
Abstract
Objectives
Exacerbations of chronic obstructive pulmonary disease (COPD) are the third largest cause of emergency hospital admissions in the UK. This systematic literature review explored the relationship between the hospitalization rates and the COPD comorbidities, anxiety, and depression.
Methods
The Centre for Research Dissemination’s framework for systematic reviews was followed using search terms relating to COPD, anxiety, depression, and hospital admission. Papers identified were assessed for relevance and quality, using a suitable Critical Appraisal Skills Programme tool and Mixed Methods Assessment Tool.
Results
Twenty quantitative studies indicated that anxiety and depression led to a statistically significant increase in the likelihood of COPD patients being hospitalized. These comorbidities also led to an increased length of stay and a greater risk of mortality postdischarge. Other significant factors included lower Body-Mass Index, Airflow Obstruction, Dyspnea, and Exercise scores, female gender, lower socioeconomic status, poorer patient perceived quality of life, increased severity of lung function, and less improvement in dyspnea from admission to discharge. It was also highlighted that only 27%–33% of those with depression were being treated for it. Four qualitative studies revealed that patients saw anxiety and depression as a major factor that affected their ability to cope with and self-manage their condition.
Implications
Findings from the systematic review have highlighted a need for better recognition and treatment of anxiety and depression amongst individuals with COPD. Ongoing research will develop and test strategies for promoting better management and self-management as a means of reducing hospital admissions.
Background
Chronic obstructive pulmonary disease (COPD) is a major cause of chronic morbidity and mortality worldwide. The 2002 World Health ReportCitation1 listed COPD as the fifth leading cause of death in the world. Further increases in its prevalence and mortality are expected to make it the third leading cause of mortality by 2015.Citation2,Citation3 COPD is a complex disease, triggered mostly by exposure to cigarette smoking. It leads not only to pulmonary damage but also to systemic impairment. There is also a growing awareness of systemic inflammation, cardiovascular, neurologic, psychiatric, and endocrine morbidities that are common comorbidities of the condition and have a long-term detrimental effect on the morbidity and mortality of COPD patients.Citation4,Citation5
COPD has a major effect on the lives of the sufferers, particularly in terms of impaired exercise performance and functional capacity. The presence of daily symptoms and a high exacerbation frequency are other important factors.Citation6 COPD also accounts for many visits to health care professionals in the UK. General practitioner consultations for COPD in one year range from 4.17 per 1,000 consultations in people aged 45–64 years to 8.86 per 1,000 in 65–74 years to 10.32 per 1,000 in 75–84 year olds.Citation7–Citation9 These rates are four times those for the chest pain caused by ischemic heart disease. Exacerbations are also an important cause of hospitalization and are responsible for about 10% of all acute medical admissions.Citation10,Citation11 They are also the second largest cause of unplanned hospital admissionsCitation12 and strongly influence the health-related quality of life for the sufferer.Citation5,Citation13–Citation15
Donaldson et alCitation16 demonstrated that the frequency of the occurrence of the acute exacerbations contributed to long-term decline in lung function in COPD. They showed that patients with COPD who suffered frequent exacerbations experienced a significantly greater decline in forced expiratory volume in 1 second (FEV1) than patients who had infrequent exacerbations. Exacerbations are more common than previously believed (2.5–3 per year [mean]).Citation13 Also, following an exacerbation, the incomplete recovery of lung function after the event means that the patient may not regain his or her stable lung function, which may contribute to a decline in lung function with time, which is characteristic of COPD.Citation14–Citation16 These findings emphasize the importance of targeting COPD exacerbations to reduce disease progression and, particularly, to detect patients who are frequent exacerbators and the underlying factors that contribute to these exacerbations.
Anxiety and depression are common comorbidities of COPD.Citation17–Citation19 The literature also suggests that there may be a relationship between these comorbidities and the exacerbations of COPD.Citation20 This literature is not, however, conclusiveCitation21,Citation22 due to: different tools being used to measure anxiety and depression; studies being conducted in different countries that have noncomparable health services; and some studies that include asthmatics, as well as people with COPD. Untreated or incompletely treated depression and anxiety may also have major implications for compliance with medical treatment, due to the effects on cognitive functioning and the decreased effectiveness of any self-management activities that the person may instigate.Citation23–Citation25 The way in which anxiety and depression may be associated with COPD exacerbations may also have a relationship with this issue of ineffective coping and self-management strategies adopted by the patients. Depression may also be a significant predictor of mortality following hospitalization for acute exacerbation.Citation26
Aim and objectives
In this paper, we wanted to examine critically the relationship between anxiety/depression and the exacerbations of COPD that result in hospital admission and readmissions and to investigate whether there are other mediating factors involved.
Objectives
Our objectives were: 1) to clarify the evidence base available regarding the relationship between anxiety/depression and the exacerbations of COPD that lead to hospital admissions and readmissions; and 2) to identify any other factors that might lead to the hospitalization following an exacerbation of COPD patients with the comorbidities of anxiety and depression. These other factors may also include the ability to cope and to self-manage their condition, as well as other comorbidities and social factors.
Materials and methods
A systematic review of the literature was carried out following the University of York’s Centre for Reviews and Dissemination’s (CRD) guidance.Citation27 The review question was framed in terms of population, investigation, outcome, and study design (PIOS), with the population being anyone with COPD – any age, any gender, and any severity. The conclusion of the investigation was that these people had the comorbidities of anxiety and/or depression, and the outcome was admission to the hospital for the exacerbation of COPD.
The study design for the research studies sourced was not specified and not restricted by date or place where the study was carried out; this was done so as not to restrict the review. The inclusion criteria for the review were studies relating to having COPD and the comorbidities of anxiety and depression and patients being admitted to the hospital with an acute exacerbation of COPD.
Initially, the Cochrane Review database was searched to ensure that a similar review had not already been carried out nor was it in the process of being conducted. Electronic databases were then searched to elicit literature relevant to the review question set. These electronic databases included PubMed/Medline, Cumulative Index to Nursing and Allied Health Literature, Embase, Web of Science, and PsycINFO. The search terms were broken down in terms of PIOS and outlined in .
Table 1 Search terms used in the electronic database search
Following the searches of these individual areas that used OR to combine all the terms, the population search terms were then combined with the outcome search terms with OR; they were then further combined with the intervention search terms, using the search words “anxiety” and “depression” separately – combining with AND for the final outcome of the searching.
Other potential research papers were identified from the reference lists of the articles read in full text for the final review. Abstracts from relevant conferences that were identified by the database searches were also reviewed, and authors were contacted for further information on relevant abstracts. This extra clarification and checking process has been identified by the CRDCitation27 as good practice to ensure a complete inclusion of relevant data.
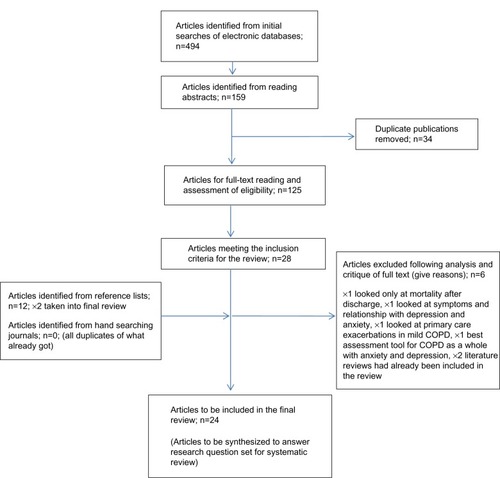
The selection of the studies retrieved from the electronic searching was done in distinct stages. Initially, all duplications were removed. Then, the titles and abstracts were reviewed against the inclusion criteria for the review. Remaining articles were then screened by reading the full text, which then left the remaining articles to be reviewed in a final review (). Two researchers reviewed the full-text articles to decide on the final articles to be included. A third reviewer was available to resolve any disagreements that occurred in this process. This peer review was also carried out during the data extraction stage of the review.
Figure 1 Flow chart of study selection process.
The systematic review of the literature was carried out May 2012–September 2012. It should be stressed however that although the last search was run at the end of September 2012, an alert system was set up on the electronic search databases to highlight any new research being published that may have had relevance to the search area topic. When this paper was submitted for publication, no further research publications had been identified that addressed the question set in this systematic review.
Data extraction was carried out using the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelinesCitation28 for the individual study designs that were included in the final review. The methodology of the articles was reviewed using the appropriate Critical Appraisal Skills Programme tool for critique of literature.Citation29
During the data-extraction stage of the review, quality checks were carried out on each individual study to be included in the final systematic review. For this process, the Mixed Methods Appraisal Tool version 2011 (MMAT, Department of Family Medicine, McGill University, Montreal, QC, Canada) was used.Citation30
The MMAT has been designed for the appraisal stage of complex systematic literature reviews that include qualitative, quantitative, and mixed methods studies. The MMAT permits the reviewer to appraise concomitantly and describe the methodological quality for the three methodology domains: mixed, qualitative, and quantitative; subdivided into three sub domains; and randomized controlled trials, nonrandomized, and descriptive. The MMAT allows the appraisal of most common types of study methodology and design; different sections of the tools are used for the appraisal of the different study types. For each relevant study selected for a systematic mixed studies review, the methodological quality can then be described using the corresponding criteria. The MMAT has been designed to appraise the methodological quality of the studies retained for a systematic mixed studies review, not the quality of their reporting (writing). This distinction is important – as good research may not be well-reported.
The scoring metrics for the MMAT can be presented as *, **, ***, or ****, where the * represents the number of criteria met, divided by 4. This becomes: the single * represents 25%; the **, 50%; the ***, 75%; and the ****, 100%, and represents top quality.
Due to the heterogeneity of the final articles included in the review, the methodology chosen for the synthesis of the findings was via narrative synthesis, using the guidance developed by Popay et alCitation31 to provide some structure and transparency of the results generated.
Method of synthesis
“Narrative synthesis” refers to an approach to the systematic review – the synthesis of findings from multiple studies that relies primarily on the use of words and text to summarize and explain the findings of the synthesis.Citation31
The narrative synthesis guidanceCitation31 identifies four elements of the process of narrative synthesis: 1) developing a theory of how the intervention works, why, and for whom; 2) developing a preliminary synthesis; 3) exploring the relationships within and between the studies; and 4) assessing the robustness of the synthesis.
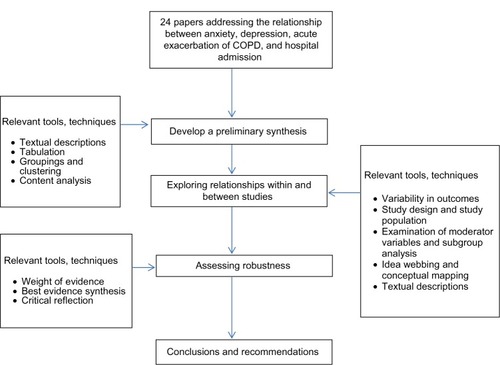
For each element of the synthesis process, the guidance describes a number of useful tools and techniques. The choice of specific tools and techniques at each point in the process will depend on the type of data being synthesized. Only the tools and techniques actually used in this synthesis are described in this article. illustrates the synthesis process.
Figure 2 Synthesis process used in the review of the literature.
Results
Theoretical development
COPD exacerbations are best defined as the worsening of respiratory symptoms.Citation14 More strategies to reduce exacerbation frequency urgently need to be delivered and evaluated. Clinicians will be in a better position to reduce the morbidity associated with COPD exacerbations significantly and – at last – improve the quality of life for our patients with this debilitating condition. Hence, it is important to understand the relationship between the comorbid conditions of anxiety and depression and the acute COPD exacerbations that result in hospital admissions. Theories can then be developed to postulate on such a relationship and other mediating factors involved, but the facts cannot be unveiled without undertaking this systematic review and conducting a thorough and systematic synthesis of the findings. Only then will the nature of this relationship and, indeed, if other factors are involved, be discovered.
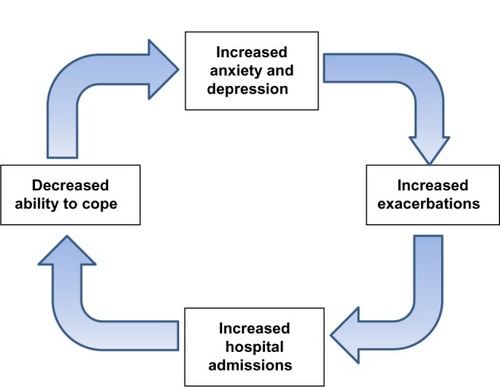
illustrates the theoretical relationship between anxiety and depression and the acute exacerbations of COPD that result in admission or readmission to the hospital.
Figure 3 Diagrammatic representation of the theoretical relationship between anxiety and depression and acute exacerbations of COPD that result in hospital admissions or readmission.
Preliminary synthesis
The guidance suggests that the way in which a reviewer approaches the preliminary synthesis will depend – in part – on whether the evidence to be synthesized is qualitative, quantitative, or both.Citation31 In this synthesis, the data to be synthesized is predominantly quantitative from the methodologies of cohort and case control/series nature, amounting to 20 studies.
There were also three qualitative studies and one mixed-method study. With this in mind, the tools utilized in this preliminary synthesis are textual description, tabulation of data, groupings, and clusters.
The purpose of this preliminary synthesis is to deliver an initial description of the results of the individual studies included in the systematic review, which relate to the primary research question asked at the start of the systematic review. Through this, the reviewer will begin to construct an explanation of how and why a particular factor had the relationships reported, of how and why particular factors impinged in situations, and to test the robustness of the results of the synthesis.
Tabulation of data was considered the most natural starting point for the synthesis while extracting data from the included studies during the review process. This is shown in , which provides a summary of all the studies included in the systematic review.
Table 2 Data extraction table of all articles included in the systematic review
It is apparent from that the majority of the studies directly supported the notion that there was a positive relationship between anxiety and depression and the resultant admissions or readmissions to the hospital for an acute exacerbation of COPD. Findings also highlighted other mediating factors that were involved in this relationship. These included: perceived quality of life; severity of disease; female sex; lower body-mass index, airflow obstruction, dyspnea, and exercise (BODE) scores (an index of COPD mortality; the lower the score, the more chance of death from COPD); low socioeconomic status; persistent smoking; long-term oxygen therapy (LTOT); decreased self-efficacy and compliance; increased dyspnea; a sense of loss; and an inability to cope and previous admissions for acute exacerbation of COPD.
Another important factor demonstrated by the results in was the heterogeneity of the studies, in terms of populations, country of origin, sample sizes, statistical tests applied, and outcomes. The data extraction table () was examined in more depth to determine the presence of dominant groups or clusters of characteristics, by which the subsequent synthesis could be organized. These groupings incorporated study methodology, populations under study and settings, factors under investigation, and outcomes recorded. was organized into the different methodologies. From this, it was apparent that in studies of the same basic methodology, different factors were included in the models under investigation. Some used the measurement of depression and anxiety; some used one of these conditions alone. There was also variation in the tools used to measure these factors.
In addition, some studies used depression and anxiety as secondary outcome measures, with the quality of life and BODE scores as the primary outcome measures under investigation. The end results, though, still yielded information that could contribute to the answering of the research question set at the start of the systematic review.
From comparing and cross reading the included studies in the final systematic review, there is evidence that the comorbidities of depression and anxiety do have a significant relationship with higher rates of admissions and readmissions for the acute exacerbation of COPD.Citation26,Citation32–Citation44 This was found in 17 of the final 24 (71%) studies.
Other areas shown from the included studies were that the presence of the comorbidities of depression and anxiety meant that once admitted, patients had longer lengths of stay in the hospitalCitation48 and a greater risk of mortality postdischarge.Citation20,Citation26,Citation32,Citation41
Mediating factors observed to be significant in this relationship between the comorbidities of anxiety, depression, and the acute exacerbation of COPD included: lower BODE scores;Citation19,Citation32,Citation33 perceived quality of life, which also had a direct correlation with worsening depression and increased risk of exacerbations;Citation19 lower socioeconomic status;Citation37 increased severity of anxiety; female sex;Citation19,Citation34,Citation44,Citation45 increasing rate of decline in lung function;Citation36 less improvement in dyspnea; increased partial pressure of carbon dioxide (PaCO2); decreased partial pressure of oxygen (PaO2); and increased pH from admissions to discharge.Citation34,Citation43,Citation46
It was also highlighted that only 27%–33% of patients with depression and COPD were being treated with antidepressant medication, which suggests the underdiagnosis and undertreatment of depression in the COPD population.Citation41 This proposition – that depression is underdiagnosedCitation41 – is also supported by the findings of Fan et al,Citation47 who stated that although there is a high prevalence of depression in COPD patients, only 33% receive any medication for it. There was no data relating to nonpharmacological-management techniques.
Analysis for the qualitative studies, which examined patients’ perceptions and subjective experiences, suggested that anxiety should be seen as an important issue for COPD patients. Anxiety might provide an important indicator of actual illness severity and assist clinicians in determining the support and care that these people require.Citation48 It is essential, then, that anxiety is recognized as an important sign but not necessarily the cause of dyspnea for patients with COPD in acute exacerbation. It was also highlighted that depression is significantly related to decreased quality of life, which – in turn – can lead to decreased compliance, resulting in an increased incidence of exacerbations and the associated risk of mortality on discharge following the exacerbations.Citation41 The relationship between depression and lower levels of quality of life was also highlighted by Coventry et al,Citation37 Gudmundsson et al,Citation19 Ng et al,Citation45 and Xu et al.Citation44
An examination of the patients’ perceptions and experiences in the qualitative and mixed methods studies showed that they felt a real sense of loss of control over their health, which led to an increased dependence and loss of autonomy.Citation52 These consequences imposed on the patients also triggered an increase in depression and a resultant decrease in the quality of life.Citation39 Their ability to cope was compromised, which again, led to increased levels of anxiety and depression.Citation39 These perceptions and experiences were also confounded by the perceived lack of information and guidance given to patients postdischarge, which led to increased levels of anxiety.Citation39
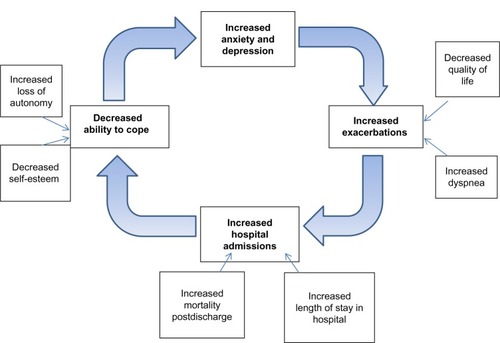
It can be seen from this synthesis of the data that the relationship of anxiety and depression to the acute exacerbation of COPD is significant, but it is also complex, multifaceted, and concerns many interrelated factors. These factors build on the preliminary theoretical model shown in ; the expanded theoretical perspective of this relationship is shown in .
Figure 4 Idea webbing of factors involved in the relationship of anxiety and depression and the acute exacerbation of COPD.
It is important to point out that there were two studies which reported that anxiety and depression were not significant factors in the relationship between the exacerbations and the hospital admissions. These two studies were by Soler et alCitation50 and Chen and Narsavage.Citation51 On closer examination of these two studies, the study by Chen and NarsavageCitation51 was carried out in rural Taiwan. It was acknowledged within the paper itself that rural and cultural subgroups may have different perceptions of their condition, especially of having depression, which is regarded quite negatively by some cultures. This may have affected the perceptions and feedback from the participants about their condition when interviewed and even how they presented to the hospital, as some cultures would suffer at home rather than go to the hospital. It was also noted that the participants would access different hospitals in a wide area, which could make the collection of quality data difficult to achieve.
The study by Soler et alCitation50 only examined anxiety and – although it showed itself to be a significant factor in the relationship under question – depression was excluded. Very often, however, these two conditions were present together in the person. They highlighted that significant factors were the use of inhaled salmeterol (a long-acting bronchodilator inhaler medication) and, also, cardiac arrhythmias.
On a closer examination of the study group characteristics, the majority of participants were on salmeterol at the start of the study, which was not the case in the other studies included in the review. Also, the study group only consisted of people with severe COPD, in which cardiac arrhythmias are commonly found as a comorbidity. It is not surprising, therefore, that both of these factors had a higher chance of showing themselves to be significant. Although these findings are relevant if relating the findings to only people with severe COPD, this review is considering the relation of anxiety and depression to acute exacerbations and resultant hospital admissions and readmissions to the general COPD population, which the other studies in the review consider.
This model () builds on the original theory of the relationship between anxiety and depression and the exacerbations of COPD. The additional variables are those discovered from the systematic review of the literature, and they enhance the preliminary theoretical model further in the quest to gain a deeper understanding of the relationship under review.
Finally, during the process of data extraction, quality checks on the methodology of all the included articles in the review were carried out using the MMAT version 2011.Citation30 Quality appraisal of all the included studies in this systematic review showed that 16 of 24 (66% or two-thirds) had a **** rating. Therefore, they met 100% of the quality criteria, and eight (33% or one-third) had a quality rating of ***. Therefore, they met 75% of the quality criteria used, a number that was still symbolic of high-quality studies. The reasons for the drop in the star rating to three stars were: because there was no information about the missing data or the dropout rate of the participants (n=6); invalid tools were used to measure the outcomes (n=1); and there was no consideration of how the researcher involved in the study influenced the participants (n=1). Overall, the quality of the included studies in this systematic review was of high, if not good, quality – meeting between 75%–100% of the quality criteria in the MMAT evaluation tool.
Reflecting critically on the process of narrative synthesis
The synthesis of mixed study results does not have the rigorous techniques and tools that are available to meta analysis. This is not to say that the quality of the content and results of the systematic review are any less valuable. The question that was originally identified lent itself to both qualitative and quantitative study results; this is why the inclusion criteria were kept wide.
The problem with the narrative synthesis up until now has been that there was no standard way in which the literature was synthesized. It was left to the personal preference and also to the experience of the reviewers; therefore, transparency and rigor could be arguably flawed. The guidance on the narrative synthesisCitation31 helps to enhance the quality and transparency of narrative synthesis and, hence, why it was chosen for the synthesis stage of the overall systematic review. The amount of methodological heterogeneity in the studies included in the final systematic review also led to the decision to undertake such a method of synthesis.
The levels of bias were reduced by having a second reviewer (an experienced qualitative researcher) at the selection and data extraction stages of the systematic review; this reviewer also reviewed the narrative synthesis once completed. It was also reviewed by an expert in the field of narrative synthesis and one of the main authors of the narrative synthesis guidance. This peer review process aimed to reduce any possible bias that may have resulted if the whole process had been undertaken single-handed.
Discussion
For decades, the psychiatric morbidity of medically ill patients has been acknowledged. However, there has been relatively little focus on psychiatric disorders in patients with COPD, except for prevalence studies.Citation41,Citation52 The results of this systematic review have highlighted a relationship between anxiety and depression and the admission to the hospital with acute exacerbations of COPD. It has also been observed that more evidence is needed to substantiate the evidence further.
COPD is a severe and irreversible pulmonary disease that impacts the patient’s general physical condition, functioning, and quality of life.Citation53 COPD patients constitute a substantial part of the medically ill patients, both in hospital wards and in outpatient clinics. They present a considerable challenge to the health care system.Citation3,Citation46,Citation54
The association between COPD and psychiatric disorders – in particular generalized anxiety, panic disorder, and depression – has been acknowledged for many years. The prevalence of psychiatric comorbidity in these patients, as well as the effect of treatment and the prognosis, remains unclear. The diagnostic procedure is complicated by an overlap or close association of somatic and psychiatric symptoms in COPD patients who suffer from comorbid anxiety and depression.
Caring for such an irreversible condition is challenging, with the most important task being not to cure but to optimize the quality of life of the individual patients.Citation54 The quality of life of a chronically ill patient may be particularly complicated by a concurrent depressive disorder that may bring the patient into a vicious circle. The depressed mood will lower the ability needed to cope with the chronic disease. The physical symptoms will then become less tolerable, and the psychosocially debilitating effect of the disease may be enforced by the depressed mood.Citation55,Citation56
The impact of anxiety and depression on COPD patients, their families, and society is significant. Depressed patients with a chronic medical illness are usually sicker than their counterpartsCitation55,Citation57 and have lower treatment adherence.Citation56,Citation58,Citation59 Depression adversely affects physical functioning in people with COPD, such as a reduced 12-minute walk distance.Citation56 By compromising health status, mood disorders may lead to an increased risk of hospitalizationCitation20 and rehospitalization.Citation19 Depression may also be a significant predictor of mortality following hospitalization for acute exacerbation.Citation26
Exacerbations of COPD cause morbidity, hospital admissions, and mortality; they strongly influence health-related quality of life.Citation13 Physiological recovery after an exacerbation is often incomplete, which decreases the health-related quality of life and resistance to future exacerbations. It is important to identify COPD patients who suffer from frequent exacerbations.
More strategies to reduce exacerbation frequency urgently need to be delivered and evaluated. We will then, as clinicians, be in a better position to reduce the morbidity associated with COPD exacerbations significantly and, at last, improve the quality of life of patients with this debilitating condition. Therefore, there is a need to understand the relationship of the comorbid conditions of anxiety and depression to COPD and the acute exacerbation that results in hospital admissions, and a need to determine if there are any other factors involved. This systematic review has highlighted that there is a relationship between anxiety and depression and an increased number of exacerbations, resulting in hospital admission for people with COPD. This relationship, however, is not a simple linear one; many other mediating factors have also been discovered. It has also highlighted the heterogeneity of the evidence base that is currently available and the need for a more consistent approach in future research strategies to address this area of clinical importance so that clinical decision making can be made with accuracy.
Conclusion
Following the synthesis of the data from the systematic review to answer the question “what is the relationship of anxiety and depression to the exacerbations of COPD and the resultant admissions/readmissions to hospital, and are there any other mediating factors involved,” the concluding remarks are:
Some literature supported the fact that anxiety and depression were significant factors in patients’ admissions and readmissions to the hospital following an acute exacerbation of COPD.
The literature also highlighted other significant factors in the relationship between anxiety, depression, and the acute exacerbation of COPD resulting in admission and readmission to hospital. These factors included: reduced quality of life; increasing severity of disease; female gender; lower BODE scores; low socioeconomic status; persistent smoking; increased dyspnea; PaCO2 and decreased PaO2 from admission to discharge; LTOT; sense of loss and inability to cope; decrease in self-efficacy and compliance with treatment; and previous admissions for acute exacerbation of COPD.
Although this goes some way to answering the research question set at the start of the systematic review, for any significant changes to be implemented into clinical practice, further research needs to be carried out. The examination of literature review indicated several implications for the conduct of research in this area; and further research should consider using standardized tools to measure the outcomes, using more comparative study participants and not just men, or groups of COPD patients who were already involved in another study about their disease state. Some studies in this systematic review were done in different countries with different cultural groups who have differing beliefs about diseases. This was discussed by these study authors as being a significant confounding factor; future research should consider and accommodate for this in study design and methodology.
This systematic review was a preliminary review of the literature into this important area of clinical care. Managing depression and anxiety starts with an accurate diagnosis. Many COPD patients have transitory mood symptoms during exacerbations that improve spontaneously as their physical state improves. The challenge is: to identify those who have more permanent and sustained anxiety and depression; to develop ways of screening for and then implementing effective management strategies to alleviate the impact of these comorbidities; and to enable them to cope better with their COPD. The end result should be a reduction in the number of exacerbations that result in unplanned admissions to hospital, which have a devastating effect on the patients and their families.
Disclosure
The authors report no conflicts of interest in this work.
References
- World Health OrganizationWorld Health ReportGenevaWorld Health Organization2002 Available from: http://www.who.int/whr/2002Accessed September 29, 2013
- MurrayCJLopezADAlternative projections of mortality and disability by cause, 1990–2020: Global Burden of Disease StudyLancet19973499064149815049167458
- Department of HealthAn Outcomes Strategy for Chronic Obstructive Pulmonary Disease (COPD) and Asthma in EnglandLondonHer Majesty’s Stationery Office2011 Available from: https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/216139/dh_128428.pdfAccessed September 29, 2013
- JenningsJHDigiovineBObeidDFrankCThe association between depressive symptoms and acute exacerbations of COPDLung2009187212813519198940
- BarnesPJCelliBRSystemic manifestations and comorbidities of COPDEur Respir J20093351165118519407051
- OzkayaSFindikSAticiAGThe cost of hospitalization in patients with acute exacerbation of chronic obstructive pulmonary diseaseClinicoecon Outcomes Res20113151821935328
- CalverleyPPMPA1998COPD; the key factsLondonBLF
- PauwelsRARabeKFBurden and clinical features of chronic obstructive pulmonary disease (COPD)Lancet2004364943461362015313363
- Calderón-LarrañagaACarneyLSoljakMAssociation of population and primary healthcare factors with hospital admissions rates for chronic obstructive pulmonary disease in England; national cross-sectional studyThorax201166319119621076143
- MiravitllesMMurioCGuerreroTGisbert R; DAFNE Study Group; Decisiones sobre Antibioticoterapia y Farmacoeconomía en laEPOCPharmacoeconomic evaluation of acute exacerbations of chronic bronchitis and COPDChest200212151449145512006427
- RobertsCMStoneRALoweDPurseyNABuckinghamRJCo-morbidities and 90-day outcomes in hospitalized COPD exacerbationsCOPD20118535436121864116
- Royal College of Physicians, British Thoracic Society, British Lung FoundationReport of the National Chronic Obstructive Pulmonary Disease Audit 2008; Clinical Audit of COPD Exacerbations Admitted to Acute NHS Units Across the UKLondonThe Health Foundation2008 Available from: http://www.rcplondon.ac.uk/sites/default/files/report-of-the-national-copd-audit-2008-resources-and-organisation-of-care-in-acute-nhs-units-across-the-uk.pdfAccessed September 29, 2013
- WedzichaJADonaldsonGCExacerbations of chronic obstructive pulmonary diseaseRespir Care2003481212041213 discussion 1213–121514651761
- WedzichaJASeemungalTACOPD exacerbations: defining their cause and preventionLancet2007370958978679617765528
- SeemungalTADonaldsonGCBhowmikAJefferiesDJWedzichaJATime course and recovery of exacerbations in patients with chronic obstructive pulmonary diseaseAm J Respir Crit Care Med200016151608161310806163
- DonaldsonGCSeemungalTABhowmikAWedzichaJARelationship between exacerbation frequency and lung function decline in chronic obstructive pulmonary diseaseThorax2002571084785212324669
- AndenaesRKalfossMHWahlAPsychological distress and quality of life in hospitalized patients with chronic obstructive pulmonary diseaseJ Adv Nurs200446552353015139941
- YohannesAMBaldwinRCConnollyMJPredictors of 1-year mortality in patients discharged from hospital following acute exacerbation of chronic obstructive pulmonary diseaseAge Ageing200534549149616107452
- GudmundssonGGislasonTJansonCRisk factors for rehospitalisation in COPD: role of health status, anxiety and depressionEur Respir J200526341441916135721
- FanVSCurtisJRTuSPMcDonellMBFihnSDAmbulatory Care Quality Improvement Project InvestigatorsUsing quality of life to predict hospitalisation and mortality in patients with obstructive lung diseasesChest2002122242943612171813
- Garcia-AymerichJFarreraEFélezMAIzquierdoJMarradesRMAntóJMEstudi del Factors de Risc d’Agudització de la MPOC investigatorsRisk factors of readmission to hospital for a COPD exacerbation: a prospective studyThorax200358210010512554887
- PeruzzaSSergiGVianelloAChronic obstructive pulmonary disease (COPD) in elderly subjects: impact on functional status and quality of lifeRespir Med200397661261712814144
- BosleyCMCordenZMReesPJCochraneGMPsychological factors associated with use of home nebulized therapy for COPDEur Respir J1996911234623508947083
- KunikMERoundyKVeazeyCSurprisingly high prevalence of anxiety and depression in chronic breathing disordersChest200512741205121115821196
- GudmundssonCGislasonTJansonCDepression, anxiety and health status after hospitalisation for COPD: a multicentre study in the Nordic countriesRespir Med20061001879315893921
- AlmagroPCalboEOchoa de EchagüenAMortality after hospitalization for COPDChest200212151441144812006426
- Centre for Reviews and DisseminationSystematic Reviews: CRD’s Guidance for Undertaking Reviews in Health CareLayerthorpeYork Publishing Services Ltd2009 Available from: http://www.york.ac.uk/inst/crd/pdf/Systematic_Reviews.pdfAccessed September 29, 2013
- von ElmEAltmanDGEggerMPocockSJGøtzschePCVandenbrouckeJPSTROBE InitiativeThe Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studiesJ Clin Epidemiol200861434434918313558
- Critical Appraisal Skills Programme2013 Retrieved on 19.4.13 from; http://www.casp-uk.netAccessed September 29, 2013
- PluyePRobertECargoMMixed Methods Appraisal Tool Version 2011Quebec, CanadaMcGill University2011 Available from: http://mixedmethodsappraisaltoolpublic.pbworks.com/f/MMAT%202011%20criteria%20and%20tutorial%202011-06-29.pdfAccessed January 17, 2013
- PopayJRobertsHSowdenAGuidance on the Conduct of Narrative Synthesis in Systematic Reviews; A Product from the ESRC Methods ProgrammeLancaster, UKLancaster University2006 Available from: http://www.lancaster.ac.uk/shm/research/nssr/research/dissemination/publications/NS_Synthesis_Guidance_v1.pdfAccessed September 29, 2013
- AbramsTEVaughan-SarrazinMVan der WegMWAcute exacerbations of chronic obstructive pulmonary disease and the effect of existing psychiatric comorbidity on subsequent mortalityPsychosomatics201152544144921907063
- AlcázarBGarcía-PoloCHerrejónAFactors associated with hospital admissions for exacerbation of chronic obstructive pulmonary diseaseArch Bronconeumol20124837076 Spanish [with English abstract]22196478
- AlmagroPBarreiroBOchoa de EchaguenARisk factors for hospital admissions in patients with chronic obstructive pulmonary diseaseRespiration200673331131716155352
- CaoZOngKCEngPTanNCNgTP 2006Frequent hospital readmissions for acute exacerbation of COPD and their associated factorsRespirology200611218819516548905
- CarneiroRSousaCPintoAAlmeidaFOliveiraJRRochaNRisk factors for readmission after hospital discharge in chronic obstructive pulmonary disease. The role of quality of life indicatorsRev Port Pneumol2010165759777 Portuguese [with English abstract]20927493
- CoventryPAGemmellIToddCJPsychosocial risk factors for hospital readmissions in COPD patients on early discharge services: a cohort studyBMC Pulm Med2011114922054636
- EisnerMDBlancPDYelinEHInfluence of anxiety on health outcomes in COPDThorax201065322923420335292
- Gruffydd-JonesKLangley-JohnsonCDyerCBadlanKWardSWhat are the needs of patients following discharge from hospital after an acute exacerbation of chronic obstructive pulmonary disease (COPD)?Prim Care Respir J200716636336818038104
- LaurinCLabrecqueMDupuisGBaconSLCartierALavoieKLChronic obstructive pulmonary disease patients with psychiatric disorders are at greater risk of exacerbationsPsychosom Med200971666767419561164
- MaurerJRebbapragadaVBorsonSACCP Workshop Panel on Anxiety and Depression in COPDAnxiety and depression in COPD: current understanding, unanswered questions, and research areasChest2008134Suppl 443S56S18842932
- QuintJKBaghai-RavaryRDonaldsonGGWedzichaJARelationship between depression and exacerbations in COPDEur Respir J2008321536018321938
- RegvatJŽmitekAVegnutiMKošnikMŠuškovičSAnxiety and depression during hospital treatment of exacerbation of chronic obstructive pulmonary diseaseJ Int Med Res20113931028103821819737
- XuWColletJPShapiroSIndependent effect of depression and anxiety on chronic obstructive pulmonary disease exacerbations and hospitalizationsAm J Respir Crit Care Med2008178991392018755925
- NgTPNitiMTanWCCaoZOngKCEngPDepressive symptoms and chronic obstructive pulmonary disease: effect on mortality, hospital admission, symptom burden, functional status, and quality of lifeArch Intern Med20071671606717210879
- KimHFKunikMEMolinariVAFunctional impairment in COPD patients: the impact of anxiety and depressionPsychosomatics201041646547111110109
- FanVSRamseySDGiardinoNDNational Emphysema Treatment Trial (NETT) Research GroupSex, depression, and risk of hospitalization and mortality in chronic obstructive pulmonary diseaseArch Intern Med2007167212345235318039994
- BaileyPHThe dyspnea-anxiety-dyspnea cycle: COPD patients’ stories of breathlessness: “It’s scary when you can’t breathe”Qual Health Res200414676077815200799
- NicolsonPAndersonPThe patient’s burden; physical and psychological effects of acute exacerbations of chronic bronchitisJ Antimicrob Chemother200045253210719009
- SolerJJSánchezLRománPMartínezMAPerpiñáMRisk factors of emergency care and admissions in COPD patients with high consumption of health resourcesRespir Med200498431832915072172
- ChenYJNarsavageGLFactors related to chronic obstructive pulmonary disease readmissions in TaiwanWest J Nurs Res200628110512416676728
- MikkelsenRLMiddelboeTPisingerCStageKBAnxiety and depression in patients with chronic obstructive pulmonary disease (COPD). A reviewNord J Psychiatry2004581657014985157
- ViegiGPistelliFSherrillDLMaioSBaldacciSCarrozziLDefinition, epidemiology and natural history of COPDEur Respir J2007305993101317978157
- van EdeLYzermansCJBrouwerHJPrevalence of depression in patients with chronic obstructive pulmonary disease: a systematic reviewThorax199954868869210413720
- CiechanowskiPSKatonWJRussoJEDepression and diabetes: impact of depressive symptoms on adherence, function, and costsArch Intern Med2000160213278328511088090
- FelkerBKatonWHendrickSCThe association between depressive symptoms and health status in patients with chronic pulmonary diseaseGen Hosp Psychiatry2001232566111313071
- SullivanMSimonGSpertusJRussoJDepression-related costs in heart failure careArch Intern Medicine20021621618601866
- DiMatteoMRLepperHSCroghanTWDepression is a risk factor for noncompliance with medical treatment: meta-analysis of the effects of anxiety and depression on patient adherenceArch Intern Medicine20001601421012107
- LinEHKatonWVon KorffMRelationship of depression and diabetes self-care, medication adherence, and preventive careDiabetes Care20042792154216015333477
- DalalAAShahMLunacsekOHananiaNAClinical and economic burden of depression/anxiety in chronic obstructive pulmonary disease patients within a managed care populationCOPD20118429329921827298