
Abstract
Bacterial infection of the lower respiratory tract in chronic obstructive pulmonary disease (COPD) patients is common both in stable patients and during acute exacerbations. The most frequent bacteria detected in COPD patients is Haemophilus influenzae, and it appears this organism is uniquely adapted to exploit immune deficiencies associated with COPD and to establish persistent infection in the lower respiratory tract. The presence of bacteria in the lower respiratory tract in stable COPD is termed colonization; however, there is increasing evidence that this is not an innocuous phenomenon but is associated with airway inflammation, increased symptoms, and increased risk for exacerbations. In this review, we discuss host immunity that offers protection against H. influenzae and how disturbance of these mechanisms, combined with pathogen mechanisms of immune evasion, promote persistence of H. influenzae in the lower airways in COPD. In addition, we examine the role of H. influenzae in COPD exacerbations, as well as interactions between H. influenzae and respiratory virus infections, and review the role of treatments and their effect on COPD outcomes. This review focuses predominantly on data derived from human studies but will refer to animal studies where they contribute to understanding the disease in humans.
COPD overview
Chronic obstructive pulmonary disease (COPD) is a major cause of morbidity and is the fourth leading cause of mortality worldwide.Citation1 Conservative estimates suggest a 10% prevalence in the general population, but among heavy smokers, this figure increases to almost 50%.Citation2 The clinical course of COPD is characterized by a progressive decline in lung function, accompanied by worsening exercise tolerance and health status. The pathological hallmark of COPD is an abnormal inflammatory response in the airways and alveoli. The principal abnormalities in airways are the presence of an inflammatory cellular infiltrate and remodeling that thickens the airway wall, thereby reducing the airway diameter and increasing resistance to flow.Citation2 In the lung parenchyma, COPD is characterized by prominent inflammatory infiltrates in the alveolar walls, destruction of alveoli, and enlargement of air spaces. Cigarette smoking is a predominant etiological factor in the development of COPD, but other factors such as burning biomass fuels for cooking and heating are important causes, particularly in developing countries. Although exposure to cigarette smoke/biomass smoke is required for the development of COPD, disease progression and airway inflammation persist even after smoking cessation.Citation3 Therefore, other factors contribute to persistence of inflammation and progression of the disease. One such factor is respiratory infection, with both bacterial and viral infections implicated in contributing to the pathogenesis of COPD.Citation4,Citation5 Bacteria are commonly detected in COPD, with the most common organism isolated being Haemophilus influenzae in most studies. The chronic clinical course of COPD is punctuated by periods of increased symptoms, termed acute exacerbations,Citation6 which have both short- and long-term adverse effects in COPD patients. They have immediate effects resulting in considerable morbidity and mortality in COPD and are a major cause of excess health care costs, as they often result in unscheduled health care visits, treatment costs, and hospitalizations. Exacerbations also have long-term effects, as frequent exacerbations are associated with more rapid decline in lung function, airway and systemic inflammation, and impaired quality of life.Citation7–Citation9 Approximately half of all COPD exacerbations are associated with bacterial infections, and as is the case in stable COPD, the most common bacteria detected is H. influenzae.Citation10 Therefore, H. influenzae may have a major pathogenic role both in stable COPD and in COPD exacerbations and has been the focus of much research interest.
H. influenzae: bacteriology
H. influenzae is a pleomorphic Gram-negative coccobacillus that is isolated exclusively from humans, predominantly from the respiratory tract. It is a member of the Pasteurellaceae family and is capable of growing either aerobically or anaerobically,Citation11 and strains are divided into two groups on the basis of the presence of a polysaccharide capsule. Encapsulated strains are reactive with typing antisera (typeable), whereas unencapsulated strains are nonreactive (nontypeable H. influenzae [NTHi]). Six encapsulated serotypes (a–f) have been identified and account for the majority of invasive Haemophilus infections such as septicemia, pneumonia, and meningitis. NTHi, in contrast, rarely causes invasive disease but commonly colonizes the upper respiratory tract and can cause mucosal infections in both children and adults. The vast majority of Haemophilus strains isolated from the respiratory tract in COPD patients are NTHi. H. influenzae is a common commensal of the upper respiratory tract, with 20% of children colonized in the first year of life and up to 50% colonized by age 5 years.Citation12 Disease caused by NTHi is predominantly by contiguous spread from the nasopharynx to adjacent structures such as sinuses, the middle ear, and trachea. In contrast to the frequent detection of H. influenzae in the upper respiratory tract, lower respiratory tract colonization appears rare in healthy individuals. In 70 healthy subjects from six different studies undergoing bronchoscopy, H. influenzae was detected in only 4%.Citation13 Two subsequent studies that were not included in this analysis have been published more recently. In the first, H. influenzae was not detected in any of 26 healthy individuals undergoing bronchoscopy during anesthesia for elective surgery.Citation14 In the second, H. influenzae was isolated in two (13.3%) of 15 healthy subjects who had never smoked, but in zero of 20 exsmokers.Citation15 Therefore, from these results, the true prevalence of lower respiratory tract colonization with H. influenzae in healthy individuals is unclear, but it is undoubtedly lower than that in the upper respiratory tract. These studies were small, and therefore it is difficult to draw conclusions from them regarding the prevalence of H. influenzae colonization in the general population. Discrepancies in detection rates between studies are likely to be related to differences in characteristics of the populations studied, such as age, sex, smoking history, and so on, and further studies with greater numbers of participants are required.
Methods to detect H. influenzae
For many years, the standard method for detection of H. influenzae in respiratory samples was growth on culture plates and identification using morphological characteristics and growth requirements. However, culture has a number of drawbacks, including difficulty in distinguishing H. influenzae from other bacterial species, such as Haemophilus haemolyticus and Haemophilus parainfluenzae, as well as low sensitivity. H. influenzae possesses the ability to persist in biofilms and within host cells, and organisms in these niches may not be detected using culture of airway samples such as sputum, bronchial wash, and bronchoalveolar lavage.Citation16 Culture-independent techniques based on detection and amplification of nucleic acid sequences using polymerase chain reaction (PCR) have been developed during the past 2 decades to detect pathogens such as H. influenzae. Protein D is a highly conserved surface lipoprotein present in all encapsulated and nonencapsulated H. influenzae strains,Citation17 making its gene (hpd) an attractive target for the development of a PCR assay. An hpd real-time PCR assay can detect both encapsulated H. influenzae and NTHi strains with high sensitivity and specificity.Citation18 Studies comparing bacterial detection rates using culture and PCR have consistently demonstrated greater sensitivity with PCR. Detection rates of H. influenzae in nasopharyngeal swabs collected from healthy individuals are 2.5–3 times greater with PCR compared with culture.Citation19,Citation20 As will be described in the following section, this has also been reported in COPD patients. However even with PCR, distinguishing H. influenzae from other species such as H. haemolyticus can be difficult,Citation21 and more sophisticated techniques such as proteomic profiling may be required.Citation22 More recently, newer techniques have been developed based on the sequencing of the 16S gene encoding bacterial ribosomal RNA. The 16S gene contains invariant regions used for priming the sequencing reaction and variable regions that permit genus- and species-level identification. High-throughput sequencing and sorting of the amplicons generated enables the identification of entire microbial communities. These techniques have revealed the presence of a respiratory “microbiome,” even in the respiratory tracts of healthy individuals, and overturned the previous dogma that the lower airways are sterile in health.Citation23 Initial studies have revealed that the genus Proteobacteria that includes Haemophilus is overrepresented in the airways of subjects with asthma and COPD compared with in healthy individuals.Citation24 Further studies of the respiratory microbiome are likely to radically change our understanding of the role of bacteria such as H. influenzae in both health and disease.
The epidemiology of H. influenzae in COPD
It is well established that bacteria are often present in the lower airways in patients with stable COPD, although colonization rates vary between different studies and are affected by factors such as disease severity, treatments used, and sampling methods used. A pooled analysis of studies using bronchoscopic sampling reported that potentially pathogenic organisms were present in 29% of stable COPD patients,Citation13 and studies using sputum have reported that potentially pathogenic organisms are present in up to half of COPD patients.Citation25–Citation27 The most common organisms detected in COPD patients are consistently H. influenzae, Streptococcus pneumoniae, and Moraxella catarrhalis, with H. influenzae accounting for around half of all isolates in the airways of COPD patients.Citation13,Citation25–Citation27 However, the true prevalence of infection with H. influenzae in COPD may be underestimated by studies using culture for bacterial detection. In a longitudinal study over the course of 7 years, Murphy et al reported frequent episodes when sputum cultures were negative that were preceded and followed by positive cultures with the same strains of H. influenzae, and strain-specific H. influenzae DNA was detected in some of the sputum samples that had negative cultures.Citation28 Other studies using PCR have confirmed higher detection rates compared with culture alone in COPD,Citation29–Citation31 with H. influenzae detected in 60% of sputum samples using PCR compared with only 30% using culture.Citation31
Bacteria can be detected in sputum in 50%–60% of COPD patients during acute exacerbations, and H. influenzae is consistently among the most common bacteria reported.Citation10,Citation13,Citation32 As discussed previously, even this may be an underestimate because of the limitations of culture. In a study of 15 chronic bronchitis patients with acute respiratory failure, NTHi was detected in only one bronchial wash specimen, whereas using in situ hybridization, intracellular NTHi was present in 13 (86.7%) of 15 bronchial biopsies.Citation14 Sequencing studies have revealed that Proteobacteria are a key component of the respiratory microbiome in COPD exacerbations.Citation33, Citation34
Therefore, although it is clear that lower respiratory tract infection with H. influenzae is much more prevalent in COPD patients compared with healthy individuals, the exact prevalence remains to be determined and is highly dependent on the diagnostic method used.
Host immunity and immune evasion in H. influenzae infection
H. influenzae commonly colonizes the nasopharynx and causes upper respiratory tract disease in healthy individuals, but infection of the lower airways is rare because of host immune responses that prevent spread to the lower respiratory tract. In contrast, H. influenzae is commonly found in the lower airways of patients with COPD, implying that mucosal host immune mechanisms are impaired. H. influenzae possesses a number of mechanisms to avoid or neutralize host immune responses, and therefore it is likely that the combination of pathogen immune evasion and impaired host immunity combine to promote lower airway infection in COPD.
Host immunity to H. influenzae in healthy individuals
Structural components
The structural integrity of the respiratory tract is vital to preventing infection with inhaled microorganisms. Important mechanisms including an intact respiratory epithelium, mucus production, and mucociliary clearance via the action of cilia and cough act to prevent infection with respiratory pathogens such as H. influenzae.Citation4,Citation11 The importance of these mechanisms in host defense is highlighted by high rates of H. influenzae infection in conditions such as cystic fibrosisCitation35 and immotile cilia syndromesCitation36 that are characterized by abnormal mucociliary function.
Cellular immunity
Immune cells such as neutrophils and alveolar macrophages are present in large numbers in the airways and constitute a first line of defense against respiratory pathogens. Macrophages recognize microorganisms via the presence of surface receptors such as toll-like receptors leading to phagocytosis, microbicidal killing, and initiation of immune responses.Citation11 A key component of the NTHi cell wall is lipooligosaccharide, which is recognized by toll-like receptor 4, leading to macrophage activation and phagocytosis,Citation37 and the membrane protein P2, recognized by toll-like receptor 2.Citation38,Citation39 P6 is a specific trigger of macrophage activation, with secretion of interleukin 8 (IL-8) and tumor necrosis factor α being key effectors of P6-induced macrophage responses.Citation40
Complement and immunoglobulin A
The complement system is an essential part of the innate immune system, and activation of complement results in protein activation and deposition on the surface of pathogens, resulting in opsonization and phagocytosis. Invading pathogens activate complement either through antibody binding (classical pathway) or spontaneously via the alternative pathway.Citation41 Although complement is not present in the healthy human respiratory tract, after infection and inflammation, the permeability of the mucosa increases and plasma, including complement proteins, enters the airway lumen.Citation42,Citation43 Immunoglobulin A (IgA) is the main element of the humoral immune response that provides protection against microbial antigens at mucosal surfaces, including the lung. Mucosal IgA can bind to bacteria and prevent mucosal attachment and facilitate cytotoxicity.Citation44 The importance of complement and IgA in host defense against pathogens is illustrated by the increased susceptibility to bacterial infections, including H. influenzae, seen in patients with complement deficiencies and hypogammaglobulinemia.Citation45,Citation46
Adaptive immunity
The adaptive immune response consists of humoral (B-cell-mediated) and cellular (T-cell-mediated) immunity.Citation4,Citation47 Hypogammaglobulinemia is a risk factor for systemic infection by NTHi, illustrating the importance of antibodies.Citation48 T-helper cells and cytotoxic T lymphocytes contribute by producing interferon γ,Citation4 which enhances the macrophage-induced killing of NTHi.Citation49 Cytotoxic T cells and natural killer cells may be particularly important in the control of intracellular pathogens,Citation50 and there is evidence that impaired T-helper responses to H. influenzae contribute to the failure to eradicate intracellular infection,Citation49 resulting in chronic airway infection.Citation47
Mechanisms of immune evasion by H. influenza
Phase variation and antigenic change
H. influenzae has the ability to lose or gain cell structures, thereby allowing it to evade host immune responses, particularly antibody-mediated immunity. This property is called phase variation and has been reported for a number of different components of H. influenzae, including adhesins, pili, and lipooligosaccharide.Citation51,Citation52 Furthermore, some strains of H. influenzae undergo permanent changes in the amino acid sequences of important immunogenic surface proteins such as P2 and P5 in a manner reminiscent of antigenic drift in influenza viruses.Citation53 There is evidence that phase variation may contribute to persistent infection in COPD, as it has been reported that serial isolates of H. influenzae from patients with COPD demonstrate decreased levels of HMW1 and HMW2 in association with persistence.Citation54
Intracellular growth/biofilms
H. influenzae exhibits a number of different growth strategies that promote survival, including intracellular growth and the formation of biofilms.Citation52 Biofilms are microbial communities that are encased within a matrix and can be found in a number of environments, including the human respiratory tract. Biofilms are believed to confer protection from a number of immune mechanisms such as antimicrobial peptides and antibodies, as well as from antibiotics, thereby promoting survival and persistence. There is evidence from both human studies and animal models that H. influenzae forms biofilms, which is likely to be an important mechanism in promoting persistent infection in the human respiratory tract.Citation55–Citation58 Although H. influenzae is predominantly an extracellular pathogen, there is evidence it is able to enter cells of the respiratory tract. H. influenzae has been detected in epithelial cells,Citation59,Citation60 adenoidal tissue,Citation61,Citation62 and monocytes/macrophages.Citation63 As is the case for biofilm formation, intracellular growth may offer H. influenzae protection from antibody-mediated immune responses and antibiotics, and therefore may be another important mechanism of persistent infection.Citation64 As discussed previously, both biofilms and intracellular growth may also contribute to underdetection of H. influenzae using sputum culture.
Complement/IgA
Complement and IgA are important mechanisms of host protection against H. influenzae. Some strains of H. influenzae demonstrate reduced susceptibility to complement, and although the exact mechanisms of this are unknown, a number of factors including lipooligosaccharide and surface proteins P2 and P5 are believed to contribute.Citation41 In addition, it has been demonstrated that NTHi can acquire host complement inhibitors such as vitronectin,Citation65,Citation66 and factor H.Citation67 NTHi can also secrete proteases that cleave the main IgA subclass IgA1,Citation68 thus offering protection against IgA-mediated cytotoxicity.
Metabolic adaptations
In addition to changes to structural components, organisms in the human respiratory tract may undergo adaptations in metabolic pathways to survive in a hostile environment with limited nutrients, low pH, and high levels of reactive oxygen species. Such adaptations adopted by H. influenzae include production of urease,Citation69 antioxidants,Citation70 and proteins involved in iron and heme metabolism.Citation71 There is evidence that upregulation of these metabolic pathways is related to the ability of NTHi strains to survive in the respiratory tract.Citation72–Citation74
Mechanisms of H. influenzae infection in COPD
There are a number of structural and functional changes in the airways of COPD patients that compromise host immunity to respiratory pathogens. H. influenzae has developed a number of mechanisms to evade host immune responses, many of which are already impaired in COPD. Therefore, among respiratory pathogens, H. influenzae appears to be uniquely adapted to exploit the already-impaired host immunity in COPD and establish persistent infection.
Bacterial adhesion
The first step in establishing infection in the respiratory tract by a pathogen is adhesion to the respiratory epithelium. H. influenzae possesses a number of cell surface proteins and structures that facilitate adhesion to respiratory mucosal surfaces. These include the presence of pili (rodlike projections present on a small subset of strainsCitation75) and a number of surface proteins that facilitate adhesion. The membrane proteins P2 and P5 facilitate binding of the bacteria to mucus,Citation38 and the adhesins HMW1, HMW2, protein E, and protein F bind to epithelial cells and extracellular matrix proteins.Citation76–Citation78 Protein D is a highly conserved 42 kDa surface lipoprotein identified in all strains of H. influenzae. The activity of protein D as a virulence factor is as a glycerophosphodiesterase that promotes adherence of NTHi to airway epithelial cells and internalization by macrophagesCitation63 and impairs ciliary function.Citation79–Citation81 The airways in COPD patients are characterized by damaged epithelium, mucous hypersecretion, and reductions in cilia numbers and function. Therefore, this combination of exposed extracellular matrix, excess mucus, and impaired mucociliary clearance provides an ideal environment for the adhesion and subsequent growth of H. influenzae. Strains of H. influenzae isolated from COPD patients are more likely to express adhesion molecules such as HMW.82
Cellular and humoral immunity
Inflammatory cells in the airways such as neutrophils and macrophages are increased in COPD, which would be expected to result in more effective clearance of inhaled pathogens. However, the opposite is the case, as the function of these immune cells is impaired. Several studies have demonstrated that phagocytosis of H. influenzae and production of cytokines by macrophages is impaired in COPD.Citation40,Citation83–Citation86 Impaired production of cytokines by macrophages in response to H. influenzae has been related to exacerbation frequency in COPD patients.Citation83 As discussed previously, survival of H. influenzae has been documented in macrophagesCitation87 and epithelial cells,Citation88 and intracellular H. influenzae is more common in patients with chronic bronchitis compared with in healthy subjects.Citation14 Therefore, impaired macrophage responses to NTHi may promote intracellular survival, but further studies are required to prove this conclusively.
In addition to compromised macrophage function, T lymphocyte cell responses to H. influenzae in COPD are also impaired.Citation89 Again, this may have clinical implications, as robust T-cell responses to the surface P6 lipoprotein are associated with a reduced risk for exacerbations.Citation90 A recent paper reported that numbers of T regulatory cells are increased in COPD patients.Citation91 Moreover T regulatory cells from COPD patients suppressed P6-specific T-cell proliferation to a greater extent than T regulatory cells from healthy controls; therefore, this may be an important mechanism of reduced effector T-cell responses to H. influenzae. Variations in antigenic components of the organism, including the membrane outer proteins P2 and P5Citation92, Citation93 and the immunoglobulin A1 protease,Citation94 may contribute to immune evasion and reduced host immunity.
There is evidence that IgA secretion is impaired in COPDCitation95 and that reduced levels of Haemophilus-specific IgA may be related to chronic infection with H. influenzae.Citation96,Citation97
Inflammatory responses and H. influenzae in stable COPD
The presence of bacteria in the lower respiratory tract in stable COPD patients is termed colonization, but there is increasing evidence that this is not a benign phenomenon but is associated with adverse outcomes. Bacterial infection in stable COPD is associated with increased airways and systemic inflammation,Citation98 more frequent exacerbations,Citation27 and poorer health status.Citation15,Citation99 Therefore, chronic infection or persistent infection may be more accurate descriptions than colonization.Citation100 Whether all bacterial species have adverse effects is unknown, as few studies have examined the role of specific bacteria such as H. influenzae. Data from animal models have suggested that NTHi can induce both inflammatory and structural changes in the lungs. Chronic instillation of NTHi in mice induced an inflammatory infiltrate similar to that seen in COPD, with increases in inflammatory cytokines and cells (neutrophils, macrophages, and CD8+ T cells) and airway collagen deposition.Citation101 When exposed to both cigarette smoke and NTHi, mice developed structural changes typical of COPD, including emphysema, lung inflammation, and goblet cell metaplasia in both large and small airways.Citation102
Human studies have reported that H. influenzae is associated with higher sputum levels of inflammatory mediators such as neutrophils, IL-1β, IL-12, IL-8, tumor necrosis factor α, and matrix metalloprotease 9.Citation97,Citation98,Citation103,Citation104 Moreover, COPD patients colonized with NTHi reported worse health status compared with noncolonized patients, and these effects were not seen in patients colonized with other bacteria.Citation98 Therefore, the presence of H. influenzae in the lower airways of COPD patients is associated with increased inflammation and poorer health status. Whether the increases in inflammatory mediators contribute to long-term structural changes, as has been reported in animal studies, is unknown, but it is an important area for further research. Further studies also are needed to determine the effects of persistent infection with H. influenzae on other outcomes such as exacerbations, disease progression, and even mortality.
H. influenzae and COPD exacerbations
H. influenzae is frequently detected in airway samples collected from COPD patients during exacerbations,Citation10 but this does not prove causation, as the organism may have been present when the patient was clinically stable. Studies comparing bacterial detection in stable and exacerbated patients have generally reported higher rates of bacterial infection in COPD exacerbations.Citation10,Citation29,Citation105,Citation106 Therefore, H. influenza infection can result in either chronic infection or acute exacerbation. The mechanisms that determine the outcome of infection are poorly understood but are likely to involve both pathogen and host factors.
Exposure to new strains of NTHi to which the host has no preexisting immunity is one mechanism that may underlie the occurrence of acute exacerbations. Sethi et al carried out molecular typing on bacteria isolated from sputum samples from COPD patients collected when stable and during exacerbations over the course of 56 months. Isolation of H. influenzae using culture alone was not associated with exacerbations, but detection of a new strain was associated with increased risk for exacerbation.Citation107 An exacerbation was diagnosed in 33% of visits at which a new bacterial strain was isolated compared with 15.4% of visits at which no new strain was present. Therefore, the majority of new strain acquisitions did not result in exacerbation, and other mechanisms must contribute. It was subsequently recognized that some strains of H. influenzae were actually H. haemolyticus species.Citation108 When the results of the study were reanalyzed with the exclusion of H. haemolyticus, the association between acquisition of a new strain of H. influenzae and acute exacerbations was stronger.Citation108 In another study from this group, an immune response to homologous H. influenzae occurred after 61% of exacerbations with newly acquired strains compared with 21.2% of exacerbations with preexisting strains.Citation109
Factors relating to pathogen-related characteristics have been less well defined, but one study has reported a different genetic profile in strains associated with exacerbations compared with strains associated with asymptomatic chronic infection.Citation110 Moreover, strains isolated from COPD patients during an exacerbation elicited greater inflammatory responses in mice and in vitro models compared with colonizing strains,Citation111 although another study failed to replicate these findings.Citation112 Therefore, it is likely there are complex interactions between host immunity and the pathogenicity of the infecting strain of H. influenzae that determine the outcomes of infection.
Respiratory viruses and Haemophilus influenzae
Other external factors may influence the interactions between host and H. influenzae; one such factor is infection with a respiratory virus. A relationship between influenza infection and H. influenzae pneumonia has long been recognized,Citation113 and in fact, H. influenzae derives its name from the original mistaken belief that it was the causative organism of influenza. Synergism between the two organisms has been demonstrated in animal models.Citation114 Respiratory virus infection can be detected in up to 40% of COPD exacerbations,Citation115 and therefore virus infections in patients with chronic bacterial infection and concurrent virus/bacterial coinfections may be a relatively common occurrence. Data from in vitro studies and animal studies have suggested a number of potential mechanisms whereby virus and bacterial infections may interact. Mice infected with rhinovirus show impaired clearance of NTHi, which is related to impaired production of chemokines by both epithelial cells and macrophages in response to bacterial infection.Citation116 Impaired chemokine responses to bacterial products in macrophages infected with rhinovirus have also been reported.Citation117 Virus infection may also have effects on the airway epithelium that promote bacterial infection. Rhinovirus infection of epithelial cells in vitro disrupts the airway epithelial barrier, resulting in increased transmigration of NTHi across the epithelial barrier.Citation118 In addition, rhinovirus infection increases expression of adhesion molecules on the surface of epithelial cells and enhances bacterial adhesion,Citation119,Citation120 and this effect has also been reported for other respiratory viruses.Citation121 Whether these mechanisms are relevant in vivo is not known. Rhinovirus infection did not increase expression of the receptor platelet activating receptor in vivo in bronchial biopsies in COPD patients.Citation122
Few studies have examined the role of concurrent virus-bacteria coinfection in COPD exacerbations. Those that are available have reported detection rates of between 12% and 25%.Citation10,Citation30 A study examining infection with respiratory viruses and H. influenzae found evidence of coinfection in only 9% of exacerbations.Citation123 Our group has examined the relationship between viral and bacterial infections in COPD patients, using experimental rhinovirus infection as a model of COPD exacerbation.Citation124 In COPD subjects infected with rhinovirus, secondary bacterial infections occurred in 60%, with H. influenzae the predominant organism (46% of bacterial isolates). The peak of virus infection occurred on day 5 postinoculation, whereas the peak of bacterial infection occurred later, on day 15. Therefore, studies in naturally occurring exacerbations in which a sample is collected at a single point are likely to underestimate the frequency of coinfections, as our data demonstrate that bacterial infection occurs up to 10 days after the initial viral infection. This was confirmed by two studies that carried out sequential sampling during COPD exacerbations. In one study, samples were collected at the onset of exacerbation and again 5–7 days later.Citation125 In 19% of COPD exacerbations, a virus and bacteria were detected at exacerbation onset, but 36% of exacerbations in which a virus was detected on day 1 developed bacterial infection in the next 7 days. The commonest virus/bacteria combination was rhinovirus/H. influenzae; 78% of exacerbations in which H. influenzae was detected were preceded by symptoms of an upper respiratory tract infection. In the second study, COPD exacerbations associated with rhinovirus infection had bacteria detected in 73% of second samples collected 14 days later.Citation126 Again, H. influenzae was the most frequent bacterial isolate. In both experimentalCitation124 and natural infections,Citation106 virus infection is associated with higher bacterial loads.
Participants who developed secondary bacterial infection after experimental rhinovirus infection had lower airway levels of the antimicrobial peptides elafin and secretory leukoprotease inhibitor,Citation124 suggesting another mechanism whereby virus infections may impair antibacterial immune responses.
In the experimental rhinovirus model, no subjects had bacteria detected by sputum culture at baseline before inoculation with rhinovirus; however, using sequencing techniques to analyze the bacterial microbiome, bacterial DNA could be detected. We further examined whether virus infection had an effect on the respiratory microbiome. After virus infection, there was a 16% increase in the number of proteobacterial sequences on day 15 postinoculation.Citation33 Within the Proteobacteria phylum, there was a 21% increase in the average relative abundance of H. influenzae. At day 42 postinoculation, H. influenzae remained elevated compared with baseline, despite no organisms being detected by culture at this point. Therefore, this is the first in vivo evidence that a virus infection can induce a profound and prolonged change in the bacterial microbiome in the lungs and that there appears to be a specific interaction between rhinovirus and H. influenzae. The subjects included in the experimental infection studies had GOLD stage II COPD, had negative baseline sputum cultures, were not using inhaled cortico steroids, and had few previous exacerbations. In patients with more severe COPD with positive sputum cultures, the effect of virus infection on the bacterial microbiome may be even more pronounced. This holds out the prospect that treating or preventing viral infections may also reduce secondary bacterial infections and excessive antibiotic use.
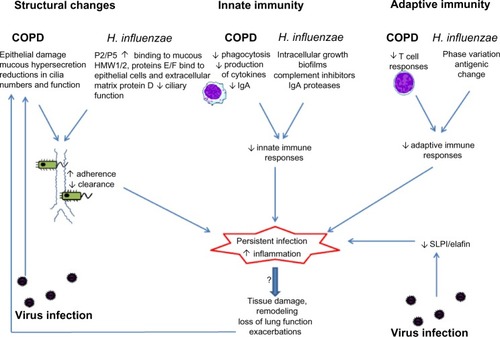
Most research has focused on bacterial infections occurring after initial virus infection. However, chronic bacterial infection may also influence host responses to respiratory virus infections. H. influenzae infection of human epithelial cells potentiates cytokine responses and increases virus binding after subsequent rhinovirus infection.Citation127 There are as yet no data investigating whether chronic bacterial infection influences responses to virus infection in vivo in COPD. The presence of bacteria in the lower airways is associated with increased exacerbations, and increased susceptibility to virus infection may be one mechanism mediating this effect, but further studies are needed to investigate this. Potential mechanisms of interactions between COPD, Haemophilus influenzae and respiratory virus infection are summarized in .
Figure 1 Interactions between chronic obstructive pulmonary disease (COPD), virus infection, and persistent infection with Haemophilus influenzae. Structural changes in the airways and impaired innate and acquired immunity in COPD are exploited by H. influenzae, leading to failure to eradicate the organism and persistent infection. Virus infections may also cause epithelial damage and immune suppression and may favor persistent infection. Persistent infection with H. influenzae enhances airway inflammation and may contribute to disease progression in COPD.
Therapies
In view of the evidence that persistent H. influenzae infection is associated with adverse outcomes in COPD, treating H. influenzae holds out the possibility of clinical benefit in COPD patients. Current anti-inflammatory therapies in COPD such as inhaled corticosteroids are not very effective. As H. influenzae infection is associated with greater airway inflammation in COPD, eradication of H. influenzae may have an anti-inflammatory effect. In this review, we focus on two interventions that are specifically relevant to Haemophilus influenzae infection: vaccination and long-term antibiotics.
Vaccination
Because of the significant mortality associated with invasive capsulated H. influenzae type b (Hib) disease in infants and children, conjugate Hib vaccines were developed that induce bactericidal antibodies to the capsular polysaccharide polyribitol ribose phosphate. Conjugation of polyribitol ribose phosphate to a carrier protein promotes antibody responses in infants younger than 2 years.Citation128 After introduction of the conjugate Hib vaccine in the United States, the incidence of invasive H. influenzae disease has decreased by 99%, reaching less than one case per 100,000 children younger than 5 years.Citation128 A vaccine for nontypeable H. influenzae is attractive because of its role in persistent infection and exacerbations in COPD. However, developing such a vaccine is likely to prove more challenging than was the case with Hib in view of the extensive antigenic variation among membrane proteins, lipopolysaccharides, and secreted virulence factors displayed by NTHi. Protein P2 is the major immunogenic outer membrane protein of NTHi and a target for human bactericidal immune responses. However, the extracellular portions of P2 demonstrate a high degree of sequence variability among strains, and antibodies that develop after a COPD exacerbation are highly strain-specific and do not prevent infection with different strains.Citation109 Point mutations of genes coding for P2 or exchange of genes between strains colonizing the respiratory tract contribute to immune evasion and bacterial persistence in the respiratory tract.Citation93,Citation129 Therefore, although a P2 vaccine candidate has shown correlates with immune protection in animal models,Citation130 it is likely to be a poor target in humans.
Protein D is a highly conserved surface lipoprotein identified in all strains of H. influenzae. Rats vaccinated with protein D have been shown to clear NTHi more effectively than controls in middle ear and pulmonary clearance models.Citation131 In a chinchilla model of otitis media, protein D vaccination conferred a 34% protection against development of NTHI-induced otitis media.Citation132 Children acquire serum antibodies to protein D within the first 2–3 years of life, and vaccination with a pneumococcal vaccine conjugated with H. influenzae protein D has been shown to induce high circulating levels of antibodies and a 35.5% reduction in otitis media caused by NTHi.Citation133 Hawdon et al also demonstrated that serum immunoglobulin G antibodies to protein D were significantly reduced in adults with COPD when compared with healthy, age-matched controls.Citation134 Therefore, on the basis of these observations, protein D-containing vaccines may be a possible candidate for providing defense against NTHi in COPD, but no clinical trials with candidate vaccines are yet available.
Oral vaccines
An alternative approach to vaccination has been the development of oral vaccines using whole killed NTHi. The mechanisms proposed for protection derived from oral vaccines are from rodent models, which demonstrated that they stimulated T-lymphocytes derived from gut-associated lymphoid tissue to translocate to bronchus-associated lymphoid tissue, thereby stimulating the respiratory epithelial host response.Citation135 A number of studies using oral vaccinations of whole killed NTHi vaccine have been published, and analyzed in a recent Cochrane review. The reviewers concluded that oral NTHi vaccination in patients with recurrent exacerbations of COPD did not significantly reduce either the severity or frequency of exacerbations.Citation136
A more recent placebo-controlled study using a new NTHi preparation (HI-1640V) in 38 COPD patients showed no effect on exacerbation frequency but did report reductions in mean duration of exacerbations, antibiotic use, and sputum cultures.Citation137
The oral administration of bacterial lysates to stimulate respiratory immune responses has been used in Europe and China for many years. The OM-85 BV bacterial extract, a lysate of eight pulmonary pathogens including H. influenzae, is the most commonly studied.Citation138,Citation139 A systematic review of published trials of oral immunization with bacterial extracts in COPD concluded that the evidence for a reduction in exacerbations was inconclusive, but there is some evidence for reduction in exacerbation severity and duration.Citation140 To date, oral vaccines have not been included in international guidelines for COPD.
Antibiotics
A number of studies have investigated the effects of long-term or pulsed antibiotics in COPD and have reported that long-term use of macrolide antibiotics is associated with a reduction in exacerbations.Citation141,Citation142 The largest double-blinded, randomized, placebo-controlled trial of azithromycin in COPD patients demonstrated an increase in time to first exacerbation, reduced exacerbation frequency, and made greater improvement in health-related quality of life in the treatment group.Citation143 Sputum cultures were not carried out, but nasopharyngeal swabs were collected in a subset of patients and showed reduced colonization in the treatment group, but increased incidence of macrolide-resistant organisms. A study of pulsed moxifloxacin also showed a reduction in exacerbations and a trend toward a reduction in subjects with bacteria cultured in sputum in the treatment group.Citation144 Macrolide antibiotics have a number of effects apart from their antibacterial effects, including anti-inflammatory and antiviral effects.Citation145 Therefore, the mechanisms whereby they reduce exacerbations in COPD are unclear. In fact, in those studies in which sputum microbiology was examined, antibiotic therapy appeared to have no effect on prevalence of positive sputum cultures.Citation141,Citation142 Therefore, the beneficial effects of macrolides may be mediated by mechanisms other than their antibacterial effects. Concerns remain regarding the development of antibiotic resistance with long-term use of antibiotics and may limit their use as a therapeutic strategy in COPD.Citation146
Conclusion
Bacterial infection is common in COPD, both as persistent infection in stable patients and in exacerbated patients. The most common bacteria detected in COPD patients is H. influenzae, and this organism appears to be uniquely adapted to exploit structural and immunological abnormalities in the lungs in COPD to establish chronic infection. Persistent infection has been termed colonization, but there is now a wealth of evidence that outcomes are worse in COPD patients with chronic bacterial infection. Most studies to date have defined the presence or absence of H. influenzae, using sputum cultures, but studies using newer molecular diagnostic methods suggest that culture underestimates the true prevalence of H. influenzae infections. Moreover, with the advent of the ability to sequence the entire respiratory microbiome, defining infection as either the presence or absence of an organism is clearly overly simplistic. Increasingly, concepts such as the diversity, richness, evenness, and dominance of bacterial populations will be used to describe the respiratory microbiome. Therefore, current thinking regarding the relationships between H. influenzae and COPD will change radically on the basis of these new concepts. This, in turn, will lead to novel therapeutic strategies that may be based on particular microbial patterns in the airways in individual COPD patients. Eradication or prevention of H. influenzae infection may lead to improved clinical outcomes in COPD, and future therapies may include vaccination, antimicrobials, augmentation of immune responses, or even manipulation of the respiratory microbiome, as has already been trialed in the gastrointestinal tract. In addition, the recognition of the relationship between respiratory virus infection and H. influenzae, coupled with the development of antiviral agents, offers the possibility of reducing the burden of bacterial infection by treating or preventing respiratory virus infections. Current therapies for COPD (inhaled bronchodilators and corticosteroids) have only modest effects and do not prevent disease progression. New therapies targeting H. influenzae offer a novel therapeutic strategy that provides the possibility of improving clinical outcomes and modifying disease activity in COPD.
Disclosure
SLJ has received institutional funding for clinical trials and research grants and consultant compensation from Centocor, Sanofi, Pasteur, GlaxoSmithKline, Chiesi, Boehringer Ingelheim, Novartis, and Synairgen, as well as consultant compensation from Grünenthal, and has share options in Synairgen. PM has received speaker’s fees and travel grants from GlaxoSmithKline and Novartis. The other authors report no conflicts of interest in this work.
References
- HalbertRJNatoliJLGanoABadamgaravEBuistASManninoDMGlobal burden of COPD: systematic review and meta-analysisEur Respir J200628352353216611654
- CosioMGSaettaMAgustiAImmunologic aspects of chronic obstructive pulmonary diseaseN Engl J Med2009360232445245419494220
- LapperreTSPostmaDSGosmanMMRelation between duration of smoking cessation and bronchial inflammation in COPDThorax200661211512116055612
- AlikhanMMLeeFEUnderstanding nontypeable Haemophilus influenzae and chronic obstructive pulmonary diseaseCurr Opin Pulm Med201420215916424441573
- SinganayagamAJoshiPVMalliaPJohnstonSLViruses exacerbating chronic pulmonary disease: the role of immune modulationBMC Med20121012722420941
- BeasleyVJoshiPVSinganayagamAMolyneauxPLJohnstonSLMalliaPLung microbiology and exacerbations in COPDInt J Chron Obstruct Pulmon Dis2012755556922969296
- DonaldsonGCSeemungalTAPatelISAirway and systemic inflammation and decline in lung function in patients with COPDChest200512841995200416236847
- DonaldsonGCSeemungalTABhowmikAWedzichaJARelationship between exacerbation frequency and lung function decline in chronic obstructive pulmonary diseaseThorax2002571084785212324669
- SeemungalTADonaldsonGCPaulEABestallJCJeffriesDJWedzichaJAEffect of exacerbation on quality of life in patients with chronic obstructive pulmonary diseaseAm J Respir Crit Care Med19981575 Pt 1141814229603117
- PapiABellettatoCMBraccioniFInfections and airway inflammation in chronic obstructive pulmonary disease severe exacerbationsAm J Respir Crit Care Med2006173101114112116484677
- KingPHaemophilus influenzae and the lung (Haemophilus and the lung)Clin Transl Med2012111023369277
- FontanalsDBouRPonsIPrevalence of Haemophilus influenzae carriers in the Catalan preschool population. Working Group on Invasive Disease Caused by Haemophilus influenzaeEur J Clin Microbiol Infect Dis200019430130410834821
- RosellAMonsóESolerNMicrobiologic determinants of exacerbation in chronic obstructive pulmonary diseaseArch Intern Med2005165889189715851640
- BandiVApicellaMAMasonENontypeable Haemophilus influenzae in the lower respiratory tract of patients with chronic bronchitisAm J Respir Crit Care Med2001164112114211911739144
- SethiSMaloneyJGroveLWronaCBerensonCSAirway inflammation and bronchial bacterial colonization in chronic obstructive pulmonary diseaseAm J Respir Crit Care Med2006173999199816474030
- ClementiCFMurphyTFNon-typeable Haemophilus influenzae invasion and persistence in the human respiratory tractFront Cell Infect Microbiol20111122919570
- JansonHRuanMForsgrenALimited diversity of the protein D gene (hpd) among encapsulated and nonencapsulated Haemophilus influenzae strainsInfect Immun19936111454645528104899
- WangXMairRHatcherCDetection of bacterial pathogens in Mongolia meningitis surveillance with a new real-time PCR assay to detect Haemophilus influenzaeInt J Med Microbiol2011301430330921276750
- UeyamaTKuronoYShirabeKTakeshitaMMogiGHigh incidence of Haemophilus influenzae in nasopharyngeal secretions and middle ear effusions as detected by PCRJ Clin Microbiol1995337183518387665655
- TianGZZhangLJWangXLRapid detection of Haemophilus influenzae and Haemophilus parainfluenzae in nasopharyngeal swabs by multiplex PCRBiomed Environ Sci201225336737122840589
- BinksMJTempleBKirkhamLAMolecular surveillance of true nontypeable Haemophilus influenzae: an evaluation of PCR screening assaysPLoS ONE201273e3408322470516
- ZhuBXiaoDZhangHMALDI-TOF MS distinctly differentiates nontypable Haemophilus influenzae from Haemophilus haemolyticusPLoS ONE201382e5613923457514
- DicksonRPErb-DownwardJRHuffnagleGBThe role of the bacterial microbiome in lung diseaseExpert Rev Respir Med20137324525723734647
- HiltyMBurkeCPedroHDisordered microbial communities in asthmatic airwaysPLoS ONE201051e857820052417
- PatelISSeemungalTAWilksMLloyd-OwenSJDonaldsonGCWedzichaJARelationship between bacterial colonisation and the frequency, character, and severity of COPD exacerbationsThorax200257975976412200518
- WilkinsonTMPatelISWilksMDonaldsonGCWedzichaJAAirway bacterial load and FEV1 decline in patients with chronic obstructive pulmonary diseaseAm J Respir Crit Care Med200316781090109512684248
- HurstJRWilkinsonTMPereraWRDonaldsonGCWedzichaJARelationships among bacteria, upper airway, lower airway, and systemic inflammation in COPDChest200512741219122615821198
- MurphyTFBrauerALSchiffmacherATSethiSPersistent colonization by Haemophilus influenzae in chronic obstructive pulmonary diseaseAm J Respir Crit Care Med2004170326627215117742
- GarchaDSThurstonSJPatelARChanges in prevalence and load of airway bacteria using quantitative PCR in stable and exacerbated COPDThorax201267121075108022863758
- BafadhelMMcKennaSTerrySAcute exacerbations of chronic obstructive pulmonary disease: identification of biologic clusters and their biomarkersAm J Respir Crit Care Med2011184666267121680942
- CurranTCoylePVMcManusTEKidneyJCoulterWAEvaluation of real-time PCR for the detection and quantification of bacteria in chronic obstructive pulmonary diseaseFEMS Immunol Med Microbiol200750111211817439541
- GroenewegenKHWoutersEFBacterial infections in patients requiring admission for an acute exacerbation of COPD; a 1-year prospective studyRespir Med200397777077712854626
- MolyneauxPLMalliaPCoxMJOutgrowth of the bacterial airway microbiome after rhinovirus exacerbation of chronic obstructive pulmonary diseaseAm J Respir Crit Care Med2013188101224123123992479
- HuangYJSethiSMurphyTNariyaSBousheyHALynchSVAirway microbiome dynamics in exacerbations of chronic obstructive pulmonary diseaseJ Clin Microbiol20145282813282324850358
- RogersGBvan der GastCJSerisierDJPredominant pathogen competition and core microbiota divergence in chronic airway infectionISME J2014 Epub ahead of print http://dx.doi.org/10.1038/ismej.2014.124
- KnowlesMRDanielsLADavisSDZariwalaMALeighMWPrimary ciliary dyskinesia. Recent advances in diagnostics, genetics, and characterization of clinical diseaseAm J Respir Crit Care Med2013188891392223796196
- WielandCWFlorquinSMarisNAThe MyD88-dependent, but not the MyD88-independent, pathway of TLR4 signaling is important in clearing nontypeable haemophilus influenzae from the mouse lungJ Immunol200517596042604916237099
- ReddyMSMurphyTFFadenHSBernsteinJMMiddle ear mucin glycoprotein: purification and interaction with nontypable Haemophilus influenzae and Moraxella catarrhalisOtolaryngol Head Neck Surg199711621751809051060
- MiyamotoNBakaletzLOSelective adherence of non-typeable Haemophilus influenzae (NTHi) to mucus or epithelial cells in the chinchilla eustachian tube and middle earMicrob Pathog19962153433568938642
- BerensonCSGarlippMAGroveLJMaloneyJSethiSImpaired phagocytosis of nontypeable Haemophilus influenzae by human alveolar macrophages in chronic obstructive pulmonary diseaseJ Infect Dis2006194101375138417054066
- HallströmTRiesbeckKHaemophilus influenzae and the complement systemTrends Microbiol201018625826520399102
- MarcMMKorosecPKosnikMComplement factors c3a, c4a, and c5a in chronic obstructive pulmonary disease and asthmaAm J Respir Cell Mol Biol200431221621915039137
- MarcMMKristanSSRozmanAComplement factor C5a in acute exacerbation of Chronic Obstructive Pulmonary DiseaseScand J Immunol201071538639120500690
- WoofJMKerrMAThe function of immunoglobulin A in immunityJ Pathol2006208227028216362985
- RamSLewisLARicePAInfections of people with complement deficiencies and patients who have undergone splenectomyClin Microbiol Rev201023474078020930072
- KainulainenLNikoskelainenJVuorinenTTevolaKLiippoKRuuskanenOViruses and bacteria in bronchial samples from patients with primary hypogammaglobulinemiaAm J Respir Crit Care Med19991594 Pt 11199120410194166
- KingPTHutchinsonPEJohnsonPDHolmesPWFreezerNJHoldsworthSRAdaptive immunity to nontypeable Haemophilus influenzaeAm J Respir Crit Care Med2003167458759212433671
- KingPTNguiJGunawardenaDHolmesPWFarmerMWHoldsworthSRSystemic humoral immunity to non-typeable Haemophilus influenzaeClin Exp Immunol2008153337638418803761
- KingPNguiJOppedisanoFRobins-BrowneRHolmesPHoldsworthSEffect of interferon gamma and CD40 ligation on intracellular monocyte survival of nontypeable Haemophilus influenzaeAPMIS2008116121043104919133006
- KingPTNguiJFarmerMWHutchinsonPHolmesPWHoldsworthSRCytotoxic T lymphocyte and natural killer cell responses to non-typeable Haemophilus influenzaeClin Exp Immunol2008152354255118462210
- van HamSMvan AlphenLMooiFRvan PuttenJPPhase variation of H. influenzae fimbriae: transcriptional control of two divergent genes through a variable combined promoter regionCell1993736118711968513502
- ErwinALSmithALNontypeable Haemophilus influenzae: understanding virulence and commensal behaviorTrends Microbiol200715835536217600718
- DuimBVogelLPuijkWFine mapping of outer membrane protein P2 antigenic sites which vary during persistent infection by Haemophilus influenzaeInfect Immun19966411467346798890224
- CholonDMCutterDRichardsonSKSerial isolates of persistent Haemophilus influenzae in patients with chronic obstructive pulmonary disease express diminishing quantities of the HMW1 and HMW2 adhesinsInfect Immun200876104463446818678658
- SwordsWENontypeable Haemophilus influenzae biofilms: role in chronic airway infectionsFront Cell Infect Microbiol201229722919686
- MurphyTFKirkhamCBiofilm formation by nontypeable Haemophilus influenzae: strain variability, outer membrane antigen expression and role of piliBMC Microbiol200221711960553
- MurphyTFKirkhamCSethiSLesseAJExpression of a peroxiredoxin-glutaredoxin by Haemophilus influenzae in biofilms and during human respiratory tract infectionFEMS Immunol Med Microbiol2005441818915780580
- LangereisJDHermansPWNovel concepts in nontypeable Haemophilus influenzae biofilm formationFEMS Microbiol Lett20133462818923808954
- St GemeJWIIIFalkowSLoss of capsule expression by Haemophilus influenzae type b results in enhanced adherence to and invasion of human cellsInfect Immun1991594132513331672302
- St GemeJWIIIFalkowSHaemophilus influenzae adheres to and enters cultured human epithelial cellsInfect Immun19905812403640442254028
- ForsgrenJSamuelsonAAhlinAJonassonJRynnel-DagööBLindbergAHaemophilus influenzae resides and multiplies intracellularly in human adenoid tissue as demonstrated by in situ hybridization and bacterial viability assayInfect Immun19946226736797507900
- ForsgrenJSamuelsonALindbergARynnel-DagööBQuantitative bacterial culture from adenoid lymphatic tissue with special reference to Haemophilus [corrected]. [corrected]Acta Otolaryngol199311356686728266797
- AhrénILJansonHForsgrenARiesbeckKProtein D expression promotes the adherence and internalization of non-typeable Haemophilus influenzae into human monocytic cellsMicrob Pathog200131315115811500100
- van SchilfgaardeMEijkPRegelinkAHaemophilus influenzae localized in epithelial cell layers is shielded from antibiotics and antibody-mediated bactericidal activityMicrob Pathog199926524926210222210
- SuYCJalalvandFMörgelinMBlomAMSinghBRiesbeckKHaemophilus influenzae acquires vitronectin via the ubiquitous Protein F to subvert host innate immunityMol Microbiol20138761245126623387957
- HallströmTTrajkovskaEForsgrenARiesbeckKHaemophilus influenzae surface fibrils contribute to serum resistance by interacting with vitronectinJ Immunol2006177143043616785539
- HallströmTZipfelPFBlomAMLauerNForsgrenARiesbeckKHaemophilus influenzae interacts with the human complement inhibitor factor HJ Immunol2008181153754518566420
- KilianMMesteckyJRussellMWDefense mechanisms involving Fc-dependent functions of immunoglobulin A and their subversion by bacterial immunoglobulin A proteasesMicrobiol Rev19885222963033045518
- MurphyTFBrauerALExpression of urease by Haemophilus influenzae during human respiratory tract infection and role in survival in an acid environmentBMC Microbiol201111118321843372
- WhitbyPWMortonDJVanwagonerTMHaemophilus influenzae OxyR: characterization of its regulation, regulon and role in fitnessPLoS ONE2012711e5058823226321
- WhitbyPWVanWagonerTMSealeTWMortonDJStullTLComparison of transcription of the Haemophilus influenzae iron/heme modulon genes in vitro and in vivo in the chinchilla middle earBMC Genomics201314192524373462
- QuJLesseAJBrauerALCaoJGillSRMurphyTFProteomic expression profiling of Haemophilus influenzae grown in pooled human sputum from adults with chronic obstructive pulmonary disease reveal antioxidant and stress responsesBMC Microbiol201010116220515494
- ZhangLPatelMXieJDavisGSMarrsCFGilsdorfJRUrease operon and urease activity in commensal and disease-causing nontypeable Haemophilus influenzaeJ Clin Microbiol201351265365523224103
- ZhangLXieJPatelMNontypeable Haemophilus influenzae genetic islands associated with chronic pulmonary infectionPLoS ONE201279e4473022970300
- St GemeJWPinknerJSIIIKrasanGPHaemophilus influenzae pili are composite structures assembled via the HifB chaperoneProc Natl Acad Sci USA1996932111913119188876237
- HallströmTSinghBResmanFBlomAMMörgelinMRiesbeckKHaemophilus influenzae protein E binds to the extracellular matrix by concurrently interacting with laminin and vitronectinJ Infect Dis201120471065107421881122
- JalalvandFSuYCMörgelinMHaemophilus influenzae protein F mediates binding to laminin and human pulmonary epithelial cellsJ Infect Dis2013207580381323230060
- St GemeJWIIIFalkowSBarenkampSJHigh-molecular-weight proteins of nontypable Haemophilus influenzae mediate attachment to human epithelial cellsProc Natl Acad Sci U S A1993907287528798464902
- JohnsonRWMcGillivaryGDenoëlPPoolmanJBakaletzLOAbrogation of nontypeable Haemophilus influenzae protein D function reduces phosphorylcholine decoration, adherence to airway epithelial cells, and fitness in a chinchilla model of otitis mediaVaccine20112961211122121167861
- DennyFWEffect of a toxin produced by Haemophilus influenzae on ciliated respiratory epitheliumJ Infect Dis19741292931004544023
- JansonHCarlnBCervinAEffects on the ciliated epithelium of protein D-producing and -nonproducing nontypeable Haemophilus influenzae in nasopharyngeal tissue culturesJ Infect Dis1999180373774610438362
- van SchilfgaardeMvan UlsenPEijkPCharacterization of adherence of nontypeable Haemophilus influenzae to human epithelial cellsInfect Immun20006884658466510899870
- BerensonCSKruzelRLEberhardtEImpaired innate immune alveolar macrophage response and the predilection for COPD exacerbationsThorax201469981181824686454
- BerensonCSKruzelRLEberhardtESethiSPhagocytic dysfunction of human alveolar macrophages and severity of chronic obstructive pulmonary diseaseJ Infect Dis2013208122036204523908477
- TaylorAEFinney-HaywardTKQuintJKDefective macrophage phagocytosis of bacteria in COPDEur Respir J20103551039104719897561
- BerensonCSWronaCTGroveLJImpaired alveolar macrophage response to Haemophilus antigens in chronic obstructive lung diseaseAm J Respir Crit Care Med20061741314016574934
- CraigJECliffeAGarnettKHighNJSurvival of nontypeable Haemophilus influenzae in macrophagesFEMS Microbiol Lett20012031556111557140
- ClementiCFHåkanssonAPMurphyTFInternalization and trafficking of nontypeable Haemophilus influenzae in human respiratory epithelial cells and roles of IgA1 proteases for optimal invasion and persistenceInfect Immun201482143344424218477
- KnoblochJSchildKJungckDThe T-helper cell type 1 immune response to gram-negative bacterial infections is impaired in COPDAm J Respir Crit Care Med2011183220421420709824
- AbeYMurphyTFSethiSLymphocyte proliferative response to P6 of Haemophilus influenzae is associated with relative protection from exacerbations of chronic obstructive pulmonary diseaseAm J Respir Crit Care Med2002165796797111934723
- KalathilSGLugadeAAPradhanVT-regulatory cells and programmed death 1+ T cells contribute to effector T-cell dysfunction in patients with chronic obstructive pulmonary diseaseAm J Respir Crit Care Med20141901405024825462
- DuimBBowlerLDEijkPPJansenHMDankertJvan AlphenLMolecular variation in the major outer membrane protein P5 gene of nonencapsulated Haemophilus influenzae during chronic infectionsInfect Immun1997654135113569119473
- DuimBvan AlphenLEijkPJansenHMDankertJAntigenic drift of non-encapsulated Haemophilus influenzae major outer membrane protein P2 in patients with chronic bronchitis is caused by point mutationsMol Microbiol1994116118111898022287
- LomholtHvan AlphenLKilianMAntigenic variation of immunoglobulin A1 proteases among sequential isolates of Haemophilus influenzae from healthy children and patients with chronic obstructive pulmonary diseaseInfect Immun19936111457545818406854
- PolosukhinVVCatesJMLawsonWEBronchial secretory immunoglobulin a deficiency correlates with airway inflammation and progression of chronic obstructive pulmonary diseaseAm J Respir Crit Care Med2011184331732721512171
- MurphyTFLesseAJKirkhamCZhongHSethiSMunsonRSJrA clonal group of nontypeable Haemophilus influenzae with two IgA proteases is adapted to infection in chronic obstructive pulmonary diseasePLoS ONE2011610e2592321998721
- MillaresLMarinAGarcia-AymerichJSauledaJBeldaJMonsóEPAC-COPD Study GroupSpecific IgA and metalloproteinase activity in bronchial secretions from stable chronic obstructive pulmonary disease patients colonized by Haemophilus influenzaeRespir Res201213111323228114
- MarinAGarcia-AymerichJSauledaJPAC-COPD Study GroupEffect of bronchial colonisation on airway and systemic inflammation in stable COPDCOPD20129212113022458940
- DesaiHEschbergerKWronaCBacterial colonization increases daily symptoms in patients with chronic obstructive pulmonary diseaseAnn Am Thorac Soc201411330330924423399
- BeasleyVJoshiPVSinganayagamAMolyneauxPLJohnstonSLMalliaPLung microbiology and exacerbations in COPDInt J Chron Obstruct Pulmon Dis2012755556922969296
- MoghaddamSJClementCGDe la GarzaMMHaemophilus influenzae lysate induces aspects of the chronic obstructive pulmonary disease phenotypeAm J Respir Cell Mol Biol200838662963818096867
- GanesanSComstockATKinkerBMancusoPBeckJMSajjanUSCombined exposure to cigarette smoke and nontypeable Haemophilus influenzae drives development of a COPD phenotype in miceRespir Res20141511124495712
- BresserPOutTAvan AlphenLJansenHMLutterRAirway inflammation in nonobstructive and obstructive chronic bronchitis with chronic haemophilus influenzae airway infection. Comparison with noninfected patients with chronic obstructive pulmonary diseaseAm J Respir Crit Care Med20001623 Pt 194795210988111
- MarinAMonsóEGarcia-NuñezMVariability and effects of bronchial colonisation in patients with moderate COPDEur Respir J201035229530219643939
- HurstJRPereraWRWilkinsonTMDonaldsonGCWedzichaJASystemic and upper and lower airway inflammation at exacerbation of chronic obstructive pulmonary diseaseAm J Respir Crit Care Med20061731717816179639
- WilkinsonTMHurstJRPereraWRWilksMDonaldsonGCWedzichaJAEffect of interactions between lower airway bacterial and rhinoviral infection in exacerbations of COPDChest2006129231732416478847
- SethiSEvansNGrantBJMurphyTFNew strains of bacteria and exacerbations of chronic obstructive pulmonary diseaseN Engl J Med2002347746547112181400
- MurphyTFBrauerALSethiSKilianMCaiXLesseAJHaemophilus haemolyticus: a human respiratory tract commensal to be distinguished from Haemophilus influenzaeJ Infect Dis20071951818917152011
- SethiSWronaCGrantBJMurphyTFStrain-specific immune response to Haemophilus influenzae in chronic obstructive pulmonary diseaseAm J Respir Crit Care Med2004169444845314597486
- FernaaysMMLesseAJSethiSCaiXMurphyTFDifferential genome contents of nontypeable Haemophilus influenzae strains from adults with chronic obstructive pulmonary diseaseInfect Immun20067463366337416714566
- ChinCLManzelLJLehmanEEHaemophilus influenzae from patients with chronic obstructive pulmonary disease exacerbation induce more inflammation than colonizersAm J Respir Crit Care Med20051721859115805181
- GeelenTHGaajetaanGRWoutersEFThe host immune response contributes to Haemophilus influenzae virulenceRespir Med2014108114415224011804
- WangXYKilgorePELimKAInfluenza and bacterial pathogen coinfections in the 20th centuryInterdiscip Perspect Infect Dis2011201114637621747847
- LeeLNDiasPHanDA mouse model of lethal synergism between influenza virus and Haemophilus influenzaeAm J Pathol2010176280081120042666
- ZwaansWAMalliaPvan WindenMERohdeGGThe relevance of respiratory viral infections in the exacerbations of chronic obstructive pulmonary disease-A systematic reviewJ Clin Virol2014 Epub ahead of print http://dx.doi.org/10.1016/j.jcv.2014.06.025
- UngerBLFarisANGanesanSComstockATHershensonMBSajjanUSRhinovirus attenuates non-typeable Hemophilus influenzae-stimulated IL-8 responses via TLR2-dependent degradation of IRAK-1PLoS Pathog2012810e100296923055935
- OliverBGLimSWarkPRhinovirus exposure impairs immune responses to bacterial products in human alveolar macrophagesThorax200863651952518245149
- ComstockATGanesanSChattorajARhinovirus-induced barrier dysfunction in polarized airway epithelial cells is mediated by NADPH oxidase 1J Virol201185136795680821507984
- WangJHKwonHJJangYJRhinovirus enhances various bacterial adhesions to nasal epithelial cells simultaneouslyLaryngoscope200911971406141119434681
- WangJHLeeSHKwonHJJangYJClarithromycin inhibits rhinovirus-induced bacterial adhesions to nasal epithelial cellsLaryngoscope2010120119319919877190
- AvadhanulaVRodriguezCADevincenzoJPRespiratory viruses augment the adhesion of bacterial pathogens to respiratory epithelium in a viral species- and cell type-dependent mannerJ Virol20068041629163616439519
- SuriRMalliaPMartinJEBronchial platelet-activating factor receptor in chronic obstructive pulmonary diseaseRespir Med2014108689890424685340
- BandiVJakubowyczMKinyonCInfectious exacerbations of chronic obstructive pulmonary disease associated with respiratory viruses and non-typeable Haemophilus influenzaeFEMS Immunol Med Microbiol2003371697512770762
- MalliaPFootittJSoteroRRhinovirus infection induces degradation of antimicrobial peptides and secondary bacterial infection in chronic obstructive pulmonary diseaseAm J Respir Crit Care Med2012186111117112423024024
- HutchinsonAFGhimireAKThompsonMAA community-based, time-matched, case-control study of respiratory viruses and exacerbations of COPDRespir Med2007101122472248117822891
- GeorgeSNGarchaDSMackayAJHuman rhinovirus infection during naturally occurring COPD exacerbationsEur Respir J2014441879624627537
- SajjanUSJiaYNewcombDCH. influenzae potentiates airway epithelial cell responses to rhinovirus by increasing ICAM-1 and TLR3 expressionFASEB J200620122121212316914605
- AgrawalAMurphyTFHaemophilus influenzae infections in the H. influenzae type b conjugate vaccine eraJ Clin Microbiol201149113728373221900515
- HiltkeTJSchiffmacherATDagoneseAJSethiSMurphyTFHorizontal transfer of the gene encoding outer membrane protein P2 of nontypeable Haemophilus influenzae, in a patient with chronic obstructive pulmonary diseaseJ Infect Dis2003188111411712825179
- OstbergKLRussellMWMurphyTFMucosal immunization of mice with recombinant OMP P2 induces antibodies that bind to surface epitopes of multiple strains of nontypeable Haemophilus influenzaeMucosal Immunol200921637319079335
- PoolmanJTBakaletzLCrippsADeveloping a nontypeable Haemophilus influenzae (NTHi) vaccineVaccine200019Suppl 1S108S11511163473
- NovotnyLAJurcisekJAGodfroidFPoolmanJTDenoëlPABakaletzLOPassive immunization with human anti-protein D antibodies induced by polysaccharide protein D conjugates protects chinchillas against otitis media after intranasal challenge with Haemophilus influenzaeVaccine200624224804481116616975
- PrymulaRPeetersPChrobokVPneumococcal capsular polysaccharides conjugated to protein D for prevention of acute otitis media caused by both Streptococcus pneumoniae and non-typable Haemophilus influenzae: a randomised double-blind efficacy studyLancet2006367951274074816517274
- HawdonNBimanBMcCreadyWAntibody against Haemophilus influenzae protein D in patients with chronic conditions causing secondary immunodeficiencyVaccine20123071235123822230580
- ClancyRLDunkleyMA vaccine to prevent exacerbations in COPDMed J Aust201119529910021770885
- TeoEHouseHLockhartKPurchuriSNPushparajahJCrippsAWvan DrielMLHaemophilus influenzae oral vaccination for preventing acute exacerbations of chronic bronchitis and chronic obstructive pulmonary diseaseCochrane Database Syst Rev20149CD01001025201571
- TandonMKPhillipsMWatererGDunkleyMComansPClancyROral immunotherapy with inactivated nontypeable Haemophilus influenzae reduces severity of acute exacerbations in severe COPDChest2010137480581119952063
- ColletJPShapiroPErnstPRenziTDucruetTRobinsonAEffects of an immunostimulating agent on acute exacerbations and hospitalizations in patients with chronic obstructive pulmonary disease. The PARI-IS Study Steering Committee and Research Group. Prevention of Acute Respiratory Infection by an ImmunostimulantAm J Respir Crit Care Med19971566171917249412546
- CvoriscecBUstarMPardonRPalecekIStipic-MarkovicAZimicBOral immunotherapy of chronic bronchitis: a double-blind placebo-controlled multicentre studyRespiration19895531291352682862
- ArandjusCBlackPNPoolePJWood BakerRSteurer-SteyCOral bacterial vaccines for the prevention of acute exacerbations in chronic obstructive pulmonary disease and chronic bronchitisRespir Med2006100101671168116934969
- HeZYOuLMZhangJQEffect of 6 months of erythromycin treatment on inflammatory cells in induced sputum and exacerbations in chronic obstructive pulmonary diseaseRespiration201080644545220881376
- SeemungalTAWilkinsonTMHurstJRPereraWRSapsfordRJWedzichaJALong-term erythromycin therapy is associated with decreased chronic obstructive pulmonary disease exacerbationsAm J Respir Crit Care Med2008178111139114718723437
- AlbertRKConnettJBaileyWCCOPD Clinical Research NetworkAzithromycin for prevention of exacerbations of COPDN Engl J Med2011365868969821864166
- SethiSJonesPWTheronMSPULSE Study groupPulsed moxifloxacin for the prevention of exacerbations of chronic obstructive pulmonary disease: a randomized controlled trialRespir Res20101111020109213
- GielenVJohnstonSLEdwardsMRAzithromycin induces anti-viral responses in bronchial epithelial cellsEur Respir J201036364665420150207
- SerisierDJRisks of population antimicrobial resistance associated with chronic macrolide use for inflammatory airway diseasesLancet Respir Med20131326227424429132