
Abstract
Purpose
The purpose of our study was to investigate the relationship between serum sodium levels and 1-year and 3-year mortality in critically ill patients with comorbid chronic obstructive pulmonary disease using real-world data.
Methods
The data of this study were collected from the Medical Information Mart for Intensive Care-IV (MIMIC-IV) database. First of all, we used the Kaplan–Meier curves and multivariable Cox regression analyses to measure the relationship between serum sodium levels and 1-year and 3-year mortality for critically ill patients with comorbid COPD. Next, a restricted cubic spline was used to analyze non-parametrically the relationship between mortality and serum sodium as a continuous variable. In addition, we also analyzed the mortality of different subgroups.
Results
A total of 5540 eligible subjects were extracted. Compared to normal serum sodium levels, adjusted multivariable Cox regression analysis confirmed that hyponatremia and hypernatremia were still significantly associated with 1-year mortality (HR = 1.551, 95% CI = 1.333~1.805, P<0.001; HR = 1.683, 95% CI = 1.317~2.151, P<0.001, respectively) and 3-year mortality (HR = 1.507, 95% CI = 1.302~1.744, P<0.001; HR = 1.612, 95% CI = 1.269~2.048, P<0.001, respectively). In patients with or without adjustment variables, there was an obvious U-shaped non-linear relationship between serum sodium levels and 1-year and 3-year mortality with a reference level of 139 mmol/L, which indicated that patients in both hyponatremia and hypernatremia had higher mortality than normal serum sodium levels.
Conclusion
This study showed that both hyponatremia and hypernatremia were related to increased 1-year and 3-year mortality in critically ill patients with comorbid COPD, which provides a new reference for the control strategy of correcting serum sodium levels.
Introduction
Chronic obstructive pulmonary disease (COPD) is the third leading cause of death globally, with a global prevalence of 10.1% in 2017,Citation1 which is characterized by persistent respiratory symptoms and incompletely reversible airflow limitation caused by exposure to noxious particles or gases.Citation2 With the increasing prevalence of chronic obstructive pulmonary disease (COPD) worldwideCitation3,Citation4 and the increasingly aging population caused by the improvement in the medical and social environments,Citation5 it is not surprising that COPD has become a rather common comorbid disease among patients admitted to the intensive care unit (ICU). According to a prospective observational study that analyzed 194,453 hospitalized patients from Austria, COPD was present in 8.6% of ICU patients and they had higher risk-adjusted mortality compared with those without COPD.Citation6 Therefore, it is necessary to find useful indicators to predict the clinical outcomes of critically ill patients with comorbid COPD.
Serum sodium concentration is a common index in ICU and disturbances in sodium concentration are associated with increased mortality in critically ill patients.Citation7 Dysnatremias (hyponatremia and hypernatremia) can adversely affect various physiologic functions and organ systems.Citation8 Several previous studies have shown that hyponatremia and hypernatremia are independent risk factors of mortality in patients with community-acquired pneumonia,Citation9 coronavirus disease (COVID-19), pneumonia,Citation10 kidney diseaseCitation11 and acute subarachnoid hemorrhage.Citation12 Among them, there may be several possible explanations for the effect of serum sodium on lung diseases. Some studies have shown that the change of osmotic pressure caused by dysnatremias may affect pulmonary vascular permeability by affecting the receptor potential 4 channel,Citation13–Citation15 which further aggravates the COPD and raises mortality. Hypertonic environment of hypernatremia may promote systemic inflammation primarily via hyperosmolar cell stress,Citation16 which may result in damage to the lungs and reduced lung function.Citation17 Previous studies mostly focused on the relationship between hyponatremia and acute exacerbation of chronic obstructive pulmonary disease (AECOPD), while few previous studies have evaluated the association between serum sodium and critically ill patients with comorbid COPD.Citation18
Therefore, we intend to investigate the possible association between serum sodium levels and the risk of long-term mortality in critically ill patients with comorbid COPD in this study.
Materials and Methods
Data Source
In this study, all the correlative data were extracted from the Medical Information Mart for Intensive Care (MIMIC)-IV database (version: 1.0).Citation19 It is an open and freely accessible database, an update to MIMIC-III, containing information on more than 50,000 patients hospitalized in the ICUs of Beth Israel Deaconess Medical Center in Boston, MA, from 2008 to 2019.Citation20 One author, Liming Fan, has finished the Collaborative Institutional Training Initiative examination (certification number: 39010384) and accessed the database for data extraction. This study was approved by ethics committee of the First Affiliated Hospital of Zhejiang Chinese Medical University [2021-KL-197-01].
Study Population
We included all ICU consecutive adult patients (aged >18 years) with the primary diagnosis of COPD using ICD-9 codes (code = 49120, 49121, 49122 and 496) and ICD-10 codes (code = J44, J44, J440, J441 and J44) in the MIMIC-IV database. Patients were excluded according to the following criteria: (1) who had multiple admissions other than the first ICU admission; (2) length of ICU stay <24 h; (3) incomplete or unobtainable data of serum sodium measured between 24 hours before ICU admission and 24 hours after ICU admission; (4) more than 20% of individual data missing.
Data Extraction
PostgreSQL tool (version 9.6) was used to collect data from MIMIC-IV. Demographic information included age, sex, race, and insurance status. History of disease included asthma, pneumonia (such as bacterial pneumonia, viral pneumonia and ventilator-associated pneumonia), hypertension, diabetes, myocardial infarction, congestive heart failure, cerebrovascular disease, liver disease, renal disease, and malignant cancer. Vital signs on admission included temperature, heart rate (HR), respiratory rate (RR), mean arterial pressure (MAP), and pulse oximetry-derived oxygen saturation (SpO2). Laboratory-based data included sodium, bicarbonate, glucose, potassium, white blood cell count (WBC), hemoglobin (HGB) and platelet. If the patient underwent more than one laboratory examination during hospitalization, only the initial examination results were included in the analysis. In addition, we also collected treatment information data, including glucocorticoid treatment, bronchodilator treatment, antibiotic treatment, diuretic treatment, vasopressin treatment and mechanical ventilation. Charlson comorbidity index (CCI)Citation21 (Table S1), sequential organ failure assessment (SOFA)Citation22 (Table S2), Oxford acute severity of illness score (OASIS)Citation23 (Table S3) and acute physiology score III (APSIII)Citation24 (Table S4) were also extracted. In this study, the primary outcome was defined as 1-year and 3-year mortality after admission to the ICU.
Statistics
Hyponatremia, defined as a serum sodium concentration <135mmol/L, was categorized as mild-hyponatremia (130≤Na<135mmol/L), moderate-hyponatremia (125≤Na<130mmol/L) and profound-hyponatremia (<125mmol/L).Citation25 Hypernatremia was defined as the serum sodium concentration >145 mmol/L.Citation26 Normal serum sodium (135≤Na≤145mmol/L) was used as the reference category. Normally distributed continuous variables are presented as the mean ± standard deviation, and the comparison between groups was performed by the t-test or one-way analysis of variance. Non-normally distributed data are presented as the median and interquartile difference (IQR), and the Kruskal–Wallis test was used for comparison between groups. Categorical variables were presented as numbers (percentages) and tested by the chi-square test or Fisher’s exact test. The Kaplan–Meier curve was performed to determine the association between serum sodium and 1-year and 3-year mortality. The log rank test was used to compare the differences between the three groups. Variables, p<0.05 in the univariate analysis, were further incorporated into multivariate Cox proportional hazard models. Potential multicollinearity was tested by the variance inflation factor (VIF), with VIF ≥5 indicating the existence of multicollinearity. Our crude model included only the serum sodium data. In Model I, covariates were adjusted for age, gender, race and insurance status. Model II adjusted for model I plus SOFA score, glucocorticoid use, vasopressin use, invasive mechanical ventilation use, bacterial pneumonia, ventilator associated pneumonia, hypertension, myocardial infarction, congestive heart failure, renal disease, liver disease and malignant cancer. According to the above three models, the potential non-linear relationships between serum sodium (modeled as continuous variables) and the risk of mortality were evaluated with Cox regression models by restricted cubic spline with 5 knots, using a reference level of 139 mmol/L. Adjusted for the covariates of model 3, we used the multivariable Cox proportional hazards models for subgroup analysis to investigate the association between serum sodium and 1-year and 3-year mortality as it differed across various subgroups classified by age, sex, COPD types, asthma, bacterial pneumonia, ventilator-associated pneumonia, hypertension, diabetes, myocardial infarction, congestive heart failure, cerebrovascular disease, liver disease, renal disease and malignant cancer.
In this study, all tests were two-sided, and p<0.05 was considered statistically significant. Stata/SE Version 15.0 (Stata Corp, College Station, TX) and R software (R Foundation for Statistical Computing, version 4.1.0) were used for statistical analysis.
Results
Subject Characteristics
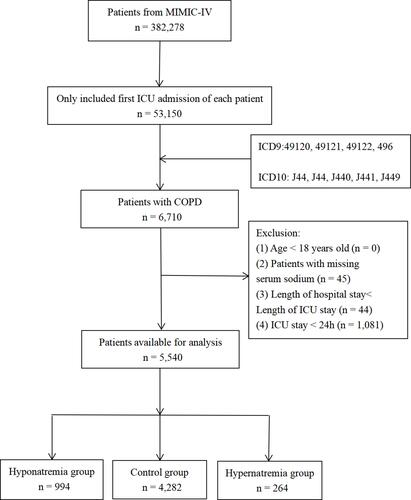
In this study were enrolled 5540 eligible subjects (). The control group, hyponatremia group, and hypernatremia group comprised 4282, 994 and 264 ICU patients, respectively. The median age was 72.31 (64.29–80.63), while 53.86% (2984/5540) subjects were male, most of whom were white. Compared with the control group, patients with hyponatremia were more likely to suffer liver disease and malignant cancer. They had lower levels of bicarbonate and higher levels of potassium and glucose, and were more likely to use vasopressin. Compared with the control group, patients with hypernatremia were more likely to receive antibiotics and invasive mechanical ventilation, and to report a history of bacterial pneumonia, congestive heart failure, renal disease and cerebrovascular disease. And they had the lower levels of SpO2 and hemoglobin, as well as the higher levels of heart rate, respiratory rate, mean arterial pressure, leukocyte count, Charlson Comorbidity Index, SOFA score, APSIII score, OASIS score, length of stay in ICU, length of stay in hospital, and 1-year and 3-year mortality ().
Table 1 Baseline and Clinical Characteristics of the Study Population
Figure 1 Flow chart of cohort selection.
Association Between HR Fluctuation and Mortality
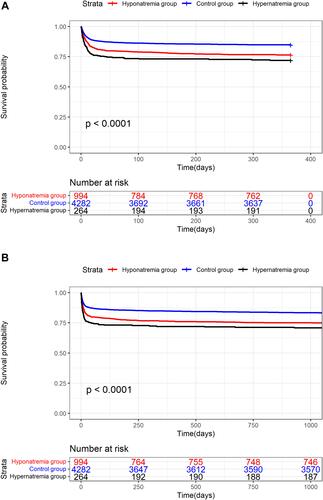
Among the 5540 patients included, 17.31% (959/5540) died during the 1-year follow-up period, and 18.86% (1045/5540) died during the 3-year follow-up period. The Kaplan–Meier curves consistently showed that hypernatremia group was significantly correlated with the highest risk of 1-year and 3-year mortality, followed by the hyponatremia and control groups (log-rank P<0.001) (). Compared with the control group, hyponatremia was significantly associated with the risk of 1-year and 3-year mortality (P<0.0001 by the log rank test). Likewise, hypernatremia was also significantly associated with the risk of 1-year and 3-year mortality compared with control group (P<0.0001 by log rank test).
Figure 2 Kaplan–Meier survival curves showing the association between serum sodium and all-cause mortality: (A) 1-year mortality; (B) 3-year mortality. Participants were divided into 3 groups based on serum sodium levels: the red line represents hyponatremia group (<135mmol/L), the blue line represents control group (135–145mmol/L), the black line represents hypernatremia group (>145mmol/L).
Cox regression models were used to determine the correlation between serum sodium and outcomes of critically ill patients with comorbid COPD (). The variables of temperature, heart rate, respiratory rate, mean arterial pressure, SpO2, Charlson Comorbidity Index, APSIII score, OASIS score, leukocyte count, hemoglobin, platelet, potassium, glucose, bicarbonate and antibiotic treatment were excluded from multivariate Cox regression models because of VIF >5. The remaining variables were selected for the multivariate analysis, including age, gender, race, insurance status, SOFA score, glucocorticoid use, vasopressin use, invasive mechanical ventilation use, bacterial pneumonia, ventilator-associated pneumonia, hypertension, myocardial infarction, congestive heart failure, liver disease, renal disease, and malignant cancer, which were significantly related to 1-year and 3-yearsmortality (Table S5).
Table 2 Association of Serum Sodium with 1-Year Mortality and 3-Year Mortality
In the unadjusted Cox model, hyponatremia and hypernatremia groups were associated with an increased risk of 1-year mortality (HR = 1.620, 95% CI = 1.395~1.881, P<0.01; HR = 2.028, 95% CI = 1.594~2.579, P<0.001, respectively) and 3-year mortality (HR = 1.568, 95% CI = 1.358~1.812, P<0.001; HR = 1.921, 95% CI = 1.518~2.430, P<0.001, respectively) compared to control group. In model I, hyponatremia and hypernatremia were identified as independent predictors of 1-year mortality (HR = 1.696, 95% CI = 1.460~1.970, P<0.001; HR = 1.800, 95% CI = 1.411~2.296, P<0.001, respectively) and 3-year mortality (HR = 1.643, 95% CI = 1.423~1.898, P<0.001; HR = 1.717, 95% CI = 1.353~2.178, P<0.001, respectively) after adjusting for age, gender, race and insurance status. In model II, after adjustment for confounders including age, gender, race and insurance status, SOFA score, glucocorticoid use, vasopressin use, invasive mechanical ventilation use, bacterial pneumonia, ventilator-associated pneumonia, hypertension, myocardial infarction, congestive heart failure, renal disease, liver disease, malignant cancer, hyponatremia and hypernatremia were still significantly related to 1-year mortality (HR = 1.551, 95% CI = 1.333~1.805, P<0.001; HR = 1.683, 95% CI = 1.317~2.151, P<0.001, respectively) and 3-year mortality (HR = 1.507, 95% CI = 1.302~1.744, P<0.001; HR = 1.612, 95% CI = 1.269~2.048, P<0.001, respectively).
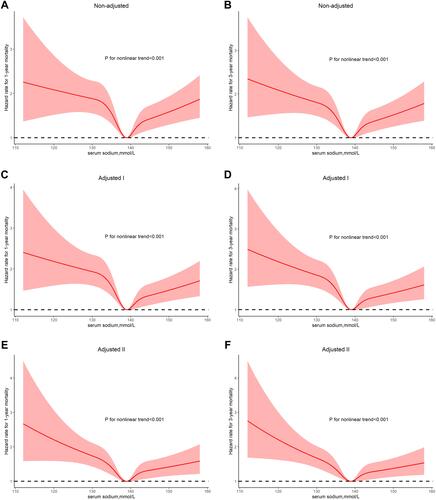
In restricted cubic splines, we observed a typical U-type curve, representing an obvious non-linear relationship between serum sodium levels and 1-year and 3-year mortality, with a serum sodium level of 139 mmol/L representing the lowest risk (all Ps for non-linear trend were <0.001; ). In patients with or without adjusted variables, the relationship between serum sodium and outcome was similar, indicating that patients in both the hyponatremia and hypernatremia groups had higher 1-year and 3-year mortality than the bottom of the curve, especially in the hyponatremia group.
Figure 3 Association between serum sodium and clinical outcomes for patients with COPD in different multivariable models. (A, C and E) association between serum sodium and 1-year mortality for patients with COPD. (B, D and F) association between serum sodium and 3-year mortality for patients with COPD. Adjusted I for age, gender, race and insurance status; Adjusted II for age, gender, race and insurance status, SOFA score, glucocorticoid use, vasopressin use, invasive mechanical ventilation use, bacterial pneumonia, ventilator-associated pneumonia, hypertension, myocardial infarction, congestive heart failure, renal disease, liver disease and malignant cancer.
Sensitivity and Subgroup Analyses
A series of subgroup analyses were conducted to verify the robustness of our results. Subgroup analyses were performed according to age, sex, COPD type, asthma, bacterial pneumonia, ventilator-associated pneumonia, hypertension, diabetes, myocardial infarction, congestive heart failure, cerebrovascular disease, liver disease, renal disease, and malignant cancer for 1-year and 3-year mortality. Observation results showed that hyponatremia and hypernatremia were also related to deteriorative mortality in different strata ( and S6). Significant interaction was observed in age (P<0.05).
Table 3 Subgroup Analysis for the Effect of Serum Sodium on 3-Year Mortality in COPD Patients
After excluding hypernatremia, we further analyzed the effect of hyponatremia on 1-year and 3-year mortality. Figure S1A and B shows the Kaplan–Meier curve for hyponatremia and normal serum sodium. The survival rate of the hyponatremia group was lower than that of the control group. Figure S1C and D shows the Kaplan–Meier curves for different degrees of hyponatremia. These show a clear difference in survival rate according to different levels of serum sodium. Even in hyponatremia patients, the decrease of serum sodium level was closely related to the decrease in survival rate. Similar trends were also observed in the multivariate Cox regression analyses (Table S7). In different models, as the degree of hyponatremia worsens, lower serum sodium levels are related with an increased risk of 1-year and 3-year mortality (all Ps for trend: <0.01).
Discussion
To our knowledge, this is the first study that evaluated the long-term effect of serum sodium on critically ill patients with comorbid COPD survival. In this retrospective cohort study, patients were divided into control group, hyponatremia group and hypernatremia group according to different serum sodium levels within 24 hours after ICU admission. According to multivariable Cox regression analysis, we found that both 1-year and the 3-year mortality in hyponatremia group and hypernatremia group were significantly increased compared to the control group. The Kaplan–Meier curves also reflect similar results. Furthermore, the association between serum sodium levels and 1-year and 3-year mortality in critically ill patients with comorbid COPD was observed in restricted cubic splines, indicating that the lowest risk of serum sodium level was 139 mmol/L. After excluding hypernatremia, we further analyzed the relationship between hyponatremia and 1-year and 3-year mortality risk, and the results showed that the risk of mortality increased with the aggravation of hyponatremia.
A large number of clinical studies have shown that the serum sodium disorder is a common electrolyte disorder both on admission and during stay amongst patients in ICU, which is also related to increased mortality.Citation8,Citation27 At present, the research on serum sodium and COPD mostly focuses on the effect of hyponatremia on AECOPD. In a prospective observational study that analyzed 602 hospitalized patients, García-Sanz et alCitation28 showed that the poor progress factors independently associated with AECOPD were hyponatremia, pneumonia, and not being home oxygen users. The results of Chalela et alCitation29 showed that hyponatremia (especially severe hyponatremia) is a predictor of adverse clinical course during COPD exacerbations. In the general hospital population, the incidence of hypernatremia is about approximately 1%. The incidence rate of ICU populations is 10–26%.Citation30 In the majority of cases, hypernatremia is hospital acquired.Citation31 However, there are few data on the relationship between hypernatremia and COPD. Our cohort study observed a typical U-shaped correlation between serum sodium levels and mortality in critically ill patients with comorbid COPD. Our findings were consistent with the results of studies showing that both hyponatremia and hypernatremia were significantly associated with poor prognosis and greater risk of mortality, including community-acquired pneumonia,Citation32 coronavirus disease 2019 (COVID-19),Citation33,Citation34 cirrhosis,Citation35 chronic kidney disease (CKD)Citation36 and severe burn injury.Citation37 In the subgroup analysis of our study, we found that hypernatremia is a more important predictor of poor prognosis in critically ill patients with comorbid COPD among older people compared with hyponatremia. Owing to a higher percentage of patients with hyponatremia in ICU,Citation8 we further analyzed the impact of hyponatremia on 1-year and 3-year mortality after excluding patients with hypernatremia. We observed that the risk of mortality increased with the severity of hyponatremia.
Although the mechanism of elevated mortality caused by serum sodium is unclear, there are several possible explanations for this phenomenon. Hyponatremia may be caused by chronic organ dysfunctions (such as heart failure and liver dysfunction), or by diuretic use, syndrome of inappropriate antidiuretic hormone (ADH) secretion, adrenal insufficiency and cerebral or renal salt wasting syndromes.Citation38 In ICU, para-pneumonic hyponatremia is caused by a syndrome of inappropriate anti-diuresis (SIAD), where hypoxia and inflammatory cytokines, such as monocyte and macrophage-derived IL-6, induce the release of a non-osmotic vasopressin.Citation39 Hyponatremia, which leads to decreased serum osmolality, can up- or down-regulate the transient receptor potential 4 ion channel, playing a key role in pulmonary vascular mechanotransduction.Citation15 Specifically, hypotonicity can stimulate these channels,Citation40–Citation42 resulting in increased endothelial calcium influx and pulmonary vascular permeability.Citation15 Therefore, hyponatremia can lead to pulmonary edemaCitation43,Citation44 and pleural effusion,Citation28 which further aggravates COPD. Hypernatremia in ICU is an iatrogenic problem due to excessive use of hypertonic solution and inadequate water substitution.Citation8 In a large retrospective double center study, Oude Lansink-Hartgring et alCitation31 observed that the incidence rate of dysnatremia has changed from hyponatremia to hypernatremia in the past twenty years. This shift may be related to the increased use of sodium-containing infusions, hydrocortisone and diuretics. Bihari et al,Citation45 however, reported that high concentration of serum sodium has no significant correlation with high mortality of ICU patients hospitalized for respiratory diseases. However, Krüger et alCitation46 found a U-shaped association between serum sodium level and mortality in these patients with community-acquired pneumonia. This is in accordance with our finding of a U-shaped association between serum sodium level and mortality of ICU patients hospitalized for COPD, ie an increased risk of mortality in both patients with hyponatremia and hypernatremia. Stewart et alCitation47 reported that hypoxemic patients with COPD may contribute significantly to sodium retention and edema, the reason of which may be a reduction in glomerular filtration rate and small elevations of aldosterone and vasopressin levels. Hypertonic environment of hypernatremia was associated with increased extravascular lung water,Citation48 which was closely related to the exacerbation of COPD. In addition, hypernatraemia, which to a certain degree reflects the effect of osmolarity, may promote systemic inflammation primarily via hyperosmolar cell stress,Citation16 which has the potential to result in damage to the lungs and reduced lung function.Citation17 Meanwhile, hyperosmolarity had a negative impact on ventilation, which may be due to the reduced response of ventilator to metabolic acidosis in hyperosmolar conditions, which was strongly associated with increased mortality.Citation49
In critically ill patients, as an independent risk factor for morbidity and mortality, the presence of COPD is increasing.Citation6 Individualized and timely risk assessment for each critically ill patient can more accurately determine treatment strategies and medical resource allocation.Citation50 Previous studies have discussed the prognostic value of several relatively convenient predictors, such as eosinophil concentrations,Citation51 red blood cell distribution width,Citation52 platelet-lymphocyte ratio,Citation53 neutrophil-lymphocyte ratio.Citation54 The serum sodium concentration can quickly assess the risk of critically ill patients with comorbid COPD. Our results provide an optimal point of 139 mmol/L for serum sodium, which may provide a reference for correcting sodium concentration to reduce mortality in critically ill patients with comorbid COPD. Thus, serum sodium may be a feasible option to evaluate the prognosis of critically ill patients with comorbid COPD.
To be honest, there are some limitations in our research. Firstly, it is impossible to adjust for all confounding factors in a retrospective cohort study. After adjusting for known confounding factors as much as possible, there are still some unmeasured variables affecting our results. Because MIMIC-IV does not record all variables we lack some indicators, such as pulmonary function, which may affect our results. In addition, we did not include detailed information on some important clinical or laboratory variables (such as neutrophil count, eosinophil count, PaO2, PaCO2 and PH) because of more than 20% missing values. Therefore, we still need some prospective studies to verify these results. Secondly, we only measured the serum sodium levels of patients admitted to ICU. We did not investigate the change trend of serum sodium, which may provide more information. Thirdly, this is a single-center study involving other populations and regions, the results of which should be interpreted with caution.
Conclusion
In summary, this retrospective cohort study showed a U-shaped relationship between serum sodium levels and 1-year and 3-year mortality in critically ill patients with comorbid COPD, with the lowest risk related to serum sodium of 139 mmol/L. Both hyponatremia and hypernatremia increase the risk of all-cause mortality, and as the degree of hyponatremia worsens, the mortality rate gradually increases. Serum sodium levels may be an available and reliable predictor of the risk of mortality in critically ill patients with comorbid COPD, which should be considered and further verified in future studies of serum sodium control strategies.
Ethics Approval and Consent to Participate
The MIMIC-IV database has received ethical approval from the institutional review boards (IRBs) at Beth Israel Deaconess Medical Center and Massachusetts Institute of Technology. Because the database does not contain protected health information, a waiver of the requirement for informed consent was included in the IRB approval.
Disclosure
The authors report no conflicts of interest in this work.
Additional information
Funding
References
- Celli BR, Wedzicha JA. Update on clinical aspects of chronic obstructive pulmonary disease. N Engl J Med. 2019;381 (13):1257–1266. doi:10.1056/NEJMra1900500
- Vogelmeier CF, Criner GJ, Martinez FJ, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 report. Gold executive summary. Am J Respir Crit Care Med. 2017;195 (5):557–582. doi:10.1164/rccm.201701-0218PP
- Soriano JB, Abajobir AA, Abate KH, GBD 2015 Chronic Respiratory Disease Collaborators. Global, regional, and national deaths, prevalence, disability-adjusted life years, and years lived with disability for chronic obstructive pulmonary disease and asthma, 1990–2015: a systematic analysis for the Global Burden Of Disease Study 2015. Lancet Respir Med. 2017;5 (9):691–706.
- Salvi S, Kumar GA, Dhaliwal RS, India State-Level Disease Burden Initiative CRD Collaborators. The burden of chronic respiratory diseases and their heterogeneity across the states of India: the Global Burden of Disease Study 1990–2016. Lancet Glob Health. 2018;6 (12):e1363–e1374.
- The Lancet Public Health. Ageing: a 21st century public health challenge? Lancet Public Health. 2017;2 (7):e297.
- Funk GC, Bauer P, Burghuber OC, et al. Prevalence and prognosis of COPD in critically ill patients between 1998 and 2008. Eur Respir J. 2013;41 (4):792–799. doi:10.1183/09031936.00226411
- Overgaard-Steensen C, Ring T. Clinical review: practical approach to hyponatraemia and hypernatraemia in critically ill patients. Crit Care. 2013;17 (1):206. doi:10.1186/cc11805
- Funk GC, Lindner G, Druml W, et al. Incidence and prognosis of dysnatremias present on ICU admission. Intensive Care Med. 2010;36 (2):304–311. doi:10.1007/s00134-009-1692-0
- Tokgöz Akyil F, Akyil M, Çoban Ağca M, et al. Hyponatremia prolongs hospital stay and hypernatremia better predicts mortality than hyponatremia in hospitalized patients with community-acquired pneumonia. Tuberk Toraks. 2019;67 (4):239–247. doi:10.5578/tt.68779
- Ruiz-Sánchez JG, Núñez-Gil IJ, Cuesta M, et al. Prognostic impact of hyponatremia and hypernatremia in COVID-19 pneumonia. A HOPE-COVID-19 (health outcome predictive evaluation for COVID-19) registry analysis. Front Endocrinol. 2020;11:599255. doi:10.3389/fendo.2020.599255
- Combs S, Berl T. Dysnatremias in patients with kidney disease. Am J Kidney Dis. 2014;63 (2):294–303. doi:10.1053/j.ajkd.2013.09.017
- Spatenkova V, Bradac O, de Lacy P, et al. Dysnatremia as a poor prognostic indicator in patients with acute subarachnoid hemorrhage. J Neurosurg Sci. 2017;61 (4):371–379. doi:10.23736/S0390-5616.16.03411-1
- Garcia-Elias A, Lorenzo IM, Vicente R, et al. IP3 receptor binds to and sensitizes TRPV4 channel to osmotic stimuli via a calmodulin-binding site. J Biol Chem. 2008;283 (46):31284–31288. doi:10.1074/jbc.C800184200
- Mizuno A, Matsumoto N, Imai M, et al. Impaired osmotic sensation in mice lacking TRPV4. Am J Physiol Cell Physiol. 2003;285 (1):C96–C101. doi:10.1152/ajpcell.00559.2002
- Yin J, Kuebler WM. Mechanotransduction by TRP channels: general concepts and specific role in the vasculature. Cell Biochem Biophys. 2010;56 (1):1–18. doi:10.1007/s12013-009-9067-2
- Rugg C, Ströhle M, Treml B, et al. ICU-acquired hypernatremia is associated with persistent inflammation, immunosuppression and catabolism syndrome. J Clin Med. 2020;9 (9):3017. doi:10.3390/jcm9093017
- Pogson ZE, McKeever TM, Fogarty A. The association between serum osmolality and lung function among adults. Eur Respir J. 2008;32 (1):98–104. doi:10.1183/09031936.00144207
- Tokgöz Akyıl F, Tural Önür S, Abalı H, et al. Hyponatremia is an independent predictor of emergency department revisits in acute exacerbation of COPD. Clin Respir J. 2021;15 (10):1063–1072. doi:10.1111/crj.13409
- Goldberger AL, Amaral LA, Glass L, et al. PhysioBank, physiotoolkit, and physioNet: components of a new research resource for complex physiologic signals. Circulation. 2000;101 (23):E215–E220. doi:10.1161/01.cir.101.23.e215
- Li L, Zou G, Liu J. Preoperative glucose-to-lymphocyte ratio is an independent predictor for acute kidney injury after cardiac surgery in patients in intensive care unit. Int J Gen Med. 2021;14:6529–6537. doi:10.2147/IJGM.S335896
- Demircan NC, Alan Ö, Başoğlu Tüylü T, et al. Impact of the Charlson comorbidity index on dose-limiting toxicity and survival in locally advanced and metastatic renal cell carcinoma patients treated with first-line sunitinib or pazopanib. J Oncol Pharm Pract. 2020;26 (5):1147–1155. doi:10.1177/1078155219890032
- Moreno R, Vincent JL, Matos R, et al. The use of maximum SOFA score to quantify organ dysfunction/failure in intensive care. Results of a prospective, multicentre study. working group on sepsis related problems of the ESICM. Intensive Care Med. 1999;25 (7):686–696. doi:10.1007/s001340050931
- Johnson AE, Kramer AA, Clifford GD. A new severity of illness scale using a subset of acute physiology and chronic health evaluation data elements shows comparable predictive accuracy. Crit Care Med. 2013;41 (7):1711–1718. doi:10.1097/CCM.0b013e31828a24fe
- Knaus WA, Wagner DP, Draper EA, et al. The APACHE III prognostic system. Risk prediction of hospital mortality for critically ill hospitalized adults. Chest. 1991;100 (6):1619–1636. doi:10.1378/chest.100.6.1619
- Spasovski G, Vanholder R, Allolio B, et al. Clinical practice guideline on diagnosis and treatment of hyponatraemia. Intensive Care Med. 2014;40 (3):320–331. doi:10.1007/s00134-014-3210-2
- Qian Q. Hypernatremia. Clin J Am Soc Nephrol. 2019;14 (3):432–434. doi:10.2215/CJN.12141018
- Chi C, Patel S, Cheung NW. Admission sodium levels and hospital outcomes. Intern Med J. 2021;51 (1):93–98. doi:10.1111/imj.14777
- García-Sanz MT, Martínez-Gestoso S, Calvo-álvarez U, et al. Impact of hyponatremia on COPD exacerbation prognosis. J Clin Med. 2020;9 (2):503. doi:10.3390/jcm9020503
- Chalela R, González-García JG, Chillarón JJ, et al. Impact of hyponatremia on mortality and morbidity in patients with COPD exacerbations. Respir Med. 2016;117:237–242. doi:10.1016/j.rmed.2016.05.003
- Pokaharel M, Block CA. Dysnatremia in the ICU. Curr Opin Crit Care. 2011;17 (6):581–593. doi:10.1097/MCC.0b013e32834cd388
- Oude Lansink-Hartgring A, Hessels L, Weigel J, et al. Long-term changes in dysnatremia incidence in the ICU: a shift from hyponatremia to hypernatremia. Ann Intensive Care. 2016;6 (1):22. doi:10.1186/s13613-016-0124-x
- Ravioli S, Gygli R, Funk GC, et al. Prevalence and impact on outcome of sodium and potassium disorders in patients with community-acquired pneumonia: a retrospective analysis. Eur J Intern Med. 2021;85:63–67. doi:10.1016/j.ejim.2020.12.003
- Atila C, Sailer CO, Bassetti S, et al. Prevalence and outcome of dysnatremia in patients with COVID-19 compared to controls. Eur J Endocrinol. 2021;184 (3):409–418. doi:10.1530/EJE-20-1374
- Tzoulis P, Waung JA, Bagkeris E, et al. Dysnatremia is a predictor for morbidity and mortality in hospitalized patients with COVID-19. J Clin Endocrinol Metab. 2021;106 (6):1637–1648. doi:10.1210/clinem/dgab107
- Bernardi M, Zaccherini G. Approach and management of dysnatremias in cirrhosis. Hepatol Int. 2018;12 (6):487–499. doi:10.1007/s12072-018-9894-6
- Huang H, Jolly SE, Airy M, et al. Associations of dysnatremias with mortality in chronic kidney disease. Nephrol Dial Transplant. 2017;32 (7):1204–1210. doi:10.1093/ndt/gfw209
- Sen S, Tran N, Chan B, et al. Sodium variability is associated with increased mortality in severe burn injury. Burns Trauma. 2017;5:34. doi:10.1186/s41038-017-0098-4
- Darmon M, Diconne E, Souweine B, et al. Prognostic consequences of borderline dysnatremia: pay attention to minimal serum sodium change. Crit Care. 2013;17 (1):R12. doi:10.1186/cc11937
- Martino M, Falcioni P, Giancola G, et al. Sodium alterations impair the prognosis of hospitalized patients with COVID-19 pneumonia. Endocr Connect. 2021;10 (10):1344–1351. doi:10.1530/EC-21-0411
- Chen L, Liu C, Liu L. Osmolality-induced tuning of action potentials in trigeminal ganglion neurons. Neurosci Lett. 2009;452 (1):79–83. doi:10.1016/j.neulet.2009.01.022
- Chen L, Liu C, Liu L, Cao X. Changes in osmolality modulate voltage-gated sodium channels in trigeminal ganglion neurons. Neurosci Res. 2009;64 (2):199–207. doi:10.1016/j.neures.2009.02.012
- Becker D, Bereiter-Hahn J, Jendrach M. Functional interaction of the cation channel transient receptor potential vanilloid 4 (TRPV4) and actin in volume regulation. Eur J Cell Biol. 2009;88 (3):141–152. doi:10.1016/j.ejcb.2008.10.002
- Vanhaebost J, Palmiere C, Scarpelli MP, et al. Postmortem diagnosis of hyponatremia: case report and literature review. Int J Legal Med. 2018;132 (1):173–179. doi:10.1007/s00414-017-1601-y
- Urso C, Brucculeri S, Caimi G. Physiopathological, epidemiological, clinical and therapeutic aspects of exercise-associated hyponatremia. J Clin Med. 2014;3 (4):1258–1275. doi:10.3390/jcm3041258
- Bihari S, Peake SL, Bailey M, et al. Admission high serum sodium is not associated with increased intensive care unit mortality risk in respiratory patients. J Crit Care. 2014;29 (6):948–954. doi:10.1016/j.jcrc.2014.06.008
- Krüger S, Ewig S, Giersdorf S, et al. Dysnatremia, vasopressin, atrial natriuretic peptide and mortality in patients with community-acquired pneumonia: results from the German competence network CAPNETZ. Respir Med. 2014;108 (11):1696–1705. doi:10.1016/j.rmed.2014.09.014
- Stewart AG, Waterhouse JC, Billings CG, et al. Hormonal, renal, and autonomic nerve factors involved in the excretion of sodium and water during dynamic salt and water loading in hypoxaemic chronic obstructive pulmonary disease. Thorax. 1995;50 (8):838–845. doi:10.1136/thx.50.8.838
- Yagi T, Kaneko T, Tsuruta R, et al. Global end-diastolic volume, serum osmolarity, and albumin are risk factors for increased extravascular lung water. J Crit Care. 2011;26 (2):224.e9–13. doi:10.1016/j.jcrc.2010.07.011
- Shen Y, Cheng X, Ying M, et al. Association between serum osmolarity and mortality in patients who are critically ill: a retrospective cohort study. BMJ Open. 2017;7 (5):e015729. doi:10.1136/bmjopen-2016-015729
- Yu Y, Yu J, Yao R, et al. Admission serum ionized and total calcium as new predictors of mortality in patients with cardiogenic shock. Biomed Res Int. 2021;2021:6612276. doi:10.1155/2021/6612276
- Yang J, Yang J. Association between blood eosinophils and mortality in critically ill patients with acute exacerbation of chronic obstructive pulmonary disease: a Retrospective Cohort Study. Int J Chron Obstruct Pulmon Dis. 2021;16:281–288. doi:10.2147/COPD.S289920
- Zhu M, Dai L, Wan L, et al. Dynamic increase of red cell distribution width predicts increased risk of 30-day readmission in patients with acute exacerbation of chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2021;16:393–400. doi:10.2147/COPD.S291833
- Kumar P, Law S, Sriram KB. Evaluation of platelet lymphocyte ratio and 90-day mortality in patients with acute exacerbation of chronic obstructive pulmonary disease. J Thorac Dis. 2017;9 (6):1509–1516. doi:10.21037/jtd.2017.05.77
- Sakurai K, Chubachi S, Irie H, et al. Clinical utility of blood neutrophil-lymphocyte ratio in Japanese COPD patients. BMC Pulm Med. 2018;18 (1):65. doi:10.1186/s12890-018-0639-z