 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Background and objective
Patients with chronic obstructive pulmonary disease (COPD) present with reduced exercise capacity due to impaired oxygen consumption (VO2), caused primarily by pulmonary dysfunction and deleterious peripheral adaptations. Assuming that COPD patients present with slower VO2 and heart rate (HR) on-kinetics, we hypothesized that this finding is related to disease severity as measured by the BODE Index. In this context, the present study intends to evaluate the relationship between VO2 uptake on-kinetics during high-intensity exercise and the BODE Index in patients with COPD.
Methods
Twenty males with moderate-to-severe stable COPD and 13 healthy control subjects matched by age and sex were evaluated. COPD patients were screened by the BODE Index and then underwent an incremental cardiopulmonary exercise test and a constant speed treadmill session at 70% of maximal intensity for 6 minutes. The onset of the exercise (first 360 seconds) response for O2 uptake and HR was modeled according to a monoexponential fit.
Results
Oxygen consumption and HR on-kinetics were slower in the COPD group compared with controls. Additionally, VO2 on-kinetic parameters revealed a strong positive correlation (r = 0.77, P < 0.05) with BODE scores and a moderate negative correlation with walking distance (r = −0.45, P < 0.05).
Conclusion
Our data show that moderate-to-severe COPD is related to impaired oxygen delivery and utilization during the onset of intense exercise.
Keywords:
Introduction
Patients with chronic obstructive pulmonary disease (COPD) present with reduced exercise capacity due to a combination of factors including impaired cardiopulmonary responses,Citation1 leading to inadequate pulmonary oxygen (O2) uptake and delivery to active skeletal muscle,Citation2,Citation3 derangements in the intracellular biochemical reactions in relation to mitochondrial oxygen consumption (VO2)Citation4,Citation5 and/or mechanical abnormalities.
Following the onset of constant workload exercise, the O2 uptake increase (ie, on-kinetics) in COPD patient, which can be characterized by the time required for VO2 to achieve steady state in response to physical stress, is slowed when compared to apparently healthy matched controls. From a clinical context, O2 uptake on-kinetics has been shown to have even better prognostic value than peak VO2 in chronic disease populations.Citation6,Citation7 Moreover, recent studies have shown that, like O2 uptake on-kinetics, heart rate (HR) on-kinetics, are also slower in COPD patients.Citation1,Citation8 Some investigatorsCitation1,Citation8,Citation9 have postulated that slower O2 uptake and HR on-kineticsCitation10 may reflect the adjustment of both oxygen delivery and muscle metabolism during physical exerciseCitation11 as well as exercise performance/functional capacity in these patients.
Additionally, forced expiratory volume in 1 second (FEV1), a measurement that quantifies the degree of airway obstruction, is often used to diagnose and quantify COPD severity.Citation12 Moreover, the rate of decline in FEV1 is a good marker of disease progression and mortality, however, it does not adequately reflect systemic manifestations that contribute to reduced exercise performance in COPD.Citation13
The BODE Index, comprising of body mass index, airflow obstruction, dyspnea, and exercise capacity, has shown to be superior to FEV1 in predicting clinical outcomes in the COPD population.Citation13 This multivariate scoring system can provide useful prognostic information in COPD and reflects functional disability induced by systemic consequences of this disease.Citation13,Citation14 Recently, it have been suggested that serum C-reactive protein, an important systemic inflammation marker, combined with the BODE Index, has a higher combined prognostic value for patients with COPD.Citation15 In this context, on-kinetic alterations have been shown to be useful parameters to objectively evaluate the systemic consequences related to inability to perform submaximal exercise in COPD patients.Citation1
In this context, the present study intends to evaluate the relationship between the metabolic demand during the onset of exercise and the BODE Index in patients with COPD. Assuming that COPD patients present with slower O2 uptake and HR on-kinetics, which is an important index of exercise performance, we hypothesize that the slower O2 uptake onkinetic response is related to the level of disease severity, as represented by the BODE Index.
Methods
Study population
The study population was comprised of 20 men that volunteered to participate in the study with clinical and functional diagnosis of COPD according to the Global Initiative for Obstructive Lung DiseaseCitation16 criteria, presenting with a FEV1/forced vital capacity (FVC) of <0.7 and a postbronchodilator FEV1 < 60% predicted.
No subject in the COPD group had ever participated in a pulmonary rehabilitation program. Criteria for inclusion were: adherence to the individually prescribed treatment regimen and disease stability indicated by no change in medication dosage or exacerbation of symptoms for at least 1 month prior to study enrollment. All patients presented with dyspnea during daily activities (Medical Research Council [MRC] grades II–III).Citation17 Exclusion criteria were: malignancy, orthopedic or neurological conditions affecting the ability to exercise, peripheral arterial disease, clinically apparent heart failure, and/or any renal, hepatic, or inflammatory disease.
Thirteen healthy control subjects (control group [CG]), matched according to age and sex, were also included in this investigation. Our laboratory posted an announcement at the university inviting healthy subjects to enroll as control subjects for this study. Subjects in the CG were free of any history of arterial hypertension, serious cardiac disease, or associated lung disease, were nonsmokers, and had not participated in regular daily physical activity during the past year. All participants signed a written informed consent and the study design was approved by the Human Ethics Committee of the Universidade Federal de Sao Carlos, Brazil, in compliance with the Declaration of Helsinki.
Measurements
Lung function
All patients underwent spirometry to quantify FEV1 and FVC according to American Thoracic Society recommendations.Citation16 The values obtained were compared to the predicted normal values of Knudson et al.Citation18 Spirometry was performed using a Vitalograph® Hand-Held 2120 instrument (Ennis, Ireland), which was calibrated before each test according to manufacturer recommendations using a 1-L syringe.
Six-minute walking test (6MWT)
Performed as described by American Thoracic Society Guidelines.Citation19 Two tests were performed on alternating days within 48 hours. The test with the greatest six-minute walking distance (6MWD) was considered for analysis, as the first test tends to underestimate exercise capacity due to the subject’s lack of familiarity with the test.Citation19 Each patient was instructed to walk from one end to the other, covering as much ground as possible during the allotted time and all patients were given standardized encouragement during the test.
BODE Index
Measurements to calculate this index were performed in all subjects in the COPD group. The BODE Index (B: body mass index; O: degree of airflow obstruction; D: dyspnea; E: exercise capacity), is a multidimensional index comprising of BMI, degree of airway obstruction (FEV1), functional dyspnea (MRC dyspnea scale), and exercise capacity via the 6MWT. For calculation of the BODE Index, we used an empirical model as previously described.Citation13 For the first parameter, the value was 0 or 1. For the last three parameters, FEV1, distance walked in 6 minutes, and score on the modified MRC dyspnea scale, the patients received points ranging from 0 (lowest value) to 3 (maximal value). The points for each variable were added, so that the BODE Index was the sum of points for each variable, ranging from 0 to 10 in each subject. The BODE Index can be divided into four quartiles: quartile I is a score of 0–2; quartile II is a score of 3–4; quartile III a score of 5–6; and quartile IV a score of 7–10.
Cardiopulmonary exercise testing (CPX)
Incremental symptom-limited exercise testing was performed on a treadmill using a computer-based ventilatory expired gas analysis system (VO2000; Medgraphics Corp, St Paul, MN) in accordance with a previously described protocol.Citation20 The VO2000 uses a galvanic fuel cell for the oxygen analyzer (range 0%–96%) and a nondispersive infrared carbon dioxide analyzer (range 0%–10%), both of which were calibrated prior to each exercise test as per manufacturer instructions. A low-flow pneumotach (preVent Pneumotach, MGC; range 2–30 L · min−1) was calibrated with a 3-L volume syringe. Acceptable interday reliability for ventilation (CV 7.3%–8.8%), oxygen consumption (VO2) and carbon dioxide (VCO2; CV 5.3%–6.0%) has been demonstrated in a previous study.Citation21 VO2 (in mL · min−1) was sampled for each three breaths and 10-second averaged data were recorded for further analysis. Oxyhemoglobin saturation (SpO2, %) was determined by pulse oximetry (8500A; Nonin, Plymouth, MN). Subjects were also asked to rate their “shortness of breath” at exercise cessation using the 0–10 Borg’s category-ratio scale.Citation22
Constant speed exercise test (CSET)
The CSET were performed at 70% of the previously determined speed (during CPX) at 3° inclination on a treadmill, for 6 minutes. During the CSET, VO2, SpO2, HR, and the electrocardiogram were continuously monitored. The VO2 and HR data from the onset of CSET were used for on-kinetics analysis.
On-kinetics analysis
In order to understand the behavior of HR and VO2 during the onset of exercise, an on-kinetics analysis was performed for each variable.Citation23 The CSET VO2 and HR data obtained were entered and analyzed into SigmaPlot 10.0, Systat Software (San Jose, CA) to be analyzed. In order to eliminate an occasional errant data point arising from coughs, sighs or swallows, VO2 data that surpassed four standard deviations from the local mean was omitted.Citation24,Citation25 The onset of exercise (first 360 seconds) response was modeled using a monoexponential fit.
where ‘f(t)’ represents VO2 or HR at any time (t); ‘a0’ is the baseline value corresponding to a mean value at the last minute of baseline prior to the constant workload test; ‘a’ is the amplitude, ie, steady-state increase above baseline; ‘τ’ is the time constant, ie, the time taken to reach 63% of the function; and ‘TD’ is the time delay of the function. A warm-up was performed to minimize the effects of the cardiodynamic phase on the O2 uptake on-kinetics response.Citation26 Additionally, the mean response time (MRT, the time taken to reach 63% of total response following the onset of exercise) was calculated as the weighted sum of the ‘TD’ and ‘τ’.Citation27 The inclusion of ‘TD’ in this equation was established due the possibility that VO2 or HR does not start to rise immediately at the onset of the imposed workload.Citation28 Given the fact that ‘τ’ and MRT are time parameters from an exponential function, the lower its values, the faster the VO2 and/or HR response.Citation29,Citation30
To determine the parameters of the best curve fit, a nonlinear algorithm of least squares was used. This model adopts the minimization of the sum of square errors as a criterion for convergence. The ‘a’ and ‘a0’ describe the parameters related to the component of Y axis (VO2 or HR), the ‘τ’ and ‘TD’ describe the parameters related to X axis (time). Only the function with r > 95% was included in final analysis, which guarantees a good quality of fit.Citation28
Statistical analysis
Sample size was based on the analysis of the ‘τVO2’ values obtained in a pilot study (5 subjects) with β = 0.8 and α = 0.05 (MedCalc Software, version 11.2.1.0 (Mariakerke, Belgium)). The results suggested at least 10 subjects in each group with differences of 5 seconds were needed to be sufficiently powered. The Shapiro–Wilk test was used to verify data distribution and heterogeneous variance (Levene test). Unpaired t-tests were used in the current analysis given all parameters demonstrated a normal distribution. The data were presented as mean and standard deviation. We used Pearson correlation analysis to evaluate the relationship between the variables. The level of significance was set at 5% (SigmaPlot version 11.0).
Results
Anthropometric characteristics
lists the demographic characteristics of the subjects studied. There were no differences in age or anthropometric characteristics. Two patients had GOLD stage II COPD, ten had GOLD stage III and eight had stage IV of COPD. As expected, COPD subjects had lower values of pulmonary function compared with healthy controls. All subjects completed the 6MWT protocol without complication.
Table 1 Age, anthropometric, and functional characteristics of COPD and control (CG) groups
lists values of O2 uptake on-kinetics analysis achieved during the CSET. The COPD group exercise at a lower power output and achieved a lower VO2 and HR “steady state” (‘a’, amplitude). Moreover, the time constant ‘τ’ associated with reaching VO2 steady state was longer in COPD. The VO2 and HR MRT was longer in the COPD group in compared with the CG (P < 0.05).
Table 2 On-kinetics parameters obtained during constant workload exercise tests (CWET) in COPD and control groups
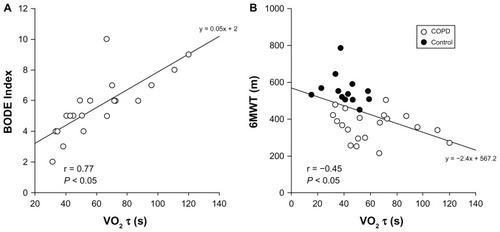
The Pearson correlation presented with a modest relationship between 6MWT distance and τVO2 (; r = −0.45, P < 0.05) as well as FEV1 (r = −0.49, P = 0.05). Interestingly, however, the relationship between the BODE Index and τVO2 demonstrated a strong correlation (; r = 0.77, P < 0.01).
Figure 1 Relationship between the BODE Index (A) and the 6MWT (B) with the time constant (τ) for the on-transient of pulmonary oxygen (O2) uptake in COPD patients.
Abbreviations: COPD, chronic obstructive pulmonary disease; 6MWT, 6-Minute Walking Test; VO2τ, oxygen uptake on kinetic.
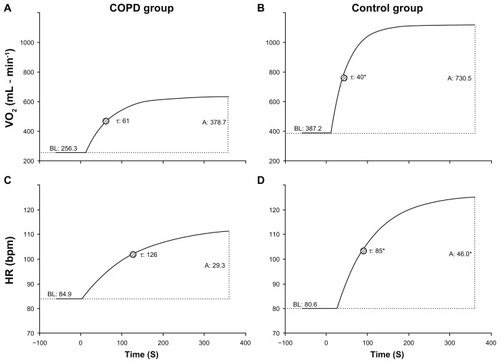
Finally, illustrates the mean fit of O2 uptake and HR on-kinetics during CSET performed on a treadmill, which shows significant differences between the COPD and CG (P < 0.05). For the construction of these functions, the values obtained for the O2 uptake on-kinetics analysis (the same listed in ) were inserted in the kinetics equation described above and plotted as a function.
Figure 2 Illustration of the fitted curves using the means of VO2 (A and B) and HR (C and D) kinetics during the constant-speed exercise tests (CSET) performed on a treadmill at intense exercise (70% of peak) in COPD (A and C) and control patients (B and D).
Abbreviations: COPD, chronic obstructive pulmonary disease; HR, heart rate; VO2, oxygen consumption.
Discussion
The main important finding of the present study is that τVO2 demonstrated a strong correlation with the BODE Index. In addition, this study revealed that O2 uptake and HR on-kinetics were slower in the COPD group compared to the CG during CSET. These results indicate that a combined analysis of exercise on-kinetic responses and the BODE Index may serve as an important marker of diminished functional capacity, potentially indicating a worse prognosis in this patient population.
On-kinetics of oxygen uptake and heart rate
Due the fact that parameters “τ” and “MRT” are exponential time constants,Citation29 lower values indicate a better adjustment to exercise and more favorable physiologic function.
Based on the kinetic responses observed in the current study, we found that O2 uptake and HR on-kinetics were slower (higher values of ‘τ’ and ‘MRT’) in COPD patients compared to the CG during CSET on a treadmill. In accordance with our results, several investigatorsCitation1,Citation31,Citation32 have reported that O2 uptake on-kinetics are delayed in patients with COPD during constant work rate exercise on a cycle ergometer. The exact mechanism of slowed on-kinetics in patients with COPD is unclear, but Chiappa et alCitation1 demonstrated that it may be related to a prolonged O2 delivery and utilization at the onset of exercise.Citation6 It is widely recognized that disturbances in the diffusive and/or convective transport of O2 to skeletal muscle mitochondriaCitation33,Citation34 and/or intramyocyte metabolic machineryCitation35–Citation37 could explain the attenuation of O2 uptake on-kinetics in patients with cardiopulmonary and metabolic disorders.
In fact, hypoxemia,Citation3 autonomic imbalance,Citation38 blood flow redistribution from peripheral to respiratory muscles,Citation39,Citation40 derangements in muscle vasodilatation capacity,Citation41 and increased intrathoracic and/or pleural pressures (swings on central hemodynamic adjustments) can all negatively impact the O2 uptake response at the onset of exercise. Some therapeutic strategiesCitation31,Citation32,Citation40,Citation42 have been demonstrated to increase the O2 uptake on-kinetics speed, supporting the importance of different interventions on the respiratory-mechanical system in order to improve functional capacity in COPD patients.
The other important issue investigated in the current study is slower HR on-kinetics identified in the experimental group, which has been previously described in patients with COPD.Citation1 In fact, cardiovascular responses that should help maintain adequate O2 delivery to contracting muscle are impaired in COPD. Supposedly, slower HR on-kinetics can be explained by autonomic imbalance,Citation43 pulmonary vascular alteration, and/or effects of mechanisms of breathing on venous return.Citation38 Therefore, the assessment of HR on-kinetics may have particular clinical utility in reflecting physiologic function, disease severity and the response to therapeutic interventions in this chronic disease population.
On-kinetics: BODE Index relationship
The BODE Index has proven useful in evaluating the severity of COPD. As this index incorporates measures of airway obstruction, body mass composition, symptomatology and functional capacity, it captures a comprehensive panel of limitations induced by COPD. Assuming that severe COPD induces expressive peripheral muscle dysfunction and functional limitation, it seems rational to suspect that these patients presented with slowed O2 uptake on-kinetics as an additional reflection of their advanced disease severity. Interestingly, however, in this regard the BODE Index demonstrated a strong correlation with O2 uptake on-kinetics. In fact, the correlation was much stronger than for the 6MWD or FEV1. These results may be explained by the fact that COPD has a systemic component that includes significant extrapulmonary effects that may contribute to disease severity variability amongst patients. In parallel, O2 uptake and HR on-kinetics may infer the impairment of central cardiorespiratory and/or peripheral muscle in these patients.
To the best of our knowledge, this study is the first to assess the relationship between the BODE Index and O2 uptake on-kinetics, which adds another dimension to BODE Index interpretation. Previous studies have shown that the BODE Index is correlated to other markers of functional performance. Regueiro et alCitation44 evaluated 10 moderate to severe COPD patients and demonstrated a strong correlation between the sit-to-stand test, hand grip strength test and the 6MWT (−0.86 against −0.45 in our study) and the BODE Index. These authors suggested that the BODE Index could be used to predict functional capacity. Simon et alCitation45 demonstrated that 39 patients with moderate to severe COPD presented a significant relationship between the BODE Index and physical activity assessed by the London Chest Activity of Daily Living Scale score. These authors suggested that BODE Index can therefore assist in the interpretability of the London questionnaire. Another recent studyCitation46 was able to demonstrate that higher amounts of daily physical activity in 107 patients with moderate-to-severe COPD was associated with a lower BODE Index. In agreement, Mantoani et alCitation47 found a significant moderate correlation between the BODE Index and amount of daily physical activity in 67 patients with COPD. Accordingly, the results of the current study add to this body of literature by demonstrating a correlation between the BODE Index and another marker of exertional physiology, O2 uptake on-kinetics. Thus, this allows us to infer that the BODE Index may reflect the degree of central/peripheral physiologic dysfunction induced by COPD and manifested by slower O2 uptake and HR on-kinetics.
Limitations of this study
Firstly, it should be recognized that breath-by-breath analysis is the best way to obtain samples to fit the O2 uptake on-kinetic response, however, other authorsCitation48,Citation49 have used this approach previously and showed reliability of the data collectedCitation50 with good fit results. Secondly, the protocol used in this study was conducted on a treadmill. In fact, protocols on a cycle ergometer allow for a more precise measurement of external work rate. However, in this study we aimed to assess the functional capacity of COPD patients using an exercise mode that may more closely mimic activities of daily living (ie, ambulation). Moreover, exercise tests on a treadmill have been used to assess the on-kinetic response in the past.Citation25,Citation51,Citation52 Thirdly, we analyzed the time (‘τ’) to achieve 63% of steady rate, which may be overestimated by τHR if compared to other studies that used T1/2 (50% of steady state).Citation1 However, we observed that the current study found COPD subjects presented with slower HR on-kinetics when compared to the CG, indicating a central limitation in these patients. Finally, we used a 6-minute protocol to analyze HR on-kinetics in order to compare it with O2 uptake on-kinetic response. However, our results showed that the exponential model used to analyze the HR response may not be best represented by a 6-minute sample.
Importance of this study
Previous investigators have reported that COPD patients present with delayed O2 uptake on-kinetics, which was also demonstrated in the current study using a constant speed on a treadmill. However, no previous investigation demonstrated that the degree of COPD severity is related to the O2 uptake on-kinetic response. This is an important consideration as it adds another dimension to interpretation of the BODE Index, which is frequently employed in clinical practice. Delayed O2 uptake and HR on-kinetics may be related to the reduction in exercise tolerance associated with poor prognosis assessed by the BODE Index in COPD patients.
Some therapeutic strategies that optimize exercise tolerance (ie, dynamic and/or strength training), accelerating exercise on-kinetics, may decrease the risk of exacerbations and death in these patients.Citation53 Additionally, O2 uptake on-kinetics analysis can be used as a follow-up measure in many different therapeutic interventions.
Conclusion
In general, our data show that patients with moderate to severe COPD have impaired O2 uptake and HR on-kinetics at the onset of intense exercise on a treadmill. In addition, we found a strong relationship between the BODE Index and O2 uptake on-kinetics. Thus, COPD severity leads to an attenuated on-kinetics response during exercise which can be captured by the BODE Index.
Acknowledgments
This study received financial support from FAPESP (2009/01842-0) and CNPq (#483945/2007-2). The coauthors Thomas Beltrame (#130549/2011-8) and Michel Silva Reis received CNPq and PNPD-Capes fellowship, respectively. A Borghi-Silva is an Established Investigator (level II) of the Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq), Brazil.
Disclosure
The authors report no conflicts of interest in this work.
References
- ChiappaGRBorghi-SilvaAFerreiraLFKinetics of muscle deoxygenation are accelerated at the onset of heavy-intensity exercise in patients with COPD: relationship to central cardiovascular dynamicsJ Appl Physiol200810451341135018356477
- SalaERocaJMarradesRMEffects of endurance training on skeletal muscle bioenergetics in chronic obstructive pulmonary diseaseAm J Respir Crit Care Med199915961726173410351910
- SomfayAPorszaszJLeeSMCasaburiREffect of hyperoxia on gas exchange and lactate kinetics following exercise onset in nonhypoxemic COPD patientsChest2002121239340011834648
- WuyamBPayenJFLevyPMetabolism and aerobic capacity of skeletal muscle in chronic respiratory failure related to chronic obstructive pulmonary diseaseEur Respir J1992521571621559579
- CasaburiRSkeletal muscle dysfunction in chronic obstructive pulmonary diseaseMed Sci Sports Exerc200133Suppl 7S662S67011462075
- ShimizuNKoikeAKoyamaYKobayashiKMarumoFHiroeMKinetics of pulmonary gas exchange during and while recovering from exercise in patients after anterior myocardial infarctionJpn Circ J199963645946610406586
- PooleDCHiraiDMCoppSWMuschTIMuscle oxygen transport and utilization in heart failure: implications for exercise (in)toleranceAm J Physiol Heart Circ Physiol20123025H1050H106322101528
- LavenezianaPValliGOnoratiPPaolettiPFerrazzaAMPalangePEffect of heliox on heart rate kinetics and dynamic hyperinflation during high-intensity exercise in COPDEur J Appl Physiol2011111222523420852881
- Puente-MaestuLSanzMLSanzPNunezAGonzalezFWhippBJReproducibility of the parameters of the on-transient cardiopulmonary responses during moderate exercise in patients with chronic obstructive pulmonary diseaseEur J Appl Physiol200185543444111606012
- NeryLEWassermanKAndrewsJDHuntsmanDJHansenJEWhippBJVentilatory and gas exchange kinetics during exercise in chronic airways obstructionJ Appl Physiol1982536159416026818216
- HughsonRLOxygen uptake kinetics: historical perspective and future directionsAppl Physiol Nutr Metab200934584085019935845
- PauwelsRABuistASCalverleyPMJenkinsCRHurdSSGlobal strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. NHLBI/WHO Global Initiative for Chronic Obstructive Lung Disease (GOLD) Workshop summaryAm J Respir Crit Care Med200116351256127611316667
- CelliBRCoteCGMarinJMThe body-mass index, airflow obstruction, dyspnea, and exercise capacity index in chronic obstructive pulmonary diseaseN Engl J Med2004350101005101214999112
- MarinJMCoteCGDiazOPrognostic assessment in COPD: health related quality of life and the BODE indexRespir Med2011105691692121282050
- LiuSFWangCCChinCHChenYCLinMCHigh value of combined serum C-reactive protein and BODE score for mortality prediction in patients with stable COPDArch Bronconeumol201147942743221821335
- Lung function testing: selection of reference values and interpretative strategiesAmerican Thoracic SocietyAm Rev Respir Dis19911445120212181952453
- FabbriLMHurdSSGlobal Strategy for the Diagnosis, Management and Prevention of COPD: 2003 updateEur Respir J20032211212882441
- KnudsonRJLebowitzMDHolbergCJBurrowsBChanges in the normal maximal expiratory flow-volume curve with growth and agingAm Rev Respir Dis198312767257346859656
- ATS Committee on Proficiency Standards for Clinical Pulmonary Function LaboratoriesATS statement: guidelines for the six-minute walk testAm J Respir Crit Care Med2002166111111712091180
- Borghi-SilvaABaldisseraVSampaioLML-carnitine as an ergogenic aid for patients with chronic obstructive pulmonary disease submitted to whole-body and respiratory muscle training programsBraz J Med Biol Res200639446547416612469
- CrouterSEAntczakAHudakJRDellaValleDMHaasJDAccuracy and reliability of the ParvoMedics TrueOne 2400 and MedGraphics VO2000 metabolic systemsEur J Appl Physiol200698213915116896734
- BorgGAPsychophysical bases of perceived exertionMed Sci Sports Exerc19821453773817154893
- AndrewPJonesDCPOxygen Uptake Kinetics in Sport, Exercise and MedicineNew York, NYRoutledge2005
- BeardenSEMoffattRJLeg electromyography and the VO2-power relationship during bicycle ergometryMed Sci Sports Exerc20013371241124511445775
- BorraniFCandauRMilletGYPerreySFuchslocherJRouillonJDIs the VO2 slow component dependent on progressive recruitment of fast-twitch fibers in trained runners?J Appl Physiol20019062212222011356785
- WhippBJWardSALamarraNDavisJAWassermanKParameters of ventilatory and gas exchange dynamics during exerciseJ Appl Physiol1982526150615136809716
- BellCPatersonDHKowalchukJMPadillaJCunninghamDAA comparison of modelling techniques used to characterise oxygen uptake kinetics during the on-transient of exerciseExp Physiol200186566767611571496
- RossiterHBWardSAKowalchukJMHoweFAGriffithsJRWhippBJDynamic asymmetry of phosphocreatine concentration and O(2) uptake between the on- and off-transients of moderate- and high-intensity exercise in humansJ Physiol2002541Pt 3991100212068057
- MotulskyHJRansnasLAFitting curves to data using nonlinear regression: a practical and nonmathematical reviewFASEB J1987153653743315805
- BeardenSEMoffattRJVO2 and heart rate kinetics in cycling: transitions from an elevated baselineJ Appl Physiol20019062081208711356769
- SiqueiraACBorghi-SilvaABravoDMFerreiraEMChiappaGRNederJAEffects of hyperoxia on the dynamics of skeletal muscle oxygenation at the onset of heavy-intensity exercise in patients with COPDRespir Physiol Neurobiol3020101721–281420417729
- BertonDCBarbosaPBTakaraLSBronchodilators accelerate the dynamics of muscle O2 delivery and utilisation during exercise in COPDThorax201065758859320627914
- HughsonRLTschakovskyMEHoustonMERegulation of oxygen consumption at the onset of exerciseExerc Sport Sci Rev200129312913311474961
- MacDonaldMJNaylorHLTschakovskyMEHughsonRLPeripheral circulatory factors limit rate of increase in muscle O(2) uptake at onset of heavy exerciseJ Appl Physiol2001901838911133896
- BurnleyMJonesAMCarterHDoustJHEffects of prior heavy exercise on phase II pulmonary oxygen uptake kinetics during heavy exerciseJ Appl Physiol20008941387139611007573
- GrassiBPooleDCRichardsonRSKnightDREricksonBKWagnerPDMuscle O2 uptake kinetics in humans: implications for metabolic controlJ Appl Physiol19968039889988964765
- GrassiBGladdenLBSamajaMStaryCMHoganMCFaster adjustment of O2 delivery does not affect V(O2) on-kinetics in isolated in situ canine muscleJ Appl Physiol1998854139414039760333
- HeindlSLehnertMCrieeCPHasenfussGAndreasSMarked sympathetic activation in patients with chronic respiratory failureAm J Respir Crit Care Med2001164459760111520722
- RichardsonRSSheldonJPooleDCHopkinsSRRiesALWagnerPDEvidence of skeletal muscle metabolic reserve during whole body exercise in patients with chronic obstructive pulmonary diseaseAm J Respir Crit Care Med1999159388188510051266
- Borghi-SilvaAOliveiraCCCarrascosaCRespiratory muscle unloading improves leg muscle oxygenation during exercise in patients with COPDThorax2008631091091518492743
- GaenzerHNeumayrGMarschangPSturmWKirchmairRPatschJRFlow-mediated vasodilation of the femoral and brachial artery induced by exercise in healthy nonsmoking and smoking menJ Am Coll Cardiol20013851313131911691501
- ChiappaGRQueirogaFJrMedaEHeliox improves oxygen delivery and utilization during dynamic exercise in patients with chronic obstructive pulmonary diseaseAm J Respir Crit Care Med2009179111004101019299497
- Castello-SimoesVPolaquini SimoesRBeltrameTEffects of aerobic exercise training on variability and heart rate kinetic during submaximal exercise after gastric bypass surgery – a randomized controlled trialDisabil Rehabil6232012 [Epub ahead of print.]
- RegueiroEMDi LorenzoVABassoRPPessoaBVJamamiMCostaDRelationship of BODE Index to functional tests in chronic obstructive pulmonary diseaseClinics (Sao Paulo)2009641098398819841705
- SimonKMCarpesMFCorreaKSdos SantosKKarlohMMayerAFRelationship between daily living activities (ADL) limitation and the BODE index in patients with chronic obstructive pulmonary diseaseRev Bras Fisioter201115321221821829985
- JehnMSchmidt-TrucksässAMeyerASchindlerCTammMStolzDAssociation of daily physical activity volume and intensity with COPD severityRespir Med2011105121846185221803556
- MantoaniLCHernandesNAGuimarãesMMVitorassoRLProbstVSPittaFDoes the BODE index reflect the level of physical activity in daily life in patients with COPD?Rev Bras Fisioter20111513113721789363
- HughsonRLAlterations in the oxygen deficit-oxygen debt relationships with beta-adrenergic receptor blockade in manJ Physiol19843493753876429319
- ArenaRHumphreyRPeberdyMAMadiganMComparison of oxygen uptake on-kinetic calculations in heart failureMed Sci Sports Exerc200234101563156912370556
- MyersJWalshDSullivanMFroelicherVEffect of sampling on variability and plateau in oxygen uptakeJ Appl Physiol19906814044102312484
- BauerTABrassEPNehlerMBarstowTJHiattWRPulmonary VO2 dynamics during treadmill and arm exercise in peripheral arterial diseaseJ Appl Physiol200497262763415090483
- Brunner-La RoccaHPWeilenmannDFollathFOxygen uptake kinetics during low level exercise in patients with heart failure: relation to neurohormones, peak oxygen consumption, and clinical findingsHeart19998121211279922345
- BarakatSMicheleGGeorgePNicoleVGuyAOutpatient pulmonary rehabilitation in patients with chronic obstructive pulmonary diseaseInt J COPD200831155162