
Abstract
Purpose
The Spanish Activity Questionnaire in COPD (SAQ-COPD) is a short, simple physical activity (PA) measurement instrument for patients with chronic obstructive pulmonary disease (COPD). In this study, we analyzed its validity and sensitivity to change.
Methods
Prospective scale validation study. An accelerometer (DynaPort MoveMonitor®) and the Yale Physical Activity Survey (YPAS) were used as reference standards. The analyses examined the criterion validity (Spearman correlations), internal consistency (Cronbach’s alpha), factorial structure, test-retest reliability (intraclass correlation coefficient, ICC), sensitivity to change and receiver operating characteristic (ROC) curve to classify patients with low PA.
Results
A total of 300 patients diagnosed with COPD were analyzed (73% males, mean age 66 ± 8 years, 40.3% with severe airflow limitation). Cronbach’s alpha was 0.60 and Spearman's correlations with accelerometer measurements of PA [number of steps, metabolic equivalents (MET), physical activity level (PAL)] and YPAS ranged from 0.37 to 0.53 (all p < 0.001). ICC was 0.69 (95% CI 0.61–0.74) and the area under the ROC curve to identify low PA was 0.65 (95% confidence interval: 0.58–0.73). Significant variations in SAQ-COPD scores were found between groups defined by YPAS for change.
Conclusion
The SAQ-COPD questionnaire is a valid instrument for classifying PA in patients with COPD. Correlations with other instruments provide criterion validity and also demonstrate good sensitivity to change.
Introduction
Research conducted in the last decade on physical activity (PA) has positioned it as a key factor in the course of chronic obstructive pulmonary disease (COPD).Citation1 It is therefore increasingly necessary to assess the role played by pathophysiological abnormalities derived from the disease and psychological, behavioral, cultural, and social factors in the eventual decrease in PA in patients with COPD.Citation2,Citation3
It is known that COPD patients have lower PA levels than healthy individuals of the same age.Citation4 This decrease in activity begins in the early stages of disease,Citation5 even before the onset of dyspnea,Citation6 and is a predictor of poor prognosis, including hospitalizations, mortalityCitation7,Citation8 and health-related quality of life.Citation9 Fortunately, the lack of PA in patients with COPD is a potentially treatable condition that constitutes an important therapeutic goal.Citation3 Therefore, current research focuses on optimizing its identification for the promotion of both pharmacological and non-pharmacological therapeutic interventions.
PA in COPD can be quantified by specific monitors and questionnaires. Although objective measures of the amount and frequency of activity recorded by pedometers or accelerometers are increasingly rigorous, they are limited for capturing the multifactorial nature of PA, the symptoms experienced by patients while they are active, or patient adaptation mechanisms to overcome their limitations.Citation10 In addition, they are relatively expensive and difficult to use in daily practice.Citation11 In contrast, questionnaires based on subjective patient perception and recall measures allow patients to be categorized according to their PA level,Citation12 but have limitations for evaluating activity patterns or detecting small changes in daily PA.Citation13 In other words, they can classify PA but do not adequately rate or quantify it. Monitors and questionnaires are therefore complementary instruments, and it has been proposed to create and validate hybrid instruments, which combine a questionnaire and activity monitors,Citation13 as these have shown valid and reliable results in different clinical situations, as well as their capacity to respond to pharmacological and non-pharmacological interventions.Citation14
However, clinical practice requires simple, accessible, and easily applicable tools that allow a comprehensive assessment of PA in patients with COPD, based on total activity, amount and difficulty. One of the limitations for the use of PA questionnaires is that there are no standardized instruments sensitive to the low-intensity activities typical of patients with chronic respiratory diseases. Tools sensitive to changes in activity in these patients are therefore needed to assess therapeutic interventions and be feasible for use in all health-care settings.Citation15
With this objective, a multidisciplinary panel of pulmonologists and primary care, sports medicine and rehabilitation physicians developed a PA questionnaire for patients with COPD called SAQ-COPD (Spanish Physical Activity in COPD).Citation16 This questionnaire aims to quantify the PA performed and to explore its main limiting factors and the patient’s attitude to it. To assess its usefulness in clinical practice, the purpose of this study was to perform the initial validation of the SAQ-COPD questionnaire in patients with COPD, using as reference elements the objective measurement of PA by an accelerometer and another questionnaire previously validated in this disease.
Methods
This is a prospective, observational, scale validation study conducted between September 2018 and October 2020, involving 13 centers, 11 specialist care centers and 2 primary care centers, in 8 Spanish autonomous communities. The study was approved by the Ethics Committee of the Hospital Universitario La Paz (Madrid), with number of ethical approval PI-3011. All patients gave their written informed consent to participate, complying with the Declaration of Helsinki.
Enrolled patients had a diagnosis of COPD (FEV1/FVC <0.7, smoking history of at least 10 pack-years and chronic respiratory symptoms). Patients were consecutively selected at the participating centers in an attempt to maintain the same proportion of patients in terms of severity of airflow limitation according to the Global Initiative for Chronic Obstructive Lung Disease criteria (GOLD 2017).Citation17 Main exclusion criteria were presence of limitations, physical handicaps or medical conditions requiring rest, mental or cognitive impairment that prevented completion of the questionnaire, institutionalization, treatment with continuous home oxygen therapy without available portable oxygen concentrators or liquid oxygen, and occurrence of a moderate-to-severe COPD exacerbation in the four weeks before inclusion.
The study was conducted in 6 visits during 6 months of follow-up: visit 1 at day −7 (screening), visit 2 at day 0 (baseline), visit 3 at day 7 (administration of the accelerometer for test-retest), visit 4 at day 14 (test-retest), visit 5 at day 173 (administration of the accelerometer for sensitivity to change) and visit 6 at day 180 (sensitivity to change).
SAQ-COPD Questionnaire
The expert committee had previously developed the SAQ-COPD questionnaire using a methodology of selection by rounds (Delphi method) with subsequent discussion of the outcome.Citation16 The SAQ-COPD questionnaire is divided into two blocks. The first block of 4 items measures PA in four categories: low, moderate, intense and inactivity. Each item is rated on a 0 to 5 Likert scale based on the average daily time spent performing the PA represented by each category in the last 7 days. The score for each PA category is obtained by multiplying the Likert scale value by the number of days indicated, with the minimum score ranging from 0 to 35. The total score is the sum of the scores obtained in each category, with a range between 0 and 140. The second block evaluates the profile and the impact only in patients classified as having low PA in the first block. SAQ-COPD questionnaire was administered by clinician at baseline, at visit 4 after 14 days for test-retest and at visit 6 after 6 months for sensitivity to change.
SAQ-COPD Validation Tools
Accelerometer
The DynaPort MoveMonitor® accelerometer (McRoberts, B.V Raamweg 43, 2596 HN Den Haag, Netherlands) was used because of its high validity to estimate energy expenditure and discriminate between different walking speeds in patients with COPD.Citation18
Patients had to place the accelerometer in the lateral-dorsal region of their waist and use it for 7 consecutive days, with the minimum time of use defined as at least 3 days on which 70% or more of the daytime period was recorded. At 7 days of the accelerometer recording, patients completed the SAQ-COPD,Citation16 since the questions referring to the previous 7 days coincided with the period of use of this instrument. The number of steps per day, physical activity time (hours/day), intensity (MET-h/day), energy expenditure (kcal), and basal metabolic rate (kcal) were obtained for each patient. Physical Activity Level (PAL) is the relationship between total energy expenditure and basal metabolic rate of accelerometer placement periods. Patients placed the accelerometer during 7 days between the screening and baseline visits, between visits 3 and 4, and between visits 5 and 6. Accelerometer measures were registered at baseline, at visit 4 and at visit 6.
Yale Physical Activity Survey (YPAS)
The validated Spanish versionCitation19 of the YPASCitation20 was used. This questionnaire measures the volume, frequency and intensity of PA in a wide list of activities performed in the past 4 weeks based on the daily time spent in the activity (hours) and energy expenditure in the activity. The 7 questions of the questionnaire, which combine frequency and intensity of activities, provide an activity summary index ranging from 0 to 137, with a cut-off point for discriminating sedentary patients of 51.Citation19 YPAS questionnaire was administered by the clinician at baseline and at visit 6 after 6 months for sensitivity to change.
Other Variables of Interest
Sociodemographic, clinical characteristics of patients and main comorbidities were collected at baseline. Responses to CAT (COPD assessment test) questionnaire on health-related quality of lifeCitation21 were collected at baseline and at 6 months. At baseline, a 6-minute walk test was performed in duplicate, according to the recommendations of the American Thoracic Society,Citation22 and the 5-STS (five-repetition sit-to-stand test)Citation23 that measures the time taken by the patient to rise five times from a chair, thus allowing examination of lower limb function.
Statistical Analysis
Sociodemographic and clinical characteristics of patients are presented using descriptive statistics. Normally distributed quantitative variables are reported as mean and standard deviation, and qualitative variables as numbers and percentages.
The validation process integrated the analysis of feasibility, validity, reliability and sensitivity to change. For the feasibility analysis, we used the time taken to complete the questionnaire reported in the development study (4.53 min),Citation16 the percentage of patients with no missing data in the questionnaire, the percentage of patients with no missing data in each dimension, and the variability of responses using the ceiling-floor effect. A ceiling or floor effect was considered when 15% or more responses accumulated at the higher or lower values, respectively.
The validity of the questionnaire was based on: a) concept validity, already analyzed in the opinion of the experts during the creation of the questionnaire;Citation16 b) criterion validity using the reference standards: accelerometer and YPAS; c) construct validity using the Varimax rotation method to aid responses grouping according to underlying (latent) factors that identify the possible dimensions, and to determine the unidimensionality of the instrument.
The overall internal consistency was assessed with baseline score using Cronbach’s alpha statistical method. Test-retest or intra-observer reliability was examined in patients who remained stable between baseline and test-retest visits, considering “stability” as any change lower or equal in absolute value to the standard deviation of the accelerometer physical activity level (PAL) parameter. The intraclass correlation coefficient (ICC) is presented. Interobserver reliability was obtained using the t-test statistic.
As measures of sensitivity to change, the means in SAQ-COPD score in stable or non-stable patients according to YPAS are presented. Cohen criteria were used to estimate the effect size and quantify the difference in means. Diagnostic sensitivity and specificity to discriminate inactive patients from active patients were obtained by analyzing ROC curves using as reference standards the number of steps and PAL of the accelerometer. The cut-off points chosen to classify the population as inactive or active were 6000 steps and 1.7 PAL, respectively.
Results
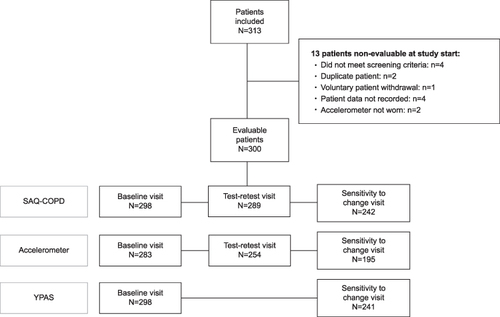
Of 313 patients recruited, 300 were finally evaluated (). shows the main anthropometric and clinical characteristics. Patients were mainly aged 70–80 years, predominantly male, from urban areas and retired, with moderate comorbidities and moderate-to-severe airflow limitation. Most were in groups A and B of the GOLD classification and were ‘non-exacerbators’.
Table 1 Sociodemographic and Baseline Clinical Data in the Study Population
Figure 1 Flow chart. Abbreviations: SAQ-COPD, Spanish Activity Questionnaire in COPD; YPAS, Yale Physical Activity Scale.
Patients recorded a mean number of steps per day of 7108 ± 4329, and the PAL measured using the accelerometer was 1.7 ± 0.2 (). Using cut-off point 51 for the YPAS activity summary index score,Citation24 70.5% of patients were classified as sedentary. According to SAQ-COPD, 77.3% of patients performed at least 30 minutes of low-intensity PA daily and 31.5% performed at least 30 minutes of moderate PA, while only 18.8% performed some type of intense PA on a daily basis (Supplementary Figure 1). A total of 81.2% of patients who did not perform any type of intense PA were in the lowest score range of the intense PA dimension, causing a floor effect. No significant differences were found in mean PAL, MET and daily number of accelerometer steps according to the intense PA category of the SAQ-COPD (Supplementary Table 1).
Internal consistency of the SAQ-COPD total score showed a Cronbach’s alpha of 0.60. Correlations between SAQ-COPD scores and the accelerometer and YPAS ranged from 0.37 to 0.53 (), with the YPAS activity summary index being the strongest. Supplementary Table 2 shows correlations for baseline scores between accelerometer and YPAS reference standards ranging from 0.21 to 0.38, with the greatest association between the YPAS activity summary index and accelerometer METs. Correlations between accelerometer and YPAS were obtained for follow-up scores ranging from 0.24 to 0.36 (Supplementary Table 3).
Table 2 Estimation of Daily PA in the Study Population
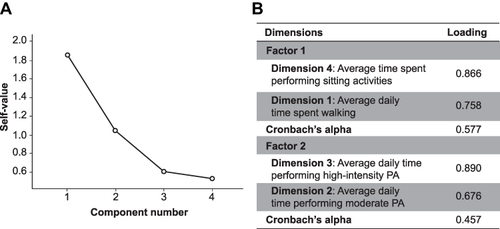
Analysis of construct validity found 2 factors with a cumulative variance explanation exceeding 70% (). Cronbach’s alpha analysis on these two factors did not improve the value of the 4 dimensions taken together. The test-retest reliability for the total score and the different dimensions are shown in .
Table 3 Correlation Between SAQ-COPD and Accelerometer PA Measurements and YPAS
Figure 2 (A) Sedimentation of the SAQ-COPD factorial analysis; (B) factorial analysis of the SAQ-COPD dimensions. Abbreviations: SAQ-COPD, Spanish Activity Questionnaire in COPD.
The mean change in SAQ-COPD total score from baseline to follow-up was 18.6±15.9. Statistically significant differences in SAQ-COPD score change were observed between groups defined by the change in YPAS PA as “stable” (17.0±14.4) and “non-stable” (22.9±18.6); (p = 0.05).
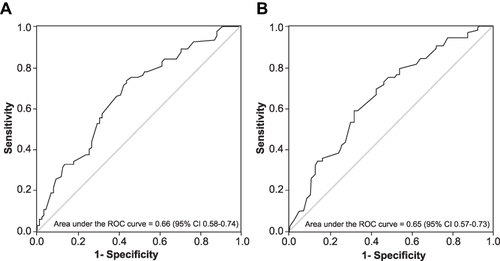
shows that the area under the ROC curve (AUC) between PA according to SAQ-COPD and inactivity according to PAL in the accelerometer was 0.66 (95% CI: 0.58–0.74; p < 0.001). shows that the AUC between PA by SAQ-COPD score and inactivity by steps number was 0.65 (95% CI: 0.57–0.73; p < 0.001). ROC curve identified that having less than 61.5 points on SAQ-COPD classifies the patient as inactive with a specificity of 53.1% (95% CI: 42.7% to 63.4%) and a sensitivity of 72.9% (95% CI: 62.9% to 81.5%) for the threshold established by the number of steps, and a sensitivity of 72.9% (95% CI: 63.5% to81.0%) and a specificity of 56.5% (95% CI: 45.3% to67.2%) for PAL.
Figure 3 ROC curves. Predictive ability of the SAQ-COPD questionnaire to identify physical inactivity with respect to physical activity level or PAL criteria (A) and number of steps (B) provided by the accelerometer.
Supplementary Table 4 shows the conditioning factors reported by “inactive” patients for not performing PA according to the SAQ-COPD. “Shortness of breath” is the symptom that slowed down activity the most, though it accounts for only 17–19% of cases. Leg discomfort, either fatigue or pain, was a limiting factor in 9.2% and 8.5% of patients, respectively. Only the impact of not performing PA on social life and patient dependence positively correlated with their health-related quality of life assessed by CAT, though with Spearman coefficients of 0.31 and 0.34, respectively; p < 0.001 ().
Table 4 Test-Retest Reliability of the SAQ-COPD Questionnaire in Patients with COPD
Table 5 Correlation Between SAQ-COPD and CAT Impact Measure in Patients with Low PA
Discussion
This is the first study to examine the validity of the SAQ-COPD questionnaire to discriminate patients with COPD according to the intensity of their PA and to identify inactive individuals by comparison with the accelerometer and YPAS reference standards. Overall, the results, in a sample of 300 COPD patients, show moderate validity and good sensitivity to change.
Internal consistency of the SAQ-COPD total score was moderate as were correlations between SAQ-COPD score and accelerometer measurements and YPAS. Our findings are similar to those obtained in the validation study of YPAS in COPD patients showing correlations with the accelerometer between 0.30 and 0.48 in somewhat older individuals than our patients.Citation24 The criterion validity correlations obtained for SAQ-COPD are similar to those previously achieved between the questionnaires PASE (Physical Activity Survey for the Elderly) (0.23–0.59), YPAS (0.23–0.61) and CHAMPS (Community Healthy Activities Seniors) (0.26–0.46), with three very different validation measures: activity monitoring, performance tests (EPESE index and 6-minute walk) and other self-reported measures (SF-36) in healthy elderly subjects.Citation25 In this regard, it should be noted that both in our study and those mentioned above, correlations between subjective measures were higher than those seen with objective measures of activity, which reinforces the idea that self-reported PA tends to be overestimated.Citation26
Correlations between YPAS and accelerometer were lower than values observed in the YPAS validation study in COPD.Citation24 However, as in that study, we found the highest correlation coefficient between the activity summary index of the questionnaire and the accelerometer steps, which are the most accepted measurements for each instrument.Citation27 The highest correlation coefficient for SAQ-COPD score was observed for the accelerometer MET rather than for the daily number of steps even though the former has a greater precision for quantifying movement than for estimating energy expenditure. This is particularly well known in populations such as ours, where low-intensity PA is performed (eg, walking slowly).Citation27 Therefore, correlation coefficients could be increased with validity measures that clearly reflect the low-intensity PA.
This study also found no differences in the number of steps, PAL and MET measured by the accelerometer in the different categories of intense PA according to the SAQ-COPD. Although this may be more related to the small number of patients present in some of the categories than to the precision of the accelerometer to quantify PA, it is again shown that self-reported perception and direct measurement may differ. Interestingly, studies categorizing PA by intensity level (low, moderate, or intense) show greater differences between self-reporting and objective measurement in intense category levels.Citation28
To discriminate inactive patients with COPD, the accepted cut-off points for healthy individuals and those with the disease were used.Citation29,Citation30 The analysis showed that the cut-off point with the best diagnostic precision for SAQ-COPD was 61.5. The ROC curve shows that SAQ-COPD discriminates 66.6% of patients with inactive COPD. This value, while not high, could be considered useful in the early identification of inactivity in COPD patients. Sensitivity and specificity indices are moderate, which requires us to consider SAQ-COPD as a tool with a moderate level of precision.
SAQ-COPD questionnaire shows a test-retest reliability of 0.68, a moderate ICC given that in general for reliability to be considered good it should have exceeded 0.75.Citation31 However, in the specific case of the assessment of PA instruments, 0.70 has been suggested as a sufficient cut-off point to consider reliability as acceptable.Citation32,Citation33 Based on this, test-retest reliability for SAQ-COPD total score can be considered acceptable. To date, and since this is the first validation study, we cannot compare this result to previous ICC values for SAQ-COPD, but the test-retest reliability of YPAS (0.59) and CHAMPS (0.64) for detecting sedentary behavior in elderly patients is lower than reported here.Citation34
The observed floor effect would subtract discriminatory capacity from the intense PA dimension but does not invalidate the results. The exploratory factor analysis shows an explanation of 70% of the total variance by two main factors, indicating that the questions of each factor measure internally the same concept. This floor effect of the intense PA dimension was predictable. That is, it was expected that patients would not perform intense PA, but when designing the study, it was considered that a questionnaire designed to assess changes in activity should also contain this item.
Apart from the validation results, it should be noted that mood, external conditioning factors and family obligations had little impact on our patients with COPD when performing PA. These results contrast with previously published data showing behavioral and social factors as ‘conditioning factors’ of PA. In fact, lack of time and motivation, particularly in sedentary patients with COPD, appear to be among the most limiting factors in other populations.Citation35 This could be an explanation for the low correlation that other authors have obtained between PA (“patient can and wants to do it”) and stress tests (“patient can do it”).Citation35 Cultural and lifestyle factors undoubtedly influence these differences.
The results of this study also show that our patients with COPD, mostly with moderate-to-severe airflow limitation, usually perform low-to-moderate intensity PA, which does not necessarily have to be less effective. Indeed, participation in a PA equivalent to walking for at least 2 hours per week has been associated with a 30%–40% reduction in the risk of COPD-related hospital admission and mortality.Citation36 In our study, 77.3% of patients reported walking at least 30 minutes daily and 31.5% met the PA recommendations for adult patients of engaging in moderate activity of ≥30 minutes on at least 5 days per week.Citation37
The weak correlation we found between the impact measure for patients with low-intensity PA according to SAQ-COPD and CAT questionnaires can be explained in part by the impact of the disease shown by patients on their wellbeing and daily life according to the total CAT score.Citation21
SAQ-COPD measures have also demonstrated sensitivity to change after 6 months. This is an important consideration when selecting an instrument to measure the results of a PA intervention.Citation38 Our literature review indicates that SAQ-COPD is the only PA questionnaire specific for patients with COPD that has assessed sensitivity to change.
A limitation of this study is that time in a sedentary lifestyle has been considered as “inactivity” because, although both concepts are strongly correlated, they are different domains with their particularities and determinants,Citation39 so that both may or may not be present in the same individual.Citation39 In fact, 40% of patients spend 21%–42% of the day in sedentary activities - this finding being much lower than reported in healthy adultsCitation40 and other series of COPD patients with similar airflow limitation (62.6%).Citation39 Additionally, this study did not explore the effect that certain covariates, such as biological sex, may have on physical activity. Also, during recruitment of study sample, patients were stratified exclusively by severity of airflow limitation and not by dyspnea, so none of the patients evaluated had mMRC 4 dyspnea, which could limit the generalization of results to the most symptomatic patients. Another potential limitation is having considered the same time in PA for all intensity levels when activity variability is greater in less severe COPD, and activity is mainly limited from GOLD stage II.Citation41 The low representation of patients with mild obstruction in our study is due to their poor representation in clinics, probably because of the existing underdiagnosis and the lack of primary care centers at recruitment. In the interpretation of the results, patient loss over the follow-up in each of the instruments analyzed also cannot be completely disregarded.
Conclusion
The SAQ-COPD questionnaire is an instrument with acceptable psychometric results, good internal consistency, and acceptable predictive validity. It is an easy-to-use tool that could be incorporated into clinical practice in the near future along with validated tools to identify inactive COPD patients and promote healthy interventions. However, future studies and routine administration of the current SAQ-COPD questionnaire in standard clinical practice will help refine the current model.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically review the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and all agree to be accountable for all aspects of the work.
Disclosure
JJ Soler-Cataluña reports receiving funding from GSK, consulting fees from Chiesi, GSK, and Bial, lecture fees from Bial, Chiesi, GSK, Meranini, Boehringer, and AstraZeneca, and attendance at meetings from Chiesi, Boehringer Novartis, and Menarini. L Puente Maestu reports financial support for educational activities from GSK, Chiesi, and lecture fees from Esteve, Novartis, Boehringer, and Sanofi, research grants from Grifols, honoraria for advisory board participation, and committed support in the form of a Menarini grant. M Román Rodríguez reports grants from Astra Zeneca, during the conduct of the study; grants or personal fees from Astra Zeneca, GSK, Boehringer Ingelheim, Cipla, Teva, and Menarini, outside the submitted work. C Esteban, J Gea, R Bernabeu Mora, J Ancochea and E. Pleguezuelos Cobo declare that they have no conflicts of interest. F García-Río reports funding for his institution from GSK, Menarini, Chiesi, lecture fees from Novartis, Chiesi, Esteve, Gebro Pharma, Teva, and fees for advisory board participation from AstraZeneca, Pfizer, Rovi, GSK and Boehringer.
Acknowledgments
The authors are very grateful to all participating patients for making the validation study of the SAQ-COPD questionnaire possible. Medical writing support was provided by Isabel Caballero from Dynamic S.L.U. (Evidenze Clinical Research), funded by AstraZeneca Farmacéutica Spain, S.A.
Additional information
Funding
References
- O’Donnell DE. Increasing physical activity in chronic obstructive pulmonary disease one step at a time. Am J Respir Crit Care Med. 2018;198(8):977–978. doi:10.1164/rccm.201804-0755ED
- Garcia-Rio F, Lores V, Mediano O, et al. Daily physical activity in patients with chronic obstructive pulmonary disease is mainly associated with dynamic hyperinflation. Am J Respir Crit Care Med. 2009;180(6):506–512. doi:10.1164/rccm.200812-1873OC
- Spruit MA, Pitta F, McAuley E, ZuWallack RL, Pulmonary Rehabilitation NL. Physical activity in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2015;192(8):924–933. doi:10.1164/rccm.201505-0929CI
- Vorrink SN, Kort HS, Troosters T, Lammers JW. Level of daily physical activity in individuals with COPD compared with healthy controls. Respir Res. 2011;12:33. doi:10.1186/1465-9921-12-33
- Van Remoortel H, Hornikx M, Demeyer H, et al. Daily physical activity in subjects with newly diagnosed COPD. Thorax. 2013;68(10):962–963. doi:10.1136/thoraxjnl-2013-203534
- Gouzi F, Prefaut C, Abdellaoui A, et al. Evidence of an early physical activity reduction in chronic obstructive pulmonary disease patients. Arch Phys Med Rehabil. 2011;92(10):1611–1617 e2. doi:10.1016/j.apmr.2011.05.012
- Garcia-Rio F, Rojo B, Casitas R, et al. Prognostic value of the objective measurement of daily physical activity in patients with COPD. Chest. 2012;142(2):338–346. doi:10.1378/chest.11-2014
- Gimeno-Santos E, Frei A, Steurer-Stey C, et al. Determinants and outcomes of physical activity in patients with COPD: a systematic review. Thorax. 2014;69(8):731–739. doi:10.1136/thoraxjnl-2013-204763
- Esteban C, Quintana JM, Aburto M, et al. Impact of changes in physical activity on health-related quality of life among patients with COPD. Eur Respir J. 2010;36(2):292–300. doi:10.1183/09031936.00021409
- Dobbels F, de Jong C, Drost E, et al. The PROactive innovative conceptual framework on physical activity. Eur Respir J. 2014;44(5):1223–1233. doi:10.1183/09031936.00004814
- Liao SY, Benzo R, Ries AL, Soler X. Physical activity monitoring in patients with chronic obstructive pulmonary disease. Chronic Obstr Pulm Dis. 2014;1(2):155–165. doi:10.15326/jcopdf.1.2.2014.0131
- Garcia-Aymerich J, Serra I, Gomez FP, et al. Physical activity and clinical and functional status in COPD. Chest. 2009;136(1):62–70. doi:10.1378/chest.08-2532
- Gimeno-Santos E, Raste Y, Demeyer H, et al. The PROactive instruments to measure physical activity in patients with chronic obstructive pulmonary disease. Eur Respir J. 2015;46(4):988–1000. doi:10.1183/09031936.00183014
- Garcia-Aymerich J, Puhan MA, Corriol-Rohou S, et al. Validity and responsiveness of the Daily- and Clinical visit-PROactive Physical Activity in COPD (D-PPAC and C-PPAC) instruments. Thorax. 2021;76(3):228–238. doi:10.1136/thoraxjnl-2020-214554
- Shephard RJ. Limits to the measurement of habitual physical activity by questionnaires. Br J Sports Med. 2003;37(3):197–206; discussion 206. doi:10.1136/bjsm.37.3.197
- Soler-Cataluna JJ, Puente Maestu L, Roman-Rodriguez M, et al. [Creation of the SAQ-COPD questionnaire to determine physical activity in COPD patients in clinical practice] Creacion del cuestionario SAQ-COPD (Spanish Physical Activity Questionnaire in COPD) para la medida de la actividad fisica de pacientes con EPOC en la practica clinica. Arch Bronconeumol. 2018;54(9):467–475. doi:10.1016/j.arbres.2018.01.016
- Vogelmeier CF, Criner GJ, Martinez FJ, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 report. GOLD executive summary. Am J Respir Crit Care Med. 2017;195(5):557–582. doi:10.1164/rccm.201701-0218PP
- Rabinovich RA, Louvaris Z, Raste Y, et al. Validity of physical activity monitors during daily life in patients with COPD. Eur Respir J. 2013;42(5):1205–1215. doi:10.1183/09031936.00134312
- De Abajo S, Larriba R, Marquez S. Validity and reliability of the Yale physical activity survey in Spanish elderly. J Sports Med Phys Fitness. 2001;41(4):479–485.
- Dipietro L, Caspersen CJ, Ostfeld AM, Nadel ER. A survey for assessing physical activity among older adults. Med Sci Sports Exerc. 1993;25(5):628–642. doi:10.1249/00005768-199305000-00016
- Jones PW, Harding G, Berry P, Wiklund I, Chen WH, Kline Leidy N. Development and first validation of the COPD Assessment Test. Eur Respir J. 2009;34(3):648–654. doi:10.1183/09031936.00102509
- Laboratories ATSCoPSfCPF. ATS statement: guidelines for the six-minute walk test. Am J Respir Crit Care Med. 2002;166(1):111–117. doi:10.1164/ajrccm.166.1.at1102
- Medina-Mirapeix F, Valera-Novella E, Morera-Balaguer J, Bernabeu-Mora R. Prognostic value of the five-repetition sit-to-stand test for mortality in people with chronic obstructive pulmonary disease. Ann Phys Rehabil Med. 2021;65(5):101598. doi:10.1016/j.rehab.2021.101598
- Donaire-Gonzalez D, Gimeno-Santos E, Serra I, et al. [Validation of the Yale physical activity survey in chronic obstructive pulmonary disease patients] Validacion del cuestionario de actividad fisica de Yale en pacientes con enfermedad pulmonar obstructiva cronica. Arch Bronconeumol. 2011;47(11):552–560. doi:10.1016/j.arbres.2011.07.002
- Harada ND, Chiu V, King AC, Stewart AL. An evaluation of three self-report physical activity instruments for older adults. Med Sci Sports Exerc. 2001;33(6):962–970. doi:10.1097/00005768-200106000-00016
- Shin KC. Physical activity in chronic obstructive pulmonary disease: clinical impact and risk factors. Korean J Intern Med. 2018;33(1):75–77. doi:10.3904/kjim.2017.387
- Pitta F, Troosters T, Probst VS, Spruit MA, Decramer M, Gosselink R. Quantifying physical activity in daily life with questionnaires and motion sensors in COPD. Eur Respir J. 2006;27(5):1040–1055. doi:10.1183/09031936.06.00064105
- Prince SA, Adamo KB, Hamel ME, Hardt J, Connor Gorber S, Tremblay M. A comparison of direct versus self-report measures for assessing physical activity in adults: a systematic review. Int J Behav Nutr Phys Act. 2008;5:56. doi:10.1186/1479-5868-5-56
- Depew ZS, Novotny PJ, Benzo RP. How many steps are enough to avoid severe physical inactivity in patients with chronic obstructive pulmonary disease? Respirology. 2012;17(6):1026–1027. doi:10.1111/j.1440-1843.2012.02207.x
- Waschki B, Kirsten A, Holz O, et al. Physical activity is the strongest predictor of all-cause mortality in patients with COPD: a prospective cohort study. Chest. 2011;140(2):331–342. doi:10.1378/chest.10-2521
- Koo TK, Li MY. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropr Med. 2016;15(2):155–163. doi:10.1016/j.jcm.2016.02.012
- Forsen L, Loland NW, Vuillemin A, et al. Self-administered physical activity questionnaires for the elderly: a systematic review of measurement properties. Sports Med. 2010;40(7):601–623. doi:10.2165/11531350-000000000-00000
- Terwee CB, Mokkink LB, van Poppel MN, Chinapaw MJ, van Mechelen W, de Vet HC. Qualitative attributes and measurement properties of physical activity questionnaires: a checklist. Sports Med. 2010;40(7):525–537. doi:10.2165/11531370-000000000-00000
- Gennuso KP, Matthews CE, Colbert LH. Reliability and validity of 2 self-report measures to assess sedentary behavior in older adults. J Phys Act Health. 2015;12(5):727–732. doi:10.1123/jpah.2013-0546
- Aguilaniu B, Roche N. The difficulties of measuring and improving physical activity in COPD. NPJ Prim Care Respir Med. 2014;24:14014. doi:10.1038/npjpcrm.2014.14
- Garcia-Aymerich J, Lange P, Benet M, Schnohr P, Anto JM. Regular physical activity reduces hospital admission and mortality in chronic obstructive pulmonary disease: a population based cohort study. Thorax. 2006;61(9):772–778. doi:10.1136/thx.2006.060145
- Nelson ME, Rejeski WJ, Blair SN, et al. Physical activity and public health in older adults: recommendation from the American College of Sports Medicine and the American Heart Association. Med Sci Sports Exerc. 2007;39(8):1435–1445. doi:10.1249/mss.0b013e3180616aa2
- King AC, Rejeski WJ, Buchner DM. Physical activity interventions targeting older adults. A critical review and recommendations. Am J Prev Med. 1998;15(4):316–333. doi:10.1016/s0749-3797(98)00085-3
- Schneider LP, Furlanetto KC, Rodrigues A, Lopes JR, Hernandes NA, Pitta F. Sedentary behaviour and physical inactivity in patients with chronic obstructive pulmonary disease: two sides of the same coin? COPD. 2018;15(5):432–438. doi:10.1080/15412555.2018.1548587
- Owen N, Salmon J, Koohsari MJ, Turrell G, Giles-Corti B. Sedentary behaviour and health: mapping environmental and social contexts to underpin chronic disease prevention. Br J Sports Med. 2014;48(3):174–177. doi:10.1136/bjsports-2013-093107
- Watz H, Waschki B, Meyer T, Magnussen H. Physical activity in patients with COPD. Eur Respir J. 2009;33(2):262–272. doi:10.1183/09031936.00024608