
Abstract
Background
Chronic obstructive pulmonary disease (COPD) is a major public health problem that remains largely under-diagnosed, mainly due to the under-use of spirometry to establish the diagnosis. The aim of this study is to evaluate the effectiveness of the Moroccan Arabic dialect version of the COPD Assessment Test (CAT) in screening for COPD.
Methods
This was a cross-sectional study carried out in primary care facilities in Morocco, involving participants aged 40 and over. The performance of CAT in detecting cases of COPD was measured with reference to the results of spirometry, considered to be the gold Standard.
Results
A total of 477 participants were included in the study. The prevalence of COPD was 6.7%. Internal consistency of the Moroccan Arabic dialect version of the CAT was high, with a Cronbach’s alpha of 0.89. The total score of the CAT and of each item was significantly higher in subjects with COPD than in those without (P=0.000). Significantly negative correlations were found between CAT total score and FEV1 (r = −0.33, p=0.000), CAT and FVC (r = −0.22, p=0.000), CAT and FEV1/FVC ratio (r = −0.22, p=0.000). The receiver operating characteristic curve showed an area under the curve of 0.93. A CAT score of 10 was the optimal cut-off value for COPD screening, with a sensitivity, specificity, positive predictive value, and negative predictive value of 78.1%, 93.9%, 48.1% and 98.4%, respectively.
Conclusion
The results of the present study showed that the CAT could be used as a screening tool for COPD. The use of this tool by healthcare professionals in primary care settings will improve and promote early diagnosis of this chronic disease.
Background
Chronic obstructive pulmonary disease (COPD) refers to a heterogeneous lung condition characterized by chronic respiratory symptoms (dyspnea, cough, and sputum), resulting from persistent airway and/or alveolar abnormalities, often leading to progressive airflow limitation.Citation1 COPD is a major public health problem responsible for significant economic and social disadvantage.Citation2,Citation3 In 2016, 213 million cases of COPD were recorded worldwide,Citation4 and 3.23 million deaths were expected in 2019 due to COPD.Citation5 Internationally, the prevalence of COPD continues to rise.Citation6 Thus, according to World Health Organization (WHO) projections on mortality and disease burden, COPD will become the third leading cause of death by 2030.Citation7
The diagnosis of COPD relies on the performance of a lung function test called spirometry, considered the gold standard for confirming cases with an obstructive disorder.Citation8 However, the unavailability of spirometers in primary care units limits their use in daily clinical practice.Citation9 This leads to the under-diagnosis of COPD worldwide. Consequently, identifying cases of COPD at an early stage remains a challenge for healthcare systems worldwide.
Several efforts have been made to address the under-diagnosis of COPD. The Global Initiative for Chronic Obstructive Lung Disease (GOLD) regularly updates its guidelines on all aspects of COPD, including diagnosis and screening, to reflect the latest developments and innovations.Citation10 In addition, the World Health Organization (WHO) continues to place non-communicable diseases, including COPD, at the heart of its concerns, encompassing activities ranging from prevention and screening to management.Citation11 In addition, several case-finding tools have been developed to combat the problem of under-utilization of spirometry. These include portable devices such as peak flow meters and microspirometers. In addition, screening questionnaires are considered simple, easy-to-use, and inexpensive case-finding tools for identifying COPD patients.Citation12
To address the problem of under-diagnosis and promote early diagnosis of COPD, we propose to evaluate the use of the COPD Assessment Test (CAT) in COPD case detection. The COPD Assessment Test (CAT) is a short questionnaire originally developed to assess the impact of COPD on the daily lives of sufferers.Citation13 It consists of eight questions covering the symptoms of the disease and their effects on patients’ lives. The CAT questionnaire has been widely used, and its total score has been significantly correlated with validated questionnaires on the impact of COPD on the health status of affected patients.Citation14
In Morocco, COPD is a public health problem, yet it remains largely underdiagnosed.Citation15 Therefore, the aim of this work is to evaluate the effectiveness of the Moroccan Arabic dialect version of the CAT questionnaire in screening for COPD in the population attending primary health care facilities. These facilities are considered to be patients’ first point of contact with the healthcare system in Morocco. Although we have already estimated the prevalence of COPD in people aged 40 and over and identified the risk factors associated with its development in the first part of this research,Citation16 which explains certain similarities between the two studies, it should be noted that this study addresses another facet of our overall research, namely the effectiveness of the CAT tool in screening for cases of COPD in Morocco. With the exception of a single study conducted by Jones et al in which the authors used the CAT questionnaire to measure the impact of COPD on patients in the Middle East and North Africa, including Morocco,Citation17 to our knowledge, no study has yet been conducted in Morocco to investigate the usefulness of the CAT tool in screening for COPD cases based on spirometry results. In fact, a weakness of the study conducted by Jones et al is that it defines COPD cases on the basis of clinical and subjective data (presence of chronic bronchitis or emphysema and/or lifetime smoking exposure of around 10 packs per year), rather than on the basis of spirometry results. The Moroccan dialectal Arabic version of the CAT was obtained by following a rigorous process of translation, back-translation, and reconciliation. The questionnaire was initially translated from English into Moroccan dialectal Arabic by two translators. The two translated versions were compared and synthesized into a single consensus version, which was then back-translated by a third translator to check the faithfulness of the translation to the original. The back-translated version was then compared with the original version of the instrument. The research team then discussed each word of the questionnaire and made the necessary readjustments to ensure the cultural and linguistic appropriateness of the questionnaire.
Materials and Methods
Study Design and Participants
This was a cross-sectional study involving participants aged 40 and over. The study was conducted at primary health care facilities in the province of Settat, Morocco. Participants aged 40 and over were asked to complete a questionnaire (including CAT) and to perform a spirometry test before and after administration of a bronchodilator. Participants aged under 40, with one or more contraindications to spirometry, unable to perform a spirometry test, and those who refused to take part in the study were excluded from the study.
Data Collection
In parallel with the CAT questionnaire, we collected a range of data, including socio-demographic characteristics (such as age, gender, education level, marital status, and place of residence) and tobacco consumption. Smoking status was categorized as never-smokers, former smokers, and current smokers.Citation18 Participants’ weight and height were measured. Body mass index (BMI) was categorized according to the WHO classification.Citation19 The Moroccan dialect Arabic version of the CAT questionnaire can be obtained on reasonable request from the corresponding author.
Pulmonary Function Test
Study participants underwent lung function testing before and after bronchodilator administration, using a spirometer (Spirolab MIR® Model, Rome, Italy). The test was performed in accordance with the recommendations of the American Thoracic Society (ATS) by a single and unique investigator trained for this purpose.Citation20 COPD was defined according to the Global Initiative for Chronic Obstructive Lung Disease (GOLD) diagnostic criteria as a ratio of mean expiratory volume in one second (FEV1) to forced vital capacity (FVC) of less than 0.7.Citation21
Statistical Analysis
Statistical analyses were performed using IBM SPSS (Statistical Package for Social Sciences) version 21 software. Data were expressed as means ± standard deviation for quantitative variables and as percentages (%) for qualitative variables. Data normality was verified using the Shapiro–Wilk test. Depending on the distribution of the variables studied, the Mann-Whitney test was used for comparison between groups. Categorical variables were compared using the Chi-square test. Correlation between the CAT total score and pulmonary function parameters was measured by Spearman correlation coefficient. The internal consistency of the Moroccan Arabic dialect version of the CAT was assessed by calculating Cronbach’s alpha. A Cronbach’s alpha greater than 0.7 indicates good internal consistency of the instrument. The test’s performance in terms of intrinsic values and field performance, namely specificity, sensitivity, negative predictive value, and positive predictive value, were calculated with reference to the results of spirometry, considered the gold standard in confirming cases of COPD. The receiver operating characteristic (ROC) curve was generated to detect the discriminative properties of different CAT score cut-off points in the identification of COPD cases. The area under the curve (AUC) was calculated to determine the diagnostic capacity of the CAT. Values of p<0.05 were considered as statistically significant.
Ethical Considerations
The study was conducted in accordance with the Declaration of Helsinki and was approved by the ethics committee of the Moroccan Association for Research and Ethics (approval number IRB00012973). Informed consent was obtained from each participant at the beginning of the study.
Results
Characteristics of the Study Sample
A total of 477 participants meeting the study inclusion criteria were included in the final analysis. The mean age of the participants was 54.91 ± 11.9 years, and 38.6% were men. COPD was identified in 32 study participants, generating a prevalence of 6.7%. Only three of the study participants (0.6%) had previously undergone spirometry testing. The majority of patients identified as having COPD (93.75%) were not diagnosed. shows the socio-demographic and clinical characteristics of the study sample.
Table 1 Baseline Characteristics of Study Participants (N=477)
Internal Consistency of the CAT
The internal consistency of the Moroccan Arabic dialect version of the CAT is high, with a Cronbach’s alpha of 0.89, indicating good homogeneity between questionnaire items. ()
Table 2 Internal Consistency of the Moroccan Arabic Dialect Version of CAT
CAT Score in Patients with and without COPD
The mean total CAT score was 16.94 ±9.71 in participants with COPD, compared with 3.59 ± 4.21 in those without (p=0.000). A similar trend was observed for the overall scores of each questionnaire item, which were significantly higher in affected participants than in unaffected participants. shows the distribution of the total score and of each CAT item in participants with and without COPD.
Table 3 CAT Results for Participants with and without COPD (N=477)
CAT Score and Pulmonary Function Parameters
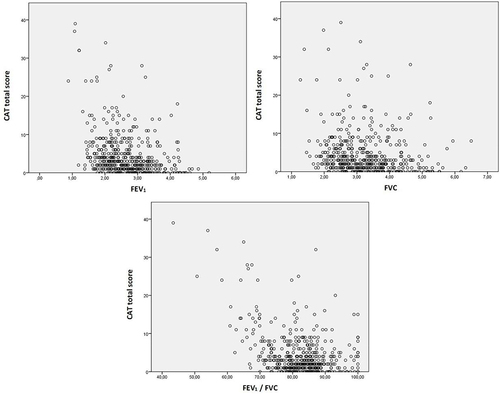
The calculation of Spearman correlation coefficients revealed significantly negative correlations between FEV1, FVC, and FEV1/FVC ratio and the total CAT score. Consequently, an increase in CAT score leads to a significant decrease in pulmonary function parameters ( and ).
Table 4 Correlation Between Total CAT Score and Pulmonary Function Parameters
Figure 1 Correlation between total CAT score and pulmonary function parameters.
CAT Performance in COPD Screening
The receiver operating characteristic (ROC) curve showed an area under the curve (AUC) of 0.93 (95% CI; 0.89–0.97) (p=0.000) ().
Figure 2 Receiver operating characteristic (ROC) curve for the COPD Assessment Test (CAT) in COPD case screening.
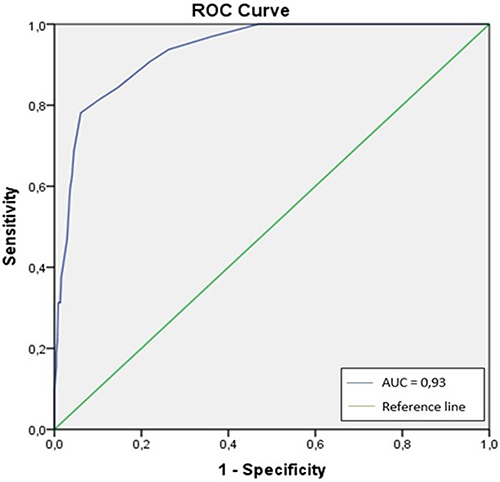
Test performance of CAT in terms of intrinsic values and field performance at each cut-off point is presented in . A CAT score of 10 was the optimal cut-off value for COPD screening, with a sensitivity, specificity, positive predictive value, and negative predictive value of 78.1%, 93.9%, 48.1%, and 98.4%, respectively ().
Table 5 Sensitivity, Specificity, Positive and Negative Predictive Values for the Different CAT Cut-off Points
Discussion
The aim of this study was to evaluate the effectiveness of the Moroccan Arabic dialect version of the CAT questionnaire in screening for COPD. To our knowledge, this is the first evaluation of the diagnostic performance of the CAT in the Moroccan context.
Despite the progress made in terms of the national healthcare system, non-communicable diseases, including COPD, constitute one of the main challenges facing this system.Citation22 Indeed, the rapid economic and demographic transition that Morocco has undergone in recent decades has contributed to an increase in the burden of morbidity and mortality linked to this type of disease.Citation23–25 COPD is a major public health problem in Morocco.Citation15,Citation26,Citation27 Our study revealed a prevalence of 6.7%. This value is lower than that reported by a previous national study, which reported a prevalence of 12.6%.Citation15 This result could be explained by the relatively low proportion of men, smokers, and the elderly, considered to be high-risk groups for developing irreversible airway limitation.
Our results revealed that COPD remains largely underdiagnosed, with an estimated underdiagnosis rate of 93.75%. This finding is similar to the results of other studies, which have all shown extremely high rates of underdiagnosis, mainly due to the underutilization of spirometry.Citation28–30 These data illustrate the importance of seeking alternatives to spirometry to detect cases of COPD and promote early diagnosis of this chronic respiratory pathology, considered as a major public health problem worldwide.Citation31
To address this problem of under-diagnosis, we investigated the ability of the COPD Assessment Test (CAT), originally designed to assess the impact of COPD on the daily lives of sufferers, to screen for cases of COPD. For the record, Jones et al have previously evaluated a classical Arabic version of the CAT to measure the impact of COPD on the daily lives of affected patients in the Middle East and North Africa, including Morocco.Citation17 However, classical Arabic is not commonly used in Morocco, and many people only speak the Moroccan dialect,Citation32,Citation33 hence the need to translate and validate the original version of the CAT in our Moroccan context. The results of this translation work showed good internal consistency of the Moroccan Arabic dialect version of the CAT, with an estimated Cronbach’s alpha of 0.89, testifying to good consistency between its items. The Cronbach’s alpha obtained in our study is similar to that obtained by Jones et al.Citation13
The distribution of mean CAT scores was significantly higher in participants with COPD than in those without. In addition, significantly negative correlations were found between the total CAT score and lung function parameters, namely FEV1, FVC, and FEV1/FVC ratio. Similar results have been documented in the scientific literature,Citation34 indicating that high CAT scores reflect a significant deterioration in lung function.
The receiver operating characteristic (ROC) curve showed an area under the curve (AUC) of 0.93. This result is very encouraging, as it suggests that the test has a high capacity to differentiate between classes. In other words, it is effective in discriminating between positive and negative test results with high precision. According to the ROC curve, a CAT score of 10 was found to be the optimum threshold value for detecting cases of COPD. This threshold value was also found in an earlier study conducted in Japan.Citation35 The intrinsic and field performance values of the Moroccan Arabic dialect version of the CAT were, respectively, 78.1%, 93.9%, 48.1%, and 98.4% for sensitivity, specificity, positive predictive value, and negative predictive value. The low positive predictive value (48.1%) could be explained by the low prevalence of COPD found in our series. However, these results are better than those obtained by Demirci et al in Turkey, who reported a sensitivity, specificity, positive predictive value, and negative predictive value, respectively, of 66.67%, 75.15%, 10.53% and 98.09%.Citation34 Taken together, our results indicate that the Moroccan Arabic dialect version of the CAT shows a very good performance in detecting cases of COPD and could be used as a promising alternative to spirometry. Indeed, health care units are rarely equipped with spirometers.Citation36
It should be noted that lack of awareness may be a barrier to the adoption of the CAT questionnaire, even though it is an inexpensive, easy, and quick to administer case-finding tool. Indeed, a lack of COPD awareness exists among both patients and healthcare professionals. Consequently, raising awareness of COPD among healthcare professionals and the value of using CAT to promote early detection, as well as training in its use and interpretation of its results, are crucial to its successful implementation in Morocco’s primary healthcare facilities, considered the first point of contact between the population and the healthcare system. In addition, effective health communication is essential to raise patients’ awareness of COPD and the value of early detection.Citation37,Citation38
To our knowledge, this is the first study to assess the effectiveness of the CAT in COPD screening in Morocco. The strength of the present study lies in the fact that the performance of the Moroccan Arabic dialect version of the CAT in terms of intrinsic values and field performance was calculated based on the results of spirometry with a reversibility test. This examination is considered the gold standard for confirming cases of COPD. Nevertheless, we did not assess associations between CAT scores and other risk factors such as gender, age, and smoking status. Furthermore, the cultural and linguistic specificity of CAT adaptation could hamper the generalizability of our results. Therefore, similar studies in other settings, particularly where spirometry is underused, are needed in order to generalize the results of this study and reduce the underdiagnosis associated with COPD.
Conclusions
The results of this study highlight the usefulness of the Moroccan Arabic dialect version of the CAT as a high-performance tool for COPD screening. The use of this tool by healthcare professionals in their daily practice could help avoid the need for costly and less available spirometry tests, reduce the rate of under-diagnosis and promote early diagnosis of this chronic pathology, which represents a national public health problem. In addition, efforts to educate and raise awareness of its importance need to be deployed to ensure its implementation and adoption in care units. We plan to establish associations between CAT scores and the following factors: gender, age, and smoking status, using advanced statistical techniques which will enable us to propose an even stronger model for COPD case detection. Similar studies in other settings, particularly where spirometry is under-utilized, are needed to generalize the results of this study and reduce the under-diagnosis of COPD worldwide.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
Additional information
Funding
References
- Celli B, Fabbri L, Criner G, et al. Definition and nomenclature of chronic obstructive pulmonary disease: time for its revision. Am J Respir Crit Care Med. 2022;206(11):1317–1325. doi:10.1164/rccm.202204-0671PP
- Ferrer M, Alonso J, Morera J, et al. Chronic obstructive pulmonary disease stage and health-related quality of life. the quality of life of chronic obstructive pulmonary disease study group. Ann Intern Med. 1997;127(12):1072–1079. doi:10.7326/0003-4819-127-12-199712150-00003
- Iheanacho I, Zhang S, King D, et al. Economic burden of Chronic Obstructive Pulmonary Disease (COPD): a systematic literature review. Int J Chron Obstruct Pulmon Dis. 2020;15:439–460. doi:10.2147/COPD.S234942
- López-Campos JL, Tan W, Soriano JB. Global burden of COPD. Respirology. 2016;21(1):14–23. doi:10.1111/resp.12660
- Chronic obstructive pulmonary disease. Available from: https://www.who.int/news-room/fact-sheets/detail/chronic-obstructive-pulmonary-disease-(copd). Accessed July 03, 2024.
- Varmaghani M, Dehghani M, Heidari E, et al. Global prevalence of chronic obstructive pulmonary disease: systematic review and meta-analysis. East Mediterr Health J. 2019;25(1):47–57. doi:10.26719/emhj.18.014
- Mathers CD, Loncar D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med. 2006;3(11):e442. doi:10.1371/journal.pmed.0030442
- Wheatley JR. Spirometry: key to the diagnosis of respiratory disorders. Med J Aust. 2017;207(10):422–423. doi:10.5694/mja17.00684
- Heffler E, Crimi C, Mancuso S, et al. Misdiagnosis of asthma and COPD and underuse of spirometry in primary care unselected patients. Respir Med. 2018;142:48–52. doi:10.1016/j.rmed.2018.07.015
- Sharma M, Joshi S, Banjade P, et al. Global initiative for chronic obstructive lung disease (GOLD) 2023 guidelines reviewed. Open Respir Med J. 2024;18:e18743064279064. doi:10.2174/0118743064279064231227070344
- Global action plan for the prevention and control of noncommunicable diseases 2013–2020. Available from: https://www.who.int/publications/i/item/9789241506236. Accessed July 03, 2024.
- Lin CH, Cheng SL, Chen CZ, et al. Current progress of COPD early detection: key points and novel strategies. Int J Chron Obstruct Pulmon Dis. 2023;18:1511–1524. doi:10.2147/COPD.S413969
- Jones PW, Harding G, Berry P, et al. Development and first validation of the COPD assessment test. Eur Respir J. 2009;34(3):648–654. doi:10.1183/09031936.00102509
- Jones PW, Brusselle G, Dal negro RW, et al. Properties of the COPD assessment test in a cross-sectional European study. Eur Respir J. 2011;38(1):29–35. doi:10.1183/09031936.00177210
- El Rhazi K, Nejjari C, BenJelloun MC, et al. Prevalence of chronic obstructive pulmonary disease in Fez, Morocco: results from the BOLD study. Int J Tuberc Lung Dis. 2016;20(1):136–141. doi:10.5588/ijtld.15.0029
- Al Wachami N, Arraji M, Iderdar Y, et al. Prevalence and risk factors of chronic obstructive pulmonary disease among users of primary health care facilities in Morocco. Int J Chron Obstruct Pulmon Dis. 2024;19:375–387. doi:10.2147/COPD.S443081
- Jones PW, Shahrour N, Nejjari C, et al. Psychometric evaluation of the COPD assessment test: data from the BREATHE study in the Middle East and North Africa region. Respir Med. 2012;106(2):S86–99. doi:10.1016/S0954-6111(12)70017-3
- Laraqui O, Hammouda R, Laraqui S, et al. Prevalence of chronic obstructive respiratory diseases amongst fishermen. Int Marit Health. 2018;69(1):13–21. doi:10.5603/IMH.2018.0003
- World Health Organization. Waist Circumference and Waist-to-Hip Ratio: Report of a WHO Expert Consultation, Geneva, December 8-11, 2008. Geneva: World Health Organization; 2011.
- Miller M, Hankinson J, Brusasco V, et al. Standardization of Spirometry, 1994 Update. American thoracic society. Am J Respir Crit Care Med. 1995;152(3):1107–1136. doi:10.1164/ajrccm.152.3.7663792
- Vogelmeier CF, Criner GJ, Martinez FJ, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 Report: GOLD executive summary. Eur Respir J. 2017;49(3):1700214. doi:10.1183/13993003.00214-2017
- Mahdaoui M, Kissani N. Morocco’s healthcare system: achievements, challenges, and Perspectives. Cureus. 2023;15(6):e41143. doi:10.7759/cureus.41143
- Ministry of Health Morocco. National survey of noncommunicable diseases risk factors 2017–2018. Available from: https://www.sante.gov.ma/Documents/2019/05/Rapport%20de%20l%20enqu%C3%AAte%20Stepwise.pdf. Accessed July 03, 2024.
- World Bank. World Development Indicators. Washington D.C: World Bank; 2015.
- Haut Commissariat au Plan. Recensement général de la population et de l’habitat. [General Census of Population and Housing]. Présentation des principaux résultats; 2015. French. Available from: http://www.hcp.ma. Accessed July 03, 2024.
- Benslimane A, Garcia-Larsen V, El Kinany K, et al. Association between obesity and chronic obstructive pulmonary disease in Moroccan adults: evidence from the BOLD study. SAGE Open Med. 2021;9:20503121211031428. doi:10.1177/20503121211031428
- Benmaamar S, Es-Sabbahi B, Taghyioullah Haiba M, et al. Economic burden of chronic obstructive pulmonary disease in Morocco: a cost of illness study. Monaldi Arch Chest Dis. 2024. doi:10.4081/monaldi.2024.2745
- Kaplan A, Thomas M. Screening for COPD: the gap between logic and evidence. Eur Respir Rev. 2017;26(143):160113. doi:10.1183/16000617.0113-2016
- Lamprecht B, Soriano JB, Studnicka M, et al. Determinants of underdiagnosis of COPD in national and international surveys. Chest. 2015;148(4):971–985. doi:10.1378/chest.14-2535
- Hill K, Goldstein RS, Guyatt GH, et al. Prevalence and underdiagnosis of chronic obstructive pulmonary disease among patients at risk in primary care. CMAJ. 2010;182(7):673–678. doi:10.1503/cmaj.091784
- Z ZP, Ji YX, Zhang XJ, et al. Distributions and trends of the global burden of COPD attributable to risk factors by SDI, age, and sex from 1990 to 2019: a systematic analysis of GBD 2019 data. Respir Res. 2022;23(1):90. doi:10.1186/s12931-022-02011-y
- Iddins A. Debating Darija: telquel and language politics in modern Morocco. Med Cult Society. 2015;37(2):288–301. doi:10.1177/0163443714560133
- Belghiti N. “Chapitre 10: le paysage linguistique au Maroc entre politiques publiques et réalité sociale in Re-penser les politiques linguistiques en Afrique à l’ère de la mondialisation [Chapter 10: The Linguistic Landscape in Morocco Between Public Policies and Social Reality in Re-penser les politiques linguistiques en Afrique à l’ère de la mondialisation]. Observatoire européen du plurilinguisme. Plurilinguisme. 2023;2023:259–278. doi:10.3917/oep.bigir.2023.01.0259
- Demirci H, Eniste K, Basaran EO, et al. A multicenter family practitioners’ research on chronic obstructive pulmonary disease screening using the COPD assessment test. Prim Health Care Res Dev. 2017;18(6):603–607. doi:10.1017/S1463423617000408
- Yoshimoto D, Nakano Y, Onishi K, et al. The relationship between the COPD Assessment Test score and airflow limitation in Japan in patients aged over 40 years with a smoking history. Int J Chron Obstruct Pulmon Dis. 2014;9:1357–1363. doi:10.2147/COPD.S61265
- Plum C, Stolbrink M, Zurba L, et al. Availability of diagnostic services and essential medicines for non-communicable respiratory diseases in African countries. Int J Tuberc Lung Dis. 2021;25(2):120–125. doi:10.5588/ijtld.20.0762
- Nicely Aken S. Health communication: from theory to practice. J Med Libr Assoc. 2008;96(1):72–73. doi:10.3163/1536-5050.96.1.72
- Rimal RN, Lapinski MK. Why health communication is important in public health. Bull World Health Organ. 2009;87(4):247–247a. doi:10.2471/blt.08.056713