
Abstract
Background
Patients with chronic obstructive pulmonary disease (COPD) are more inclined to have a high level of social vulnerability due to their physical and psychological burden. However, to date, there have been no study on social frailty in patients with COPD. This study aimed to investigate the prevalence, characteristics, and impact of social frailty in patients with COPD.
Methods
Social frailty was assessed using five items in a questionnaire. A patient was diagnosed with social frailty if responses to two or more items were positive. Four hundred and five patients with COPD were assessed for social frailty, dyspnea, and appetite. We also prospectively examined the number of acute exacerbation and unexpected hospitalization for 1 year.
Results
Thirty-six percent of patients with COPD had social frailty. They had reduced appetite and more severe dyspnea [Simplified Nutritional Appetite Questionnaire score: odds ratio (OR) 0.81, 95% confidence interval (CI) 0.69‒0.95, p < 0.01; modified Medical Research Council score: OR 1.42, 95% CI 1.05‒1.93, P = 0.02] than patients without social frailty. Social frailty was not a risk factor for moderate acute exacerbation of COPD but a risk factor for severe acute exacerbation and all-cause unexpected hospitalization (severe acute exacerbation: β, standardized regression coefficient: 0.13, 95% CI 0.01‒0.25, P = 0.04, unexpected hospitalization: β 0.17, 95% CI 0.05‒0.29, P = 0.01).
Conclusion
The prevalence of social frailty is 36%; however, social frailty has a marked clinical impact in patients with COPD.
Introduction
Frailty is a state of vulnerability, in which homeostasis is lost due to exposure to stressors,Citation1 resulting in an increased risk of falls, disability, and mortality.Citation2 The concept of frailty involves physical, psychological, and social domains.Citation3 In the past, predominantly physical frailty has been studied, but recently, social frailty has begun to attract attention, given that low levels of social activity and participation in social roles adversely affect physical functions.Citation4 Similarly, social frailty increases the risk of physical disability and mortality.Citation5,Citation6
Several studies have reported the influence of social factors in patients with chronic obstructive pulmonary disease (COPD). A previous study showed that patients with COPD have low levels of social participation.Citation7 In patients with COPD, low social participation and respiratory function are associated with life satisfaction,Citation8 social support and self-efficacy with overall functioning,Citation9 single marital status with an increased risk of readmission,Citation10 and physical activity with the level of physical activity of their cohabiting loved ones.Citation11 These studies showed that single patients were more likely to have no one to support them in adhering to medication, ensuring physical activity, and healthy eating habitsCitation10 and that the higher the physical activity of people close to them, the higher the physical activity of patients with COPD.Citation11 Based on these backgrounds, it was expected that social factors would have a large impact on patients with COPD.
Social frailty refers to low social activity, low level of social role, and poor social relationships, and is associated with the risk of malnutrition and mortality among the elderly.Citation6,Citation12,Citation13 Social frailty is assessed by combining various factors, such as age, education, marital status, sex, living alone, income, and neighborhood.Citation6 The impact of social frailty on some diseases, such as the increased risk of heart failureCitation14 and osteosarcopenia patients,Citation15 has attracted attention. However, no study on social frailty in patients with COPD have been conducted, and the prevalence and characteristics of patients with COPD with social frailty are unknown. Patients with COPD often have multifaceted impairments, such as decreased physical activityCitation16,Citation17 and psychological burdens, such as anxiety.Citation18,Citation19 Therefore, the prevalence of social frailty may be high in patients with COPD. In addition, socially frail patients with COPD are expected to have an increased risk of acute exacerbation of COPD and unexpected hospitalization due to reduced dietary intake, as well as increased threshold for visiting medical institutions.
The aim of this study was to investigate the prevalence, characteristics, and impact of social frailty on acute exacerbation and unexpected hospitalization in patients with COPD.
Materials and Methods
Study Design and Patients
This was a multicenter, prospective, observational study conducted between January 2018 and February 2021. We recruited patients who regularly visited four facilities in Japan. In this study, outpatients were randomly selected by their attending physicians and agreed to participate in the study. COPD was diagnosed by spirometry (post-bronchodilator FEV1 /FVC < 0.7) according to the Global Initiative for Chronic Obstructive Lung Disease.Citation20 The inclusion criteria were as follows: age ≥40 years and a history of smoking as well as diagnosis of COPD. The physician recorded the patient’s objective findings and the patient completed the questionnaire. Adherence with the study was determined based on patient data and medical records. The following exclusion criteria were also applied: acute exacerbation of COPD within 4 weeks, concomitant respiratory diseases other than COPD, concurrent active malignancy, and inability to read and understand the questionnaires. Patients were excluded for the following reasons: not meeting the inclusion criteria (11 patients), not trackable for 1 year (29 patients), missing data on social frailty (1 patient), complications of interstitial pneumonia (3 patients), active non-tuberculous mycobacteria infection (1 patient), and lung cancer (2 patients).
This study was carried out in accordance with the Declaration of Helsinki guidelines and was approved by the ethics committee of Showa University School of Medicine (approval number: 2453) and by an independent ethics committee. All patients provided informed consent.
Definition of Social Frailty and Its Severity
Social frailty was examined using five questions in the baseline survey, which investigated the following: (1) going out less frequently than in the previous year, (2) not sometimes visiting friends, (3) not feeling helpful to friends or family, (4) living alone, and (5) not talking to someone every day.Citation6 In accordance with a previous study, we defined social robustness as when none of the five issues were present, social prefrailty as when one issue was present, and social frailty as when two or more issues were present.Citation6
Clinical Measurements and Definition of Exacerbation and Hospitalization
Body mass index (BMI) was calculated in kg/m2. Dyspnea was evaluated using the modified Medical Research Council (mMRC) dyspnea scale.Citation21 The total scores range from 0 to 4, and a high score indicates severe dyspnea. Patient health status was assessed using the COPD Assessment Test (CAT) and high score indicates a poor health condition.Citation22 Appetite was measured using the Simplified Nutritional Appetite Questionnaire (SNAQ).Citation23 The possible scores range from 4 to 20, and a low score indicates a poor appetite. Mood disorders were assessed using the Hospital Anxiety and Depression Scale (HADS-Anxiety and HADS-Depression).Citation24 The HADS comprises 14 items divided into two subscales, HADS-Anxiety and HADS-Depression, each of which contains seven items and a higher score means a stronger mental load. Low physical performance was defined as the inability to rise from a chair five times without using the arms.Citation25
Participants were followed up for 1 year to determine whether they had exacerbations. Moderate exacerbation of COPD was defined as an exacerbation requiring the administration of antibiotics and/or systemic steroids, but not hospitalization. Severe exacerbation of COPD was defined as an exacerbation that required hospitalization. Unexpected hospitalization was defined as all-cause hospitalization, per year, excluding scheduled surgery and scheduled hospitalization for examination. The outpatient physician recorded the frequency of exacerbations and unexpected hospitalization based on direct patient interviews, a prescription record book, a diary kept by patients, and a medical record review.
Statistical Analysis
Continuous variables were presented as mean ± standard deviation. One-way analysis of variance, the Kruskal‒Wallis test, and chi-squared tests were used to compare social frailty severity groups (social robust, social prefrailty, and social frailty). The Kruskal‒Wallis test was used to analyze the proportion of social frailty severity by age group. Spearman’s rank correlation analysis was performed to evaluate the associations between the social frailty score and several clinical factors. Logistic regression analysis was performed to identify clinical factors associated with social frailty. Multivariate linear regression analysis was performed to identify factors associated with the number of moderate and severe COPD acute exacerbation and unexpected hospitalization from baseline to 1 year. We did not use p-value to determine variables; rather, we focused on clinical factors to determine the factors to be used in the multivariate analysis.
All statistical tests were two-tailed, and P-values < 0.05 were considered to indicate statistical significance. All statistical analyses were performed using JMP Pro for Macintosh version 16 (SAS Institute, Cary, NC, USA).
Results
Participant Characteristics
Patient characteristics are presented in . Overall, 405 patients with COPD with a mean age of 74.3 ± 8.0 years were enrolled in this study. The mean CAT score and %FEV1 were 14.1 ± 7.8 and 65.1 ± 22.4%, respectively. The prevalence of social robustness, social prefrailty, and social frailty was 122 (30.1%), 134 (33.1%), and 149 (36.8%), respectively. The more severe the social frailty, the older the patient, the worse the CAT, mMRC, SNAQ, HADS-Anxiety, and HADS-Depression scores, the worse the %FEV1, the more difficult it was for the patient to get up from a chair, and the more frequent was the severe acute exacerbation and unexpected hospitalization (P < 0.05).
Table 1 Characteristics of Study Participants According to the Social Frailty Group/Level
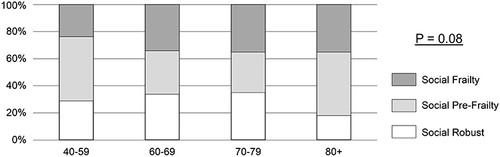
shows the percentage of the severity of social frailty according to age group. The prevalence of social frailty or prefrailty was >60% in all age groups. Although the ratio of the severity of social frailty tended to increase as the age of the group increased, there was no significant difference among groups (P = 0.08).
Figure 1 Prevalence of the severity of social frailty by age group. The prevalence of social frailty or prefrailty was more than 60% in all age groups. There were no significant differences among groups (P = 0.08).
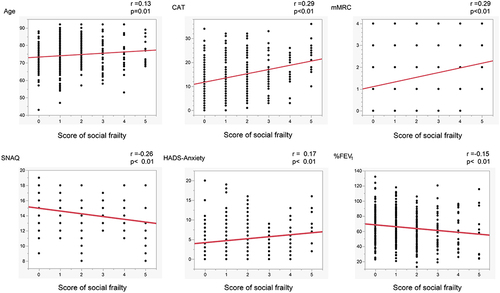
shows the association between social frailty and clinical factors in patients with COPD. Each of the clinical factors had a weak but significant correlation with social frailty (age: r = 0.13, P = 0.01; CAT: r = 0.29, P < 0.01; mMRC: r = 0.29, P < 0.01; SNAQ: r = −0.26, P < 0.01; HADS-Anxiety: r = 0.17; P < 0.01; %FEV1: r = −0.15, P < 0.01).
Figure 2 Relationship between social frailty score and clinical factors in patients with chronic obstructive pulmonary disease. Spearman’s rank correlation was used to test this relationship. The total score of social frailty was significantly correlated with each clinical factor (P < 0.05).
Clinical Characteristics of Patients with Social Frailty
Logistic regression analysis was performed to investigate the characteristics of patients with COPD who had social frailty (). SNAQ and mMRC were significantly associated with social frailty, independently of age, sex, and other clinical factors (SNAQ score: odds ratio [OR], 0.81 [95% confidence interval (CI): 0.69‒0.95], P < 0.01; mMRC score: OR, 1.42 [95% CI: 1.05‒1.93], P = 0.02). Other clinical factors, including age and %FEV1, were not significantly associated with social frailty according to logistic regression analysis.
Table 2 Clinical Characteristics of Patients with Social Frailty
Impact of Social Frailty on Acute Exacerbation and Unexpected Hospitalization
Multivariate linear regression analysis showed that the risk factors for moderate acute exacerbation were CAT and %FEV1 [CAT: β, standardized regression coefficient, 0.24 (95% CI: 0.10 to 0.39), P < 0.01; %FEV1: β, standardized regression coefficient: −0.16 (95% CI: −0.28 to −0.03), P = 0.01], while social frailty was not a risk factor (). Social frailty was a risk factor for severe acute exacerbation [β, standardized regression coefficient: 0.13 (95% CI: 0.00 to 0.25), P = 0.04] (). Similarly, social frailty was also a risk factor for unexpected hospitalization [β, standardized regression coefficient: 0.10 (95% CI: 0.03 to 0.18), P = 0.01], and unable to get up from a chair was also a risk factor for unexpected hospitalization [β, standardized regression coefficient: 0.10 (95% CI: 0.02 to 0.18), P = 0.01]. ().
Table 3 Impact of Social Frailty on Acute Exacerbation and Unexpected Hospitalization in Patients with Chronic Obstructive Pulmonary Disease
Discussion
To the best of our knowledge, this is the first study to evaluate the prevalence and characteristics of social frailty in patients with COPD. This study showed the following important findings in patients with COPD: first, the prevalence of social frailty and social prefrailty is 36.8% and 33.1%, respectively; second, social frailty is associated with a reduced appetite and more severe dyspnea; and third, social frailty is a risk factor for severe acute exacerbation and unexpected hospitalization.
Among patients with COPD in this study, 36.8% and 33.1% had social frailty and social prefrailty, respectively. Considering that the prevalence of social frailty was 10.2‒14.7% in previous studies of older residents in communities in Japan and Korea,Citation6,Citation26,Citation27 which used the same criteria as in this study, patients with COPD seem to have a higher risk of social frailty, in a disease-specific manner. A possible reason for the higher prevalence of social frailty in patients with COPD may be that physical symptoms and mood disorders derived from COPD may reduce social activity, self-affirmation, and the frequency of conversation, leading to social frailty. Previous studies have shown that social vulnerability increases with age;Citation26,Citation28 however, in this study, there was no significant relationship between age group and severity of social frailty in the multivariate analysis. This study showed that even non-older patients with COPD may have social frailty, given that the incidence of social frailty was as high as 23.5%, even in the age group of 40‒59 years.
This study showed that dyspnea was associated with social frailty, which may be related to the decreasing social activity in patients with COPD. This hypothesis is supported by previous studies suggesting that the presence of dyspnea leads to decreased physical activity,Citation29 and that low physical function limits mobility and social activities.Citation30,Citation31 In addition, this study showed that patients with COPD who have social frailty have a reduced appetite. This result is consistent with previous studies that showed that socially isolated older adults may be at a higher risk of dietary inadequacy and poor nutrition.Citation32,Citation33 Eating out is expected to provide nutritional intake as well as social connection.Citation33 Patients with social frailty may have a low appetite because they eat out less frequently due to lack of motivation to go out as well as a lack of friends or partners to visit. The impact of social frailty on patients with COPD is significant, since it was reported that a loss of appetite, leading to nutritional disorders and weight loss, can lead to a worse prognosisCitation34 and increase the risk of acute exacerbationsCitation35 in patients with COPD.
The present study showed that social frailty is a risk factor for severe acute exacerbation and unexpected hospitalization. Acute exacerbation of COPD is important because it induces deterioration of respiratory functionCitation36 and increases the risk of mortality and results in high medical costs.Citation37 While previous studies have shown that social frailty is a risk factor for hospitalization and readmission in the general population,Citation38,Citation39 no previous study has shown that social frailty is a risk factor for unexpected hospitalization in patients with COPD. Patients with social frailty were more likely to live alone and have less social interaction, making it more difficult for them to obtain social support, and placing them at a higher risk of deterioration and of being hospitalized. In addition, physicians may have admitted such patients with social frailty because they consider it a risk to manage the patient in an outpatient setting. A previous study reported that community-dwelling older people with social frailty have high levels of inflammatory cytokines.Citation40 Systemic inflammation is a characteristic finding in patients with COPD and has been reported to exacerbate comorbidities, such as cardiovascular disease, diabetes, and osteoporosis.Citation41 Therefore, higher levels of inflammatory cytokines may have increased the risk of hospitalization in patients with COPD who are socially frail.
We propose that social frailty should be assessed actively in patients with COPD, as social frailty can be improved through appropriate interventions. In fact, community group interventions, including physical exercise and social participation, prevent the development of functional disabilities in older individuals.Citation42,Citation43 It has been reported that various interventions, such as group, individual, and mixed interventions, may be promising tools for addressing social isolation and loneliness.Citation44 Recently, it has been reported that digital interventions may be a new method for reducing loneliness in adults.Citation45 However, the effectiveness of interventions for patients with COPD who are social frail has not been demonstrated to date, and further studies are therefore needed.
This study had several limitations. First, we did not longitudinally assess social frailty, appetite, and dyspnea; thus, we could not assess their causal relationship accurately. Second, all the study participants were secondary- and tertiary-care patients; thus, the findings of this study, particularly the prevalence of social frailty, may not be applicable to primary-care hospitals. Third, we did not measure the level of physical activity, functional aerobic capacity, and other frailty markers of the participants. Therefore, we were unable to analyze their impact on social frailty. We did not evaluate the patients’ economic and geographical factors. However, given that all Japanese citizens are covered by national health insurance and considering the size and location of the participating centers, we did not consider that the patients’ economic or geographic circumstances had a significant impact. Fourth, most participants were males and on average, the participants had moderate levels of COPD in our study. Our results may not be the same in people with severe COPD. However, to the best of our knowledge, this is the first study that has investigated social frailty in patients with COPD. In addition, this study has the strength of not being affected by COVID-19, as it used data from patients who participated until February 2020, considering that the Japanese government announced a state of emergency to prevent the spread of COVID-19 in Japan after April 2020.
Conclusions
In this study, 36% of patients with COPD had social frailty. These individuals had reduced appetite, more severe dyspnea, and were at high risk of severe acute exacerbation and unexpected hospitalization. In patients with COPD, social frailty is markedly prevalent and has a strong clinical impact. The results of this study indicate the importance of investigating the long-term impact of social frailty and the need for intervention trials for social frailty in patients with COPD.
Abbreviations
CAT, COPD assessment test; CI, confidence interval; COPD, chronic obstructive pulmonary disease; FEV1, forced expiratory volume in one second; FVC, forced vital capacity; HADS, Hospital Anxiety and Depression Scale; mMRC, modified Medical Research Council dyspnea scale; OR, odds ratio; SNAQ, Simplified Nutritional Appetite Questionnaire.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
The authors thank all the patients and the team of investigators, who took part in the study. The authors thank Hideki Inoue who collected data on the participants.
Disclosure
KH reports personal fees from AstraZeneca, Boehringer Ingelheim, Kracie Pharma, Ltd., and GlaxoSmithKline outside of the submitted work. AT reports personal fees from AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, KYORIN Pharmaceutical, and Sanofi outside of the submitted work. NO reports personal fees from AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, KYORIN Pharmaceutical, Novartis, and Sanofi outside of the submitted work. TH reports personal fees from AstraZeneca, Boehringer Ingelheim, and GlaxoSmithKline outside of the submitted work. SS reports personal fees from AstraZeneca, GlaxoSmithKline, KYORIN Pharmaceutical, Sanofi, and Tanabe-Mitsubishi outside of the submitted work. HS reports personal fees from AstraZeneca, Boehringer Ingelheim, Kyorin Pharmaceutical, GlaxoSmithKline, Novartis, Kracie Pharma, Ltd., Gilead Sciences, Tsumura and Co, MSD K.K., and Sanofi outside of the submitted work. The authors report no other conflicts of interest in this work.
Additional information
Funding
References
- Clegg A, Young J, Iliffe S, Rikkert MO, Rockwood K. Frailty in elderly people. Lancet. 2013;381(9868):752–762. doi:10.1016/S0140-6736(12)62167-9
- Fried LP, Tangen CM, Walston J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol a Biol Sci Med Sci. 2001;56(3):M146–M156. doi:10.1093/gerona/56.3.M146
- Gobbens RJ, Luijkx KG, Wijnen-Sponselee MT, Schols JM. Toward a conceptual definition of frail community dwelling older people. Nurs Outlook. 2010;58(2):76–86. doi:10.1016/j.outlook.2009.09.005
- Buchman AS, Boyle PA, Wilson RS, et al. Loneliness and the rate of motor decline in old age: the Rush Memory and Aging Project, a community-based cohort study. BMC Geriatr. 2010;10(1):77. doi:10.1186/1471-2318-10-77
- Yamada M, Arai H. Social frailty predicts incident disability and mortality among community-dwelling Japanese older adults. J Am Med Dir Assoc. 2018;19(12):1099–1103. doi:10.1016/j.jamda.2018.09.013
- Makizako H, Shimada H, Tsutsumimoto K, et al. Social frailty in community-dwelling older adults as a risk factor for disability. J Am Med Dir Assoc. 2015;16(11):1003.e7–1003.e1.003E11. doi:10.1016/j.jamda.2015.08.023
- Liu Y, Croft JB, Anderson LA, Wheaton AG, Presley-Cantrell LR, Ford ES. The association of chronic obstructive pulmonary disease, disability, engagement in social activities, and mortality among US adults aged 70 years or older, 1994–2006. Int J Chron Obstruct Pulmon Dis. 2014;9:75–83. doi:10.2147/COPD.S53676
- Lee SH, Lee H, Kim YS, Park HK, Lee MK, Kim KU. Social support is a strong determinant of life satisfaction among older adults with chronic obstructive pulmonary disease. Clin Respir J. 2020;14(2):85–91. doi:10.1111/crj.13104
- Marino P, Sirey JA, Raue PJ, Alexopoulos GS. Impact of social support and self-efficacy on functioning in depressed older adults with chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2008;3(4):713–718. doi:10.2147/COPD.S2840
- Wong AW, Gan WQ, Burns J, Sin DD, van Eeden SF. Acute exacerbation of chronic obstructive pulmonary disease: influence of social factors in determining length of hospital stay and readmission rates. Can Respir J. 2008;15(7):361–364. doi:10.1155/2008/569496
- Mesquita R, Nakken N, Janssen DJA, et al. Activity levels and exercise motivation in patients with COPD and their resident loved ones. Chest. 2017;151(5):1028–1038. doi:10.1016/j.chest.2016.12.021
- Pek K, Chew J, Lim JP, et al. Social frailty is independently associated with mood, nutrition, physical performance, and physical activity: insights from a theory-guided approach. Int J Environ Res Public Health. 2020;17(12):4239. doi:10.3390/ijerph17124239
- Qi X, Li J. The relationship between social frailty and depressive symptoms in the elderly: a scoping review. Int J Environ Res Public Health. 2022;19(24):16683. doi:10.3390/ijerph192416683
- Jujo K, Kagiyama N, Saito K, et al. Impact of social frailty in hospitalized elderly patients with heart failure: a FRAGILE-HF registry subanalysis. J Am Heart Assoc. 2021;10(17):e019954. doi:10.1161/JAHA.120.019954
- Inoue T, Maeda K, Satake S, Matsui Y, Arai H. Osteosarcopenia, the co-existence of osteoporosis and sarcopenia, is associated with social frailty in older adults. Aging Clin Exp Res. 2022;34(3):535–543. doi:10.1007/s40520-021-01968-y
- Garcia-Aymerich J, Serra I, Gómez FP, et al. Physical activity and clinical and functional status in COPD. Chest. 2009;136(1):62–70. doi:10.1378/chest.08-2532
- Ichinose M, Minakata Y, Motegi T, et al. A non-interventional, cross-sectional study to evaluate factors relating to daily step counts and physical activity in Japanese patients with chronic obstructive pulmonary disease: STEP COPD. Int J Chron Obstruct Pulmon Dis. 2020;15:3385–3396. doi:10.2147/COPD.S277782
- Maurer J, Rebbapragada V, Borson S, et al. Anxiety and depression in COPD: current understanding, unanswered questions, and research needs. Chest. 2008;134(4 Suppl):43S–56S. doi:10.1378/chest.08-0342
- Divo M, Cote C, de Torres JP, et al. Comorbidities and risk of mortality in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2012;186(2):155–161. doi:10.1164/rccm.201201-0034OC
- GOLD. Global strategy for the diagnosis, management and prevention of COPD, Global Initiative for Chronic Obstructive Lung Disease (GOLD); 2023. Available from: https://goldcopd.org/wp-content/uploads/2023/03/GOLD-2023-ver-1.3-17Feb2023_WMV.pdf. Accessed April 17, 2023.
- Mahler DA, Ward J, Waterman LA, McCusker C, ZuWallack R, Baird JC. Patient-reported dyspnea in COPD reliability and association with stage of disease. Chest. 2009;136(6):1473–1479. doi:10.1378/chest.09-0934
- Jones PW, Harding G, Berry P, Wiklund I, Chen WH, Kline Leidy N. Development and first validation of the COPD Assessment Test. Eur Respir J. 2009;34(3):648–654. doi:10.1183/09031936.00102509
- Wilson MM, Thomas DR, Rubenstein LZ, et al. Appetite assessment: simple appetite questionnaire predicts weight loss in community-dwelling adults and nursing home residents. Am J Clin Nutr. 2005;82(5):1074–1081. doi:10.1093/ajcn/82.5.1074
- Zigmond AS, Snaith RP. The Hospital Anxiety and Depression Scale. Acta Psychiatr Scand. 1983;67(6):361–370. doi:10.1111/j.1600-0447.1983.tb09716.x
- Ensrud KE, Ewing SK, Taylor BC, et al. Comparison of 2 frailty indexes for prediction of falls, disability, fractures, and death in older women. Arch Intern Med. 2008;168(4):382–389. doi:10.1001/archinternmed.2007.113
- Tsutsumimoto K, Doi T, Makizako H, et al. Association of social frailty with both cognitive and physical deficits among older people. J Am Med Dir Assoc. 2017;18(7):603–607. doi:10.1016/j.jamda.2017.02.004
- Yoo M, Kim S, Kim BS, et al. Moderate hearing loss is related with social frailty in a community-dwelling older adults: the Korean Frailty and Aging Cohort Study (KFACS). Arch Gerontol Geriatr. 2019;83:126–130. doi:10.1016/j.archger.2019.04.004
- Andrew MK, Mitnitski A, Kirkland SA, Rockwood K. The impact of social vulnerability on the survival of the fittest older adults. Age Ageing. 2012;41(2):161–165. doi:10.1093/ageing/afr176
- O’Donnell DE, Milne KM, James MD, de Torres JP, Neder JA. Dyspnea in COPD: new mechanistic insights and management implications. Adv Ther. 2020;37(1):41–60. doi:10.1007/s12325-019-01128-9
- Yi X, Pope Z, Gao Z, et al. Associations between individual and environmental factors and habitual physical activity among older Chinese adults: a social-ecological perspective. J Sport Health Sci. 2016;5(3):315–321. doi:10.1016/j.jshs.2016.06.010
- Nagai K, Tamaki K, Kusunoki H, et al. Physical frailty predicts the development of social frailty: a prospective cohort study. BMC Geriatr. 2020;20(1):403. doi:10.1186/s12877-020-01814-2
- Kalousova L. Social isolation as a risk factor for inadequate diet of older Eastern Europeans. Int J Public Health. 2014;59(5):707–714. doi:10.1007/s00038-014-0582-6
- Huang CH, Okada K, Matsushita E, et al. Sex-specific association between social frailty and diet quality, diet quantity, and nutrition in community-dwelling elderly. Nutrients. 2020;12(9):2845. doi:10.3390/nu12092845
- Celli BR, Cote CG, Marin JM, et al. The body-mass index, airflow obstruction, dyspnea, and exercise capacity index in chronic obstructive pulmonary disease. N Engl J Med. 2004;350(10):1005–1012. doi:10.1056/NEJMoa021322
- Hallin R, Koivisto-Hursti UK, Lindberg E, Janson C. Nutritional status, dietary energy intake and the risk of exacerbations in patients with chronic obstructive pulmonary disease (COPD). Respir Med. 2006;100(3):561–567. doi:10.1016/j.rmed.2005.05.020
- Donaldson GC, Seemungal TA, Bhowmik A, Wedzicha JA. Relationship between exacerbation frequency and lung function decline in chronic obstructive pulmonary disease. Thorax. 2002;57(10):847–852. doi:10.1136/thorax.57.10.847
- Soler-Cataluña JJ, Martínez-García MA, Román Sánchez P, Salcedo E, Navarro M, Ochando R. Severe acute exacerbations and mortality in patients with chronic obstructive pulmonary disease. Thorax. 2005;60(11):925–931. doi:10.1136/thx.2005.040527
- Teo N, Gao Q, Nyunt MSZ, Wee SL, Ng TP. Social frailty and functional disability: findings from the Singapore longitudinal ageing studies. J Am Med Dir Assoc. 2017;18(7):637.e13–637.e19. doi:10.1016/j.jamda.2017.04.015
- Giuli C, Spazzafumo L, Sirolla C, Abbatecola AM, Lattanzio F, Postacchini D. Social isolation risk factors in older hospitalized individuals. Arch Gerontol Geriatr. 2012;55(3):580–585. doi:10.1016/j.archger.2012.01.011
- Nascimento CMC, Zazzetta MS, Gomes GAO, et al. Higher levels of tumor necrosis factor β are associated with frailty in socially vulnerable community-dwelling older adults. BMC Geriatr. 2018;18(1):268. doi:10.1186/s12877-018-0961-6
- Barnes PJ. Inflammatory mechanisms in patients with chronic obstructive pulmonary disease. J Allergy Clin Immunol. 2016;138(1):16–27. doi:10.1016/j.jaci.2016.05.011
- Kanamori S, Kai Y, Aida J, et al. Social participation and the prevention of functional disability in older Japanese: the JAGES cohort study. PLoS One. 2014;9(6):e99638. doi:10.1371/journal.pone.0099638
- Hikichi H, Kondo N, Kondo K, Aida J, Takeda T, Kawachi I. Effect of a community intervention programme promoting social interactions on functional disability prevention for older adults: propensity score matching and instrumental variable analyses, JAGES Taketoyo study. J Epidemiol Community Health. 2015;69(9):905–910. doi:10.1136/jech-2014-205345
- Poscia A, Stojanovic J, La Milia DI, et al. Interventions targeting loneliness and social isolation among the older people: an update systematic review. Exp Gerontol. 2018;102:133–144. doi:10.1016/j.exger.2017.11.017
- Shah SGS, Nogueras D, van Woerden H, Kiparoglou V. Effectiveness of digital technology interventions to reduce loneliness in adults: a protocol for a systematic review and meta-analysis. BMJ Open. 2019;9(9):e032455. doi:10.1136/bmjopen-2019-032455