoms. Likewise, a given treatable trait may be associated with different therapeutic goals.
Figure 1 Definition of therapeutic goals and treatable traits. The numbers and letters are for illustrative purposes only.
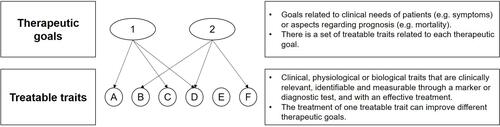
We have identified some issues regarding the therapeutic goals approach. Firstly, some therapeutic goals such as mortality are common to all COPD patients. Secondly, there is a risk of selecting some therapeutic goals over others, reducing the overall benefit of this approach. Addressing all potential treatable traits, although more complex, allows meeting the individual variability of COPD patients.
In the treatable traits strategy, most authorsCitation14,Citation18 dot not consider dyspnea and exacerbations as treatable traits, since there are several traits that can be related to them. The treatable traits identified in most publications are specific characteristics, measurable through a marker or diagnostic test and with an effective treatment.
They were divided into three main groups: pulmonary, extrapulmonary, and behavioral.Citation14
An important question arises: how to assess TTs?
The key point of this approach is the importance and priority given to each TT during patient assessment. In this process, attention shall be paid to identifying appropriate TTs, based on their i) clinical impact; ii) prevalence, iii) impact on specific disease outcomes; iv) impact on the patient; and v) availability of measurement methods.Citation14 With this in mind, two approaches have been proposed:Citation18
i) a broad approach, in which the TTs are assessed all at once. This systematic assessment may achieve the greatest benefit by meeting the individual heterogeneity of COPD patients. However, it increases complexity and is more time consuming, limiting its feasibility, especially in primary care.
ii) a focused approach, in which only some treatable traits are assessed. Although easier to implement, it raises some questions about the priority of some TTs over others. The recognized individual variability in COPD limits the potential benefits of such an approach.
The possibility of a phased-approach has already been mentioned,Citation18 but to our knowledge there is no guide proposed with this type of approach yet.
We, herein, suggest a phased-approach – a multidisciplinary model based on two distinct phased strategies to be adopted independently, in sequence, or with some degree of overlap, with the potential to be implemented in both primary care and hospital settings. By hospital setting, we mean care by respiratory specialists, whether provided in hospital outpatient departments, in outpatient clinics, or even in inpatient settings.
Initially, patients should be assessed using a focused approach, with one subset of TTs being addressed in all patients with COPD. However, some patients may present with advanced disease at diagnosis or may progress despite this initial treatment. These patients require more specialized assessment and should progress to a second phase, in which a broader approach is recommended.
In this paper, we will be using the terms:
- first phase, meaning the initial and focused assessment that shall be performed on each COPD patient, in both settings (primary care and hospital);
- second phase, meaning the extended approach that shall be implemented in severe and progressive cases where a more refined assessment is warranted. This second phase shall ideally be implemented in the hospital setting.
Regarding COPD, the TT approach proposed here considers both stable disease and exacerbations.
Treatable Traits in Stable COPD
The pulmonary, extrapulmonary, and behavioral treatable traits proposed to be addressed in the first and second phases, along with the corresponding TIM and therapeutic approaches, are presented in and .
Table 1 Treatable Traits to Be Addressed in the First Phase
Table 2 Treatable Traits to Be Addressed in the Second Phase
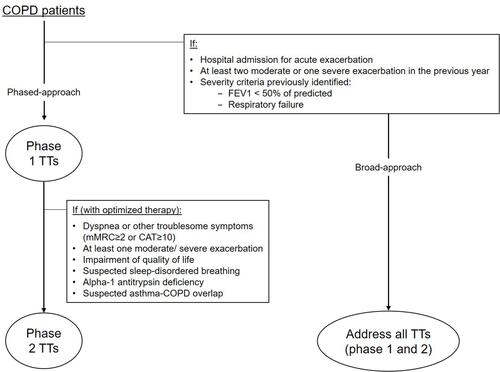
The treatable traits included in the first phase () are well known among the medical community and easily measured, by non-respiratory physicians, using widely available biomarkers. In addition, they provide essential information for initial diagnosis and treatment proposal. Like most authors, we are not considering frequent exacerbations as a treatable trait, as several TTs may be related to it. However, the initial assessment regarding the history of exacerbations is extremely important as these patients deserve a more accurate and comprehensive assessment. Patients with frequent exacerbations should have a broad approach right from the start, with assessment of all treatable traits, which allows the identification of different therapeutic pathways. In , patients who benefit from a broad approach as an initial assessment are identified.
Figure 2 Algorithm for COPD management based on the treatable traits strategy.
Some TTs are present in both phases, reflecting different TIMs and/or different treatments. AAT deficiency, for example, should be investigated in every COPD patient using a widely available and inexpensive biomarker – quantitative determination of serum AAT.Citation25 If low AAT levels are found, patients should progress to the second phase, where this trait will have a more refined assessment through phenotyping and genotyping, and other traits will also be addressed. It is important to acknowledge that AAT levels should be assessed outside of inflammatory and infectious processes, as AAT behaves as an acute phase protein.Citation26
Also, chronic bronchitis takes part of both phases. It is easily identified in the first phase and can be addressed initially by smoking cessation and mucolytics. More specific treatments like phosphodiesterase-4 (PDE-4) inhibitors should be reserved for the second phase.
Depending on the patient’s response to the proposed treatment, it might be necessary to resort to the second phase to identify the traits that underlie disease progression.
However, an important question remains: when should COPD patients progress to the second phase, and which patients would benefit from the broad approach (concomitant first and second phases) at diagnosis?
According to our proposal, this transition should be based on the level of severity ().
Eosinophilic Airway Inflammation
The role of eosinophils in the pathophysiology of COPD is not entirely understood. In contrast to asthma, COPD was traditionally regarded as a mainly neutrophilic inflammatory disease. However, increased numbers of eosinophils have been detected in the airways of COPD patients, from sputum to bronchoalveolar lavage.Citation27 Indeed, in a subset of COPD patients, eosinophilic airway inflammation may be present both in stable disease and during exacerbations.Citation28,Citation29
Why is eosinophilic inflammation a treatable trait? Firstly, it relates to clinically important outcomes: an increased blood eosinophil count (BEC) in stable phase is related to increased risk of exacerbationsCitation30,Citation31 and increased decline in lung function.Citation32,Citation33 Furthermore, it has been shown to predict therapeutic response. The presence of eosinophilic airway inflammation has been consistently associated with response to inhaled corticosteroids (ICS) treatment in post-hocCitation33,Citation34 and pre-specified analyses of randomized controlled trials.Citation35 The GOLD document already recognizes BEC as a biomarker to guide ICS therapy in patients with COPD.Citation36 This treatable trait is identifiable and measurable through a TIM – BEC. Previous studies have considered sputum eosinophil counts.Citation21 However, it raises questions regarding accessibility and reproducibility (as patients do not always provide adequate samples).Citation24 BEC is widely available, demonstrates a good correlation with sputum eosinophil counts and may be used as a surrogate measure for airway eosinophilia in COPD.Citation37 Most authors consider that BEC should be regarded as a continuous variable rather than a dichotomous one. In fact, BEC is a dose-dependent variable, so different thresholds represent therapeutic responses of distinct magnitude.Citation24 Approximate thresholds have been suggested – some COPD studies suggest a relative threshold ≥2% of total white blood cells,Citation38,Citation39 while others suggest an absolute threshold.Citation9,Citation40 The GOLD report considers two absolute thresholds: 100 and 300 cells/μL blood. Studies consistently show that BEC below 100 eosinophils/μL is not associated with a clinical benefit of ICS in terms of exacerbation prevention. This benefit occurs in patients with BEC ≥100 eosinophils/μL, and a greater magnitude of response is expected when BEC ≥ 300 eosinophils/μL.Citation24
Some authors have studied the potential benefit of IL-5 targeted biological therapy in the subset of COPD patients with eosinophil-mediated airway inflammation, with promising results when patients are carefully selected.Citation41
What about neutrophilic airway inflammation in COPD? Neutrophils and neutrophil dysfunction are implicated in the inflammatory changes in the airways of COPD patients, causing chronic bronchitis and emphysema.Citation42 Airway neutrophilia in COPD has been associated with clinical severity,Citation43 disease progressionCitation44 and exacerbations.Citation45 However, there are no specific treatments available targeting this trait.Citation18 Rather, there are specific subsets of COPD patients generally related to neutrophilic airway inflammation that can be addressed in this TT approach, such as chronic bronchitis and chronic bronchial infection.Citation46,Citation47
Chronic Bronchial Infection
Over the last decade, several studies, based on culture-independent microbial sequencing, have demonstrated that the lung is not sterile. Instead, a complex microbial ecosystem exists – the lung microbiome.Citation48,Citation49 The majority of the microbiota plays an essential role in lung epithelial integrity, resistance to colonization, and homeostasis of the respiratory immune system.Citation50 However, it also contains potentially pathogenic microorganisms.Citation51
It has been shown that the composition of the lung microbiota differs in healthy individuals and in COPD patients, both in richness and diversity.Citation52 The composition of the microbiota varies along the bronchial tree and according to the stages of severity in COPD.Citation53,Citation54 More severe COPD is associated with reduced microbial diversity. Changes in lung microbiome diversity and abundance have a profound impact on respiratory immune system homeostasis and make the airways of COPD patients susceptible to opportunistic growth of pathogenic microorganisms – dysbiosis.Citation51 Indeed, studies have shown that in stable COPD, 25–50% of patients have bacterial growth in respiratory samples.Citation51,Citation55 In the absence of symptoms of acute infection, this isolation has been regarded as bacterial colonization. However, persistence of these bacteria leads to maladaptive immune responses, with deleterious consequences,Citation56 making the term chronic bronchial infection more adequate.Citation47
Chronic bronchial infection is more frequent in patients with concomitant bronchiectasis,Citation47 and potentially pathogenic microorganisms isolated include Haemophilus influenzae, Moraxella catarrhalis, Streptococcus pneumoniae and Pseudomonas aeruginosa.Citation51,Citation57 Chronic bronchial bacterial infection is an important TT to address – it has clinical relevance (for example, colonization of the airways with Haemophilus influenzae appears to be related to a more rapid decline in lung function and higher exacerbation rates), is feasible to identify, and is treatable, although the correct treatment is still under debate.Citation47
Although not considered treatable traits, attention should also be paid to fungi and mycobacteria.Citation17,Citation58,Citation59 The role of fungi in COPD is less well understood. Aspergillus species cause most fungal infections in COPD patients, but apart from the increased risk of invasive aspergillosis, the clinical significance of a positive filamentous fungal culture remains uncertain.Citation60,Citation61 Viruses are detected during half of COPD exacerbations, but the role of chronic viral infection is yet to be determined.Citation62
It should be borne in mind that the history of mycobacterial infection limits the ICS use in COPD patients, as an association between ICS use and the risk on nontuberculous mycobacterial pulmonary infection in this population has already been suggested.Citation63
Emphysema
Emphysema is a recognized treatable trait with undeniable clinical relevance,Citation64 identifiable and measurable through chest computed tomography (CT)Citation65 and treatable. Indeed, lung volume reduction surgery has been shown to increase survival in a subset of emphysematous COPD patients.Citation8 This evidence provides a solid basis for discussing the importance of imaging in the management of COPD.
Airway disease and pulmonary emphysema are the major determinants of airway obstruction in COPD.Citation66 It is undeniable that patients with predominantly airway disease and those with predominantly emphysema are distinct patients.Citation65 Furthermore, these determinants may coexist in the same patient to varying degrees,Citation66 and the relative contributions of each determinant may be assessed by imaging.Citation67 Chest CT enables objective quantification of each determinant,Citation62 more than a visual assessmentCitation68–Citation70 allowing identification of TTs.
Chest CT has other advantages: i) it excludes alternative diagnoses; ii) it establishes the presence of pulmonary comorbidities that are often related to COPD, such as bronchiectasis, diffuse lung disease, and lung cancer; and iii) it assesses the need for both lung surgery and transplantation.Citation4,Citation71
More than emphysema itself, it is already recognised that the occurrence of lung hyperinflation (LH) is related to symptoms, decreased exercise capacity, occurrence of exacerbations and is an independent predictor of mortality.Citation20,Citation72–Citation75 We consider LH as a treatable trait to be addressed by respiratory physicians in Phase II. Conventionally, LH is defined as an increase in total lung capacity (TLC) > 120% of the predicted value. Several authors have suggested that this definition should be avoided, but there is still no consensus on the definition or classification of severity. Definitions based on residual volume (RV), functional residual capacity (FRC), RV/TLC or IC/TLC (IC: inspiratory capacity) have been proposed.Citation76,Citation77 In this document, we define LH as a reduced ratio IC/TLC. Indeed, this measure, with a cutoff of ≤25%, has already demonstrated a relationship with poor outcomes such as mortality.Citation72,Citation73,Citation75
Systemic Inflammation
COPD is increasingly considered a multisystemic disease, with airway and systemic inflammation.Citation78 High levels of several inflammatory markers have been found in COPD patients, indicating the presence of persistent systemic inflammation.Citation79 This is also considered a treatable trait by most authors.Citation14,Citation15,Citation18,Citation21 In fact, systemic inflammation is related to worse outcomes, such as increased exacerbation rates and increased all-cause mortality.Citation80 A link between systemic inflammation and increased risk of cardiovascular disease, diabetes, lung cancer, and pneumonia has also been detected.Citation81
In 2013, a pilot study addressing treatable traits in COPD used an inflammometry algorithm, addressing airway inflammation (eosinophilic and neutrophilic) and systemic inflammation. In fact, inflammatory processes are not mutually exclusive, and a patient may exhibit more than one and require more than one therapeutic approach.Citation21
Several inflammatory markers have already been used to identify systemic inflammation in COPD. However, in the TT strategy, availability and feasibility are required, making C-Reactive Protein (CRP) the appropriate TIM.Citation14,Citation18,Citation21 The proposed cut-off for CRP to detect systemic inflammation is 3 mg/L.Citation18,Citation21
Some meta-analyses have found a beneficial effect of statins on clinical outcomes in COPD patients.Citation82,Citation83 McDonald and colleagues described improvements in health-related quality of life (HRQoL) when targeting systemic inflammation with statins.Citation21,Citation84
Comorbidities
COPD often coexists with other diseases. In 2012, the impact of comorbidities on COPD was highlighted with the development of a COPD-specific comorbidity test score (COTE index).Citation85 A COTE score ≥ 4 points proved to be associated with an increased risk of death in each quartile of the BODE index. Comorbidities that contributed to increased risk of death were displayed graphically in the so-called “COPD comorbidome”.Citation85
Cardiovascular comorbidities are highly prevalent in COPD patients,Citation86 and recently complex cardio-respiratory interactions have been identified – many authors refer to a “cardiopulmonary continuum”Citation87 – with an important link to the systemic inflammation discussed above.
The TT strategy recommends that comorbidities be researched and addressed from an integrative perspective to improve outcomes in COPD patients.
Particular mention should be made regarding osteoporosis. In fact, most published reference articles on the TT strategy do not mention it as a treatable trait. Lately, there has been increasing evidence linking the presence of osteoporosis, especially osteoporotic fractures, with poor outcomes in COPD, making it a potential treatable trait to address.Citation88,Citation89 Recognising that COPD-associated osteoporosis is under-assessed and undertreated, and that osteoporotic fractures have profound impact on the quality of life of patients with COPD, we have included osteoporosis as a treatable trait.
Treatable Traits Applied to COPD Exacerbations
Exacerbations, defined as acute worsening of respiratory symptoms resulting in additional therapy, are major events with a negative impact on COPD patients.Citation4 Indeed, research has demonstrated their association with worse clinical outcomes, such as accelerated decline in lung function, increased rates of hospital admissions and readmissions, poor quality of life, worsening of underlying comorbidities and increased mortality.Citation17,Citation58,Citation75,Citation90
According to GOLD report, moderate exacerbations are defined as an acute worsening of respiratory symptoms that results in additional therapy with antibiotics and/or oral corticosteroids and severe exacerbations those requiring hospitalisation or an emergency department visit. Severe exacerbations should be distinguished from moderate ones, as they pose significantly more risks.Citation91,Citation92 In fact, following a hospitalization for COPD exacerbation, the 1-year mortality risk is 25%;Citation93 this figure is higher than that observed following hospital admission for acute myocardial infarction.Citation94
Despite advances in the management and treatment of COPD, exacerbation rates remain high, with a considerable burden on healthcare systems.Citation95 This trend calls for specific action, towards the management of these events, as well as their risk factors.
The TT approach has been traditionally applied to the management of stable COPD. Some authors have looked at its application to exacerbations, particularly for risk assessment and management of these events.Citation18,Citation22,Citation59
We, herein, aim to explore how the TT strategy can be applied to reduce the risk of future exacerbations and improve the management of COPD exacerbations.
Risk of Exacerbation
Several factors have been associated with an increased risk of COPD exacerbations.Citation4 However, the strongest predictor for a future exacerbation remains the history of exacerbations in the previous year,Citation96 and this is the only risk factor addressed in most COPD guidelines.Citation4 From the ECLIPSE study, it is known that after a first exacerbation, the risk of having a second event more than doubles. After a second exacerbation, the risk of a future event more than quintuplicates.Citation96
A question arises: should we wait for the first exacerbation to occur? Or should we be proactive?
The TT strategy represents an opportunity to be proactive. It allows for addressing TTs already related to exacerbation risk ():
In a patient with no previous exacerbations, the first phase in the TT approach proposed here contains some of the TTs related to exacerbation risk.
After a first moderate/severe exacerbation, the focus should be on the prevention of future events and thus we propose that patients progress to the second phase, in which all these TTs can be addressed.
Table 3 Treatable Traits Associated with Increased Risk of Exacerbation*
The effectiveness of this approach in preventing exacerbations remains to be determined.
Finally, we acknowledge hospitalization as a golden opportunity to apply the TT strategy. There is no denying the major impact of hospitalizations on the natural course of COPD – increased risk of future events, delayed recovery, impaired quality of life and mortality.Citation95–Citation97 This approach, in the hospital setting, is facilitated for readier access to diagnostic tests (to characterize TIMs) and a multidisciplinary team approach. However, this does not apply to all TTs as many traits need to be assessed in a stable phase. These should be addressed at reassessment ≥ 4 weeks after discharge from hospital.
Exacerbation Management
Research and clinical practice have highlighted that the management of COPD exacerbations depends on a variety of factors. At present, some studies have identified TTs that can guide the management of these events and improve outcomes.Citation18,Citation98,Citation99
The GOLD document already mentions the importance of sputum color and biomarkers, such as CRP and procalcitonin, for the management of exacerbations, namely, to guide the use of antibiotics during these events.Citation4
As exacerbations are heterogeneous disease states (varying in terms of clinical manifestations, etiology and response to treatment), patients may benefit from a systematic identification of associated traits that would guide their management.Citation17 Understanding the biological mechanisms underlying exacerbations and grouping them according to their etiology seems to be an effective way to improve intervention strategies. In this context, an approach based on the acronym ABCDEFGX – Airway viral infection, Bacterial infection, Coinfection, Depression/anxiety, pulmonary Embolism, cardiac Failure (or failure of lung integrity-pneumothorax), General environment and X (unknown) – has been proposed.Citation100–Citation102 This acronym-based approach was evaluated in a pilot study with patients hospitalized due to COPD exacerbations.Citation101 To identify etiologic phenotypes, patients underwent sputum culture, nasopharyngeal swab (for respiratory viruses), chest X-ray, serum white blood cells, CRP measurement, and application of the Hospital Anxiety and Depression Scale. Changes in patients’ environment were addressed and the investigation of pulmonary embolism was left to the decision of the attending physician. This study highlighted the clinical relevance of characterizing exacerbations by using available methods in routine clinical practice.
In a study by Bafadhel and colleagues, four clusters of acute exacerbation were identified: bacterial, viral, eosinophilic predominant and pauci-inflammatory.Citation17 These clusters were clinically indistinguishable, creating the need to find biomarkers. Randomized controlled trials (RCTs) were then designed to validate a biomarker-driven approach in exacerbation management, with promising results.Citation103–Citation105 These RCTs showed that this targeted approach has the potential to reduce treatment failure and minimize adverse effects by reducing unnecessary treatment.
Classification of COPD exacerbations according to their causative agent seems to be the most consensual approach: bacterial infection, viral infection, increased eosinophilic inflammation, and others (eg enhanced exposure to noxious agents).Citation22
Bacterial Infection
Despite the widespread use of antibiotics, bacteria are responsible for only about 50% of all COPD exacerbations.Citation106,Citation107 Current approaches to exacerbation management lack a reliable marker of bacterial infection that would guide antibiotic prescribing in a targeted manner. Some markers have been proposed. Clinical markers such as the Anthonisen criteria and sputum color are subjective and lack sensitivity and specificity.Citation22,Citation108 The most commonly referred biomarkers are CRP and procalcitonin.
The CRP-guided approach in COPD exacerbations has been shown to reduce antibiotic use without affecting clinical outcomes, both in primary careCitation109 and in hospital admissionsCitation103 with thresholds of 40 mg.L−1 and 50 mg.L−1 for antibiotic prescribing, respectively.
Procalcitonin has also been regarded as a useful biomarker in guiding antibiotic therapy. However, a recent meta-analysis contradicted these resultsCitation110 and therefore further investigation is warranted.
Viral Infection
Viruses, mainly rhinovirus, influenza, and respiratory syncytial virus, have been detected in 30–50% of COPD exacerbations.Citation102,Citation111,Citation112
There is also a subset of COPD exacerbations with bacterial and viral coinfection, which is related to poorer outcomes such as increased length of hospital stay.Citation21 Concurrent or recent upper respiratory symptoms or coryza may indicate viral etiology, but also coinfection. Some biomarkers have been studied, but a reliable biomarker of viral infection in COPD exacerbations remains to be identified.
Further research is needed to support new therapeutic strategies. In the meantime, prevention through vaccines is recommended to decrease the risk of exacerbation, the frequency of exacerbation and the morbidity associated with COPD.
Increased Eosinophilic Inflammation
As in the stable phase, eosinophilic airway inflammation has been identified as an important TT in the management of COPD exacerbations. Since it is associated with a lower length of hospital stay and reduced mortality, it has prognostic significance.Citation99 In fact, eosinopenia (BEC<50 cell/µL) correlates with worse clinical outcomes and is therefore being considered a poor prognostic factor.Citation99 Moreover, there has been evidence of an inverse relationship between blood eosinophil counts and bacterial infection, in COPD exacerbations.Citation113
Just as BEC predicts therapeutic response to inhaled corticosteroids in stable COPD, it also predicts therapeutic response to systemic corticosteroids during exacerbation. A post-hoc analysis of 3 RCTs showed that patients with BEC≥2% who did not receive oral corticosteroids had significantly more treatment failure than patients who did.Citation114 Similarly, treatment with oral corticosteroids in patients with BEC<2% showed no benefit. In severe exacerbations, the Corticosteroid Reduction in COPD trial (CORTICO-COP)Citation105 applied a BEC-based algorithm to guide oral corticosteroid treatment – prednisolone was prescribed on days with BEC≥300 cell/μL, for a maximum of 5 days, and compared with standard treatment. The eosinophil-guided approach had similar outcomes, while reducing systemic corticosteroid exposure by 60%. This systemic steroid-sparing strategy may minimize harm by reducing unnecessary treatment. Given the variability in blood eosinophil counts during COPD exacerbations, the appropriate threshold for guiding oral corticosteroid treatment is still under debate.
Others
Pulmonary embolism (PE) is one of the other causes of COPD exacerbations and has a prevalence of 20–25% among unexplained COPD exacerbations.Citation115 However, many of these are subsegmental PEs and may not be clinically relevant.Citation116 More research is warranted before a systematic assessment of PE can be proposed.
A clinical trial of over 16.000 COPD patients with cardiovascular disease or risk factors for cardiovascular disease demonstrated that acute exacerbations increase the risk of subsequent cardiovascular events, especially in the first 30 days after exacerbation.Citation117 European experts now recommend cardiovascular risk assessment in all hospitalized patients with an exacerbation of COPD. They recommend that troponin and Brain Natriuretic Peptide (BNP) be assessed, within 4 hours of admission.Citation118
Based on the research to date, and the availability and feasibility of trait identification markers and therapeutic options, we propose two major TTs in the management of COPD exacerbations with respect to etiology:
bacterial infection
increased eosinophilic inflammation.
Discussion
The high morbidity and mortality associated with COPD require a change regarding the management of this condition. A strategy based on the TT approach may create conditions to improve the quality of life and survival of COPD patients.
Some personalized approaches are already in place in COPD management. In daily practice, physicians choose the right inhaler for the right patient and respiratory rehabilitation is probably one of the best current examples of multidimensional and personalized approaches in COPD.
On the other hand, many patients are still assessed in a one-size-fits-all format. This is evident, for example, during the management of most acute exacerbation events, which are still approached conservatively, with double prescription of antibiotics and systemic corticosteroids, most often disregarding what might have triggered the event.
Recent advances in more personalized approaches have been proposed, but far from the level of personalization already seen in other therapeutic areas.
Our multidisciplinary TT model for addressing COPD, based on a two-phase strategy, considers distinct disease stages and severity as a means of ensuring appropriate assessment and treatment of all patients by primary care physicians (in an early or less severe stage) and respiratory physicians (in non-responders and severe disease). However, the implementation of a TT approach introduces a wide range of additional parameters to the standard routine, increasing the complexity, costs, and length of consultations. In addition, the multidisciplinary nature of this strategy requires extended and reinforced teams comprising specialized healthcare professionals who can intervene and manage identified TTs. All these aspects may create resistance to its widespread implementation. Still, as tailored treatment strategies are generally more effective and allow better risk-benefit ratios, we believe that the benefits will soon outweigh the costs of the initial stage.
Given the complexity, some authors propose that the TTs to be address should be more focused, according to the selected therapeutic goal,Citation19 as mentioned above. However, the authors also recognize that most patients have multiple therapeutic goals and that some, such as mortality, should be assessed ubiquitously.Citation119 This calls for a serious investment in the identification of therapeutic markers in the stable stages of the disease.
This strategy cannot translate into reality without adequate validation of the TT approach in the setting of specifically designed clinical trials, which would compare the outcomes of traditional assessment with those of a TT approach. In line with this requirement, McDonald and colleaguesCitation21 designed a pilot study to validate a strategy developed to identify therapeutic targets and implement an individualized treatment program based on inflammometry, multidimensional assessment and case management. The authors proved that this strategy could result in tangible benefits for COPD patients, mainly in terms of quality of life.Citation21,Citation84
In conclusion, the treatable traits strategy has been proposed as a step towards precision medicine in the management of chronic airway diseases in both stable phase and acute exacerbation. This article sought to provide a guide for clinical practice in the application of this strategy to COPD. Although its prospective validation is still lacking, we believe that this is the way forward for the future of the COPD approach.
Acknowledgments
Medical writing support for this article was provided by Paula Pinto, PhD, of PMA – Pharmaceutical Medicine Academy and was funded by Bial. All authors contributed equally to this work and should be considered co-first authors for this study.
Disclosure
Prof. Dr. João Cardoso reports personal fees from Astra Zeneca, GSK, Bial, Boehringer Ingelheim, Mylan and Novartis, outside the submitted work. Prof. Dr. António Jorge Ferreira reports personal fees from TEVA Pharma, Bial, GSK, Boehringer Ingelheim and Mylan; and personal fees and non-financial support from Menarini, outside the submitted work. Dr. Miguel Guimarães reports personal fees from GSK, Novartis, Menarini, Bial and Boehringer Ingelheim, outside the submitted work. Dr. Ana Sofia Oliveira reports personal fees from Medinfar, GSK, Bial, Novartis and Menarini, outside the submitted work. Dr. Paula Simão reports personal fees from Bial, GSK, Novartis and Boehringer Ingelheim, outside the submitted work. Dr. Maria Sucena reports personal fees and non-financial support from Bial, CSL Behring and Grifols, outside the submitted work. The authors report no other conflicts of interest in this work.
Additional information
Funding
References
- Agusti A. The path to personalised medicine in COPD. Thorax. 2014;69(9):857–864. doi:10.1136/thoraxjnl-2014-205507
- Vogelmeier CF, Criner GJ, Martinez FJ, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 report. GOLD executive summary. Am J Respir Crit Care Med. 2017;195(5):557–582. doi:10.1164/rccm.201701-0218PP
- Pauwels R. Global initiative for chronic obstructive lung diseases (GOLD): time to act. Eur Respir J. 2001;18(6):901–902. doi:10.1183/09031936.01.0027401
- Global Initiative for Chronic Obstructive Lung Disease - GOLD. Global strategy for the diagnosis, management and prevention of chronic obstructive pulmonary disease; 2021.
- Zatloukal J, Brat K, Neumannova K, et al. Chronic obstructive pulmonary disease - diagnosis and management of stable disease; a personalized approach to care, using the treatable traits concept based on clinical phenotypes. Position paper of the Czech Pneumological and Phthisiological Society. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2020;164(4):325–356. doi:10.5507/bp.2020.056
- Anthonisen NR, Skeans MA, Wise RA, et al. The effects of a smoking cessation intervention on 14.5-year mortality: a randomized clinical trial. Ann Intern Med. 2005;142(4):233–239. doi:10.7326/0003-4819-142-4-200502150-00005
- Cranston JM, Crockett AJ, Moss JR, Alpers JH. Domiciliary oxygen for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2005;4:CD001744. doi:10.1002/14651858.CD001744.pub2
- Fishman A, Martinez F, Naunheim K, et al. A randomized trial comparing lung-volume-reduction surgery with medical therapy for severe emphysema. N Engl J Med. 2003;348(21):2059–2073. doi:10.1056/NEJMoa030287
- Lipson DA, Criner GJ, Lomas DA. Single-inhaler triple versus dual therapy in patients with COPD. N Engl J Med. 2018;379(6):592–593. doi:10.1056/NEJMc1807380
- Chapman KR, Burdon JGW, Piitulainen E, et al. Intravenous augmentation treatment and lung density in severe α1 antitrypsin deficiency (RAPID): a randomised, double-blind, placebo-controlled trial. Lancet. 2015;386(9991):360–368. doi:10.1016/S0140-6736(15)60860-1
- Rahaghi FF, Monk R, Ramakrishnan V, Beiko T, Strange C. Alpha-1 antitrypsin augmentation therapy improves survival in severely deficient patients with predicted FEV1 between 10% and 60%: a retrospective analysis of the NHLBI alpha-1 antitrypsin deficiency registry. Int J Chron Obstruct Pulmon Dis. 2020;15:3193–3199. doi:10.2147/COPD.S263725
- Vock DM, Durheim MT, Tsuang WM, et al. The survival benefit of lung transplantation in the modern era of lung allocation. Ann Am Thorac Soc. 2017;14:172–181. doi:10.1513/AnnalsATS.201606-507OC
- Agustí A, Celli B, Faner R. What does endotyping mean for treatment in chronic obstructive pulmonary disease? Lancet. 2017;390(10098):980–987. doi:10.1016/S0140-6736(17)32136-0
- Agusti A, Bel E, Thomas M, et al. Treatable traits: toward precision medicine of chronic airway diseases. Eur Respir J. 2016;47(2):410–419. doi:10.1183/13993003.01359-2015
- Agustí A, Bafadhel M, Beasley R, et al. Precision medicine in airway diseases: moving to clinical practice. Eur Respir J. 2017;50(4):1701655. doi:10.1183/13993003.01655-2017
- Han MK, Agusti A, Calverley PM, et al. Chronic obstructive pulmonary disease phenotypes: the future of COPD. Am J Respir Crit Care Med. 2010;182(5):598–604. doi:10.1164/rccm.200912-1843CC
- Bafadhel M, McKenna S, Terry S, et al. Acute exacerbations of chronic obstructive pulmonary disease: identification of biologic clusters and their biomarkers. Am J Respir Crit Care Med. 2011;184(6):662–671. doi:10.1164/rccm.201104-0597OC
- McDonald VM, Fingleton J, Agusti A, et al. Treatable traits: a new paradigm for 21st century management of chronic airway diseases: Treatable Traits Down Under International Workshop report. Eur Respir J. 2019;53:5. doi:10.1183/13993003.02058-2018
- Pérez de Llano L, Miravitlles M, Golpe R, et al. A proposed approach to chronic airway disease (CAD) using therapeutic goals and treatable traits: a look to the future. Int J Chron Obstruct Pulmon Dis. 2020;15:2091–2100. doi:10.2147/COPD.S263430
- van Dijk M, Gan CT, Koster TD, et al. Treatment of severe stable COPD: the multidimensional approach of treatable traits. ERJ Open Res. 2020;6(3):00322–2019. doi:10.1183/23120541.00322-2019
- McDonald VM, Higgins I, Wood LG, Gibson PG. Multidimensional assessment and tailored interventions for COPD: respiratory utopia or common sense? Thorax. 2013;68(7):691–694. doi:10.1136/thoraxjnl-2012-202646
- Mathioudakis AG, Janssens W, Sivapalan P, et al. Acute exacerbations of chronic obstructive pulmonary disease: in search of diagnostic biomarkers and treatable traits. Thorax. 2020;75(6):520–527. doi:10.1136/thoraxjnl-2019-214484
- McDonald VM, Hiles SA, Godbout K, et al. Treatable traits can be identified in a severe asthma registry and predict future exacerbations. Respirology. 2019;24(1):37–47. doi:10.1111/resp.13389
- Singh D, Agusti A, Anzueto A, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease: the GOLD science committee report 2019. Eur Respir J. 2019;53:5. doi:10.1183/13993003.00164-2019
- Miravitlles M, Dirksen A, Ferrarotti I, et al. European Respiratory Society statement: diagnosis and treatment of pulmonary disease in α 1 -antitrypsin deficiency. Eur Respir J. 2017;50(5):1700610. doi:10.1183/13993003.00610-2017
- Lopes AP, Mineiro MA, Costa F, et al. Portuguese consensus document for the management of alpha-1-antitrypsin deficiency. Pulmonology. 2018;24(Suppl 1):1–21. doi:10.1016/j.pulmoe.2018.09.004
- Rutgers SR, Timens W, Kaufmann HF, van der Mark TW, Koëter GH, Postma DS. Comparison of induced sputum with bronchial wash, bronchoalveolar lavage and bronchial biopsies in COPD. Eur Respir J. 2000;15(1):109–115. doi:10.1183/09031936.00.15110900
- Brusselle G, Pavord ID, Landis S, et al. Blood eosinophil levels as a biomarker in COPD. Respir Med. 2018;138:21–31. doi:10.1016/j.rmed.2018.03.016
- Saha S, Brightling CE. Eosinophilic airway inflammation in COPD. Int J Chron Obstruct Pulmon Dis. 2006;1(1):39–47. doi:10.2147/copd.2006.1.1.39
- Vedel-Krogh S, Nielsen SF, Lange P, Vestbo J, Nordestgaard BG. Blood eosinophils and exacerbations in chronic obstructive pulmonary disease. The Copenhagen General Population Study. Am J Respir Crit Care Med. 2016;193(9):965–974. doi:10.1164/rccm.201509-1869OC
- Kerkhof M, Freeman D, Jones R, Chisholm A, Price DB; Respiratory Effectiveness Group. Predicting frequent COPD exacerbations using primary care data. Int J Chron Obstruct Pulmon Dis. 2015;10:2439–2450. doi:10.2147/COPD.S94259
- Rogliani P, Ora J, Puxeddu E, Cazzola M. Airflow obstruction: is it asthma or is it COPD? Int J Chron Obstruct Pulmon Dis. 2016;11:3007–3013. doi:10.2147/COPD.S54927
- Barnes PJ. Inflammatory mechanisms in patients with chronic obstructive pulmonary disease. J Allergy Clin Immunol. 2016;138(1):16–27. doi:10.1016/j.jaci.2016.05.011
- Bafadhel M, Peterson S, De Blas MA, et al. Predictors of exacerbation risk and response to budesonide in patients with chronic obstructive pulmonary disease: a post-hoc analysis of three randomised trials. Lancet Respir Med. 2018;6(2):117–126. doi:10.1016/S2213-2600(18)30006-7
- Pascoe S, Barnes N, Brusselle G, et al. Blood eosinophils and treatment response with triple and dual combination therapy in chronic obstructive pulmonary disease: analysis of the IMPACT trial. Lancet Respir Med. 2019;7(9):745–756. doi:10.1016/S2213-2600(19)30190-0
- Singh S, Verma SK, Kumar S, et al. Correlation of severity of chronic obstructive pulmonary disease with potential biomarkers. Immunol Lett. 2018;196:1–10. doi:10.1016/j.imlet.2018.01.004
- Schleich F, Corhay J-L J-L, Louis R. Blood eosinophil count to predict bronchial eosinophilic inflammation in COPD. Eur Respir J. 2016;47(5):1562–1564. doi:10.1183/13993003.01659-2015
- Pascoe S, Locantore N, Dransfield MT, Barnes NC, Pavord ID. Blood eosinophil counts, exacerbations, and response to the addition of inhaled fluticasone furoate to vilanterol in patients with chronic obstructive pulmonary disease: a secondary analysis of data from two parallel randomised controlled trials. Lancet Respir Med. 2015;3(6):435–442. doi:10.1016/S2213-2600(15)00106-X
- Papi A, Vestbo J, Fabbri L, et al. Extrafine inhaled triple therapy versus dual bronchodilator therapy in chronic obstructive pulmonary disease (TRIBUTE): a double-blind, parallel group, randomised controlled trial. Lancet. 2018;391(10125):1076–1084. doi:10.1016/S0140-6736(18)30206-X
- Roche N, Chapman KR, Vogelmeier CF, et al. Blood eosinophils and response to maintenance chronic obstructive pulmonary disease treatment. Data from the FLAME trial. Am J Respir Crit Care Med. 2017;195(9):1189–1197. doi:10.1164/rccm.201701-0193OC
- Brightling CE, Bleecker ER, Panettieri RA, et al. Benralizumab for chronic obstructive pulmonary disease and sputum eosinophilia: a randomised, double-blind, placebo-controlled, phase 2a study. Lancet Respir Med. 2014;2(11):891–901. doi:10.1016/S2213-2600(14)70187-0
- Butler A, Walton GM, Sapey E. Neutrophilic inflammation in the pathogenesis of chronic obstructive pulmonary disease. COPD. 2019;15(4):392–404. doi:10.1080/15412555.2018.1476475
- Baines KJ, Simpson JL, Gibson PG. Innate immune responses are increased in chronic obstructive pulmonary disease. PLoS One. 2011;6(3):e18426. doi:10.1371/journal.pone.0018426
- Parr DG, White AJ, Bayley DL, Guest PJ, Stockley RA. Inflammation in sputum relates to progression of disease in subjects with COPD: a prospective descriptive study. Respir Res. 2006;7:136. doi:10.1186/1465-9921-7-136
- Aaron SD, Angel JB, Lunau M, et al. Granulocyte inflammatory markers and airway infection during acute exacerbation of chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2001;163(2):349–355. doi:10.1164/ajrccm.163.2.2003122
- Martinez FJ, Calverley PMA, Goehring U-M, Brose M, Fabbri LM, Rabe KF. Effect of roflumilast on exacerbations in patients with severe chronic obstructive pulmonary disease uncontrolled by combination therapy (REACT): a multicentre randomised controlled trial. Lancet. 2015;385(9971):857–866. doi:10.1016/S0140-6736(14)62410-7
- Lopez-Campos JL, Miravitlles M, de la Rosa Carrillo D, Cantón R, Soler-Cataluña JJ, Martinez-Garcia MA. Current challenges in chronic bronchial infection in patients with chronic obstructive pulmonary disease. J Clin Med. 2020;9(6):1639. doi:10.3390/jcm9061639
- Dima E, Kyriakoudi A, Kaponi M, et al. The lung microbiome dynamics between stability and exacerbation in chronic obstructive pulmonary disease (COPD): current perspectives. Respir Med. 2019;157:1–6. doi:10.1016/j.rmed.2019.08.012
- Cui L, Lucht L, Tipton L, et al. Topographic diversity of the respiratory tract mycobiome and alteration in HIV and lung disease. Am J Respir Crit Care Med. 2015;191(8):932–942. doi:10.1164/rccm.201409-1583OC
- Man WH, de Steenhuijsen Piters WAA, Bogaert D. The microbiota of the respiratory tract: gatekeeper to respiratory health. Nat Rev Microbiol. 2017;15(5):259–270. doi:10.1038/nrmicro.2017.14
- Su YC, Jalalvand F, Thegerström J, Riesbeck K. The interplay between immune response and bacterial infection in COPD: focus upon non-typeable Haemophilus influenzae. Front Immunol. 2018;9:2530. doi:10.3389/fimmu.2018.02530
- Sze MA, Dimitriu PA, Hayashi S, et al. The lung tissue microbiome in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2012;185(10):1073–1080. doi:10.1164/rccm.201111-2075OC
- Galiana A, Aguirre E, Rodriguez JC, et al. Sputum microbiota in moderate versus severe patients with COPD. Eur Respir J. 2014;43(6):1787–1790. doi:10.1183/09031936.00191513
- Pragman AA, Kim HB, Reilly CS, Wendt C, Isaacson RE. The lung microbiome in moderate and severe chronic obstructive pulmonary disease. PLoS One. 2012;7(10):e47305. doi:10.1371/journal.pone.0047305
- Sethi S, Murphy TF. Infection in the pathogenesis and course of chronic obstructive pulmonary disease. N Engl J Med. 2008;359(22):2355–2365. doi:10.1056/NEJMra0800353
- Mammen MJ, Sethi S. COPD and the microbiome. Respirology. 2016;21(4):590–599. doi:10.1111/resp.12732
- Garcha DS, Thurston SJ, Patel ARC, et al. Changes in prevalence and load of airway bacteria using quantitative PCR in stable and exacerbated COPD. Thorax. 2012;67(12):1075–1080. doi:10.1136/thoraxjnl-2012-201924
- Oliveira AS, Munhá J, Bugalho A, et al. Identification and assessment of COPD exacerbations. Pulmonology. 2017. doi:10.1016/j.rppnen.2017.10.006
- Yii ACA, Loh CH, Tiew PY, et al. A clinical prediction model for hospitalized COPD exacerbations based on “treatable traits”. Int J Chron Obstruct Pulmon Dis. 2019;14:719–728. doi:10.2147/COPD.S194922
- Bafadhel M, McKenna S, Agbetile J, et al. Aspergillus fumigatus during stable state and exacerbations of COPD. Eur Respir J. 2014;43(1):64–71. doi:10.1183/09031936.00162912
- Hammond EE, McDonald CS, Vestbo J, Denning DW. The global impact of Aspergillus infection on COPD. BMC Pulm Med. 2020;20(1):241. doi:10.1186/s12890-020-01259-8
- Linden D, Guo-Parke H, Coyle PV, et al. Respiratory viral infection: a potential “missing link” in the pathogenesis of COPD. Eur Respir Rev. 2019;28(151):180063. doi:10.1183/16000617.0063-2018
- Brode SK, Campitelli MA, Kwong JC, et al. The risk of mycobacterial infections associated with inhaled corticosteroid use. Eur Respir J. 2017;50(3):1700037. doi:10.1183/13993003.00037-2017
- Dubé BP, Guerder A, Morelot-Panzini C, Laveneziana P. The clinical relevance of the emphysema-hyperinflated phenotype in COPD. COPD Res Pract. 2015;2(1):1. doi:10.1186/s40749-015-0017-7
- Kitaguchi Y, Fujimoto K, Kubo K, Honda T. Characteristics of COPD phenotypes classified according to the findings of HRCT. Respir Med. 2006;100(10):1742–1752. doi:10.1016/j.rmed.2006.02.003
- Hackx M, Gyssels E, Severo Garcia T, et al. Chronic obstructive pulmonary disease: CT quantification of airway dimensions, numbers of airways to measure, and effect of bronchodilation. Radiology. 2015;277(3):853–862. doi:10.1148/radiol.2015140949
- Refaee T, Wu G, Ibrahim A, et al. The emerging role of radiomics in COPD and lung cancer. Respiration. 2020;99(2):99–107. doi:10.1159/000505429
- Grydeland TB, Dirksen A, Coxson HO, et al. Quantitative computed tomography: emphysema and airway wall thickness by sex, age and smoking. Eur Respir J. 2009;34(4):858–865. doi:10.1183/09031936.00167908
- de Jong PA, Müller NL, Paré PD, Coxson HO. Computed tomographic imaging of the airways: relationship to structure and function. Eur Respir J. 2005;26(1):140–152. doi:10.1183/09031936.05.00007105
- Madani A, Zanen J, de Maertelaer V, Gevenois PA. Pulmonary emphysema: objective quantification at multi-detector row CT–comparison with macroscopic and microscopic morphometry. Radiology. 2006;238(3):1036–1043. doi:10.1148/radiol.2382042196
- Gonçalves I, Guimarães MJ, van Zeller M, et al. Clinical and molecular markers in COPD. Pulmonology. 2018;24(4):250–259. doi:10.1016/j.pulmoe.2018.02.005
- Kim YW, Lee CH, Hwang HG, et al. Resting hyperinflation and emphysema on the clinical course of COPD. Sci Rep. 2019;9(1):3764. doi:10.1038/s41598-019-40411-1
- Casanova C, Cote C, de Torres JP, et al. Inspiratory-to-total lung capacity ratio predicts mortality in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2005;171(6):591–597. doi:10.1164/rccm.200407-867OC
- O’Donnell DE, Laveneziana P. Physiology and consequences of lung hyperinflation in COPD. Eur Respir Rev. 2006;15(100):61–67. doi:10.1183/09059180.00010002
- Cardoso J, Coelho R, Rocha C, Coelho C, Semedo L, Bugalho Almeida A. Prediction of severe exacerbations and mortality in COPD: the role of exacerbation history and inspiratory capacity/total lung capacity ratio. Int J Chron Obstruct Pulmon Dis. 2018;13:1105–1113. doi:10.2147/COPD.S155848
- D’Ascanio M, Viccaro F, Calabrò N, et al. Assessing static lung hyperinflation by whole-body plethysmography, helium dilution, and impulse oscillometry System (IOS) in patients with COPD. Int J Chron Obstruct Pulmon Dis. 2020;15:2583–2589. doi:10.2147/COPD.S264261
- Rossi A, Aisanov Z, Avdeev S, et al. Mechanisms, assessment and therapeutic implications of lung hyperinflation in COPD. Respir Med. 2015;109(7):785–802. doi:10.1016/j.rmed.2015.03.010
- Young RP, Hopkins RJ. Update on the potential role of statins in chronic obstructive pulmonary disease and its co-morbidities. Expert Rev Respir Med. 2013;7(5):533–544. doi:10.1586/17476348.2013.838018
- Gan WQ, Man SFP, Senthilselvan A, Sin DD. Association between chronic obstructive pulmonary disease and systemic inflammation: a systematic review and a meta-analysis. Thorax. 2004;59(7):574–580. doi:10.1136/thx.2003.019588
- Agustí A, Edwards LD, Rennard SI, et al. Persistent systemic inflammation is associated with poor clinical outcomes in COPD: a novel phenotype. PLoS One. 2012;7(5):e37483. doi:10.1371/journal.pone.0037483
- Thomsen M, Dahl M, Lange P, Vestbo J, Nordestgaard BG. Inflammatory biomarkers and comorbidities in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2012;186(10):982–988. doi:10.1164/rccm.201206-1113OC
- Li WF, Huang YQ, Huang C, Feng YQ. Statins reduce all-cause mortality in chronic obstructive pulmonary disease: an updated systematic review and meta-analysis of observational studies. Oncotarget. 2017;8(42):73000–73008. doi:10.18632/oncotarget.20304
- Lu Y, Chang R, Yao J, Xu X, Teng Y, Cheng N. Effectiveness of long-term using statins in COPD - A network meta-analysis. Respir Res. 2019;20(1):17. doi:10.1186/s12931-019-0984-3
- Hiles SA, Gibson PG, Agusti A, McDonald VM. Treatable traits that predict health status and treatment response in airway disease. J Allergy Clin Immunol Pract. 2020. doi:10.1016/j.jaip.2020.09.046
- Divo M, Cote C, de Torres JP, et al. Comorbidities and risk of mortality in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2012;186(2):155–161. doi:10.1164/rccm.201201-0034OC
- Curkendall SM, DeLuise C, Jones JK, et al. Cardiovascular disease in patients with chronic obstructive pulmonary disease, Saskatchewan Canada cardiovascular disease in COPD patients. Ann Epidemiol. 2006;16(1):63–70. doi:10.1016/j.annepidem.2005.04.008
- Trinkmann F, Saur J, Borggrefe M, Akin I. Cardiovascular comorbidities in chronic obstructive pulmonary disease (COPD)-current considerations for clinical practice. J Clin Med. 2019;8(1):69. doi:10.3390/jcm8010069
- Pascual-Guardia S, Badenes-Bonet D, Martin-Ontiyuelo C, et al. Hospital admissions and mortality in patients with COPD exacerbations and vertebral body compression fractures. Int J Chron Obstruct Pulmon Dis. 2017;12:1837–1845. doi:10.2147/COPD.S129213
- Chen W, Lin CW, Chen YY, Chen YJ, Liang CY, Lin MS. Prevalence, risk factors, and health-related quality of life of osteoporosis in patients with COPD at a community hospital in Taiwan. Int J Chron Obstruct Pulmon Dis. 2015;1493. doi:10.2147/COPD.S85432
- Donaldson GC, Seemungal TAR, Bhowmik A, Wedzicha JA. Relationship between exacerbation frequency and lung function decline in chronic obstructive pulmonary disease. Thorax. 2002;57(10):847–852. doi:10.1136/thorax.57.10.847
- Soler-Cataluña JJ, Martínez-García MA, Román Sánchez P, Salcedo E, Navarro M, Ochando R. Severe acute exacerbations and mortality in patients with chronic obstructive pulmonary disease. Thorax. 2005;60(11):925–931. doi:10.1136/thx.2005.040527
- Rothnie KJ, Müllerová H, Smeeth L, Quint JK. Natural history of chronic obstructive pulmonary disease exacerbations in a general practice-based population with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2018;198(4):464–471. doi:10.1164/rccm.201710-2029OC
- García-Sanz MT, Cánive-Gómez JC, Senín-Rial L, et al. One-year and long-term mortality in patients hospitalized for chronic obstructive pulmonary disease. J Thorac Dis. 2017;9(3):636–645. doi:10.21037/jtd.2017.03.34
- Jernberg T, Hasvold P, Henriksson M, Hjelm H, Thuresson M, Janzon M. Cardiovascular risk in post-myocardial infarction patients: nationwide real world data demonstrate the importance of a long-term perspective. Eur Heart J. 2015;36(19):1163–1170. doi:10.1093/eurheartj/ehu505
- Halpin DM, Miravitlles M, Metzdorf N, Celli B. Impact and prevention of severe exacerbations of COPD: a review of the evidence. Int J Chron Obstruct Pulmon Dis. 2017;20:2891–2908. doi:10.1186/s12931-019-0984-3
- Hurst JR, Vestbo J, Anzueto A, et al. Susceptibility to exacerbation in chronic obstructive pulmonary disease. N Engl J Med. 2010;363(12):1128–1138. doi:10.1056/NEJMoa0909883
- Donaldson GC, Law M, Kowlessar B, et al. Impact of prolonged exacerbation recovery in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2015;192(8):943–950. doi:10.1164/rccm.201412-2269OC
- David B, Bafadhel M, Koenderman L, De Soyza A. Eosinophilic inflammation in COPD: from an inflammatory marker to a treatable trait. Thorax. 2020. doi:10.1136/thoraxjnl-2020-215167
- MacDonald MI, Osadnik CR, Bulfin L, et al. Low and high blood eosinophil counts as biomarkers in hospitalized acute exacerbations of COPD. Chest. 2019;156(1):92–100. doi:10.1016/j.chest.2019.02.406
- MacDonald M, Beasley RW, Irving L, Bardin PG. A hypothesis to phenotype COPD exacerbations by aetiology. Respirology. 2011;16(2):264–268. doi:10.1111/j.1440-1843.2010.01908.x
- MacDonald M, Korman T, King P, Hamza K, Bardin P. Exacerbation phenotyping in chronic obstructive pulmonary disease. Respirology. 2013;18(8):1280–1281. doi:10.1111/resp.12197
- McDonald VM, Osadnik CR, Gibson PG. Treatable traits in acute exacerbations of chronic airway diseases. Chron Respir Dis. 2019;16:1479973119867954. doi:10.1177/1479973119867954
- Prins HJ, Duijkers R, van der Valk P, et al. CRP-guided antibiotic treatment in acute exacerbations of COPD in hospital admissions. Eur Respir J. 2019;53(5):1802014. doi:10.1183/13993003.02014-2018
- Bafadhel M, McKenna S, Terry S, et al. Blood eosinophils to direct corticosteroid treatment of exacerbations of chronic obstructive pulmonary disease: a randomized placebo-controlled trial. Am J Respir Crit Care Med. 2012;186(1):48–55. doi:10.1164/rccm.201108-1553OC
- Sivapalan P, Lapperre TS, Janner J, et al. Eosinophil-guided corticosteroid therapy in patients admitted to hospital with COPD exacerbation (CORTICO-COP): a multicentre, randomised, controlled, open-label, non-inferiority trial. Lancet Respir Med. 2019;7(8):699–709. doi:10.1016/S2213-2600(19)30176-6
- Roede BM, Bindels PJ, Brouwer HJ, Bresser P, de Borgie CA, Prins JM. Antibiotics and steroids for exacerbations of COPD in primary care: compliance with Dutch guidelines. Br J Gen Pract. 2006;56(530):662–665.
- Roede BM, Bresser P, Prins JM, Schellevis F, Verheij TJM, Bindels PJE. Reduced risk of next exacerbation and mortality associated with antibiotic use in COPD. Eur Respir J. 2009;33(2):282–288. doi:10.1183/09031936.00088108
- Aggarwal D, Mohapatra PR, Aggarwal P. Significance of sputum purulence to guide antibiotic therapy in exacerbations of COPD. Eur Respir J. 2013;41(1):248. doi:10.1183/09031936.00083112
- Butler CC, Gillespie D, White P, et al. C-reactive protein testing to guide antibiotic prescribing for COPD exacerbations. N Engl J Med. 2019;381(2):111–120. doi:10.1056/NEJMoa1803185
- Chen K, Pleasants KA, Pleasants RA, et al. Procalcitonin for antibiotic prescription in chronic obstructive pulmonary disease exacerbations: systematic review, meta-analysis, and clinical perspective. Pulm Ther. 2020;6(2):201–214. doi:10.1007/s41030-020-00123-8
- Seemungal T, Harper-Owen R, Bhowmik A, et al. Respiratory viruses, symptoms, and inflammatory markers in acute exacerbations and stable chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2001;164(9):1618–1623. doi:10.1164/ajrccm.164.9.2105011
- Papi A. Pathophysiology of exacerbations of chronic obstructive pulmonary disease. Proc Am Thorac Soc. 2006;3(3):245–251. doi:10.1513/pats.200512-125SF
- Kolsum U, Donaldson GC, Singh R, et al. Blood and sputum eosinophils in COPD; relationship with bacterial load. Respir Res. 2017;18(1):88. doi:10.1186/s12931-017-0570-5
- Bafadhel M, Davies L, Calverley PMA, Aaron SD, Brightling CE, Pavord ID. Blood eosinophil guided prednisolone therapy for exacerbations of COPD: a further analysis. Eur Respir J. 2014;44(3):789–791. doi:10.1183/09031936.00062614
- Aleva FE, Voets LWLM, Simons SO, de Mast Q, van der Ven AJAM, Heijdra YF. Prevalence and localization of pulmonary embolism in unexplained acute exacerbations of COPD. Chest. 2017;151(3):544–554. doi:10.1016/j.chest.2016.07.034
- Ra SW, Sin DD. Should we screen for pulmonary embolism in severe COPD exacerbations? Not just yet, primum non nocere. Chest. 2017;151(3):523–524. doi:10.1016/j.chest.2016.09.018
- Kunisaki KM, Dransfield MT, Anderson JA, et al. Exacerbations of chronic obstructive pulmonary disease and cardiac events. A post hoc cohort analysis from the SUMMIT randomized clinical trial. Am J Respir Crit Care Med. 2018;198(1):51–57. doi:10.1164/rccm.201711-2239OC
- Ni Y, Shi G, Yu Y, Hao J, Chen T, Song H. Clinical characteristics of patients with chronic obstructive pulmonary disease with comorbid bronchiectasis: a systemic review and meta-analysis. Int J Chron Obstruct Pulmon Dis. 2015;10:1465–1475. doi:10.2147/COPD.S83910
- Olalde I, Mallick S, Patterson N, et al. The genomic history of the Iberian Peninsula over the past 8000 years. Science (80-). 2019;363(6432):1230–1234. doi:10.1126/science.aav4040
- Miravitlles M, Guerrero T, Mayordomo C, Sánchez-Agudo L, Nicolau F, Segú JL. Factors associated with increased risk of exacerbation and hospital admission in a cohort of ambulatory COPD patients: a multiple logistic regression analysis. The EOLO Study Group. Respiration. 2000;67(5):495–501. doi:10.1159/000067462
- Kim V, Han MK, Vance GB, et al. The chronic bronchitic phenotype of COPD: an analysis of the COPDGene study. Chest. 2011;140(3):626–633. doi:10.1378/chest.10-2948
- Burgel PR, Nesme-Meyer P, Chanez P, et al. Cough and sputum production are associated with frequent exacerbations and hospitalizations in COPD subjects. Chest. 2009;135(4):975–982. doi:10.1378/chest.08-2062
- Marin JM, Soriano JB, Carrizo SJ, Boldova A, Celli BR. Outcomes in patients with chronic obstructive pulmonary disease and obstructive sleep apnea: the overlap syndrome. Am J Respir Crit Care Med. 2010;182(3):325–331. doi:10.1164/rccm.200912-1869OC
- Gunduz C, Basoglu OK, Tasbakan MS. Prevalence of overlap syndrome in chronic obstructive pulmonary disease patients without sleep apnea symptoms. Clin Respir J. 2018;12(1):105–112. doi:10.1111/crj.12493
- Shorofsky M, Bourbeau J, Kimoff J, et al. Impaired sleep quality in COPD is associated with exacerbations: the CanCOLD cohort study. Chest. 2019;156(5):852–863. doi:10.1016/j.chest.2019.04.132
- Iyer AS, Bhatt SP, Garner JJ, et al. Depression is associated with readmission for acute exacerbation of chronic obstructive pulmonary disease. Ann Am Thorac Soc. 2016;13(2):197–203. doi:10.1513/AnnalsATS.201507-439OC
- Hoong JM, Ferguson M, Hukins C, Collins PF. Economic and operational burden associated with malnutrition in chronic obstructive pulmonary disease. Clin Nutr. 2017;36(4):1105–1109. doi:10.1016/j.clnu.2016.07.008
- Pitta F, Troosters T, Probst VS, Spruit MA, Decramer M, Gosselink R. Physical activity and hospitalization for exacerbation of COPD. Chest. 2006;129(3):536–544. doi:10.1378/chest.129.3.536
- Garcia-Rio F, Rojo B, Casitas R, et al. Prognostic value of the objective measurement of daily physical activity in patients with COPD. Chest. 2012;142(2):338–346. doi:10.1378/chest.11-2014
- Garcia-Aymerich J, Lange P, Benet M, Schnohr P, Antó JM. Regular physical activity reduces hospital admission and mortality in chronic obstructive pulmonary disease: a population based cohort study. Thorax. 2006;61(9):772–778. doi:10.1136/thx.2006.060145
- Melani AS, Bonavia M, Cilenti V, et al. Inhaler mishandling remains common in real life and is associated with reduced disease control. Respir Med. 2011;105(6):930–938. doi:10.1016/j.rmed.2011.01.005
- Maricoto T, Monteiro L, Gama JMR, Correia-de-sousa J, Taborda-Barata L. Inhaler technique education and exacerbation risk in older adults with asthma or chronic obstructive pulmonary disease: a meta-analysis. J Am Geriatr Soc. 2019;67(1):57–66. doi:10.1111/jgs.15602
- Viniol C, Vogelmeier CF. Exacerbations of COPD. Eur Respir Rev. 2018;27:147. doi:10.1183/16000617.0103-2017
- Ozyilmaz E, Kokturk N, Teksut G, Tatlicioglu T. Unsuspected risk factors of frequent exacerbations requiring hospital admission in chronic obstructive pulmonary disease. Int J Clin Pract. 2013;67(7):691–697. doi:10.1111/ijcp.12150
- Agustí A, Calverley PM, Decramer M, Stockley RA, Wedzicha JA. Prevention of exacerbations in chronic obstructive pulmonary disease: knowns and unknowns. Chronic Obstr Pulm Dis. 2014;1(2):166–184. doi:10.15326/jcopdf.1.2.2014.0134