
Abstract
Background
Pneumonia poses a significant risk in patients with moderate to severe chronic obstructive pulmonary disease but data are limited on the disease phenotypes most susceptible to pneumonia.
Methods
Cluster analysis using a data-driven recursive partitioning algorithm was employed using baseline data from two pooled one-year randomized exacerbation trials (n=3,255) of fluticasone furoate/vilanterol or vilanterol alone to identify distinct patient groups at greatest risk of pneumonia or serious (hospitalization or death) pneumonia.
Results
Five clusters were identified. Patients at greater risk of first pneumonia had more severe obstruction (forced expiratory volume in one second/forced vital capacity <46%) and either a body mass index <19 kg/m2 (hazard ratio 7.8, 95% confidence interval 4.7–13.0; n=144) or a pneumonia history and greater comorbidities (hazard ratio 4.8, 95% confidence interval 3.0–7.7; n=374) relative to the cluster with the lowest pneumonia risk (reference; n=1310). Multiple comorbidities and use of psychoanaleptics also contributed to an increased risk of pneumonia in more obstructed patients. Independent of cluster, use of inhaled corticosteroids was associated with pneumonia (hazard ratio 1.89, 95% confidence interval 1.25–2.84) and serious pneumonia (hazard ratio 2.92, 95% confidence interval 1.40–6.01).
Conclusion
Cluster analysis can identify patient populations at risk for serious safety outcomes and inform risk management strategies to optimize patient management. The greatest risk for pneumonia was in subjects with multiple pneumonia risk factors.
Introduction
Community-acquired pneumonia results in greater morbidity and mortality in patients with chronic obstructive pulmonary disease (COPD) than in those without the disease.Citation1 The annual incidence of community-acquired pneumonia in the COPD population is estimated to be 22.4 episodes per 1,000 patients,Citation2 and age, severity of COPD, and presence of comorbidity further increase the risk of hospitalization with community-acquired pneumonia. Findings further suggest an increase in pneumonia when COPD is treated with inhaled corticosteroids (ICS), although ICS also reduce the rates of moderate or severe exacerbations of COPD.Citation3 The mechanism by which ICS increase the risk of pneumonia is unclear, but may relate to reducing the inflammatory response, including neutrophils, in the respiratory tract.Citation4
Fluticasone furoate/vilanterol (FF/VI) is a new once-daily ICS/long-acting β2-agonist (LABA) combination (FF/VI 100/25 μg, BREO™ ELLIPTA™, GlaxoSmithKline, Research Triangle Park, NC, USA) that reduces exacerbations of COPD, improves lung function, and may increase the risk of pneumonia compared with the LABA (vilanterol) alone.Citation5 Factors indicated to be associated with this increased risk among patients with COPD treated with FF/VI are consistent with previous observations in the ICS/LABA class, and include older age, lower body mass index (BMI), current smoking, the occurrence of a previous pneumonia, and poorer lung function.Citation5,Citation6
We conducted a cluster analysis using data from two one-year studies of FF/VI and vilanterol to identify combinations of patient characteristics that place patients at greater risk of pneumonia for the purposes of risk management.
Materials and methods
Clinical study design and subjects
The study designs, recruitment criteria, and procedures of the two studies analyzed herein have been previously reported.Citation5 Briefly, patients aged ≥40 years with a documented diagnosis of COPDCitation7 and at least one moderate or severe exacerbation in the prior 12 months were randomized to 52 weeks of treatment with vilanterol 25 μg or FF/VI at strengths of 50/25, 100/25, or 200/25 μg. The primary efficacy endpoint was the annual rate of moderate or severe exacerbations (requiring antibiotics and/or oral corticosteroids and/or resulting in hospitalization) in each treatment arm. Pneumonia was also reported and recorded. The diagnosis was based on the investigator’s judgment based on the available clinical evidence, including a chest X-ray. Pneumonia was defined as an adverse event or as a serious adverse event if it resulted in hospitalization.
Cluster analysis methodology
Cluster analysis was employed using the R-package and RPART procedure (http://www.r-project.org/).Citation8,Citation9 Using the data-driven recursive partitioning algorithm to model time to first or severe pneumonia, the decision tree created clusters of patients based on the intent-to-treat population such that differences in risk of pneumonia were maximized among clusters. The size of the decision tree was determined by minimizing the cross validation error; and cluster membership was then assigned to each patient based on the selected tree. The three doses of FF/VI were collapsed into one group to examine treatment versus nontreatment with FF/VI. Risk of pneumonia and serious pneumonia was calculated using Cox proportional hazards, with an initial model adjusted for study, smoking status, and region as a random effect. Because these variables were part of the initial model used to calculate risk, they could not be included as variables for defining the clusters. The results of the initial analysis did not identify treatment as a variable associated with clusters (see Results section), thus treatment was included as an explanatory variable within the final model. To avoid identification of spurious clusters, the number of patients within any one cluster was set at ≥100. To avoid confounding by similar variables (eg, membership of a specific age group such as 65–75 years versus age as a continuous variable) each variable was assessed for collinearity with every other variable using Pearson’s correlation coefficients. Where two similar variables exhibited a Pearson’s correlation coefficient value ≥0.7 (eg, eosinophil count versus percentage) only one variable was retained based on the clinician’s selection. Variables included in the analysis are noted in .
Table 1 Characteristics and variables considered in initial cluster analysis
Hazard ratios (HR) and 95% confidence intervals (CI) were calculated for each cluster, using the cluster with the lowest incidence rate as the reference value. Baseline variables within each cluster are presented as proportions for categorical variables and medians (interquartile range) for continuous variables. Differences between variables in clusters were assessed using χ2 for categorical variables and the Wilcoxon rank sum test for continuous variables.
Results
Primary efficacy and safety
The primary data of these studies have already been reported.Citation5 More pneumonia, serious pneumonia, and fatal pneumonia events occurred with FF/VI than vilanterol ().
Table 2 Pneumonia, serious pneumonia, and fatal pneumonia events with FF/VI and VI
Cluster analysis
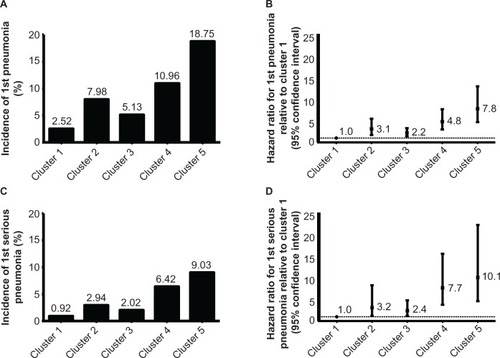
This analysis yielded five clusters combining clinical and demographic attributes, including forced expiratory volume in one second/forced vital capacity (FEV1/FVC) ratio, psychoanaleptic use, BMI, and history of pneumonia (). The final tree was based on combining the similar trees determined for all pneumonia events () and serious pneumonia events (subset of pneumonia events resulting in hospitalization; ). Treatment (FF/VI or vilanterol) was not identified as a variable in the tree that maximized the difference in risk between clusters, so was included in the final Cox model. The incidence of pneumonia and serious pneumonia was lowest in cluster 1 (2.52% and 0.92%, respectively) during the one-year study period and highest in cluster 5 (18.75% and 9.03%, respectively), generally increasing from left to right (). Relative to cluster 1 (reference), HRs for the time to first pneumonia in clusters 2–5 ranged from a 2.2-fold increased risk of first pneumonia in cluster 3 versus cluster 1 to a 7.8-fold increased risk of first serious pneumonia in cluster 5 versus cluster 1 ().
Figure 1 Cluster analysis tree of first and first serious pneumonia.
Abbreviations: BMI, bone mass index; FEV1, forced expiratory volume in one second; FVC, forced vital capacity; FF/VI, fluticasone furoate/vilanterol; VI, vilanterol.
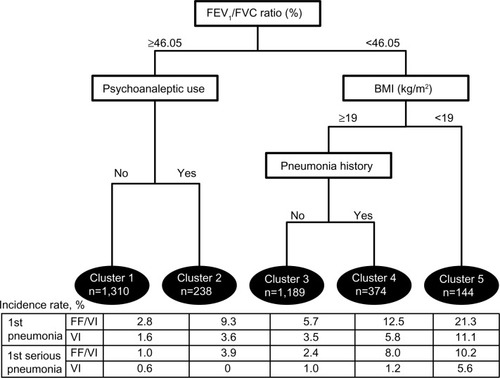
Figure 2 Incidence (A and C) and hazard ratios (B and D) for first pneumonia (A and B) and first serious pneumonia (C and D) by cluster.
Patient clusters
The clusters identified comprised the following: patients with poorer lung function (FEV1/FVC <46.05%) and lower BMI <19 kg/m2 (cluster 5); patients with poorer lung function, normal BMI and prior history (cluster 4) or no history (cluster 3) of pneumonia; and patients with better lung function in receipt (cluster 2) or not in receipt (cluster 1) of psychoanaleptics (89% antidepressants). There were significant baseline differences between clusters assessed by demographics, spirometry, COPD history, or COPD type () and comorbidities or concomitant medications (). There were no clinically significant differences in laboratory measures across clusters (data not shown).
Table 3 Patient characteristics by cluster
Table 4 Patient comorbidities and concomitant medications by cluster
Patients with the greatest risk of pneumonia and serious pneumonia (cluster 5) predominantly had a history of emphysema, the highest prevalence of current smoking, the greatest extent of reversibility, and were more likely to have experienced at least two exacerbations in the prior year compared with those in other clusters. Patients in cluster 5 also had considerably fewer comorbidities than other clusters and were in receipt of the fewest concomitant medications. Patients in clusters 4 and 2 showed higher rates of comorbidity and concomitant medication.
Patients in cluster 3 were predominantly male and had COPD for the greatest amount of time, but were the least likely to have experienced an exacerbation requiring hospitalization in the prior year; this cluster was primarily differentiated from the other clusters on the basis of poorer lung function and the absence of other defining characteristics.
Cluster 2 subjects were predominantly female, in addition to having a higher prevalence of comorbidity (and typically the highest receipt of concomitant medication). This cluster contained the fewest Hispanic and Latino patients, had the least impaired lung function, greatest proportion of current smokers, and greatest proportion of reversible patients. Forty-three percent of subjects in cluster 2 were also using psycholeptic medications, over half of whom were exposed to benzodiazepines ().
Cluster 1 (the reference population) contained the greatest number of patients overall, and were more likely to be Hispanic or Latino and more likely to have a history of COPD characterized by bronchitis than patients in the other clusters.
Treatment effects
In each cluster, pneumonia or serious pneumonia occurred more frequently with any strength of FF/VI therapy than with vilanterol alone (see Table in ). Across all clusters and relative to treatment with vilanterol alone, treatment with FF/VI at any strength (ie, all strengths combined) was associated with a significantly greater risk of first pneumonia (HR 1.89, CI 1.25–2.84) and first serious pneumonia (HR 2.92, CI 1.40–6.01). No interaction was found between treatment and cluster for first pneumonia (P=0.9741) or first serious pneumonia (P=0.8089). Doses of FF/VI were balanced across the clusters (P=0.2064, ).
Effects of variables used in the model
Smoking status (current) as a main effect was not associated with a significantly increased risk of first pneumonia (HR 1.0, CI 0.7–1.4) or first serious pneumonia (HR 0.9, CI 0.6–1.5). The distribution of geographic region across clusters was significantly different (P≤0.0001) relative to the total distribution (). Overall, approximately one third of patients were from the USA, a quarter were from Europe, and the remainder were balanced between the two “other” regions (Argentina, Chile, Mexico, Peru, and the Philippines as other region 1, and Australia, Canada, and South Africa as other region 2). In cluster 2 (in receipt of psychoanaleptics, higher lung function, more comorbidity, predominantly female), 61.3% of the population were from the USA, while compared with the total population proportionately fewer patients were from Europe or “other” region 1. The USA also provided the majority of patients in cluster 4 (poorer lung function, higher proportions of comorbidity, prior pneumonia) and cluster 5 (poorer lung function, lower BMI, greatest pneumonia risk).
Table 5 Geographic contribution to total population and each cluster
Discussion
Cluster analysis of two replicate one-year studies of FF/VI versus vilanterol identified five clusters of patients with differing risks for occurrence of pneumonia or serious pneumonia. Using the cluster with the lowest incidence of pneumonia (cluster 1) as a reference, the risk of pneumonia or serious pneumonia was significantly increased in each of the remaining clusters. The clusters identified were defined by combinations of the established pneumonia risk factors of lung function, BMI, and prior history of pneumonia, and also by the use of psychoanaleptic medication. FEV1/FVC was the main characteristic used to describe the clusters, and clusters 3, 4, and 5 were characterized by greater obstruction, as defined by FEV1/FVC, than clusters 1 and 2.
Cluster 5 had the highest risk of pneumonia, and subjects in this cluster showed the greatest extent of lung function impairment, defined as FEV1% predicted, and the lowest BMI of all the clusters. Cluster 4 subjects had more impaired lung function (FEV1% predicted), more comorbid conditions, and a prior history of pneumonia compared with cluster 1, while those in cluster 3 had only more impaired lung function (FEV1% predicted) compared with cluster 1. Cluster 2 subjects also showed an increased risk of pneumonia relative to cluster 1; cluster 2 subjects differed from those in cluster 1 by use of psychoanaleptics and an increased prevalence of comorbidities. The algorithm did not identify treatment with FF/VI versus vilanterol as a variable maximizing the difference in risk of pneumonia between clusters; however, treatment with FF/VI versus vilanterol alone did result in a significantly increased risk of pneumonia or serious pneumonia in each cluster. There was no differential treatment effect across clusters.
Vanfletern et alCitation10 have identified different COPD phenotypes based on the number and types of comorbidities, and the phenotypes identified loosely track with the clusters of varying pneumonia risk identified in our analysis, including low comorbidity (cluster 1), psychological (cluster 2), cardiovascular (clusters 2 and 4), metabolic (clusters 2 and 4), and cachectic (cluster 5) groups. In our analysis, the initial split of the population occurred based on lung function (FEV1/FVC ratio <46%). Poorer lung function is known to increase the risk of pneumonia in patients with COPD,Citation1,Citation11 so it is perhaps unsurprising that our analysis defined lung function as the initial variable associated with an increased/decreased risk of pneumonia. Increasing obstruction measured as FEV1 and increasing prevalence of emphysematous COPD generally tracked with increasing risk among the cohorts.
The poorer lung function population subsequently split on the basis of BMI and patients with both poorer lung function and a BMI <19 kg/m2 formed the cluster (cluster 5) with the greatest risk and incidence of pneumonia and serious pneumonia. This finding in part confirms that of the initial analysis, in which BMI was associated with the occurrence of pneumonia,Citation12 and also aligns with other findings.Citation11 It follows that in patients with both poor lung function and low BMI, the risk of pneumonia would be increased as a consequence of the presence of both risk factors.
Lower lung function, a prior pneumonia event, and greater prevalence of comorbidities were the defining characteristics of cluster 4. In COPD, it is known that the incidence of community-acquired pneumonia is approximately doubled in patients with a prior event,Citation2 which suggests that, as has been shown for exacerbations of COPD,Citation13 the occurrence of a prior event may increase the risk of a recurrent event.
The finding that cluster 2 comprised patients with better lung function (FEV1/FVC >46%), more psychoanaleptic use, and frequent psycholeptic use suggests that receipt of psychotropic medications presents an increased risk of pneumonia in COPD that is distinct from established factors. Other studies have reported that both psychotropic drugsCitation14 and the underlying psychiatric/neurological disorders they treatCitation15,Citation16 increase the risk of pneumonia. Patients with psychiatric and neurological disorders can have impairment in both the perception of symptoms and the seeking of health care, and may be more likely to smoke.Citation17 Patients with COPD who smoke have a higher prevalence of depression and are at greater risk of developing depression than those who do not.Citation18 Depressive symptoms are known to pose a greater risk of exacerbation, exacerbation-related hospitalization, and death in COPD.Citation19
Patients taking psychotropic medications are also at risk for aspiration pneumonia because of dysphagiaCitation14,Citation17 and relaxation of lower esophageal sphincter tone that can aggravate gastroesophageal reflux.Citation20 The most common class of psychotropic drugs used by patients in these studies was benzodiazepines, which were estimated to be dispensed to nearly one third of patients with COPD in a Canadian study.Citation21 A recent nested case-control and survival analysis in a population-based cohort indicated that benzodiazepines increase the risk of pneumonia by nearly 50%,Citation22 although an earlier study suggested that this risk was related to concomitant opioid use.Citation23 Aside from the aspiration risk cited, it has been suggested that benzodiazepine-related pneumonia may be due to immunosuppression that is mediated via activation of gamma-aminobutyric acid A receptors on macrophages.Citation24
Another important aspect related to increased risk of pneumonia identified in this analysis is the presence of multiple comorbidities. The presence of a history or risk of cardiovascular disease and the incidence of coronary artery disease and cardiac, metabolic, or vascular disorders was highest in clusters 2 and 4, in whom the risk of pneumonia was greater than in both cluster 1 (the reference population) and cluster 3. Both congestive heart failure and peripheral vascular disease are independent risk factors for the occurrence of community-acquired pneumonia.Citation2 Similarly, both cardiovascular disease and diabetes place patients with COPD at an increased risk of hospitalization for pneumonia. This would suggest that an increased risk of pneumonia would be most likely to be present in subjects with comorbid cardiovascular disease treated with FF/VI versus vilanterol. However, in other analyses of the data utilized here (not shown), subjects with comorbid cardiovascular disease treated with FF/VI had a numerically lower risk for occurrence of pneumonia when compared with subjects with no comorbid cardiovascular disease treated with vilanterol. The definition of comorbid cardiovascular disease used in this analysis was a prior or current diagnosis of coronary artery disease, myocardial infarction, arrhythmia, congestive heart failure, hypertension, cerebrovascular accident, diabetes mellitus, or hypercholesterolemia. This broad definition may have had a confounding effect by classing together morbidities, and perhaps does not adequately reflect the complexity of COPD (eg, a single factor versus multiple factors contributing to risk of pneumonia).
It is also notable that only a minority of patients were vaccinated for pneumonia (range across clusters, 4%–9%) or influenza (range 19%–23%). Vaccination rates were highest for cluster 4, which had a higher level of obstruction, pneumonia history, and more frequent comorbidities relative to other clusters. Cluster 4 patients included disproportionate numbers from the USA, suggesting that greater vaccination rates and comorbidities in this cluster could relate to differences in health systems and lifestyle or nutrition relative to other regions. Imbalances in geographic distribution across other clusters support this possibility. The low vaccination rates in these COPD study patients suggests a modifiable risk of pneumonia exists that can be further addressed within clinical practice settings and by vaccine uptake strategies. Although the evidence is not consistent, the GOLD (Global Initiative for Chronic Obstructive Lung Disease) consensus documentCitation25 and Centers for Disease Control and PreventionCitation26 recommend that influenza and pneumonia vaccination be offered to every COPD patient, where vaccination is more effective in older patients, severe COPD patients, and those with comorbid cardiovascular disease. Despite the increased risk of pneumonia in these groups, the patients with greatest risk of pneumonia are also those who receive the greatest benefit of ICS, including those with increased obstruction and low BMI.Citation6
Treatment allocation was balanced across clusters, which would be expected due to randomization. There was a small imbalance in cluster 5, with a slight underrepresentation of FF/VI 100/25 μg (17.4%) and overrepresentation of FF/VI 200/25 μg (31.3%), compared with the 25% expected. This variation likely resulted due to chance because this was the smallest of the clusters (n=144), but could have contributed to the observed increased risk of pneumonia. Based on the benefit-risk profile,Citation5 the 200/25 dose of FF/VI was not progressed for registration in COPD.
Regardless of cluster, there is an approximate two-fold increase in the relative risk of pneumonia and a nearly three-fold increase of serious pneumonia among patients treated with FF/VI relative to vilanterol; however, the absolute risk of pneumonia is greatest among those who benefit most from FF/VI (eg, clusters 4 and 5).Citation6 Risk factors that put individuals at greatest risk of pneumonia (eg, low BMI, increased airflow obstruction, multiple morbidities, and prior history of pneumonia) can be collectively assessed when making treatment decisions. If the greatest risk of pneumonia had been found among patients with modest benefit from FF/VI, the benefit–risk profile may merit a bronchodilator alone (eg, vilanterol) rather than FF/VI, to maintain a positive benefit–risk profile.
Cluster analysis is a useful tool to examine heterogeneous diseases such as COPDCitation27 and has been employed to aid in the identification of distinct clusters or phenotypes of COPD,Citation28 including those at greater risk of mortality.Citation29,Citation30 Interestingly, there is some overlap in the phenotypes identified as being at greater risk of mortality and pneumonia, including those with multiple comorbidities and moderate to severe airflow limitationCitation29,Citation30 and those with severe airflow limitation with low BMI.Citation29 Cluster analysis differs principally from subgroup analysis in that it seeks to first maximize differences between groups of patients using a data-driven algorithm and then identify multiple characteristics which define those patients. In comparison, subgroup analysis first defines patients by individual characteristics one at a time.
This analysis benefited from a large dataset representing a broad international patient population, which is an important element in allowing robust clusters to be identified. However, the generalizability of these findings is limited to patients with a history of COPD exacerbation in the past year. An additional limitation is the lack of validation via a second dataset or split sample; however, results are consistent with what is known about risk factors for pneumonia. Given the small number of pneumonia events, we were not able to evaluate the effect of ICS dose on pneumonia within clusters. Finally, definitions of pneumonia employed in the original studies and in this analysis did not include any standardized assessment of pneumonia severity, such as CURB-65 or Pneumonia Severity Index.Citation31 The definition of serious pneumonia was based on hospitalization due to pneumonia, which may vary across health systems, relative to standardized criteria.
The present analysis identified five clusters of patients with differing risks of pneumonia occurrence over one year of therapy with FF/VI or vilanterol. The clusters were in part defined by well established risk factors, such as BMI and lung function and as such, the outcomes can be considered confirmatory of other findings. The clusters were also defined by less established risk factors, such as prior occurrence of pneumonia, receipt of psychotropic medications, and presence of multiple comorbidities, and as such can be considered hypothesis-generating. Our analysis suggests that physicians should consider many factors and combination of risk factors when treating COPD patients with an ICS/LABA such as FF/VI, balancing the risks and benefit in the individual patient.
Author contributions
RLD and DBR conceived the analysis; RLD, HL and DH conducted the analysis; all authors interpreted the results, developed the manuscript, and approved the final draft for submission.
Supplementary materials
Figure S1 Cluster analysis tree of first pneumonia.
Abbreviations: BMI, bone mass index; FEV1, forced expiratory volume in one second.
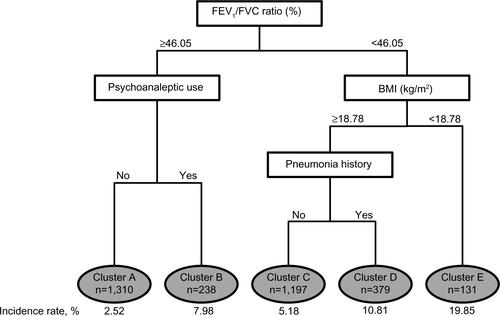
Figure S2 Cluster analysis tree of first serious pneumonia.
Abbreviations: FEV1, forced expiratory volume in one second; BMI, body mass index.
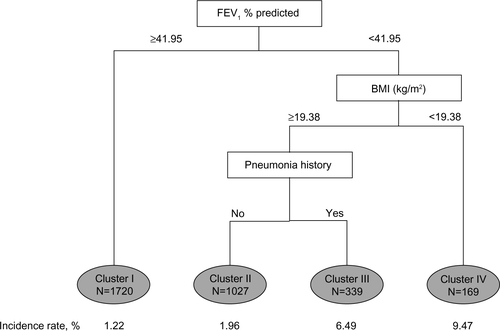
Table S1 Psychoanaleptic and psycholeptic prescription in the five clusters
Table S2 Distribution of treatment by cluster
Disclosure
This work was supported by GlaxoSmithKline (protocol number WEUKBRE6624). Editorial support in the form of development of an outline and first draft under the guidance of the lead author, collation of author comments on subsequent drafts, referencing, copyediting, and generation of tables and figures was provided by Geoff Weller, Gardiner-Caldwell Communications (Macclesfield, UK). Funding for this support was provided by GlaxoSmithKline. All authors are employees of and hold shares in GlaxoSmithKline.
References
- RestrepoMIMortensenEMPughJAAnzuetoACOPD is associated with increased mortality in patients with community-acquired pneumoniaEur Respir J200628234635116611653
- MüllerovaHChigboCHaganGWThe natural history of community-acquired pneumonia in COPD patients: a population database analysisRespir Med201210681124113322621820
- NanniniLJPoolePMilanSJKestertonACombined corticosteroid and long-acting beta(2)-agonist in one inhaler versus inhaled corticosteroids alone for chronic obstructive pulmonary diseaseCochrane Database Syst Rev20138CD00682623990350
- BarnesNCQiuYSPavordIDAntiinflammatory effects of salmeterol/fluticasone propionate in chronic obstructive lung diseaseAm J Respir Crit Care Med2006173773674316424444
- DransfieldMTBourbeauJJonesPWOnce-daily inhaled fluticasone furoate and vilanterol versus vilanterol only for prevention of exacerbations of COPD: two replicate double-blind, parallel-group, randomised controlled trialsLancet Respir Med20131321022324429127
- BREO™ ELLIPTA™ (fluticasone furoate/vilanterol inhalation powder) for treatment of chronic obstructive pulmonary disease. NDA204275 Available from: http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/Pulmonary-AllergyDrugsAdvisoryCommittee/UCM347931.pdfAccessed January 6, 2014
- CelliBRMacNeeWATS/ERS Task ForceStandards for the diagnosis and treatment of patients with COPD: a summary of the ATS/ERS position paperEur Respir J200423693294615219010
- BreimanLClassification and Regression TreesNew York, NY, USAChapman and Hall1983
- TherneauTAtkinsonBRipleyBRPART: Recursive Partitioning. R package version 4.0-12012 Available from: http://cran.r-project.org/web/packages/rpart/index.htmlAccessed January 6, 2014
- VanfleterenLESpruitMAGroenenMClusters of comorbidities based on validated objective measurements and systemic inflammation in patients with chronic obstructive pulmonary diseaseAm J Respir Crit Care Med2013187772873523392440
- CrimCCalverleyPMAndersonJAPneumonia risk in COPD patients receiving inhaled corticosteroids alone or in combination: TORCH study resultsEur Respir J200934364164719443528
- SinghSLokeYKRisk of pneumonia associated with long-term use of inhaled corticosteroids in chronic obstructive pulmonary disease: a critical review and updateCurr Opin Pulm Med201016211812219926996
- HurstJRVestboJAnzuetoASusceptibility to exacerbation in chronic obstructive pulmonary diseaseN Engl J Med2010363121128113820843247
- KnolWvan MarumRJJansenPASouvereinPCSchobbenAFEgbertsACAntipsychotic drug use and risk of pneumonia in elderly peopleJ Am Geriatr Soc200856466166618266664
- SeminogOOGoldacreMJRisk of pneumonia and pneumococcal disease in people with severe mental illness: English record linkage studiesThorax201368217117623242947
- ChouFHTsaiKYChouYMThe incidence and all-cause mortality of pneumonia in patients with schizophrenia: a nine-year follow-up studyJ Psychiatr Res201347446014623317876
- QuintJKBrownJSWeighing up risk factors for pneumonia: the role of mental illness and benzodiazepine useThorax201368212112223250999
- HananiaNAMüllerovaHLocantoreNWDeterminants of depression in the ECLIPSE chronic obstructive pulmonary disease cohortAm J Respir Crit Care Med2011183560461120889909
- PapaioannouAIBartziokasKTsikrikaSThe impact of depressive symptoms on recovery and outcome of hospitalised COPD exacerbationsEur Respir J201341481582322878874
- RushnakMJLeevyCMEffect of diazepam on the lower esophageal sphincter. A double-blind controlled studyAm J Gastroenterol19807321271307395839
- VozorisNTFischerHDWangXAndersonGMBenzodiazepine use among older adults with chronic obstructive pulmonary disease: a population-based cohort studyDrugs Aging201330318319223371396
- ObioraEHubbardRSandersRDMylesPRThe impact of benzodiazepines on occurrence of pneumonia and mortality from pneumonia: a nested case-control and survival analysis in a population-based cohortThorax201368216317023220867
- DublinSWalkerRLJacksonMLUse of opioids or benzodiazepines and risk of pneumonia in older adults: a population-based case-control studyJ Am Geriatr Soc201159101899190722091503
- SandersRDDegosVYoungWLCerebral perfusion under pressure: is the autoregulatory ‘plateau’ a level playing field for all?Anaesthesia2011661196897221933160
- VestboJHurdSSAgustíAGGlobal strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summaryAm J Respir Crit Care Med2013187434736522878278
- Centers for Disease Control and PreventionAdvisory Committee on Immunization Practices recommended immunization schedules for persons aged 0 through 18 years and adults aged 19 years and older – United States, 2013MMWR Surveill Summ201362Suppl 11
- WeatherallMShirtcliffePTraversJBeasleyRUse of cluster analysis to define COPD phenotypesEur Respir J201036347247420930198
- TraversJWeatherallMFingletonJBeasleyRTowards individualised medicine for airways disease: identifying clinical phenotype groupsEur Respir J20123941033103422467724
- BurgelPRRocheNPaillasseurJLClinical COPD phenotypes identified by cluster analysis: validation with mortalityEur Respir J201240249549622855468
- Garcia-AymerichJGómezFPBenetMIdentification and prospective validation of clinically relevant chronic obstructive pulmonary disease (COPD) subtypesThorax201166543043721177668
- LokeYKKwokCSNirubanAMyintPKValue of severity scales in predicting mortality from community-acquired pneumonia: systematic review and meta-analysisThorax2010651088489020729235